
Implementation and Effectiveness of Novel Therapeutic Substances for Advanced Malignant Melanoma in Saxony, Germany, 2010–2020—Cohort Study Based on Administrative Data

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Statistics
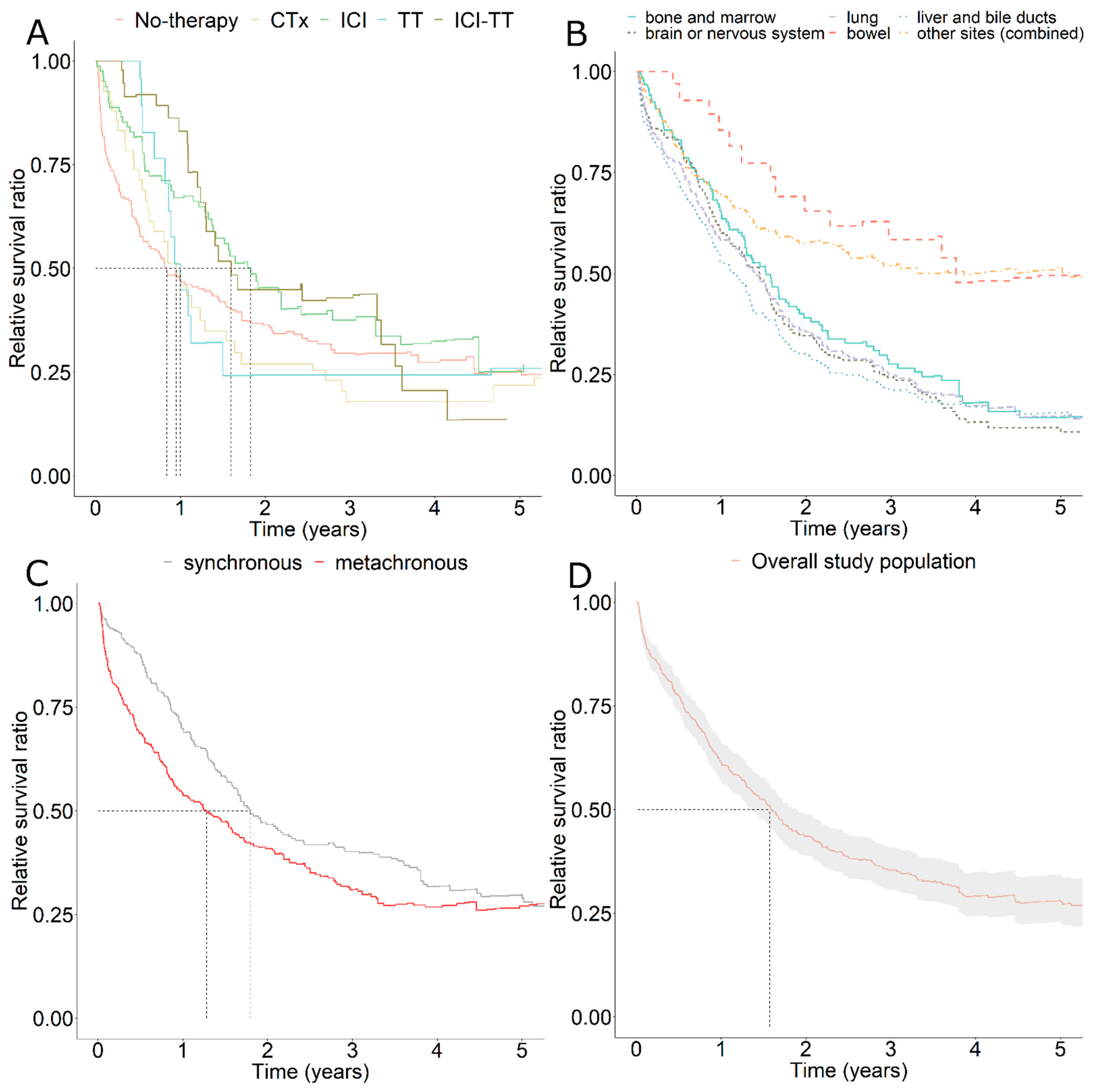
3.2. Relative Survival
3.3. Cox Regression Analysis
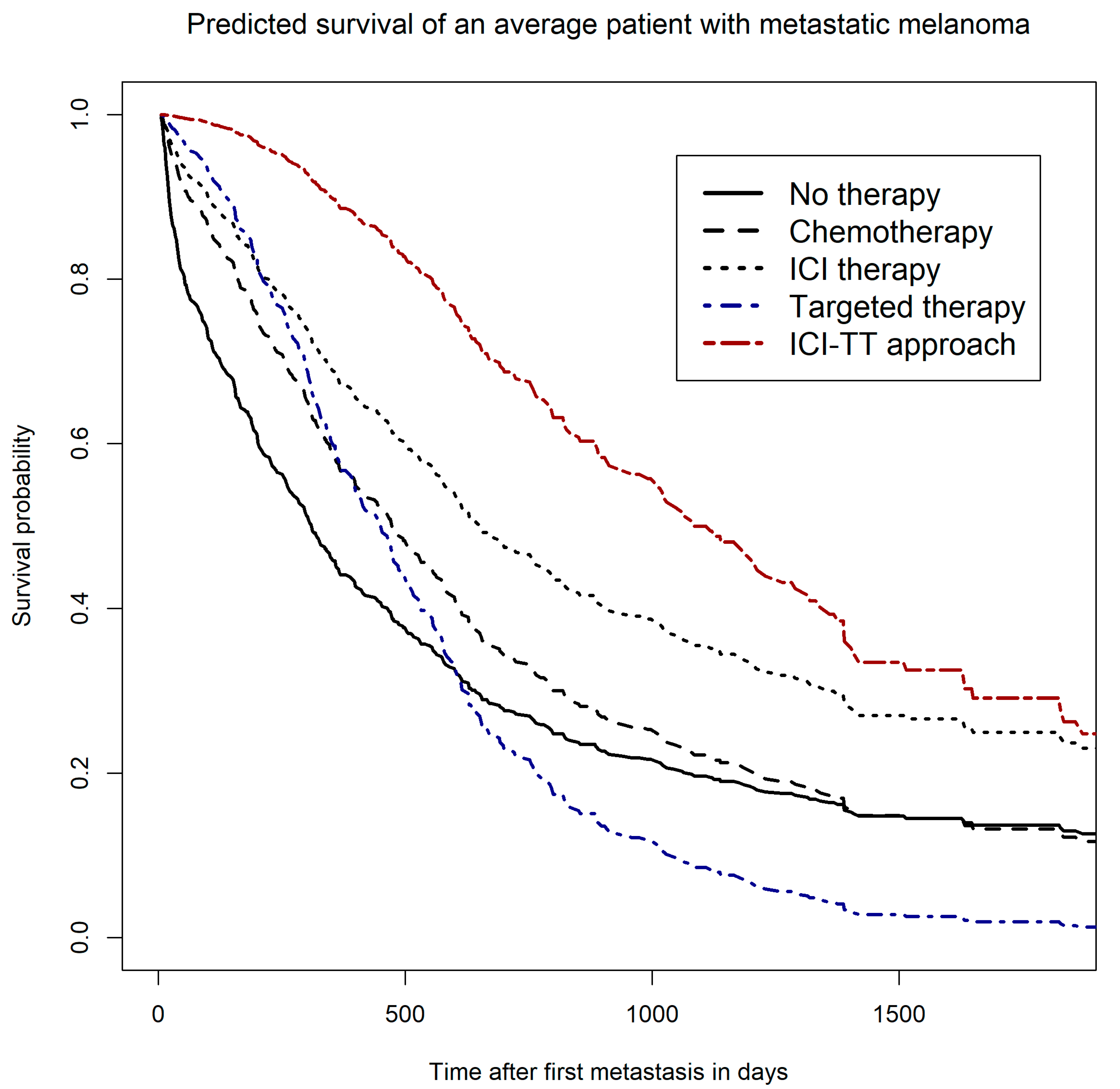
3.4. Survivor Functions—Predicted Survival of a Hypothetical Average Patient
4. Discussion
4.1. Implementation of Novel Therapies in Routine Care
4.2. Effectiveness of Novel Therapies in Routine Care
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schwabe, U.; Paffrath, D.; Ludwig, W.-D.; Klauber, J. (Eds.) Arzneiverordnungs-Report 2019: Akutelle Daten, Kosten, Trends und Kommentare; Springer: Berlin/Heidelberg, Germany, 2019; p. 1, Online-Ressource (XV, 1134 Seiten). [Google Scholar]
- Hübner, J.; Hübner, F.; Terheyden, P.; Katalinic, A. Trendwende bei der Hautkrebsmortalität. Der Hautarzt 2019, 70, 989–992. [Google Scholar] [CrossRef] [PubMed]
- McArthur, G.A.; Chapman, P.B.; Robert, C.; Larkin, J.; Haanen, J.B.; Dummer, R.; Ribas, A.; Hogg, D.; Hamid, O.; Ascierto, P.A.; et al. Safety and efficacy of vemurafenib in BRAFV600E and BRAFV600K mutation-positive melanoma (BRIM-3): Extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol. 2014, 15, 323–332. [Google Scholar] [CrossRef] [Green Version]
- Hauschild, A.; Grob, J.-J.; Demidov, L.V.; Jouary, T.; Gutzmer, R.; Millward, M.; Rutkowski, P.; Blank, C.U.; Miller, W.H.; Kaempgen, E.; et al. Dabrafenib in BRAF-mutated metastatic melanoma: A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2012, 380, 358–365. [Google Scholar] [CrossRef]
- Terheyden, P.; Krackhardt, A.; Eigentler, T. The Systemic Treatment of Melanoma: The Place of Immune Checkpoint Inhibitors and the Suppression of Intracellular Signal Transduction. Dtsch. Aerzteblatt Online 2019, 116, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Daud, A.; Gill, J.; Kamra, S.; Chen, L.; Ahuja, A. Indirect treatment comparison of dabrafenib plus trametinib versus vemurafenib plus cobimetinib in previously untreated metastatic melanoma patients. J. Hematol. Oncol. 2017, 10, 3. [Google Scholar] [CrossRef] [Green Version]
- Hellmund, P.; Schmitt, J.; Roessler, M.; Meier, F.; Schoffer, O. Targeted and Checkpoint Inhibitor Therapy of Metastatic Malignant Melanoma in Germany, 2000–2016. Cancers 2020, 12, 2354. [Google Scholar] [CrossRef] [PubMed]
- Ugurel, S.; Röhmel, J.; Ascierto, P.A.; Becker, J.C.; Flaherty, K.T.; Grob, J.J.; Hauschild, A.; Larkin, J.; Livingstone, E.; Long, G.; et al. Survival of patients with advanced metastatic melanoma: The impact of MAP kinase pathway inhibition and immune checkpoint inhibition—Update 2019. Eur. J. Cancer 2020, 130, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Ugurel, S.; Röhmel, J.; Ascierto, P.A.; Flaherty, K.T.; Grob, J.J.; Hauschild, A.; Larkin, J.; Long, G.; Lorigan, P.; McArthur, G.A.; et al. Survival of patients with advanced metastatic melanoma: The impact of novel therapies—Update 2017. Eur. J. Cancer 2017, 83, 247–257. [Google Scholar] [CrossRef] [Green Version]
- Trautmann, F.; Schuler, M.; Schmitt, J. Burden of soft-tissue and bone sarcoma in routine care: Estimation of incidence, prevalence and survival for health services research. Cancer Epidemiol. 2015, 39, 440–446. [Google Scholar] [CrossRef]
- Swart, E.; Gothe, H.; Geyer, S.; Jaunzeme, J.; Maier, B.; Grobe, T.G.; Ihle, P. Good Practice of Secondary Data Analysis (GPS): Guidelines and recommendations. Gesundheitswesen 2015, 77, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Perme, M.; Pavlič, K. Nonparametric Relative Survival Analysis with the R Package relsurv. J. Stat. Softw. 2018, 87. [Google Scholar] [CrossRef] [Green Version]
- Cox, D.R. Regression Models and Life-Tables. J. R. Stat. Soc. Ser. B Methodol. 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Garland, A.; Fransoo, R.; Olafson, K.; Ramsey, C.; Yogendran, M.; Château, D. The Epidemiology and Outcomes of Critical Illness in Manitoba; Manitoba Centre for Health Policy: Winnipeg, MB, Canada, 2012. [Google Scholar]
- Datzmann, T.; Schoffer, O.; Meier, F.; Seidler, A.; Schmitt, J. Are patients benefiting from participation in the German skin cancer screening programme? A large cohort study based on administrative data. Br. J. Dermatol 2021. [Google Scholar] [CrossRef] [PubMed]
- Shrank, W.H.; Patrick, A.R.; Brookhart, M.A. Healthy user and related biases in observational studies of preventive interventions: A primer for physicians. J. Gen. Intern. Med. 2011, 26, 546–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agresti, A. An Introduction to Categorical Data Analysis, 3rd ed.; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Gellrich, F.F.; Schmitz, M.; Beissert, S.; Meier, F. Anti-PD-1 and Novel Combinations in the Treatment of Melanoma-An Update. J. Clin. Med. 2020, 9, 223. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Ferrucci, P.F.; Fisher, R.; Del Vecchio, M.; Atkinson, V.; Schmidt, H.; Schachter, J.; Queirolo, P.; Long, G.V.; Di Giacomo, A.M.; et al. Dabrafenib, trametinib and pembrolizumab or placebo in BRAF-mutant melanoma. Nat. Med. 2019, 25, 941–946. [Google Scholar] [CrossRef] [PubMed]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef]
- Gutzmer, R.; Stroyakovskiy, D.; Gogas, H.; Robert, C.; Lewis, K.; Protsenko, S.; Pereira, R.P.; Eigentler, T.; Rutkowski, P.; Demidov, L.; et al. Atezolizumab, vemurafenib, and cobimetinib as first-line treatment for unresectable advanced BRAF(V600) mutation-positive melanoma (IMspire150): Primary analysis of the randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2020, 395, 1835–1844. [Google Scholar] [CrossRef]
- Tagliaferri, L.; Lancellotta, V.; Fionda, B.; Mangoni, M.; Casà, C.; Di Stefani, A.; Pagliara, M.M.; D’Aviero, A.; Schinzari, G.; Chiesa, S.; et al. Immunotherapy and radiotherapy in melanoma: A multidisciplinary comprehensive review. Hum. Vaccin. Immunother 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.M.; Kabarriti, R.; Brodin, N.P.; Ohri, N.; Guha, C.; Kalnicki, S.; Garg, M. Stereotactic radiosurgery with immunotherapy is associated with improved overall survival in patients with metastatic melanoma or non-small cell lung cancer: A National Cancer Database analysis. Clin. Transl. Oncol. 2021. [Google Scholar] [CrossRef]
- Long, G.V. Anti-PD 1 Brain Collaboration + Radiotherapy Extension (ABC-X Study) (ABC-X). Available online: https://clinicaltrials.gov/ct2/show/NCT03340129 (accessed on 30 November 2021).
- Sahgal, A.; Petrella, T. Concurrent Dabrafenib + Trametinib With Sterotactic Radiation in BRAF Mutation-Positive Malignant Melanoma and Brain Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT02974803 (accessed on 30 November 2021).
- Meier, F. Vemurafenib Plus Cobimetinib After Radiosurgery in Patients With BRAF-mutant Melanoma Brain Metastases (RadioCoBRIM). Available online: https://clinicaltrials.gov/ct2/show/NCT03430947 (accessed on 30 November 2021).
- Riihimäki, M.; Thomsen, H.; Hemminki, A.; Sundquist, K.; Hemminki, K. Comparison of survival of patients with metastases from known versus unknown primaries: Survival in metastatic cancer. BMC Cancer 2013, 13, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swart, E.; Schmitt, J. STandardized Reporting Of Secondary data Analyses (STROSA)—A recommendation. Z. Evid. Fortbild. Qual. Gesundhwes 2014, 108, 511–516. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Main Analysis | Sensitivity Analysis | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Population | Overall Sample | Bone C79.5 * | Brain C79.3 and C79.4 * | Liver C78.7 * | Lung C78.0 * | Locoregional Metastasis | ||||||
| n per group | 463 | 110 | 150 | 170 | 220 | 588 | ||||||
| Predictor | n | (Q1; Q3)/% | n | (Q1; Q3)/% | n | (Q1; Q3)/% | n | (Q1; Q3)/% | n | (Q1; Q3)/% | n | (Q1; Q3)/% |
| Median age at first metastasis | 75 | (64; 82) | 70 | (56; 80) | 71 | (57; 80) | 73 | (62; 80) | 74 | (64; 81) | 74 | (63; 82) |
| Sex | ||||||||||||
| Female | 209 | 45.1 | 48 | 43.6 | 57 | 38.0 | 71 | 41.8 | 93 | 42.3 | 270 | 45.9 |
| Male | 254 | 54.9 | 62 | 56.4 | 93 | 62.0 | 99 | 58.2 | 127 | 57.7 | 318 | 54.1 |
| Type of systemic therapy | ||||||||||||
| No systemic therapy | 161 | 34.8 | 28 | 25.5 | 40 | 26.7 | 37 | 21.8 | 49 | 22.3 | 223 | 37.9 |
| Chemotherapy | 125 | 27.0 | 38 | 34.5 | 48 | 32.0 | 63 | 37.1 | 79 | 35.9 | 145 | 24.7 |
| Chemotherapy exclusive | 39 | 8.4 | 5 | 4.5 | 8 | 5.3 | 19 | 11.2 | 25 | 11.4 | 45 | 7.7 |
| Interferon therapy | 79 | 17.1 | 21 | 19.1 | 30 | 20.0 | 30 | 17.6 | 42 | 19.1 | 107 | 18.2 |
| Interferon therapy exclusive | 28 | 6.0 | 2 | 1.8 | 5 | 3.3 | 5 | 2.9 | 8 | 3.6 | 46 | 7.8 |
| Immune checkpoint inhibitor therapy (ICI) | 203 | 43.8 | 67 | 60.9 | 76 | 50.7 | 94 | 55.3 | 122 | 55.5 | 237 | 40.3 |
| ICI exclusive | 75 | 16.2 | 19 | 17.3 | 20 | 13.3 | 29 | 17.1 | 42 | 19.1 | 87 | 14.8 |
| Targeted therapy (TT) | 79 | 17.1 | 26 | 23.6 | 46 | 30.7 | 41 | 24.1 | 45 | 20.5 | 85 | 14.5 |
| TT exclusive | 16 | 3.5 | 4 | 3.6 | 9 | 6.0 | 8 | 4.7 | 8 | 3.6 | 20 | 3.4 |
| ICI + TT sequential | 50 | 10.8 | 18 | 16.4 | 27 | 18.0 | 27 | 15.9 | 30 | 13.6 | 51 | 8.7 |
| ICI + TT exclusive | 31 | 6.7 | 11 | 10.0 | 17 | 11.3 | 16 | 9.4 | 18 | 8.2 | 31 | 5.3 |
| Localization of distant metastases (multiple localizations per patient are counted) | ||||||||||||
| C78 | 300 | 64.8 | 79 | 71.8 | 110 | 73.3 | 170 | 100.0 | 220 | 100.0 | 300 | 51.0 |
| C79 | 377 | 81.4 | 110 | 100.0 | 150 | 100.0 | 123 | 72.4 | 179 | 81.4 | 377 | 64.1 |
| Lung C78.0 * | 220 | 47.5 | 68 | 61.8 | 92 | 61.3 | 102 | 60.0 | 220 | 100.0 | 220 | 37.4 |
| Brain or nervous system C79.3 C79.4 * | 150 | 32.4 | 46 | 41.8 | 150 | 100.0 | 59 | 34.7 | 92 | 41.8 | 150 | 25.5 |
| Bowel C78.4 C78.5 * | 23 | 5.0 | 12 | 10.9 | 11 | 7.3 | 14 | 8.2 | 16 | 7.3 | 23 | 3.9 |
| Liver and bile ducts C78.7 * | 170 | 36.7 | 58 | 52.7 | 59 | 39.3 | 170 | 100.0 | 102 | 46.4 | 171 | 29.1 |
| Bone and marrow C79.5 * | 110 | 23.8 | 110 | 100.0 | 46 | 30.7 | 58 | 34.1 | 68 | 30.9 | 110 | 18.7 |
| Other sites (combined) | 182 | 39.3 | 110 | 100.0 | 2 | 1.3 | 37 | 21.8 | 54 | 24.5 | 182 | 31.0 |
| Number of patients with multiple localizations | 248 | 53.6 | 88 | 80.0 | 119 | 79.3 | 141 | 82.9 | 197 | 89.5 | 248 | 42.2 |
| Metastasis timing | ||||||||||||
| Synchronous | 215 | 46.4 | 56 | 50.9 | 78 | 52.0 | 89 | 52.4 | 107 | 48.6 | 287 | 48.8 |
| Metachronous | 248 | 53.6 | 54 | 49.1 | 72 | 48.0 | 81 | 47.6 | 113 | 51.4 | 301 | 51.2 |
| Other | ||||||||||||
| Resection of primary tumor | 417 | 90.1 | 100 | 90.9 | 136 | 90.7 | 147 | 86.5 | 193 | 87.7 | 534 | 90.8 |
| Influenza vaccination prior diagnosis | 280 | 60.5 | 60 | 54.5 | 77 | 51.3 | 96 | 56.5 | 131 | 59.5 | 366 | 62.2 |
| Years | ||||
|---|---|---|---|---|
| 2012–2014 | 2015–2017 | 2018–2020 | ||
| Number of patients in therapy | CTx | 56 | 97 | 81 |
| IFN | 92 | 90 | 18 | |
| ICI | 36 | 157 | 282 | |
| TT | 31 | 46 | 43 | |
| Main Analysis | Sensitivity Analysis s | ||||
|---|---|---|---|---|---|
| Number of Included Persons | N = 463 | N = 588 | |||
| Hazard Ratio (95%-CI) (Multivariable +, Time-Constant Effects, Time-Dependent Effects) | Hazard Ratio (95%-CI) (Multivariable +, Time-Constant Effects, Time-Dependent Effects) | ||||
| Hazard Ratio (95%-CI) (Multivariable +, Time-Constant Effects) | |||||
| Hazard Ratio (95%-CI) (Univariable) | |||||
| Predictor | Reference | ||||
| Age at metastasis (49–75 yrs) | 23–49 yrs | 1.582 (0.965; 2.594) | 1.680 (0.951; 2.970) | 1.802 (1.008; 3.223) | 1.993 (1.118; 3.550) |
| Age at metastasis (75–100 yrs) | 23–49 yrs | 2.589 (1.592; 4.210) | 2.555 (1.344; 4.858) | 2.645 (1.375; 5.087) | 3.019 (1.585; 5.752) |
| Female sex | Male sex | 0.872 (0.703; 1.081) | 0.960 (0.745; 1.238) | 0.947 (0.734; 1.222) | 0.945 (0.742; 1.204) |
| Metachronous Metastasis | Synchronous M. | 1.335 (1.077; 1.655) | 1.160 (0.897; 1.500) | 1.207 (0.932; 1.562) | 1.253 (0.987; 1.590) |
| Type of systemic therapy | |||||
| Chemotherapy (CTx) | No chemotherapy | 1.077 (0.852; 1.362) | 0.921 (0.705; 1.204) | 0.146 (0.041; 0.517) | 0.160 (0.047; 0.542) |
| Interaction chemotherapy with time since metastasis | - | - | - | 1.382 (1.114; 1.715) | 1.365 (1.110; 1.678) |
| Interferon therapy | No Interferon | 0.502 (0.369; 0.682) | 0.751 (0.530; 1.065) | 0.874 (0.176; 4.328) | 1.144 (0.252; 5.200) |
| Interaction interferon therapy with time since metastasis | - | - | - | 0.958 (0.736; 1.247) | 0.890 (0.694; 1.143) |
| Targeted therapy (TT) | No TT | 0.934 (0.710; 1.228) | 0.990 (0.621; 1.578) | 0.010 (0.001; 0.081) | 0.018 (0.003; 0.123) |
| Interaction targeted therapy with time since metastasis | - | - | - | 2.310 (1.629; 3.275) | 2.132 (1.543; 2.947) |
| Immune checkpoint inhibitor therapy (ICI) | No ICI | 0.706 (0.567; 0.877) | 0.559 (0.412; 0.757) | 0.113 (0.035; 0.368) | 0.092 (0.029; 0.294) |
| Interaction ICI with time since metastasis | - | - | - | 1.351 (1.097; 1.665) | 1.420 (1.162; 1.737) |
| Interaction ICI with TT | - | 0.789 (0.560; 1.110) | 0.705 (0.378; 1.313) | 0.394 (0.201; 0.775) | 0.356 (0.184; 0.688) |
| Localization of distant metastases * | |||||
| Lung C78.0 | No lung | 1.609 (1.296; 1.997) | 1.207 (0.838; 1.739) | 1.311 (0.909; 1.891) | 1.692 (1.190; 2.406) |
| Brain or nervous system C79.3 C79.4 | No brain | 1.442 (1.158; 1.795) | 1.174 (0.824; 1.672) | 1.182 (0.833; 1.676) | 1.755 (1.280; 2.406) |
| Bowel C78.4 C78.5 | no bowel | 0.511 (0.294; 0.891) | 0.438 (0.241; 0.795) | 0.431 (0.235; 0.788) | 0.425 (0.230; 0.785) |
| Liver and bile ducts C78.7 | no liver | 1.673 (1.348; 2.077) | 1.558 (1.156; 2.101) | 1.525 (1.131; 2.058) | 1.917 (1.434; 2.562) |
| Bone and marrow C79.5 | no bone | 1.200 (0.943; 1.527) | 1.030 (0.754; 1.406) | 1.069 (0.782; 1.460) | 1.383 (1.034; 1.849) |
| Other sites (combined) | no lung/brain/bowel/liver/bone | 0.515 (0.408; 0.651) | 0.607 (0.412; 0.894) | 0.650 (0.442; 0.956) | 1.045 (0.758; 1.441) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Datzmann, T.; Schmitt, J.; Fuhrmann, S.; Roessler, M.; Meier, F.; Schoffer, O. Implementation and Effectiveness of Novel Therapeutic Substances for Advanced Malignant Melanoma in Saxony, Germany, 2010–2020—Cohort Study Based on Administrative Data. Cancers 2021, 13, 6150. https://doi.org/10.3390/cancers13246150
Datzmann T, Schmitt J, Fuhrmann S, Roessler M, Meier F, Schoffer O. Implementation and Effectiveness of Novel Therapeutic Substances for Advanced Malignant Melanoma in Saxony, Germany, 2010–2020—Cohort Study Based on Administrative Data. Cancers. 2021; 13(24):6150. https://doi.org/10.3390/cancers13246150
Chicago/Turabian StyleDatzmann, Thomas, Jochen Schmitt, Saskia Fuhrmann, Martin Roessler, Friedegund Meier, and Olaf Schoffer. 2021. "Implementation and Effectiveness of Novel Therapeutic Substances for Advanced Malignant Melanoma in Saxony, Germany, 2010–2020—Cohort Study Based on Administrative Data" Cancers 13, no. 24: 6150. https://doi.org/10.3390/cancers13246150