High Throughput Molecular Characterization of Normal Karyotype Acute Myeloid Leukemia in the Context of the Prospective Trial 02/06 of the Northern Italy Leukemia Group (NILG)

 , , , , , and add
Show full author list
, , , , , and add
Show full author list
Abstract
:1. Introduction
2. Results
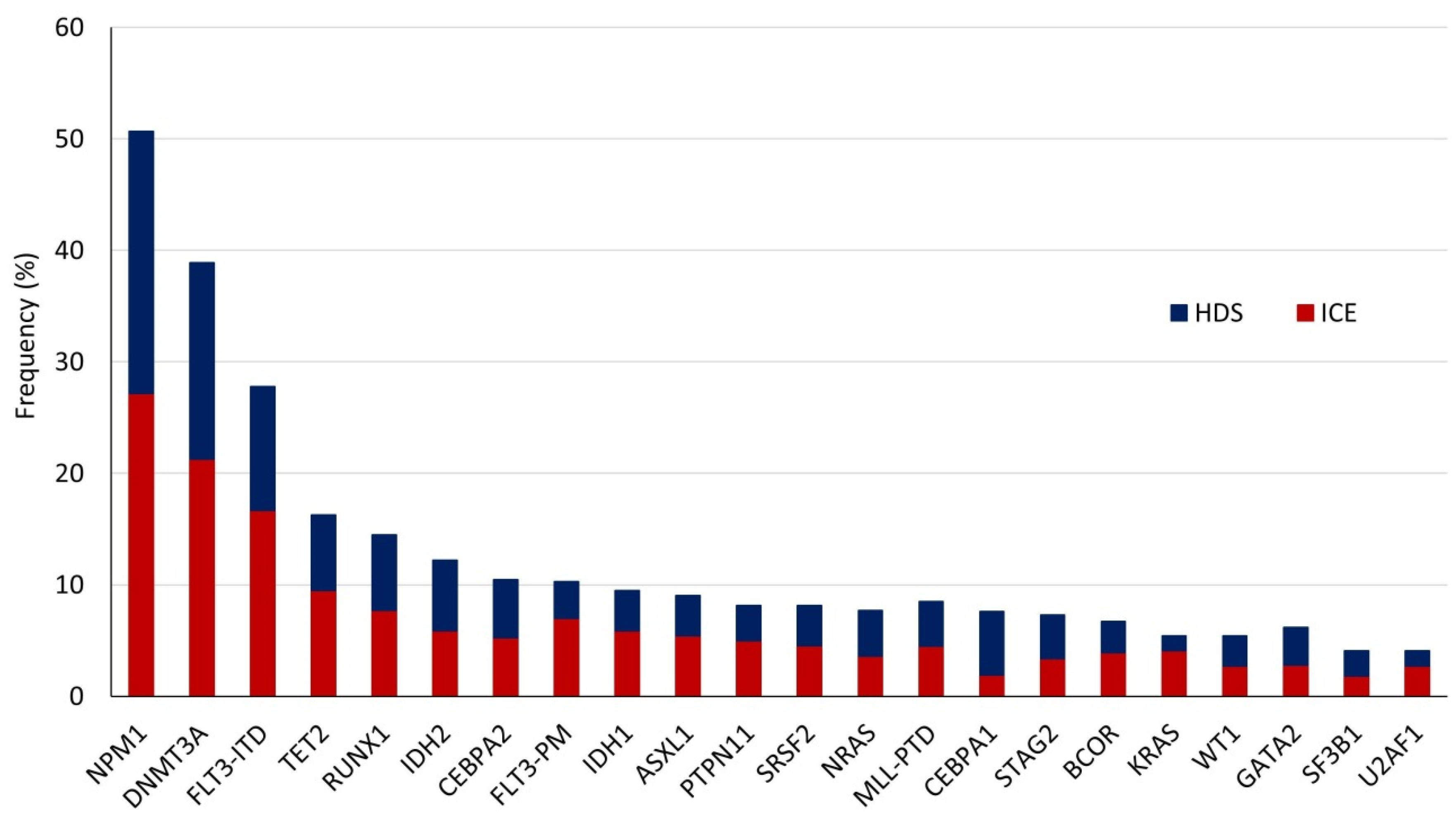
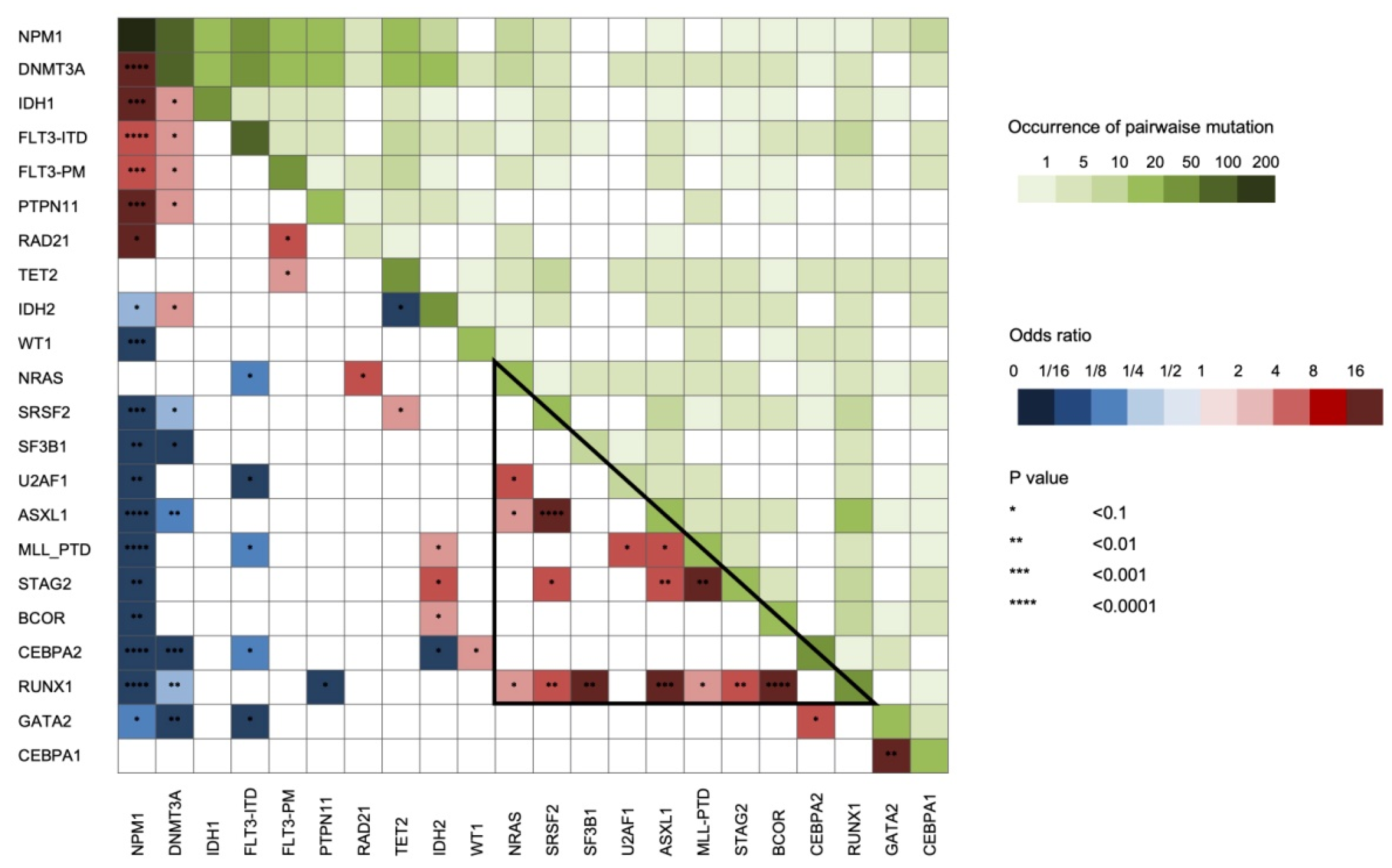
2.1. Clinical and Molecular Findings
2.2. Impact of Clinical and Molecular Profiling on CR Achievement
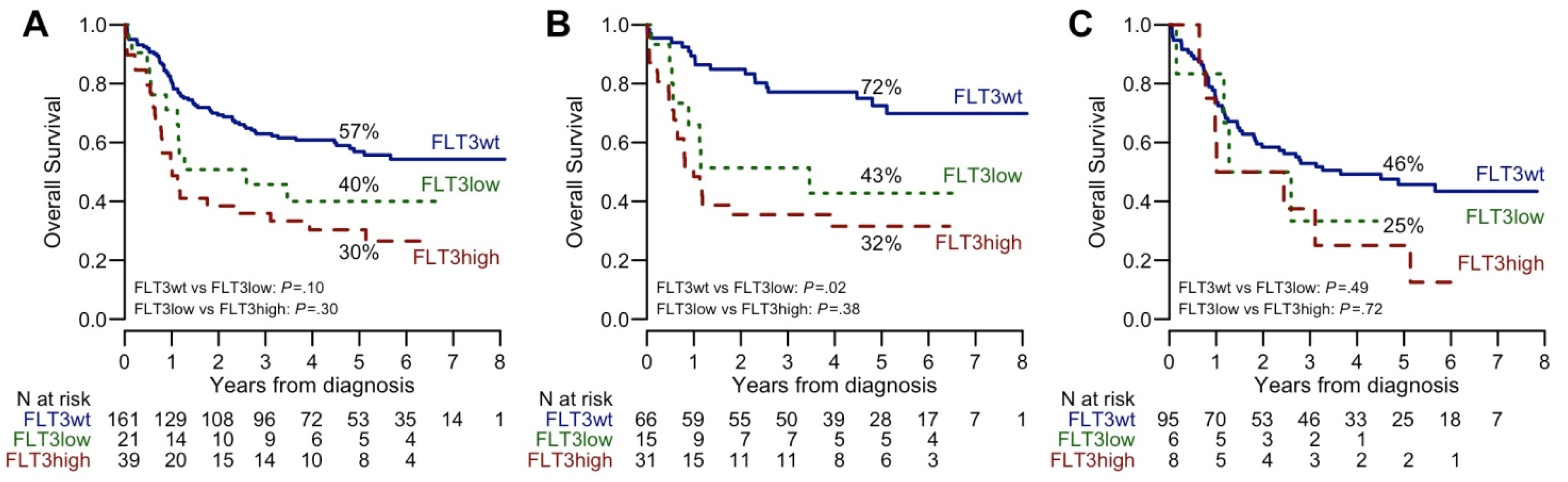
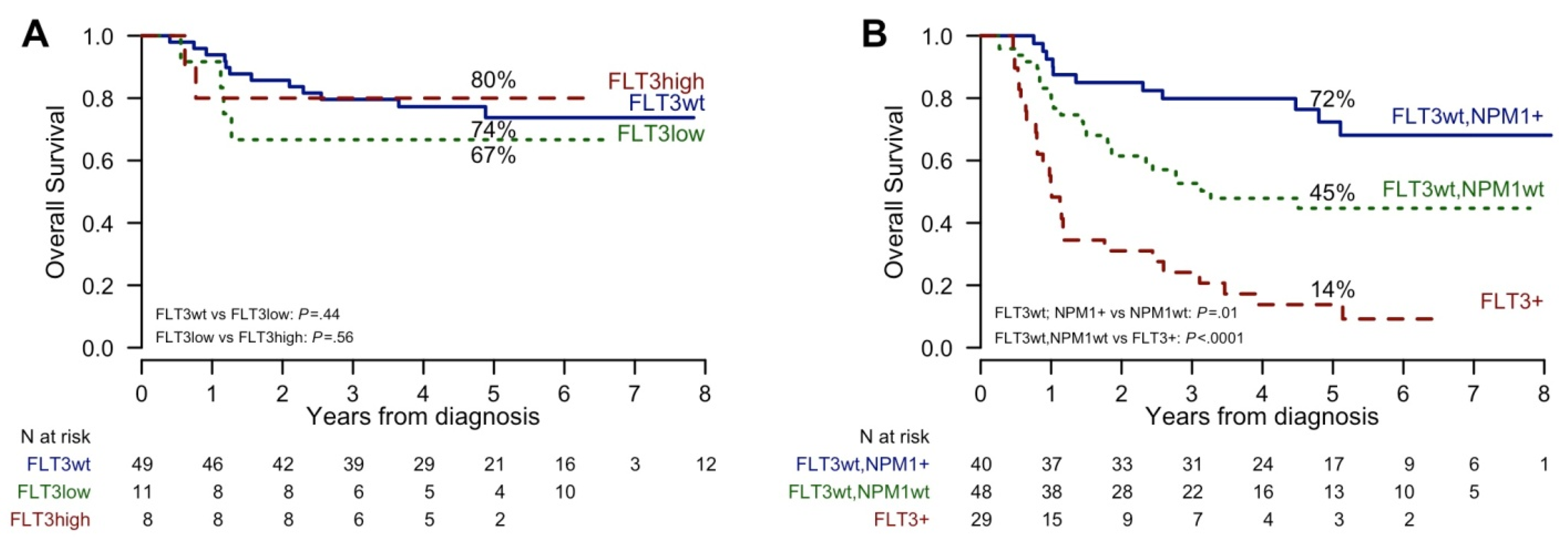
2.3. Impact of Clinical and Molecular Characteristics on Survival
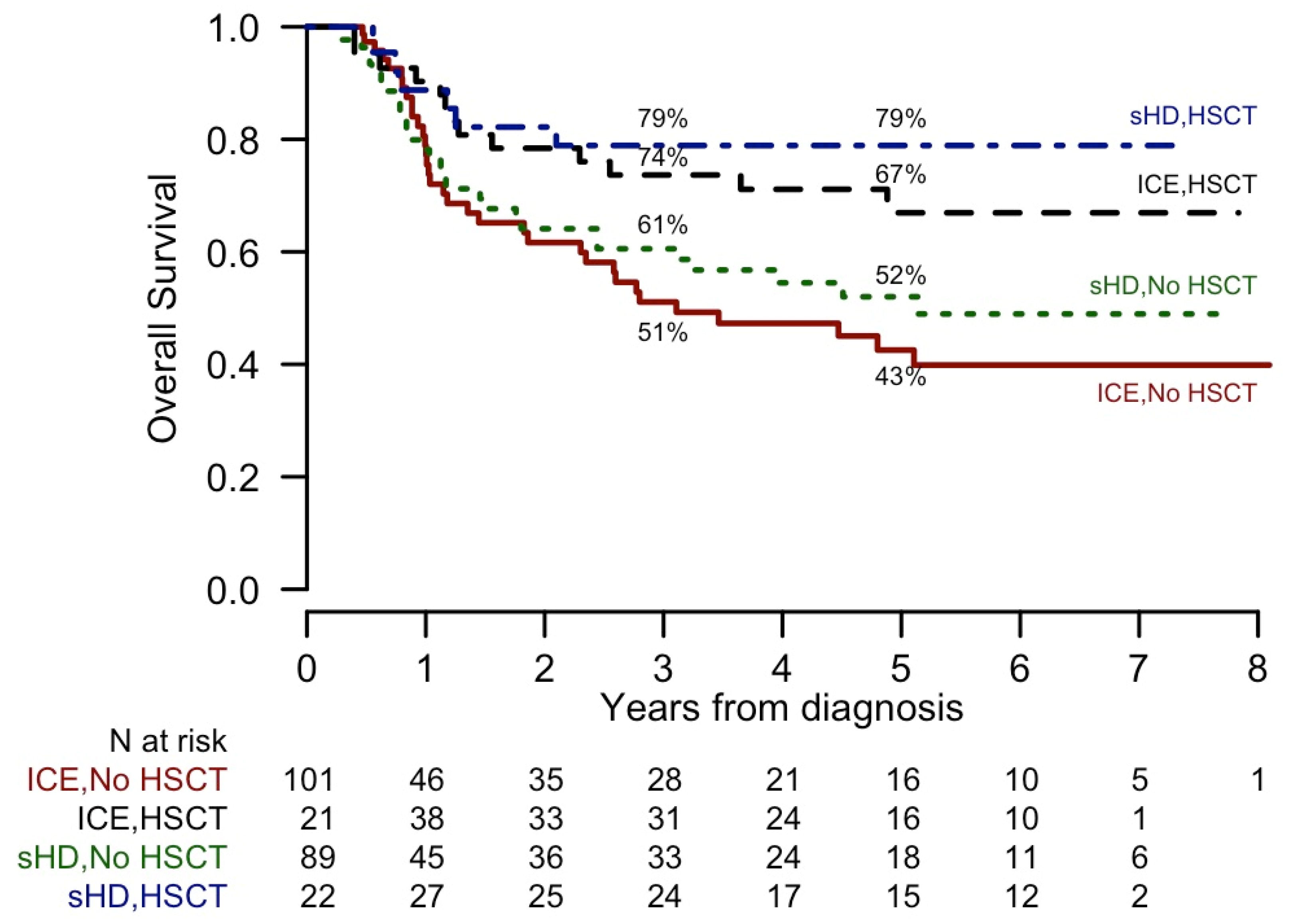
2.4. Impact of alloHSCT by Molecular Lesions
3. Discussion
4. Patients and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, J.P.; Gonen, M.; Figueroa, M.E.; Fernández, H.; Sun, Z.; Racevskis, J.; Van Vlierberghe, P.; Dolgalev, I.; Thomas, S.; Aminova, O.; et al. Prognostic Relevance of Integrated Genetic Profiling in Acute Myeloid Leukemia. N. Engl. J. Med. 2012, 366, 1079–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef] [PubMed]
- Heath, E.M.; Chan, S.M.; Minden, M.D.; Murphy, T.; Shlush, L.I.; Schimmer, A.D. Biological and clinical consequences of NPM1 mutations in AML. Leukemia 2017, 31, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Thiede, C.; Creutzig, E.; Reinhardt, D.; Ehninger, G.; Creutzig, U. Different types of NPM1 mutations in children and adults: Evidence for an effect of patient age on the prevalence of the TCTG-tandem duplication in NPM1-exon 12. Leukemia 2006, 21, 366–367. [Google Scholar] [CrossRef] [Green Version]
- Patnaik, M.S. The importance ofFLT3mutational analysis in acute myeloid leukemia. Leuk. Lymphoma 2017, 59, 2273–2286. [Google Scholar] [CrossRef] [Green Version]
- Döhner, K.; Schlenk, R.F.; Habdank, M.; Scholl, C.; Rücker, F.G.; Corbacioglu, A.; Bullinger, L.; Fröhling, S.; Döhner, H. Mutant nucleophosmin (NPM1) predicts favorable prognosis in younger adults with acute myeloid leukemia and normal cytogenetics: Interaction with other gene mutations. Blood 2005, 106, 3740–3746. [Google Scholar] [CrossRef] [Green Version]
- Fröhling, S.; Schlenk, R.F.; Breitruck, J.; Benner, A.; Kreitmeier, S.; Tobis, K.; Döhner, H.; Döhner, K. Prognostic significance of activating FLT3 mutations in younger adults (16 to 60 years) with acute myeloid leukemia and normal cytogenetics: A study of the AML Study Group Ulm. Blood 2002, 100, 4372–4380. [Google Scholar] [CrossRef] [Green Version]
- Sakaguchi, M.; Yamaguchi, H.; Najima, Y.; Usuki, K.; Ueki, T.; Oh, I.; Mori, S.; Kawata, E.; Uoshima, N.; Kobayashi, Y.; et al. Prognostic impact of low allelic ratio FLT3-ITD and NPM1 mutation in acute myeloid leukemia. Blood Adv. 2018, 2, 2744–2754. [Google Scholar] [CrossRef] [Green Version]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Saultz, J.N.; Garzon, R. Acute Myeloid Leukemia: A Concise Review. J. Clin. Med. 2016, 5, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassan, R.; Intermesoli, T.; Masciulli, A.; Pavoni, C.; Boschini, C.; Gianfaldoni, G.; Marmont, F.; Cavattoni, I.; Mattei, D.; Terruzzi, E.; et al. Randomized trial comparing standard vs sequential high-dose chemotherapy for inducing early CR in adult AML. Blood Adv. 2019, 3, 1103–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falini, B.; Spinelli, O.; Meggendorfer, M.; Martelli, M.P.; Bigerna, B.; Ascani, S.; Stein, H.; Rambaldi, A.; Haferlach, T. IDH1-R132 changes vary according to NPM1 and other mutations status in AML. Leukemia 2019, 33, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Meggendorfer, M.; Cappelli, L.V.; Walter, W.; Haferlach, C.; Kern, W.; Falini, B.; Haferlach, T. IDH1R132, IDH2R140 and IDH2R172 in AML: Different genetic landscapes correlate with outcome and may influence targeted treatment strategies. Leukemia 2018, 32, 1249–1253. [Google Scholar] [CrossRef]
- Gaidzik, V.I.; Bullinger, L.; Schlenk, R.F.; Zimmermann, A.S.; Röck, J.; Paschka, P.; Corbacioglu, A.; Krauter, J.; Schlegelberger, B.; Ganser, A.; et al. RUNX1 Mutations in Acute Myeloid Leukemia: Results From a Comprehensive Genetic and Clinical Analysis From the AML Study Group. J. Clin. Oncol. 2011, 29, 1364–1372. [Google Scholar] [CrossRef]
- Grossmann, V.; Tiacci, E.; Holmes, A.B.; Kohlmann, A.; Martelli, M.P.; Kern, W.; Spanhol-Rosseto, A.; Klein, H.-U.; Dugas, M.; Schindela, S.; et al. Whole-exome sequencing identifies somatic mutations of BCOR in acute myeloid leukemia with normal karyotype. Blood 2011, 118, 6153–6163. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.S.; Pinkus, G.S.; Ritterhouse, L.L.; Segal, J.P.; Cin, P.D.; Restrepo, T.; Harris, M.H.; Stone, R.M.; Hasserjian, R.P.; Weinberg, O.K. High NPM1 mutant allele burden at diagnosis correlates with minimal residual disease at first remission in de novo acute myeloid leukemia. Am. J. Hematol. 2019, 94, 921–928. [Google Scholar] [CrossRef]
- Harada, Y.; Nagata, Y.; Kihara, R.; Ishikawa, Y.; Asou, N.; Ohtake, S.; Miyawaki, S.; Sakura, T.; Ozawa, Y.; Usui, N.; et al. Prognostic analysis according to the 2017 ELN risk stratification by genetics in adult acute myeloid leukemia patients treated in the Japan Adult Leukemia Study Group (JALSG) AML201 study. Leuk. Res. 2018, 66, 20–27. [Google Scholar] [CrossRef]
- Stone, R.M.; Mandrekar, S.J.; Sanford, B.L.; Laumann, K.; Geyer, S.; Bloomfield, C.D.; Thiede, C.; Prior, T.W.; Döhner, K.; Marcucci, G.; et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N. Engl. J. Med. 2017, 377, 454–464. [Google Scholar] [CrossRef]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef]
- Cortes, J.; Khaled, S.; Martinelli, G.; Perl, A.E.; Ganguly, S.; Russell, N.; Krämer, A.; Dombret, H.; Hogge, D.; Jonas, B.A.; et al. Quizartinib versus salvage chemotherapy in relapsed or refractory FLT3-ITD acute myeloid leukaemia (QuANTUM-R): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 984–997. [Google Scholar] [CrossRef]
- Moarii, M.; Papaemmanuil, E. Classification and risk assessment in AML: Integrating cytogenetics and molecular profiling. Hematology 2017, 2017, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Gao, X.-N.; Yu, L. The prognostic impact of tet oncogene family member 2 mutations in patients with acute myeloid leukemia: A systematic-review and meta-analysis. BMC Cancer 2019, 19, 389. [Google Scholar] [CrossRef] [PubMed]
- Ohgami, R.S.; Ma, L.; Merker, J.D.; Gotlib, J.R.; Schrijver, I.; Zehnder, J.L.; Arber, D.A. Next-generation sequencing of acute myeloid leukemia identifies the significance of TP53, U2AF1, ASXL1, and TET2 mutations. Mod. Pathol. 2014, 28, 706–714. [Google Scholar] [CrossRef]
- Kanagal-Shamanna, R.; Loghavi, S.; Dinardo, C.D.; Medeiros, L.J.; Garcia-Manero, G.; Jabbour, E.; Routbort, M.J.; Luthra, R.; Bueso-Ramos, C.E.; Khoury, J.D. Bone marrow pathologic abnormalities in familial platelet disorder with propensity for myeloid malignancy and germline RUNX1 mutation. Haematology 2017, 102, 1661–1670. [Google Scholar] [CrossRef] [Green Version]
- Thiede, C.; Steudel, C.; Mohr, B.; Schaich, M.; Schäkel, U.; Platzbecker, U.; Wermke, M.; Bornhäuser, M.; Ritter, M.; Neubauer, A.; et al. Analysis of FLT3-activating mutations in 979 patients with acute myelogenous leukemia: Association with FAB subtypes and identification of subgroups with poor prognosis. Blood 2002, 99, 4326–4335. [Google Scholar] [CrossRef] [Green Version]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised Recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics and Mutations | All patients, N = 221 | ICE, N = 117 | sHD, N = 104 | p |
|---|---|---|---|---|
| Median age, at diagnosis (range) | 52.5 (19.8–74.8) | 54.4 (23.6–74.8) | 49.5 (19.8–72.2) | 0.0324 |
| ≤60 years | 166 (75.1) | 81 (69.2) | 85 (81.7) | 0.0319 |
| >60 years | 55 (24.9) | 36 (30.8) | 19 (18.3) | |
| Sex | 0.1765 | |||
| Female | 119 (53.8) | 58 (49.6) | 61 (58.7) | |
| Male | 102 (46.2) | 59 (50.4) | 43 (41.3) | |
| AML category | 0.0463 | |||
| Non de novo | 26 (11.8) | 9 (7.7) | 17 (16.3) | |
| De novo | 195 (88.2) | 108 (92.3) | 87 (83.7) | |
| ECOG PS | 0.4556 | |||
| 0-1 | 201 (91) | 108 (92.3) | 93 (89.4) | |
| 2-3 | 20 (9) | 9 (7.7) | 11 (10.6) | |
| Hepatomegaly | 17 (7.7) | 8 (6.8) | 9 (8.7) | 0.6130 |
| Splenomegaly | 20 (9) | 9 (7.7) | 11 (10.6) | 0.4556 |
| Extramedullary involvement | 34 (15.4) | 16 (13.7) | 18 (17.3) | 0.4550 |
| WBC count (×109/L) | 0.3677 | |||
| ≤50 | 155 (70.1) | 79 (67.5) | 76 (73.1) | |
| >50 | 66 (29.9) | 38 (32.5) | 28 (26.9) | |
| Hemoglobin (g/dL) | 9.5 (4.3–14.1) | 9.5 (5.1–14.1) | 9.5 (4.3–13.9) | 0.9144 |
| Platelets(×109/L) | 59 (5–815) | 64 (5–815) | 57.5 (8–513) | 0.8752 |
| Bone marrow blast cells, % | 80 (0–100) | 83 (10–100) | 80 (0–100) | 0.4519 |
| Peripheral blood blasts cells, % | 52 (0–100) | 50 (0–100) | 55.5 (0–100) | 0.6909 |
| Consolidation | 0.3276 | |||
| No alloHSCT | 119 (67.9) | 60 (59.4) | 59 (66.3) | |
| alloHSCT | 71 (32.1) | 41 (40.6) | 30 (33.7) | |
| FLT3 wt., NPM1 wt | 90/216 (41.7) | 42/112 (37.5) | 48/104 (46.2) | 0.1974 |
| FLT3-ITD low ratio, NPM1 wt | 6/221 (2.7) | 6/117 (5.1) | 0/104 (0) | 0.0307 |
| FLT3-ITD high ratio, NPM1 wt | 8/221 (3.6) | 4/117 (3.4) | 4/104 (3.8) | 1.0000 |
| FLT3 wt, NPM1 + | 66/221 (29.9) | 34/117 (29.1) | 32/104 (30.8) | 0.7817 |
| FLT3-ITD low ratio, NPM1 + | 15/221 (6.8) | 10/117 (8.5) | 5/104 (4.8) | 0.2700 |
| FLT3-ITD high ratio, NPM1 + | 31/221 (14) | 16/117 (13.7) | 15/104 (14.4) | 0.8730 |
| Patients Characteristics | CR | OS | DFS | |||
|---|---|---|---|---|---|---|
| HR | p | HR | p | HR | p | |
| HDS | 0.94 (0.44–2.03) | 0.8731 | 0.86 (0.59–1.26) | 0.4318 | 0.82 (0.54–1.23) | 0.3276 |
| HSCT | - | - | 0.31 (0.18–0.51) | 0.0000 | 0.29 (0.17–0.48) | <0.0001 |
| Age > 60 | 0.21 (0.09–0.45) | 0.0001 | 2.67 (1.81–3.95) | 0.0000 | 1.92 (1.22–3.02) | 0.0047 |
| Sex male | 1.67 (0.77–3.79) | 0.2019 | 0.95 (0.65–1.39) | 0.7982 | 1.06 (0.7–1.58) | 0.7901 |
| De novo | 2.62 (0.94–6.69) | 0.0503 | 0.73 (0.42–1.27) | 0.2665 | 0.76 (0.41–1.43) | 0.3975 |
| ECOG PS 2–3 | 0.25 (0.09–0.73) | 0.0076 | 2.24 (1.25–4.01) | 0.0065 | 1.06 (0.46–2.43) | 0.886 |
| WBC count > 50 | 0.74 (0.34–1.7) | 0.4621 | 1.61 (1.09–2.39) | 0.0179 | 1.37 (0.89–2.12) | 0.1533 |
| NPM1 | 1.76 (0.82–3.92) | 0.1541 | 0.71 (0.48–1.04) | 0.0780 | 0.76 (0.51–1.14) | 0.1864 |
| VAF ≤ 0.4 | 2.18 (0.87–6.27) | 0.1162 | 0.67 (0.42–1.05) | 0.0785 | 0.89 (0.57–1.39) | 0.6075 |
| VAF > 0.4 | 1.3 (0.5–3.81) | 0.6031 | 0.8 (0.48–1.33) | 0.3924 | 0.59 (0.33–1.08) | 0.0866 |
| FLT3-ITD | 0.79 (0.34–1.93) | 0.5811 | 2.23 (1.5–3.32) | 0.0001 | 2.18 (1.43–3.33) | 0.0003 |
| FLT3-ITD low | 0.95 (0.29–4.29) | 0.9380 | 1.67 (0.9–3.08) | 0.1032 | 1.55 (0.8–3.04) | 0.1966 |
| FLT3-ITD high | 0.87 (0.34–2.51) | 0.7813 | 2.43 (1.56–3.78) | 0.0001 | 2.6 (1.62–4.18) | 0.0001 |
| DNMT3A | 1.01 (0.47–2.25) | 0.9799 | 1.25 (0.85–1.83) | 0.2606 | 1.49 (0.99–2.23) | 0.0553 |
| TET2 | 0.23 (0.1–0.54) | 0.0006 | 1.38 (0.85–2.24) | 0.1926 | 0.94 (0.5–1.76) | 0.8357 |
| RUNX1 | 0.42 (0.17–1.08) | 0.0590 | 2.25 (1.43–3.55) | 0.0005 | 1.95 (1.15–3.3) | 0.0132 |
| IDH2 | 0.68 (0.25–2.17) | 0.4754 | 0.77 (0.4–1.47) | 0.4247 | 1.05 (0.56–1.97) | 0.8732 |
| CEBPA2 * | 3.37 (0.66–61.69) | 0.2450 | 0.26 (0.1–0.71) | 0.0088 | 0.21 (0.06–0.65) | 0.007 |
| FLT3_PM | 1.57 (0.42–10.17) | 0.5605 | 0.45 (0.2–1.04) | 0.0608 | 0.38 (0.16–0.94) | 0.0371 |
| IDH1 | 0.98 (0.3–4.36) | 0.9714 | 0.95 (0.51–1.78) | 0.8781 | 0.98 (0.51–1.89) | 0.9575 |
| ASXL1 | 0.25 (0.09–0.73) | 0.0076 | 1.54 (0.86–2.76) | 0.1434 | 1.3 (0.63–2.68) | 0.4827 |
| CEBPA1 * | 2.32 (0.44–42.85) | 0.4243 | 0.56 (0.23–1.39) | 0.2133 | 0.63 (0.25–1.55) | 0.3141 |
| PTPN11 | 2.95 (0.57–54.09) | 0.3022 | 0.46 (0.19–1.13) | 0.0908 | 0.58 (0.26–1.33) | 0.2018 |
| SRSF2 | 0.12 (0.04–0.34) | 0.0001 | 1.43 (0.77–2.67) | 0.2596 | 0.8 (0.29–2.17) | 0.6553 |
| NRAS | 0.74 (0.22–3.37) | 0.6557 | 1.46 (0.78–2.72) | 0.2387 | 1.31 (0.64–2.71) | 0.4607 |
| KMT2A-PTD | 2.42 (0.46–44.57) | 0.4027 | 1.34 (0.67–2.67) | 0.4037 | 1.44 (0.72–2.88) | 0.298 |
| STAG2 | 0.35 (0.1–1.36) | 0.0990 | 1.33 (0.61–2.88) | 0.4712 | 1.3 (0.52–3.23) | 0.5691 |
| BCOR | 1.95 (0.36–36.43) | 0.5310 | 1.58 (0.73–3.44) | 0.2456 | 1.52 (0.66–3.51) | 0.3258 |
| KRAS | 1.84 (0.34–34.31) | 0.5648 | 0.81 (0.33–2) | 0.6546 | 1.1 (0.48–2.52) | 0.8178 |
| WT1 | 1.84 (0.34–34.31) | 0.5648 | 0.8 (0.32–1.95) | 0.6185 | 0.75 (0.28–2.04) | 0.5736 |
| GATA2 | >99.99 (0–NA) | 0.9894 | 0 (0–Inf) | 0.9953 | 0 (0–Inf) | 0.9954 |
| SF3B1 | 1.32 (0.23–24.91) | 0.7976 | 1.42 (0.66–3.06) | 0.3689 | 1.8 (0.83–3.9) | 0.1348 |
| U2AF1 | 1.32 (0.23–24.91) | 0.7976 | 2.69 (1.3–5.55) | 0.0075 | 3.57 (1.64–7.74) | 0.0013 |
| FLT3wt, NPM1 wt | 0.58 (0.26–1.28) | 0.1744 | 1.12 (0.76–1.65) | 0.5682 | 1.08 (0.71–1.63) | 0.726 |
| FLT3-ITD low ratio, NPM1 wt | 0.81 (0.12–15.82) | 0.8505 | 1.55 (0.57–4.23) | 0.388 | 1.3 (0.41–4.1) | 0.6572 |
| FLT3-ITD high ratio, NPM1 wt | >99.99 (0–NA) | 0.9861 | 2.09 (0.97–4.49) | 0.0602 | 2.47 (1.14–5.34) | 0.0214 |
| FLT3wt, NPM1 + | 3.27 (1.21–11.42) | 0.0336 | 0.35 (0.21–0.59) | 0.0001 | 0.44 (0.27–0.71) | 0.0009 |
| FLT3-ITD low ratio, NPM1 + | 1.06 (0.28–7.03) | 0.9361 | 1.27 (0.62–2.62) | 0.5089 | 1.25 (0.58–2.7) | 0.5683 |
| FLT3-ITD high ratio, NPM1 + | 0.63 (0.25–1.83) | 0.3602 | 2.15 (1.33–3.47) | 0.0017 | 2.21 (1.31–3.75) | 0.0031 |
| Patients Characteristics | CR | OS | DFS | |||
|---|---|---|---|---|---|---|
| HR | p | HR | p | HR | p | |
| HSCT | - | - | 0.34 (0.19–0.60) | 0.0002 | 0.34 (0.19–0.60) | <0.0001 |
| Age > 60 | 0.43 (0.15–1.22) | 0.1049 | 1.37 (0.78–2.40) | 0.2661 | 0.89 (0.51–1.55) | 0.6864 |
| De novo | 2.17 (0.55–7.76) | 0.2460 | - | - | - | - |
| ECOG PS 2–3 | 0.26 (0.07–1) | 0.0398 | 1.09 (0.42–2.85) | 0.8559 | - | - |
| WBC count > 50 | - | - | 1.20 (0.67–2.14) | 0.5456 | 1.07 (0.63–1.82) | 0.8023 |
| NPM1 | 1.06 (0.33–3.3) | 0.9239 | 0.58 (0.32–1.06) | 0.0761 | 0.49 (0.28–0.88) | 0.0163 |
| FLT3-ITD | - | - | 2.76 (1.56–4.91) | 0.0005 | 2.81 (1.66–4.73) | 0.0001 |
| DNMT3A | - | - | - | - | 1.62 (0.95–2.77) | 0.0772 |
| TET2 | 0.4 (0.13–1.24) | 0.1048 | 0.74 (0.33–1.66) | 0.4715 | - | - |
| RUNX1 | 0.54 (0.15–2.03) | 0.3501 | 1.25 (0.60–2.61) | 0.5567 | 0.89 (0.43–1.87) | 0.7638 |
| CEBPA2 * | - | - | 0.20 (0.06–0.68) | 0.0097 | 0.17 (0.05–0.57) | 0.0040 |
| FLT3_PM | - | - | 0.65 (0.23–1.89) | 0.4325 | 0.65 (0.25–1.67) | 0.3731 |
| ASXL1 | 0.87 (0.19–4.63) | 0.8628 | 0.42 (0.16–1.08) | 0.0713 | - | - |
| PTPN11 | - | - | 0.60 (0.21–1.73) | 0.3450 | - | - |
| SRSF2 | 0.24 (0.06–0.95) | 0.0376 | - | - | - | - |
| STAG2 | 0.97 (0.18–6.65) | 0.9715 | - | - | - | - |
| SF3B1 | - | - | - | - | 1.02 (0.42–2.45) | 0.9663 |
| U2AF1 | - | - | 4.19 (1.72–10.23) | 0.0016 | 5.54 (2.25–13.66) | 0.0002 |
| Patients Characteristics | CR n = 90 | OS n = 90 | DFS n = 75 | |||
|---|---|---|---|---|---|---|
| HR | p | HR | p | HR | p | |
| HDS | 0.51 (0.15–1.59) | 0.2622 | 1.29 (0.72–2.32) | 0.3877 | 1.05 (0.56–1.98) | 0.8837 |
| HSCT | - | - | 0.43 (0.21–0.89) | 0.0229 | 0.42 (0.2–0.88) | 0.0225 |
| Age > 60 | 0.51 (0.16–1.69) | 0.2524 | 2.28 (1.26–4.15) | 0.0068 | 2.63 (1.35–5.11) | 0.0043 |
| Sex male | 2.38 (0.78–7.77) | 0.1336 | 0.63 (0.35–1.13) | 0.1194 | 0.86 (0.45–1.64) | 0.6537 |
| De novo | 2.38 (0.65–7.98) | 0.1657 | 0.63 (0.33–1.22) | 0.1729 | 0.58 (0.27–1.23) | 0.1569 |
| ECOG PS 2–3 | 1 (0.15–19.93) | 1.0000 | 2.66 (0.95–7.47) | 0.0635 | 2 (0.61–6.53) | 0.2504 |
| WBC count > 50 | 1.22 (0.19–23.93) | 0.8605 | 0.54 (0.13–2.24) | 0.3955 | 0.28 (0.04–2.03) | 0.2066 |
| DNMT3A | 0.48 (0.12–2.41) | 0.3219 | 2.77 (1.32–5.8) | 0.0068 | 3.83 (1.67–8.76) | 0.0015 |
| TET2 | 0.21 (0.05–0.81) | 0.0195 | 2.26 (1.09–4.71) | 0.0286 | 2.33 (0.9–5.99) | 0.0797 |
| RUNX1 | 0.41 (0.13–1.37) | 0.1323 | 2.36 (1.28–4.35) | 0.0060 | 1.96 (0.97–3.96) | 0.0608 |
| IDH2 | 0.52 (0.15–2.13) | 0.3297 | 1.03 (0.46–2.3) | 0.9439 | 1.56 (0.68–3.54) | 0.2909 |
| CEBPA2 * | 4.5 (0.81–84.34) | 0.1598 | 0.16 (0.05–0.53) | 0.0026 | 0.12 (0.03–0.5) | 0.0035 |
| ASXL1 | 0.27 (0.08–1.03) | 0.0466 | 1.26 (0.59–2.7) | 0.5564 | 1.12 (0.44–2.86) | 0.8194 |
| CEBPA1 * | >99.99 (0–NA) | 0.9934 | 0.45 (0.14–1.45) | 0.1801 | 0.72 (0.25–2.03) | 0.5315 |
| SRSF2 | 0.08 (0.02–0.31) | 0.0003 | 1.33 (0.59–2.98) | 0.4889 | 0.7 (0.17–2.93) | 0.6305 |
| NRAS | 0.57 (0.11–4.14) | 0.5123 | 2.88 (1.28–6.48) | 0.0105 | 2.9 (1.13–7.48) | 0.0272 |
| KMT2A-PTD | 3.5 (0.62–65.89) | 0.2437 | 1.05 (0.49–2.26) | 0.8960 | 1.22 (0.56–2.66) | 0.6168 |
| STAG2 | 0.79 (0.17–5.67) | 0.7783 | 1.16 (0.45–2.98) | 0.7603 | 1.57 (0.6–4.09) | 0.3593 |
| BCOR | >99.99 (0–NA) | 0.9908 | 1.31 (0.46–3.71) | 0.6128 | 1.36 (0.48–3.9) | 0.5639 |
| KRAS | >99.99 (0–NA) | 0.9914 | 0.61 (0.08–4.44) | 0.6276 | 0.6 (0.08–4.37) | 0.6138 |
| WT1 | >99.99 (0–NA) | 0.9903 | 0.58 (0.18–1.86) | 0.3584 | 0.6 (0.18–1.96) | 0.3983 |
| GATA2 | >99.99 (0–NA) | 0.9937 | 0 (0–Inf) | 0.9973 | 0 (0–99.99) | 0.9973 |
| SF3B1 | 1.44 (0.23–28.05) | 0.7417 | 1.4 (0.59–3.3) | 0.4479 | 1.77 (0.74–4.26) | 0.2010 |
| U2AF1 | 1.67 (0.27–32.28) | 0.6406 | 3.03 (1.4–6.58) | 0.0049 | 3.89 (1.69–8.93) | 0.0014 |
| Patients Characteristics | CR | OS | DFS | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| HSCT | - | - | 0.42 (0.16–1.09) | 0.0744 | 0.24 (0.09–0.62) | 0.0032 |
| Age > 60 | - | - | 1.02 (0.43–2.41) | 0.9624 | 1.12 (0.51–2.45) | 0.7778 |
| Sex male | 2.57 (0.66–11.53) | 0.1846 | 0.77 (0.33–1.78) | 0.5462 | - | - |
| De novo | 0.65 (0.11–2.96) | 0.5985 | 0.88 (0.36–2.16) | 0.7753 | 1.29 (0.50–3.33) | 0.5997 |
| ECOG PS 2–3 | - | - | 2.24 (0.54–9.31) | 0.2681 | - | - |
| DNMT3A | - | - | 2.58 (0.80–8.28) | 0.1105 | 3.57 (1.07–11.89) | 0.0383 |
| TET2 | 0.15 (0.02–0.94) | 0.0387 | 2.32 (0.70–7.63) | 0.1670 | 1.93 (0.62–6.03) | 0.2600 |
| RUNX1 | 0.44 (0.1–1.99) | 0.2747 | 2.20 (0.93–5.24) | 0.0741 | 1.93 (0.83–4.50) | 0.1277 |
| CEBPA2 * | 3.93 (0.47–98.06) | 0.2806 | 0.20 (0.04–0.92) | 0.0387 | 0.13 (0.03–0.58) | 0.0070 |
| ASXL1 | 1.38 (0.24–11.14) | 0.7367 | - | - | - | - |
| NRAS | - | - | 1.21 (0.38–3.87) | 0.7457 | 1.05 (0.34–3.29) | 0.9284 |
| SRSF2 | 0.08 (0.01–0.5) | 0.0093 | - | - | - | - |
| U2AF1 | - | - | 3.39 (1.16–9.92) | 0.0260 | 3.81 (1.35–10.78) | 0.0117 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salmoiraghi, S.; Cavagna, R.; Zanghì, P.; Pavoni, C.; Michelato, A.; Buklijas, K.; Elidi, L.; Intermesoli, T.; Lussana, F.; Oldani, E.; et al. High Throughput Molecular Characterization of Normal Karyotype Acute Myeloid Leukemia in the Context of the Prospective Trial 02/06 of the Northern Italy Leukemia Group (NILG). Cancers 2020, 12, 2242. https://doi.org/10.3390/cancers12082242
Salmoiraghi S, Cavagna R, Zanghì P, Pavoni C, Michelato A, Buklijas K, Elidi L, Intermesoli T, Lussana F, Oldani E, et al. High Throughput Molecular Characterization of Normal Karyotype Acute Myeloid Leukemia in the Context of the Prospective Trial 02/06 of the Northern Italy Leukemia Group (NILG). Cancers. 2020; 12(8):2242. https://doi.org/10.3390/cancers12082242
Chicago/Turabian StyleSalmoiraghi, Silvia, Roberta Cavagna, Pamela Zanghì, Chiara Pavoni, Anna Michelato, Ksenija Buklijas, Lara Elidi, Tamara Intermesoli, Federico Lussana, Elena Oldani, and et al. 2020. "High Throughput Molecular Characterization of Normal Karyotype Acute Myeloid Leukemia in the Context of the Prospective Trial 02/06 of the Northern Italy Leukemia Group (NILG)" Cancers 12, no. 8: 2242. https://doi.org/10.3390/cancers12082242