Development, Implementation and Assessment of Molecular Diagnostics by Next Generation Sequencing in Personalized Treatment of Cancer: Experience of a Public Reference Healthcare Hospital

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Performance Evaluation of Next Generation Sequencing
2.1.1. Next Generation Sequencing Quality Assessment
2.1.2. Comparison of Next Generation Sequencing with Conventional Methods
2.1.3. Turnaround Time (TAT) and Cost Comparison
2.1.4. Clinical Laboratory Accreditation
2.2. Next Generation Sequencing Results in the Routine Setting
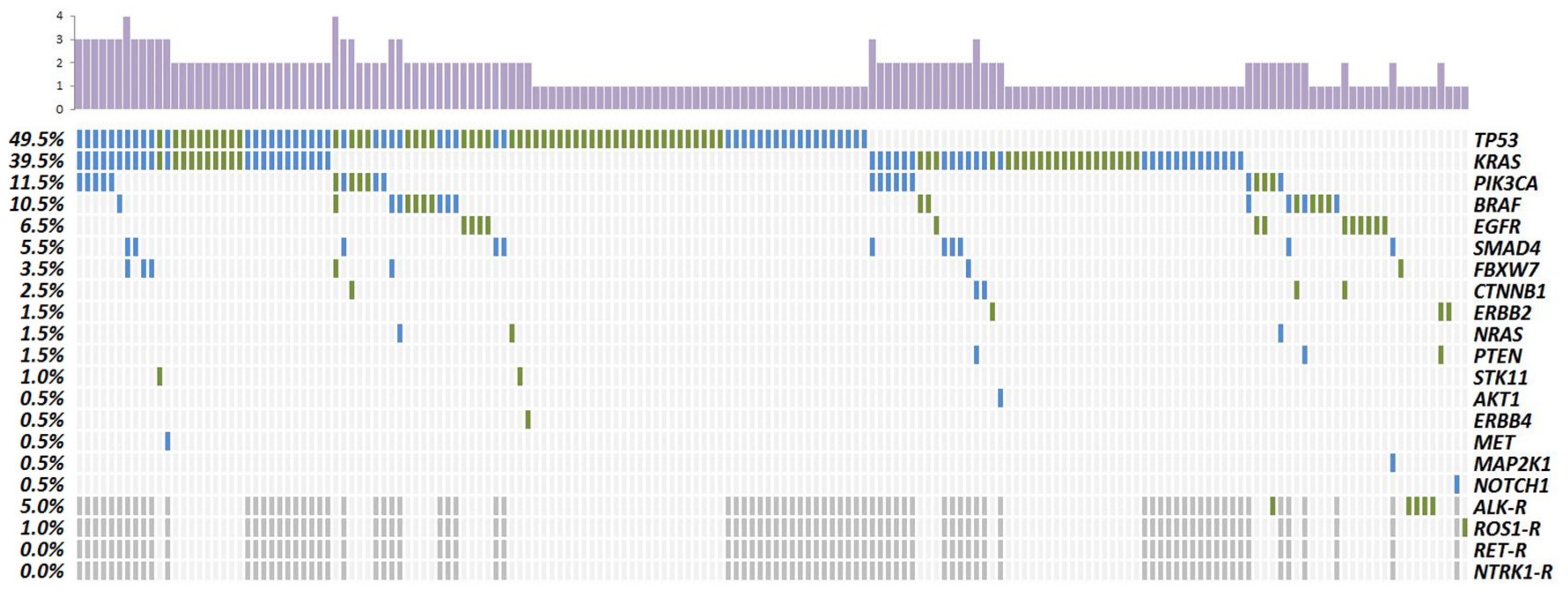
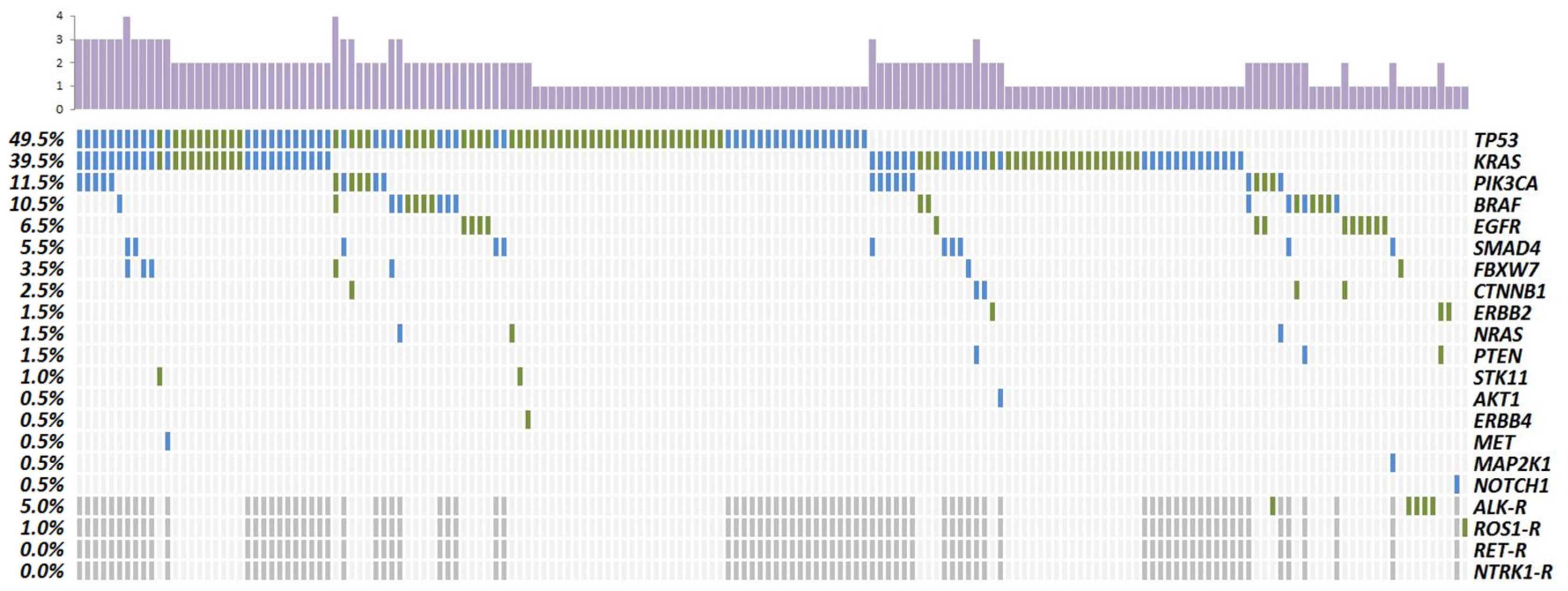
2.2.1. Pathogenic Alterations Detected by Next Generation Sequencing
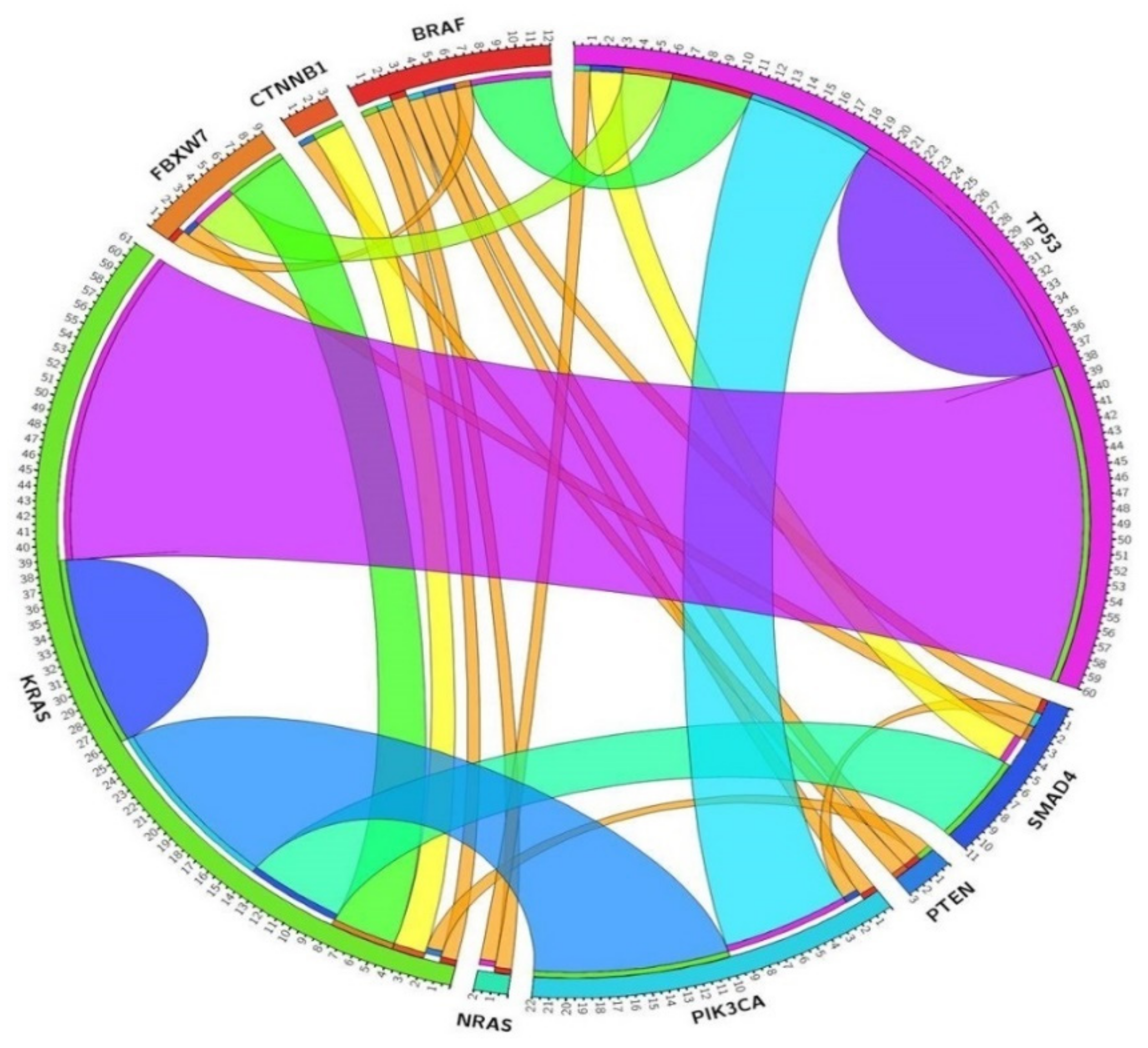
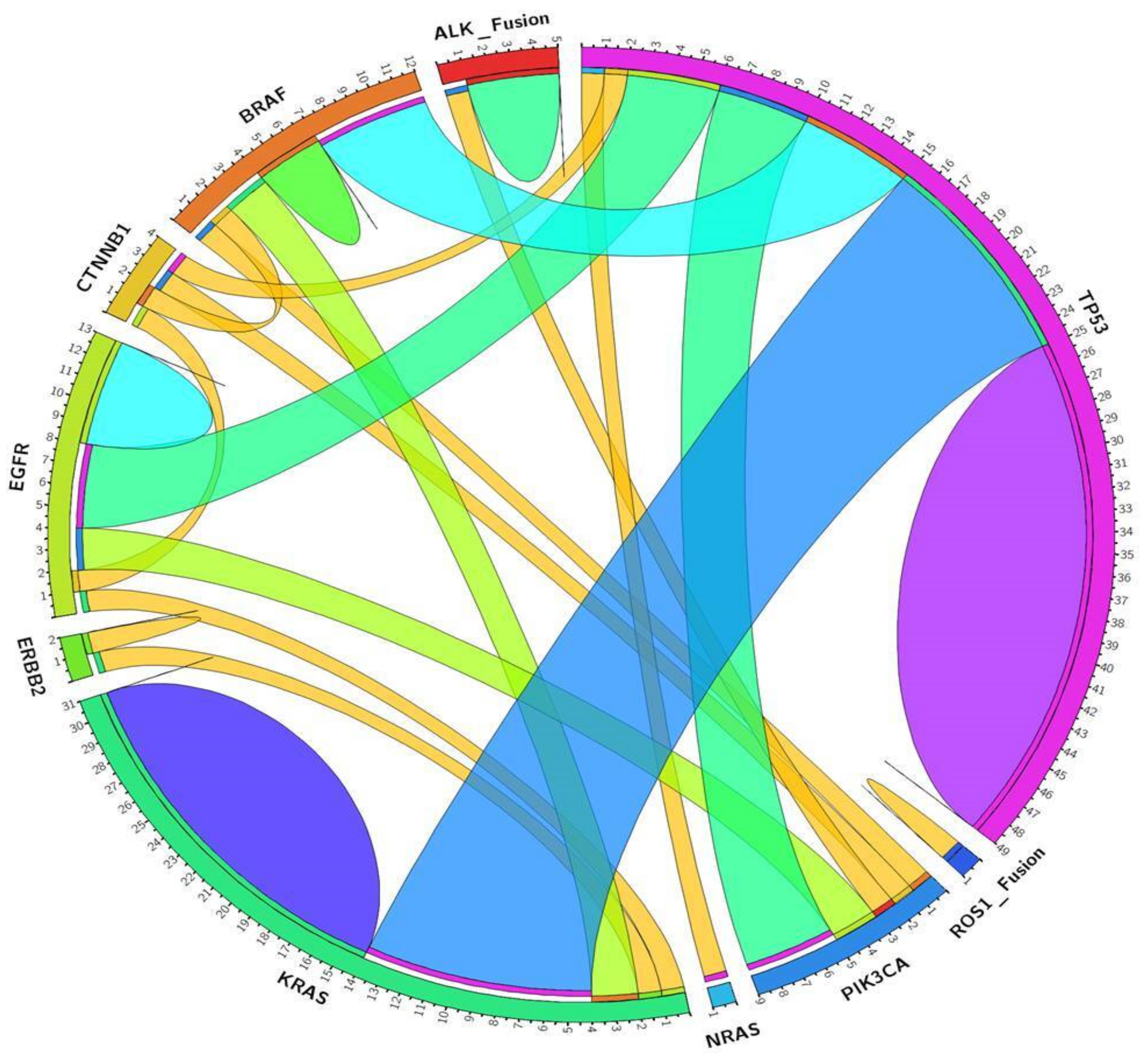
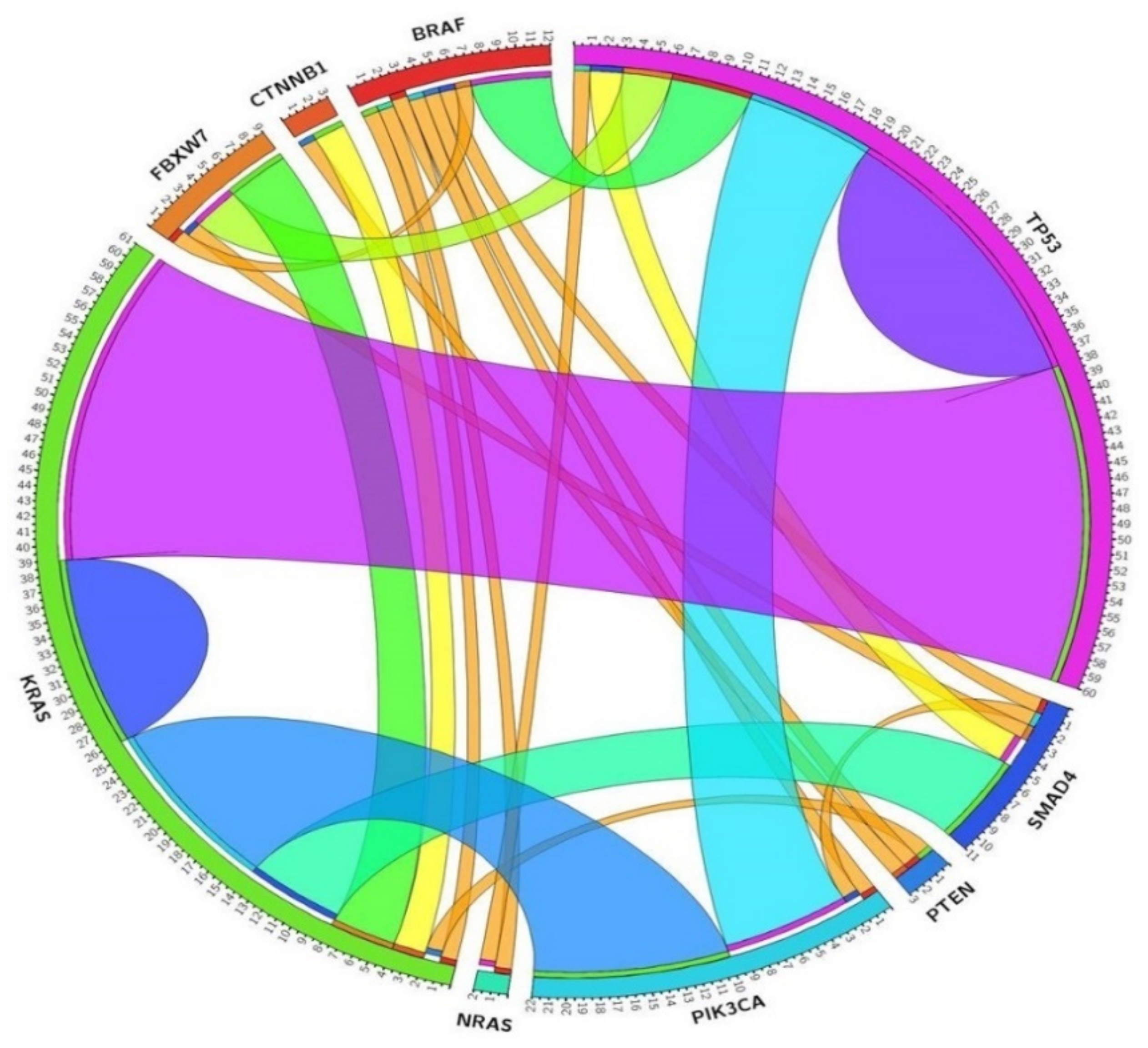
2.2.2. Concurrent Molecular Alterations
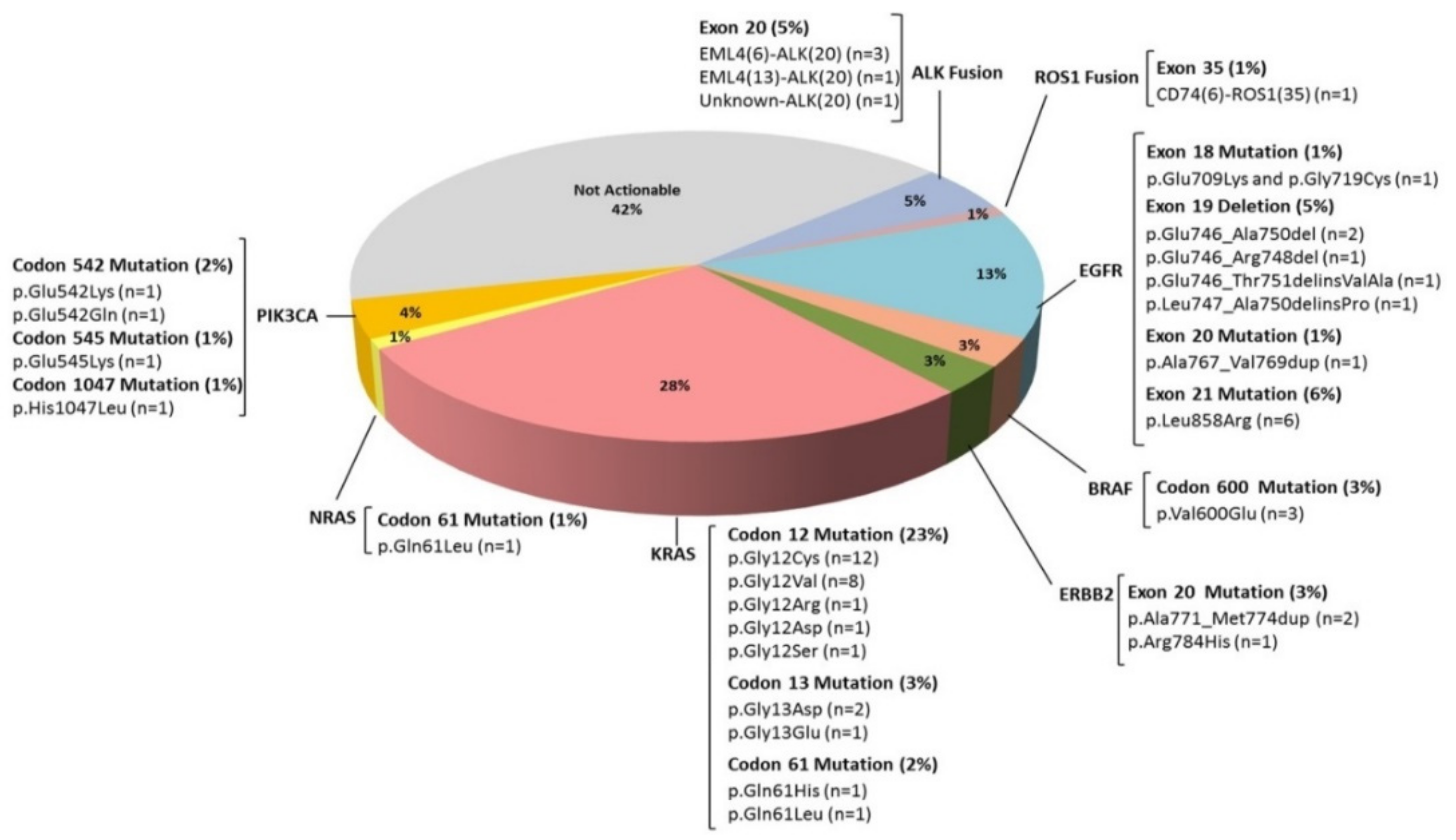
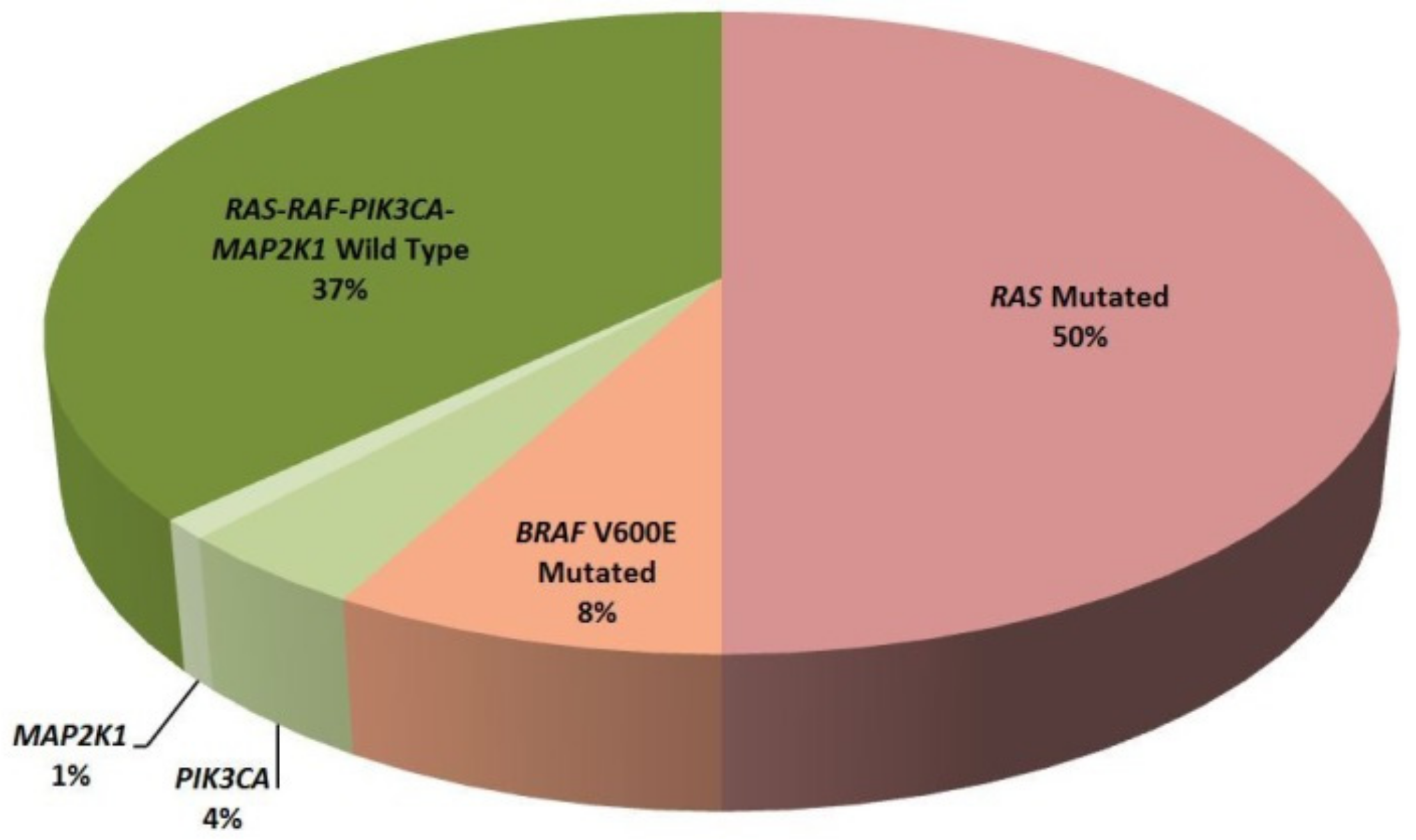
2.2.3. Clinically Relevant Genetic Variants
3. Discussion
4. Materials and Methods
4.1. Patients and Samples
4.2. DNA and RNA Preparation
4.3. Molecular Analysis by Next Generation Sequencing
4.3.1. Next Generation Sequencing Panels
4.3.2. Ion Torrent Library Preparation
4.3.3. Clonal Amplification and DNA Sequencing
4.3.4. Base Calling, Variant Annotation and Prediction Tools Analysis
4.4. Experimental Verification
4.4.1. Low Frequency Variant Detection
4.4.2. Next Generation Sequencing Metrics
4.4.3. Assessment of the Diagnostic Sensitivity and Specificity of the NGS Assay
4.4.4. External Quality Assessment (EQA) Program
4.5. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cagle, P.T.; Chirieac, L.R. Advances in treatment of lung cancer with targeted therapy. Arch. Pathol. Lab. Med. 2012, 136, 504–599. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Wilcox, W.R. Changing paradigm of cancer therapy: Precision medicine by next-generation sequencing. Cancer Biol. Med. 2016, 13, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Pannuti, A.; Filipovic, A.; Hicks, C.; Lefkowitz, E.; Ptacek, T.; Stebbing, J.; Miele, L. Novel putative drivers revealed by targeted exome sequencing of advanced solid tumors. PLoS ONE 2018, 13, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Illei, P.B.; Belchis, D.; Tseng, L.H.; Nguyen, D.; De Marchi, F.; Haley, L.; Riel, S.; Beierl, K.; Zheng, G.; Brahmer, J.R.; et al. Clinical mutational profiling of 1006 lung cancers by next generation sequencing. Oncotarget 2017, 20, 96684–96696. [Google Scholar] [CrossRef] [PubMed]
- D’Haene, N.; Fontanges, Q.; De Nève, N.; Blanchard, O.; Melendez, B.; Delos, M.; Dehou, M.F.; Maris, C.; Nagy, N.; Rousseau, E.; et al. Clinical application of targeted next-generation sequencing for colorectal cancer patients: A multicentric Belgian experience. Oncotarget 2018, 17, 20761–20768. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Späth, S.S.; Marjani, S.L.; Zhang, W.; Pan, X. Characterization of cancer genomic heterogeneity by next-generation sequencing advances precision medicine in cancer treatment. Precis. Clin. Med. 2018, 1, 29–48. [Google Scholar] [CrossRef] [Green Version]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef]
- Jennings, L.J.; Arcila, M.E.; Corless, C.; Kamel-Reid, S.; Lubin, I.M.; Pfeifer, J.; Temple-Smolkin, R.L.; Voelkerding, K.V.; Nikiforova, M.N. Guidelines for validation of Next-generation sequencing-based oncology panels: A joint consensus recommendation of the association for Molecular Pathology and College of American Pathologists. J. Mol. Diagn. 2017, 19, 341–365. [Google Scholar] [CrossRef]
- Sepulveda, A.R.; Hamilton, S.R.; Allegra, C.J.; Grody, W.; Cushman-Vokoun, A.M.; Funkhouser, W.K.; Kopetz, S.E.; Lieu, C.; Lindor, N.M.; Minsky, B.D.; et al. Molecular Biomarkers for the Evaluation of Colorectal Cancer: Guideline From the American Society for Clinical Pathology, College of American Pathologists, Association for Molecular Pathology, and the American Society of Clinical Oncology. J. Clin. Oncol. 2017, 1, 1453–1486. [Google Scholar] [CrossRef]
- D’Haene, N.; Le Mercier, M.; De Nève, N.; Blanchard, O.; Delaunoy, M.; El Housni, H.; Dessars, B.; Heimann, P.; Remmelink, M.; Demetter, P.; et al. Clinical validation of targeted next generation sequencing for colon and lung cancers. PLoS ONE 2015, 10, 1–13. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN Guidelines Insights: Colon Cancer, Version 2.2018. J. Natl. Compr. Canc. Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic Non-Small Cell Lung Cancer: Esmo Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, 192–237. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda-Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO Consensus Guidelines for the Management of Patients with Metastatic Colorectal Cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Thelen, M.H.M.; Huisman, W. Harmonization of accreditation to ISO15189. Clin. Chem. Lab. Med. 2018, 10, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- European Molecular Genetics Quality Network (EMQN) Office. Available online: https://www.emqn.org/ (accessed on 15 July 2019).
- Biankin, A.V.; Piantadosi, S.; Hollingsworth, S.J. Patient-centric trials for therapeutic development in precision oncology. Nature 2015, 526, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Friedman, A.A.; Letai, A.; Fisher, D.E.; Flaherty, K.T. Precision medicine for cancer with next-generation functional diagnostics. Nat. Rev. Cancer 2015, 15, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Raymaekers, M.; Bakkus, M.; Boone, E.; de Rijke, B.; El Housni, H.; Descheemaeker, P.; De Schouwer, P.; Franke, S.; Hillen, F.; Nolet, F.; et al. Reflections and proposals to assure quality in molecular diagnostics. Acta. Clin. Belg. 2011, 66, 33–41. [Google Scholar] [CrossRef]
- Dubbink, H.J.; Deans, Z.C.; Tops, B.B.; van Kemenade, F.J.; Koljenović, S.; van Krieken, H.J.; Blokx, W.A.; Dinjens, W.N.; Groenen, P.J. Next generation diagnostic molecular pathology: Critical appraisal of quality assurance in Europe. Mol. Oncol. 2014, 8, 830–839. [Google Scholar] [CrossRef]
- Misyura, M.; Zhang, T.; Sukhai, M.A.; Thomas, M.; Garg, S.; Kamel-Reid, S.; Stockley, T.L. Comparison of Next-Generation Sequencing Panels and Platforms for Detection and Verification of Somatic Tumor Variants for Clinical Diagnostics. J. Mol. Diagn. 2016, 6, 842–850. [Google Scholar] [CrossRef]
- Hung, S.S.; Meissner, B.; Chavez, E.A.; Ben-Neriah, S.; Ennishi, D.; Jones, M.R.; Shulha, H.P.; Chan, F.C.; Boyle, M.; Kridel, R.; et al. Assessment of Capture and Amplicon-Based Approaches for the Development of a Targeted Next-Generation Sequencing Pipeline to Personalize Lymphoma Management. J. Mol. Diagn. 2018, 20, 203–214. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Liu, H.; Hou, Y.; Zhou, X.; Liang, L.; Zhang, Z.; Shi, H.; Xu, S.; Hu, P.; Zheng, Z.; et al. Performance validation of an amplicon-based targeted next-generation sequencing assay and mutation profiling of 648 Chinese colorectal cancer patients. Virchows Arch. 2018, 472, 959–968. [Google Scholar] [CrossRef] [PubMed]
- De Leng, W.W.; Gadellaa-van Hooijdonk, C.G.; Barendregt-Smouter, F.A.; Koudijs, M.J.; Nijman, I.; Hinrichs, J.W.; Cuppen, E.; van Lieshout, S.; Loberg, R.D.; de Jonge, M.; et al. Targeted Next Generation Sequencing as a Reliable Diagnostic Assay for the Detection of Somatic Mutations in Tumours Using Minimal DNA Amounts from Formalin Fixed Paraffin Embedded Material. PLoS ONE 2016, 26, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Strom, S.P. Current practices and guidelines for clinical next-generation sequencing oncology testing. Cancer Biol. Med. 2016, 13, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magdaleno, S.M.; Cheng, A.; Petratroli, R.; Shelis, O.; Tops, B.; Le Corre, D.; Kurth, H.; Blons, H.; Amato, E.; Mafficini, A.; et al. Abstract 3575: The OncoNetwork Consortium: A global collaborative research study on the development and verification of an Ion AmpliSeq RNA gene lung fusion panel. Cancer Res. 2014, 74. [Google Scholar] [CrossRef]
- Velizheva, N.P.; Rechsteiner, M.P.; Valtcheva, N.; Freiberger, S.N.; Wong, C.E.; Vrugt, B.; Zhong, Q.; Wagner, U.; Moch, H.; Hillinger, S.; et al. Targeted next-generation-sequencing for reliable detection of targetable rearrangements in lung adenocarcinoma-a single center retrospective study. Pathol. Res. Pract. 2018, 214, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Biswas, B. Clinical Performance Evaluation of Molecular Diagnostic Tests. J. Mol. Diagn. 2016, 18, 803–812. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.P.; Ruiz-Cordero, R.; Chen, W.; Routbort, M.J.; Floyd, K.; Rodriguez, S.; Galbincea, J.; Barkoh, B.A.; Hatfield, D.; Khogeer, H.; et al. Ultra-Rapid Reporting of GENomic Targets (URGENTseq): Clinical Next-Generation Sequencing Results within 48 Hours of Sample Collection. J. Mol. Diagn. 2019, 21, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Hamblin, A.; Wordsworth, S.; Fermont, J.M.; Page, S.; Kaur, K.; Camps, C.; Kaisaki, P.; Gupta, A.; Talbot, D.; Middleton, M.; et al. Clinical applicability and cost of a 46-gene panel for genomic analysis of solid tumours: Retrospective validation and prospective audit in the UK National Health Service. PLoS Med. 2017, 14, 1–26. [Google Scholar] [CrossRef]
- Hagemann, I.S.; Devarakonda, S.; Lockwood, C.M.; Spencer, D.H.; Guebert, K.; Bredemeyer, A.J.; Al-Kateb, H.; Nguyen, T.T.; Duncavage, E.J.; Cottrell, C.E.; et al. Clinical next-generation sequencing in patients with non-small cell lung cancer. Cancer 2015, 121, 631–639. [Google Scholar] [CrossRef]
- Burrell, R.A.; Swanton, C. Tumour heterogeneity and the evolution of polyclonal drug resistance. Mol. Oncol. 2014, 8, 1095–1111. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature 2014, 511, 543–550. [Google Scholar] [CrossRef]
- Peeters, M.; Kafatos, G.; Taylor, A.; Gastanaga, V.M.; Oliner, K.S.; Hechmati, G.; Terwey, J.H.; van Krieken, J.H. Prevalence of RAS mutations and individual variation patterns among patients with metastatic colorectal cancer: A pooled analysis of randomised controlled trials. Eur. J. Cancer 2015, 13, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- El-Deiry, W.S.; Vijayvergia, N.; Xiu, J.; Scicchitano, A.; Lim, B.; Yee, N.S.; Harvey, H.A.; Gatalica, Z.; Reddy, S. Molecular profiling of 6,892 colorectal cancer samples suggests different possible treatment options specific to metastatic sites. Cancer Biol. Ther. 2015, 16, 1726–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, Z.B.; Duan, C.Y.; Li, C.B.; Cui, L.; Ogino, S. Prognostic role of tumor PIK3CA mutation in colorectal cancer: A systematic review and meta-analysis. Ann. Oncol. 2016, 10, 1836–1848. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Gong, H.; Zhao, H.; Chen, J.; Zhang, Y.; Zhang, L.; Shi, X.; Zhang, A.; Jin, H.; Zhang, J.; et al. Mutation status and prognostic values of KRAS, NRAS, BRAF and PIK3CA in 353 Chinese colorectal cancer patients. Sci. Rep. 2018, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Kim, K.K.; Kim, S.Y.; Lee, J.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Kang, W.K.; Kim, S.T. MAP2K1 Mutation in Colorectal Cancer Patients: Therapeutic Challenge Using Patient-Derived Tumor Cell Lines. J. Cancer 2017, 8, 2263–2268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jincui, G.; Yanbin, Z.; Lixia, H.; Weijun, O.; Jian, W.; Shaoli, L.; Junwen, X.; Jinlun, F.; Baomo, L. TP53 mutation is associated with a poor clinical outcome for non-small cell lung cancer: Evidence from a meta-analysis. Mol. Clin. Oncol. 2016, 5, 705–713. [Google Scholar] [CrossRef] [Green Version]
- La Fleur, L.; Falk-Sörqvist, E.; Smeds, P.; Berglund, A.; Sundström, M.; Mattsson, J.S.; Brandén, E.; Koyi, H.; Isaksson, J.; Brunnström, H.; et al. Mutation patterns in a population-based non-small cell lung cancer cohort and prognostic impact of concomitant mutations in KRAS and TP53 or STK11. Lung Cancer. 2019, 130, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Huemer, F.; Thaler, J.; Piringer, G.; Hackl, H.; Pleyer, L.; Hufnagl, C.; Weiss, L.; Greil, R. Sidedness and TP53 mutations impact OS in anti-EGFR but not anti-VEGF treated mCRC—an analysis of the KRAS registry of the AGMT (Arbeitsgemeinschaft Medikamentöse Tumortherapie). BMC Cancer 2018, 18, 1–11. [Google Scholar] [CrossRef]
- Mehrvarz Sarshekeh, A.; Advani, S.; Overman, M.J.; Manyam, G.; Kee, B.K.; Fogelman, D.R.; Dasari, A.; Raghav, K.; Vilar, E.; Manuel, S.; et al. Association of SMAD4 mutation with patient demographics, tumor characteristics, and clinical outcomes in colorectal cancer. PLoS ONE 2017, 12, 1–14. [Google Scholar] [CrossRef]
- Korphaisarn, K.; Morris, V.K.; Overman, M.J.; Fogelman, D.R.; Kee, B.K.; Raghav, K.P.S.; Manuel, S.; Shureiqi, I.; Wolff, R.A.; Eng, C.; et al. FBXW7 missense mutation: A novel negative prognostic factor in metastatic colorectal adenocarcinoma. Oncotarget 2017, 24, 39268–39279. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/wp-content/uploads/2016/11/DoH-Oct2013-JAMA.pdf (accessed on 15 July 2019).
- Catalogue of Somatic Mutations in Cancer. Available online: http://cancer.sanger.ac.uk/cosmic (accessed on 15 July 2019).
- Kopanos, C.; Tsiolkas, V.; Kouris, A.; Chapple, C.E.; Albarca-Aguilera, M.; Meyer, R.; Massouras, A. VarSome: The human genomic variant search engine. Bioinformatics 2019, 35, 1978–1980. [Google Scholar] [CrossRef] [PubMed]
- 1000 Genomes. Available online: http://browser.1000genomes.org/index.html (accessed on 15 July 2019).
- National Center for Biotechnology Information. dbSNP. Available online: https://www.ncbi.nlm.nih.gov/projects/SNP/ (accessed on 15 July 2019).
- Protein Variation Effect Analyzer. Available online: http://provean.jcvi.org/index.php (accessed on 15 July 2019).
- Kumar, P.; Henikoff, S.; Ng, P.C. Predicting the effects of coding non-synonymous variants on protein function using the SIFT algorithm. Nat. Protoc. 2009, 7, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Adzhubei, I.A.; Schmidt, S.; Peshkin, L.; Ramensky, V.E.; Gerasimova, A.; Bork, P.; Kondrashov, A.S.; Sunyaev, S.R. A method and server for predicting damaging missense mutations. Nat. Methods 2010, 7, 248–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, G.H.; Wittwer, C.T. Sensitivity and specificity of single-nucleotide polymorphism scanning by high-resolution melting analysis. Clin. Chem. 2004, 50, 1748–1754. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conventional Methods Result | ||||
|---|---|---|---|---|
| Gene | Mutation/Fusion Detected | Not Detected | Parameter | Agreement |
| EGFR-NGS Result | ||||
| Mutation Detected | 13 | 0 | PPA | 92.9% |
| Not Detected | 1 | 86 | NPA | 100% |
| OA | 99.0% | |||
| KRAS-NGS Result | ||||
| Mutation Detected | 74 | 5 | PPA | 97.4% |
| Not Detected | 2 | 50 | NPA | 90.9% |
| OA | 94.7% | |||
| NRAS-NGS Result | ||||
| Mutation Detected | 3 | 0 | PPA | 100% |
| Not Detected | 0 | 54 | NPA | 100% |
| OA | 100% | |||
| BRAF-NGS Result | ||||
| Mutation Detected | 9 | 2 | PPA | 100% |
| Not Detected | 0 | 45 | NPA | 95.8% |
| OA | 96.4% | |||
| ALK Fusions-NGS Result | ||||
| Fusion Detected | 4 | 1 | PPA | 100% |
| Not Detected | 0 | 95 | NPA | 99.0% |
| OA | 99.0% | |||
| ROS1 Fusions-NGS Result | ||||
| Fusion Detected | 1 | 0 | PPA | 100% |
| Not Detected | 0 | 99 | NPA | 100% |
| OA | 100% | |||
| Analysis | System | Hands-on Time, min (h) | Time Duration, min (h) | Costs (€) |
|---|---|---|---|---|
| NGS Analysis (8 NSCLC samples (DNA + RNA)) | ||||
| DNA and RNA isolation | Manual | 90 (1.5) | 1140 (19.0) | 166.96 |
| Quantification and sample dilution | Qubit | 30 (0.5) | 30 (0.5) | 13.68 |
| Library preparation DNA | Veriti Thermal Cycler | 120 (2.0) | 1440 (24.0) | 984.00 |
| Library preparation RNA | Veriti Thermal Cycler | 1214.72 | ||
| Emulsion PCR | One Touch | 20 (0.3) | 480 (8.0) | 124.16 |
| Enrichment | One Touch ES | 10 (0.2) | 30 (0.5) | 23.70 |
| Sequencing | PGM System | 10 (0.2) | 240 (4.0) | 607.00 |
| Data Processing and analysis | Ion Reporter | 160 (2.6) | 180 (3.0) | - |
| Laboratory personnel costs † | - | 235.60 | ||
| Total Cost | - | - | 3369.84 | |
| Cost per sample | - | - | 421.23 | |
| Working days | 440 (7.3) | 5 days | - | |
| Conventional Molecular Analysis (8 NSCLC samples (DNA)) | ||||
| DNA isolation | Manual | 60 (1.0) | 1140 (19.0) | 84.16 |
| Quantification and sample dilution | Qubit | 15 (0.25) | 30 (0.5) | 5.04 |
| EGFR (Exon 18, 19, 20 and 21) | RT-qPCR | 20 (0.3) | 120 (2.0) | 1391.50 |
| ALK- Rearrangements | IHQ | 10 (0.2) | 960 (16.0) | 672.00 |
| ROS1-Rearrangements | IHQ | 10 (0.2) | 960 (16.0) | 672.00 |
| Sanger sequencing | SS | 30 (0.5) | 480 (8.0) | 40.00 |
| Data Processing and analysis | 30 (0.5) | 30 (0.5) | - | |
| Laboratory personnel costs † | - | 76.55 | ||
| Total Cost | - | - | 2941.27 | |
| Cost per sample | 367.66 | |||
| Working days | 175 (2.9) | 3 days | - | |
| NGS Analysis (10 mCRC samples (DNA)) | ||||
| DNA isolation | Manual | 60 (1.0) | 1140 (19.0) | 105.20 |
| Quantification and sample dilution | Qubit | 15 (0.25) | 30 (0.5) | 6.30 |
| Library preparation DNA | Veriti Thermal Cycler | 120 (2.0) | 1440 (24.0) | 1230.00 |
| Emulsion PCR | One Touch | 20 (0.4) | 480 (8.0) | 77.60 |
| Enrichment | One Touch ES | 10 (0.2) | 30 (0.5) | 14.80 |
| Sequencing | PGM System | 10 (0.2) | 240 (4.0) | 379.40 |
| Data Processing and analysis | Ion Reporter | 160 (2.6) | 180 (3.0) | - |
| Laboratory personnel costs † | - | 219.85 | ||
| Total Cost | - | - | 2033.15 | |
| Cost per sample | - | - | 203.32 | |
| Working days | 395 (6.6) | 5 days | - | |
| Conventional Molecular Analysis (10 mCRC samples (DNA)) | ||||
| DNA isolation | Manual | 60 (1.0) | 1140 (19.0) | 105.20 |
| Quantification and sample dilution | Qubit | 15 (0.25) | 30 (0.5) | 6.30 |
| KRAS (Exon 2,3 and 4) | RT-qPCR | 20 (0.3) | 150 (2.5) | 1530.60 |
| NRAS (Exon 2,3 and 4) | IHQ | 20 (0.3) | 150 (2.5) | 1391.50 |
| BRAF (Codon 600) | IHQ | 30 (0.5) | 120 (2.0) | 1001.80 |
| Sanger sequencing | SS | 30 (0.5) | 480 (8.0) | 50.00 |
| Data Processing and analysis | 30 (0.5) | 30 (0.5) | - | |
| Laboratory personnel costs † | - | - | 87.05 | |
| Total Cost | - | - | 4172.47 | |
| Cost per sample | - | - | 417.25 | |
| Working days | 250 (3.4) | 4 days * | - | |
| NSCLC Patients (n = 100) | mCRC Patients (n = 100) | ||
|---|---|---|---|
| Variable | n | Variable | n |
| Age (mean ±SD) | 65.18 ± 10.66 | Age (mean ±SD) | 64.91 ± 10.82 |
| Age, years | Age, years | ||
| <60 | 30 | <60 | 34 |
| ≥60 | 70 | ≥60 | 66 |
| Gender | Gender | ||
| Male | 65 | Male | 63 |
| Female | 35 | Female | 37 |
| Anatomic site | Anatomic site | ||
| Primary tumor | 85 | Primary tumor | 85 |
| Regional lymph nodes | 5 | Liver | 7 |
| Brain | 4 | Lung | 4 |
| Liver | 2 | Peritoneum | 2 |
| Others | 4 | Others | 2 |
| Histologic NSCLC type | Histologic mCRC type | ||
| Adenocarcinoma | 87 | Adenocarcinoma | 100 |
| Squamous Cell Carcinoma | 3 | ||
| NOS | 10 | ||
| Smoking status | Tumor Location | ||
| Non-smoker | 21 | Sigmoid Colon | 31 |
| Ex-smoker | 45 | Rectum | 26 |
| Current-smoker | 34 | Right (ascending) colon | 14 |
| Left (descending) colon | 9 | ||
| Transverse colon | 6 | ||
| Splenic flexure | 5 | ||
| Cecum | 3 | ||
| Unknown | 6 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simarro, J.; Murria, R.; Pérez-Simó, G.; Llop, M.; Mancheño, N.; Ramos, D.; de Juan, I.; Barragán, E.; Laiz, B.; Cases, E.; et al. Development, Implementation and Assessment of Molecular Diagnostics by Next Generation Sequencing in Personalized Treatment of Cancer: Experience of a Public Reference Healthcare Hospital. Cancers 2019, 11, 1196. https://doi.org/10.3390/cancers11081196
Simarro J, Murria R, Pérez-Simó G, Llop M, Mancheño N, Ramos D, de Juan I, Barragán E, Laiz B, Cases E, et al. Development, Implementation and Assessment of Molecular Diagnostics by Next Generation Sequencing in Personalized Treatment of Cancer: Experience of a Public Reference Healthcare Hospital. Cancers. 2019; 11(8):1196. https://doi.org/10.3390/cancers11081196
Chicago/Turabian StyleSimarro, Javier, Rosa Murria, Gema Pérez-Simó, Marta Llop, Nuria Mancheño, David Ramos, Inmaculada de Juan, Eva Barragán, Begoña Laiz, Enrique Cases, and et al. 2019. "Development, Implementation and Assessment of Molecular Diagnostics by Next Generation Sequencing in Personalized Treatment of Cancer: Experience of a Public Reference Healthcare Hospital" Cancers 11, no. 8: 1196. https://doi.org/10.3390/cancers11081196