Phenotype-Driven Diagnostic of PTEN Hamartoma Tumor Syndrome: Macrocephaly, But Neither Height nor Weight Development, Is the Important Trait in Children

Abstract
:1. Introduction
2. Methods
3. Results
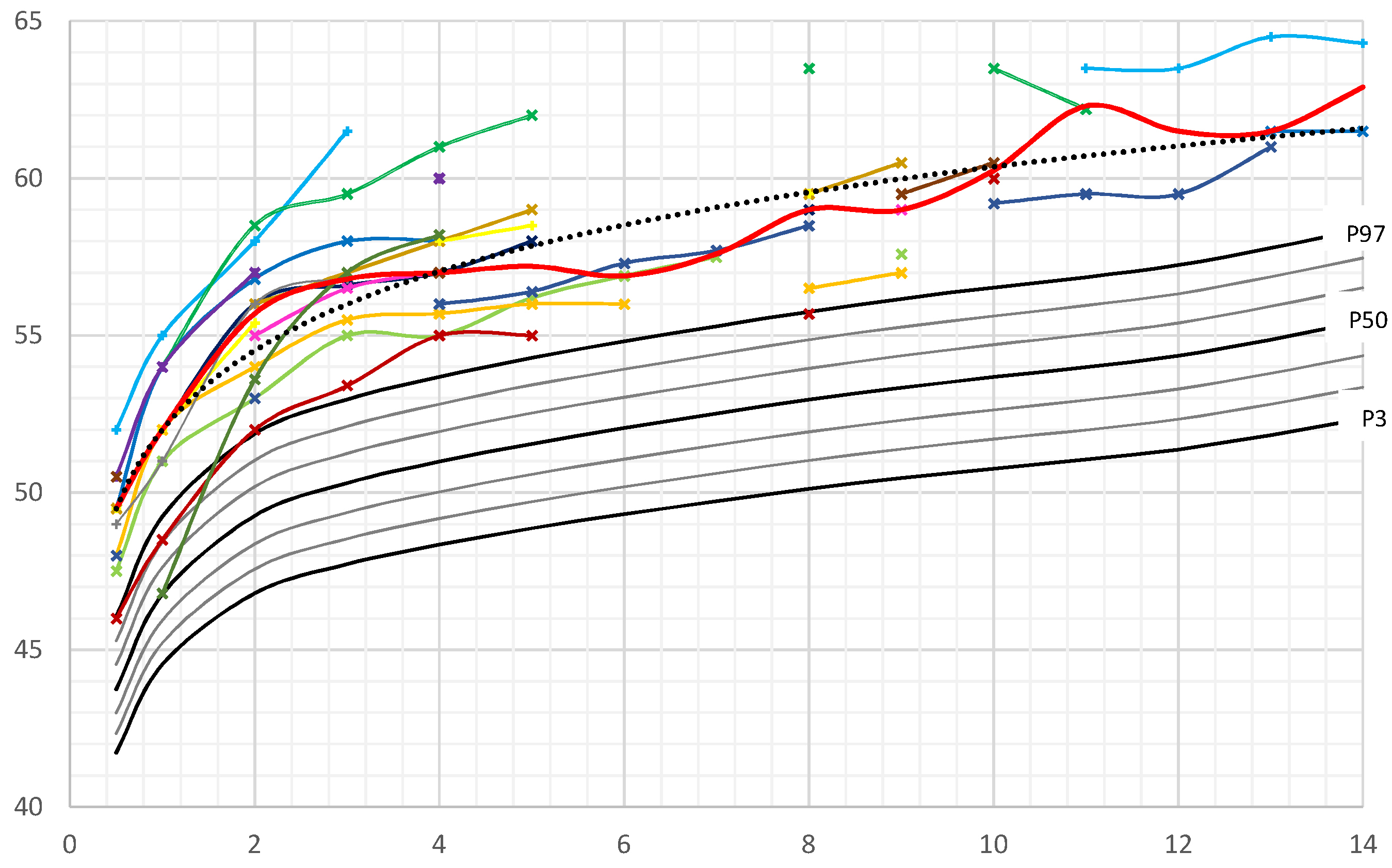
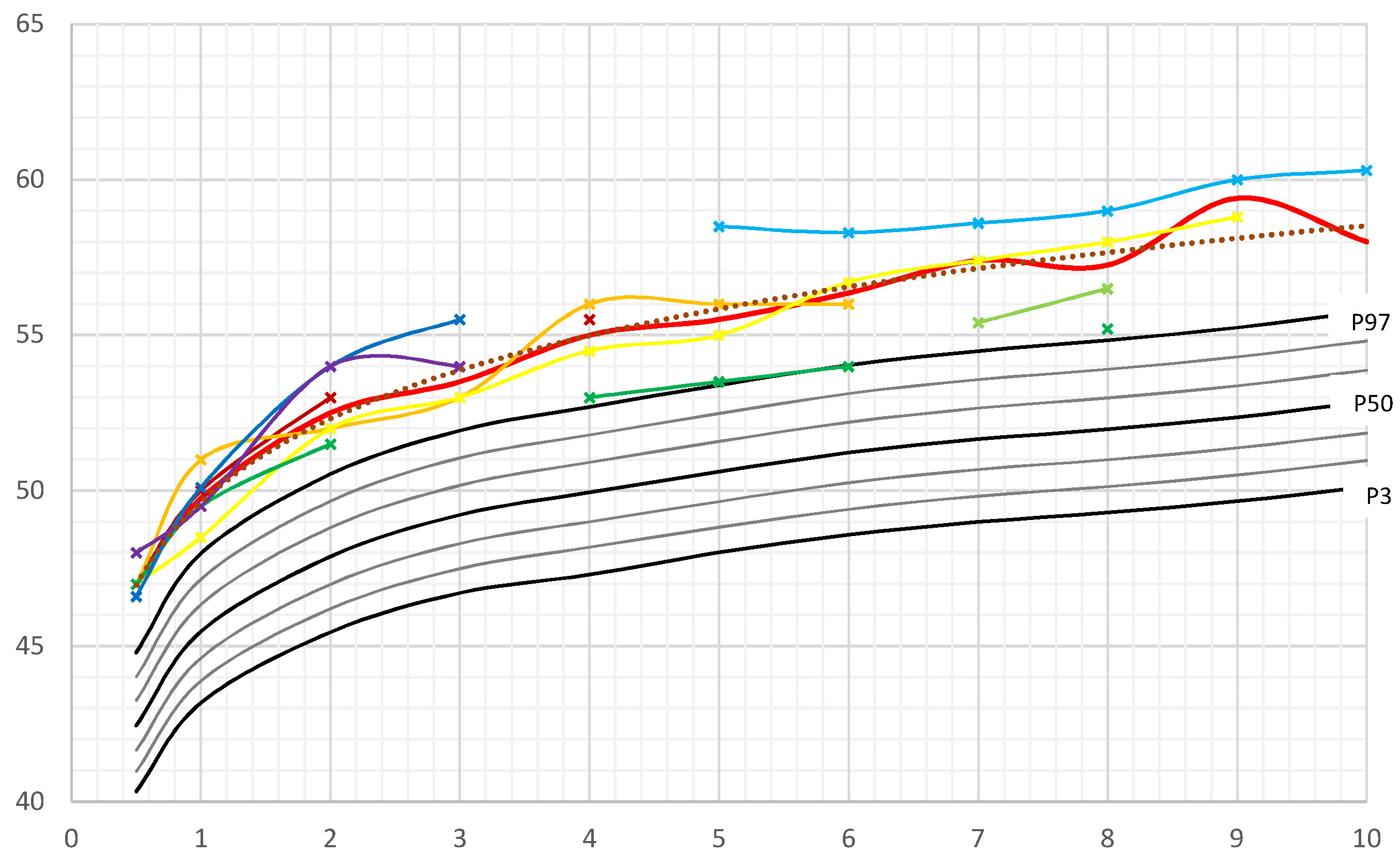
3.1. Head Circumference
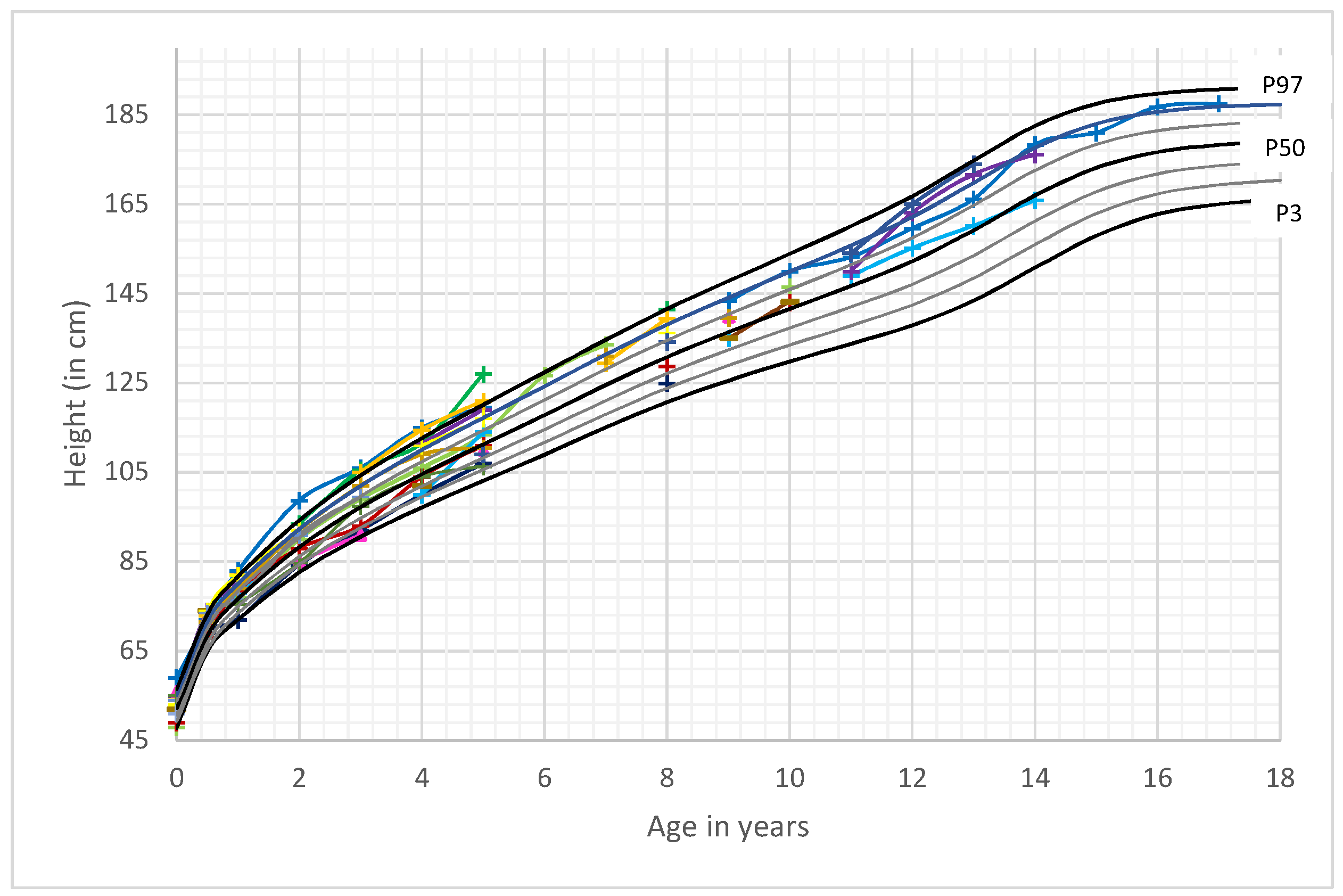
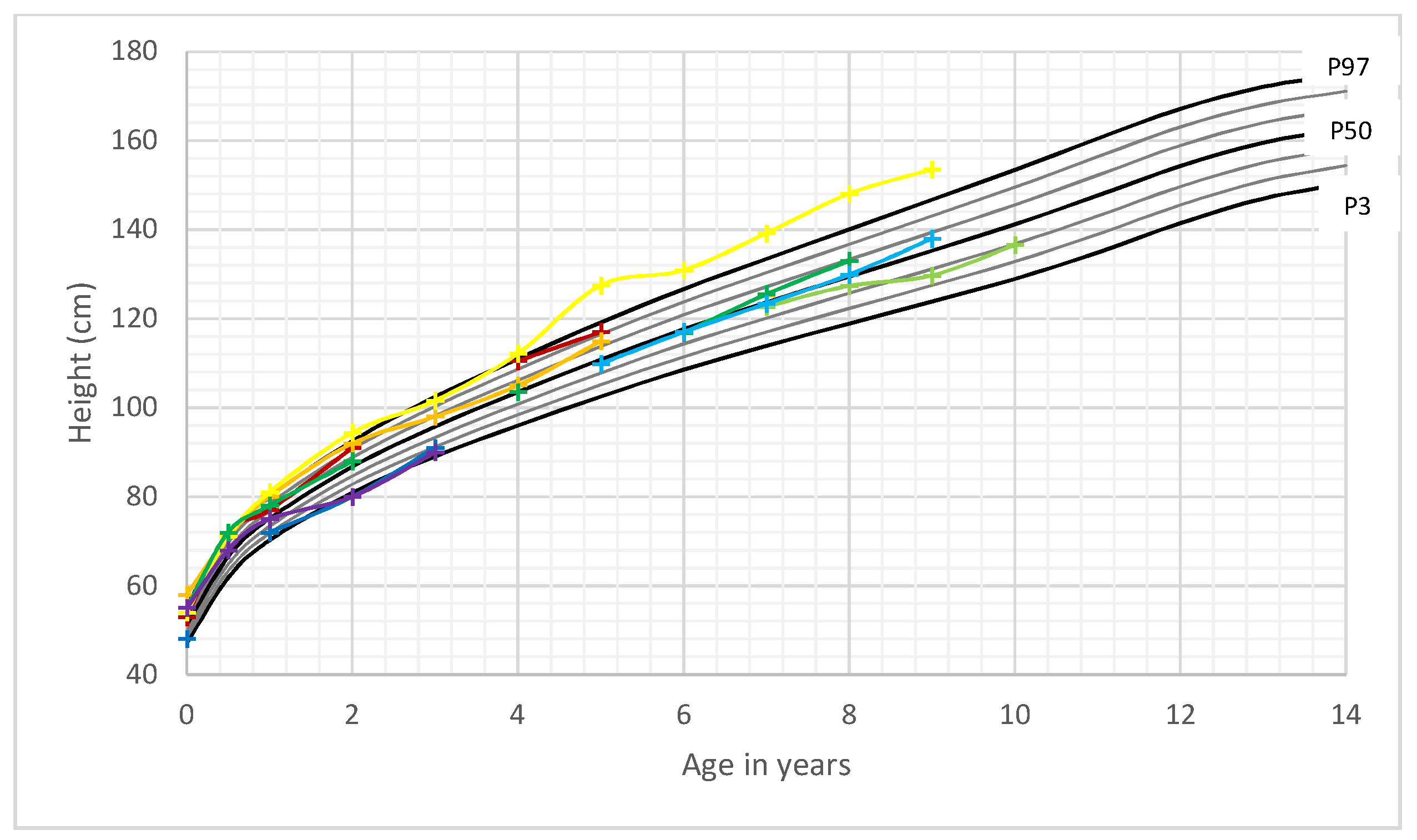
3.2. Length/Height
3.3. Weight and BMI Development
3.4. Additional Brain MRI and Clinical Characteristics of the Cohort
3.4.1. Brain MRI Scans
3.4.2. Clinical Features
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Marsh, D.J.; Kum, J.B.; Lunetta, K.L.; Bennett, M.J.; Gorlin, R.J.; Ahmed, S.F.; Bodurtha, J.; Crowe, C.; Curtis, M.A.; Dasouki, M.; et al. PTEN mutation spectrum and genotype-phenotype correlations in Bannayan-Riley-Ruvalcaba syndrome suggest a single entity with Cowden syndrome. Hum. Mol Genet. 1999, 8, 1461–1472. [Google Scholar] [CrossRef] [PubMed]
- Lachlan, K.L.; Lucassen, A.M.; Bunyan, D.; Temple, I.K. Cowden syndrome and Bannayan Riley Ruvalcaba syndrome represent one condition with variable expression and age-related penetrance: Results of a clinical study of PTEN mutation carriers. J. Med. Genet. 2007, 44, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.H.; Mester, J.L.; Ngeow, J.; Rybicki, L.A.; Orloff, M.S.; Eng, C. Lifetime cancer risks in individuals with germline PTEN mutations. Clin. Cancer Res. 2012, 18, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Pilarski, R.; Burt, R.; Kohlman, W.; Pho, L.; Shannon, K.M.; Swisher, E. Cowden syndrome and the PTEN hamartoma tumor syndrome: Systematic review and revised diagnostic criteria. J. Natl. Cancer Inst. 2013, 105, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.B.; Pilarski, R.; Axilbund, J.E.; Buys, S.S.; Crawford, B.; Friedman, S.; Garber, J.E.; Horton, C.; Kaklamani, V.; Klein, C.; et al. Genetic/Familial High-Risk Assessment: Breast and Ovarien, Version 1.2014. J. Natl. Compr. Cancer Netw. 2014, 12, 1326–1338. [Google Scholar] [CrossRef]
- Pilarski, R.; Eng, C. Will the real Cowden syndrome please stand up (again)? Expanding mutational and clinical spectra of the PTEN hamartoma tumour syndrome. J. Med. Genet. 2004, 41, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Parisi, M.A.; Dinulos, M.B.; Leppig, K.A.; Sybert, V.P.; Eng, C.; Hudgins, L. The spectrum and evolution of phenotypic findings in PTEN mutation positive cases of Bannayan-Riley-Ruvalcaba syndrome. J. Med. Genet. 2001, 38, 52–58. [Google Scholar] [CrossRef]
- Mester, J.L.; Tilot, A.K.; Rybicki, L.A.; Frazier, T.W.; Eng, C. Analysis of prevalence and degree of macrocephaly in patients with germline PTEN mutations and of brain weight in Pten knock-in murine model. Eur. J. Hum. Genet. 2011, 19, 763–768. [Google Scholar] [CrossRef]
- Starnik, T.M.; Van der Veen, J.P.; Arwert, F.; de Waal, L.P.; de Lange, G.G.; Gille, J.J.; Eriksson, A.W. The Cowden syndrome: A clinical and genetic study in 21 patients. Clin. Genet. 1986, 29, 222–233. [Google Scholar] [CrossRef]
- Ciaccio, C.; Saletti, V.; D’Arrigo, S.; Esposito, S.; Alfei, E.; Moroni, I.; Tonduti, D.; Chiapparini, L.; Pantaleoni, C.; Milani, D. Clinical spectrum of PTEN mutation in prediatric patients. A bicenter experience. Eur. J. Med. Genet. 2018. [Google Scholar] [CrossRef]
- Neuhauser, H.; Schienkiewitz, A.; Schaffrath Rosario, A.; Dortschy, R.; Kurth, B.M. Referenzperzentilen für anthropometrische Maßzahlen und Blutdruck aus der Studie zur Gesundheit von Kindern und Jugendlichen in Deutschland (KiGGS). In Beiträge zur Gesundheitsberichterstattung des Bundes, 2nd ed.; Robert Koch Institut: Berlin, Germany, 2013; ISBN 978-3-89606-218-5. [Google Scholar]
- Tanner, J.M.; Goldsteni, H.; Whitehouse, R.H. Standards for children’s height at ages 2–9 years allowing for heights of parents. Arch. Dis. Child. 1970, 45, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Stolzenberg, H.; Khal, H.; Bergmann, K.E. Body measurements of children and adolescents in Germany. Results of the German health interview and examination survey for children and adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Plamper, M.; Schreiner, F.; Gohlke, B.; Kionke, J.; Korsch, E.; Kirkpatrick, J.; Born, M.; Aretz, S.; Woelfle, J. Thyroid disease in children and adolescents with PTEN hamartoma tumor syndrome (PHTS). Eur. J. Pediatr. 2017, 177, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.H.; Baris, H.N.; Burrows, P.E.; Robson, C.D.; Alomari, A.I.; Mulliken, J.B.; Fishman, S.J.; Irons, M.B. The spectrum of vascular anomalies in patients with PTEN mutations: Implications for diagnosis and management. J. Med. Genet. 2007, 44, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.H.; Mester, J.; Peterson, C.; Yang, Y.; Chen, J.L.; Rybicki, L.A.; Milas, K.; Pederson, H.; Remzi, B.; Orloff, M.S.; et al. A clinical scoring system for selection of patients for PTEN mutation testing is proposed on the basis of a prospective study of 3042 probands. Am. J. Hum. Genet. 2011, 88, 42–56. [Google Scholar] [CrossRef]
- Kato, K.; Mizuno, S.; Inaba, M.; Fukumura, S.; Kurahashi, N.; Maruyama, K.; Ieda, D.; Ohashi, K.; Hori, I.; Negishi, Y.; et al. Distinctive facies, macrocephaly, and developmental delay are signs of PTEN mutation in childhood. Brain Dev. 2018, 40, 678–684. [Google Scholar] [CrossRef]
- Busa, T.; Milh, M.; Degardin, N.; Girard, N.; Sigaudy, S.; Longy, M.; Olshchwang, S.; Sobol, H.; Chabrol, B.; Philip, N. Clicical presentations of PTEN mutations in childhood in the absence of family history of Cowden syndrome. Eur. J. Paediatr. Neurol. 2015, 19, 188–192. [Google Scholar] [CrossRef]
- Bubien, V.; Bonnet, F.; Brouste, V.; Hoppe, S.; Barouk-Simonet, E.; David, A.; Edery, P.; Bottani, A.; Layet, V.; Caron, O.; et al. French Cowden Disease Network. High cumulative risks of cancer in patients with PTEN hamartoma tumour syndrome. J. Med. Genet. 2013, 50, 255–263. [Google Scholar] [CrossRef]
- Smpokou, P.; Fox, V.L.; Tan, W.H. PTEN hamartoma tumour syndrome: Early tumour development in children. Arch. Dis. Child. 2015, 100, 34–37. [Google Scholar] [CrossRef]
- Piccione, M.; Fragapane, T.; Antona, V.; Giachino, D.; Cupido, F.; Corsello, G. PTEN hamartoma tumor syndromes in childhood: Description of two cases and a proposal for follow-up protocol. Am. J. Med. Genet. A 2013, 161, 2902–2908. [Google Scholar] [CrossRef]
- DiLiberti, J.H. Inherited macrocephaly-hamartoma syndromes. Am. J. Med. Genet. 1998, 79, 284–290. [Google Scholar] [CrossRef]
- Hansen-Kiss, E.; Beinkampen, S.; Adler, B.; Frazier, T.; Prior, T.; Erdman, S.; Eng, C.; Herman, G. A retrospective chart review of the features of PTEN hamartoma tumour syndrome in children. J. Med. Genet. 2017, 54, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Plamper, M.; Aretz, S.; Buderus, S.; Kionke, J.; Schneider, D.; Kraegeloh-Mann, I.; Woelfe, J. AWMF Leitlinie: Diagnostik und Management von Patienten mit PTEN Hamartom Tumor Syndrom (PHTS) im Kindes- und Jugendalter. Available online: http://www.AWMF.org (accessed on 10 July 2019).
- Eng, C. PTEN Hamartoma Tumor Syndrome. 2001 Nov 29 [Updated 2016 Jun 2]. In GeneReviews® [Internet]; Adam, M.P., Ardinger, H.H., Pagon, R.A., Eds.; University of Washington: Seattle, WA, USA, 2016; ISSN 2372-0697. [Google Scholar]
- Smith, J.R.; Marqusee, E.; Webb, S.; Nose, V.; Fishman, S.J.; Shamberger, R.C.; Frates, M.C.; Huang, S.A. Thyroid nodules and cancer in children with PTEN hamartoma tumor syndrome. J. Clin. Endocrinol. Metab. 2011, 96, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Pavone, P.; Pratico, A.D.; Rizzo, R.; Corsello, G.; Ruggieri, M.; Parano, E.; Falsaperla, R. A clinical review on megalencephaly: A large brain as a possible sign of cerebral impairment. Medicine 2017, 96, e6814. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age in Years | n | Overweight n (%) | Obesity n (%) |
|---|---|---|---|
| 0.5 | 16 | 4 (25%) | 1 (6.25%) |
| 1 | 17 | 2 (11.8%) | 2 (11.8%) |
| 2 | 18 | 10 (55.5%) | 3 (16.7%) |
| 3 | 13 | 4 (30.8%) | 0 |
| 4 | 16 | 7 (43.8%) | 6 (37.5%) |
| 5 | 17 | 4 (23.5%) | 4 (23.5%) |
| 6 | 4 | 1 (25%) | 0 |
| 7 | 8 | 3 (37.5%) | 0 |
| 8 | 9 | 2 (22.2%) | 1 (11.1%) |
| 9 | 8 | 1 (12.5%) | 0 |
| 10 | 5 | 2 (40%) | 0 |
| 11 | 4 | 0 | 0 |
| 12 | 4 | 0 | 0 |
| 13 | 4 | 0 | 0 |
| Patient No (Male) | Mutation/Deletion in PTEN Gene (Localisation) | MRI Features | Add. Clinical Features (Except Macrocephaly) |
|---|---|---|---|
| 1 | c.389G>A; Arg130 Gln (exon 5) | n.d. | Follicular adenoma (thyroid), multiple GI polyps, lipoma, hemangioma |
| 2 | c.389G>A; Arg130 Gln (exon 5) | Virchow-Robin spaces (enlarged perivascular spaces) white matter abnormalities | Papillary microcarcinoma in follicular adenoma (thyroid) [14], autism, developmental delay, lipoma, penile freckling, |
| 3 | c.540C>A; p.Y180X (exon 6) | Virchow-Robin spaces | Nodular goiter, lipoma, penile freckling |
| 4 | c.737C>T.p.Pro246Leu (exon 7) | n.d. | Autoimmune thyroid disease, haemangioma, penile freckling |
| 5 | c.209+5G>A (Intron 3) | White matter abnormalities | Developmental delay |
| 6 | c.445C>T; Gln149X (exon 5) | White matter abnormalities | Autoimmune thyroid disease, penile freckling, trichilemmoma |
| 7 | c.509G>A; pSer170Asn (exon 6) | n.d. | Penile freckling |
| 8 | heterozygous deletion (exon 1–2) | Pseudotumor cerebri, Ventriculoperitoneal shunt | Multiple gastrointestinal polyps, lipoma, hydronephrosis |
| 9 | partial deletion (exon 6) | White matter abnormalities | Penile freckling, muscle hypotonia, lipoma |
| 10 | c.697C>T; pArg233 *(exon 7) | n.d. | Two follicular adenoma (thyroid), lipoma |
| 11 | c.959T>G (p.Leu320 *) | Cavernoma | Thyroid adenoma, penile freckling, lipoma, developmental delay |
| 12 | c.987dup T (p.Lys330 *) (exon 8) | n.d. | Colloid cysts of thyroid, lipoma, haemangioma |
| 13 | c.(492+1_493-1)_(1026+1_1027-1)del | Focal cortical dysplasias | Moderate developmental delay, lipoma |
| 14 | heterozygous deletion PTEN and BMPR1A Gene | Arachnoid cysts left and right of the pineal region | Little lesions of left thyroidal lobe. Additional BMPR1A deletion, severe gastrointestinal disease, juvenile polyposis requiring colectomy, penile freckling, dilatative cardiomyopathy |
| 15 | c.800_801delAG (exon 7) | Enlarged periventricular spaces, Virchow-Robin spaces | Moderately reduced IQ, scoliosis, |
| Patient No. (Female) | Mutation in PTEN Gene (Localisation) | MRI Features | Add. Clinical Features (Except MC) |
| 1 | c.741dupA; p.Pro248Thrfs*5 (exon 7) | n.d. | Follicular carcinoma and microfollicular adenoma of thyroid, lipoma |
| 2 | c.302T>C; p.Ile101Thr (exon 5) | n.d. | Suspicious lesion in ultrasound screening of thyroid, developmental delay, trichilemmoma |
| 3 | c.762dupA;p.Val255Serfs*43 (exon 7) | White matter abnormalities | Lipoma, developmental delay, precocious puberty |
| 4 | c.49C>T;p.Gln17* (exon1) | Normal MRI Scan | Nodular goiter, lipoma |
| 5 | c.1008C>G;p.Tyr336* (exon 8) | n.d. | Suspicious lesion (hyper-perfusion, microcalcific.) of the thyroid, lipoma, developmental delay |
| 6 | c.492delG;p.Gly165Glufs*2 (exon 5) | Normal MRI Scan | Follicular nodule (thyroid), lipoma |
| 7 | c.1133_1136del.pArg378ilefs*37 (exon 9) | Dysmyelinisation, microgyria, Chiari malformation I | Developmental delay, muscle hypotonia, diarrhea |
| 8 | c.389G>A; p.(Arg130 Gln) (exon 5) | White matter abnormalities | Family history, muscle hypotonia, cutis laxa, developmental delay |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plamper, M.; Gohlke, B.; Schreiner, F.; Woelfle, J. Phenotype-Driven Diagnostic of PTEN Hamartoma Tumor Syndrome: Macrocephaly, But Neither Height nor Weight Development, Is the Important Trait in Children. Cancers 2019, 11, 975. https://doi.org/10.3390/cancers11070975
Plamper M, Gohlke B, Schreiner F, Woelfle J. Phenotype-Driven Diagnostic of PTEN Hamartoma Tumor Syndrome: Macrocephaly, But Neither Height nor Weight Development, Is the Important Trait in Children. Cancers. 2019; 11(7):975. https://doi.org/10.3390/cancers11070975
Chicago/Turabian StylePlamper, Michaela, Bettina Gohlke, Felix Schreiner, and Joachim Woelfle. 2019. "Phenotype-Driven Diagnostic of PTEN Hamartoma Tumor Syndrome: Macrocephaly, But Neither Height nor Weight Development, Is the Important Trait in Children" Cancers 11, no. 7: 975. https://doi.org/10.3390/cancers11070975