Prevalence of Human Papillomavirus (HPV) Infection and the Association with Survival in Saudi Patients with Head and Neck Squamous Cell Carcinoma

 ,
, 
Abstract
:1. Introduction
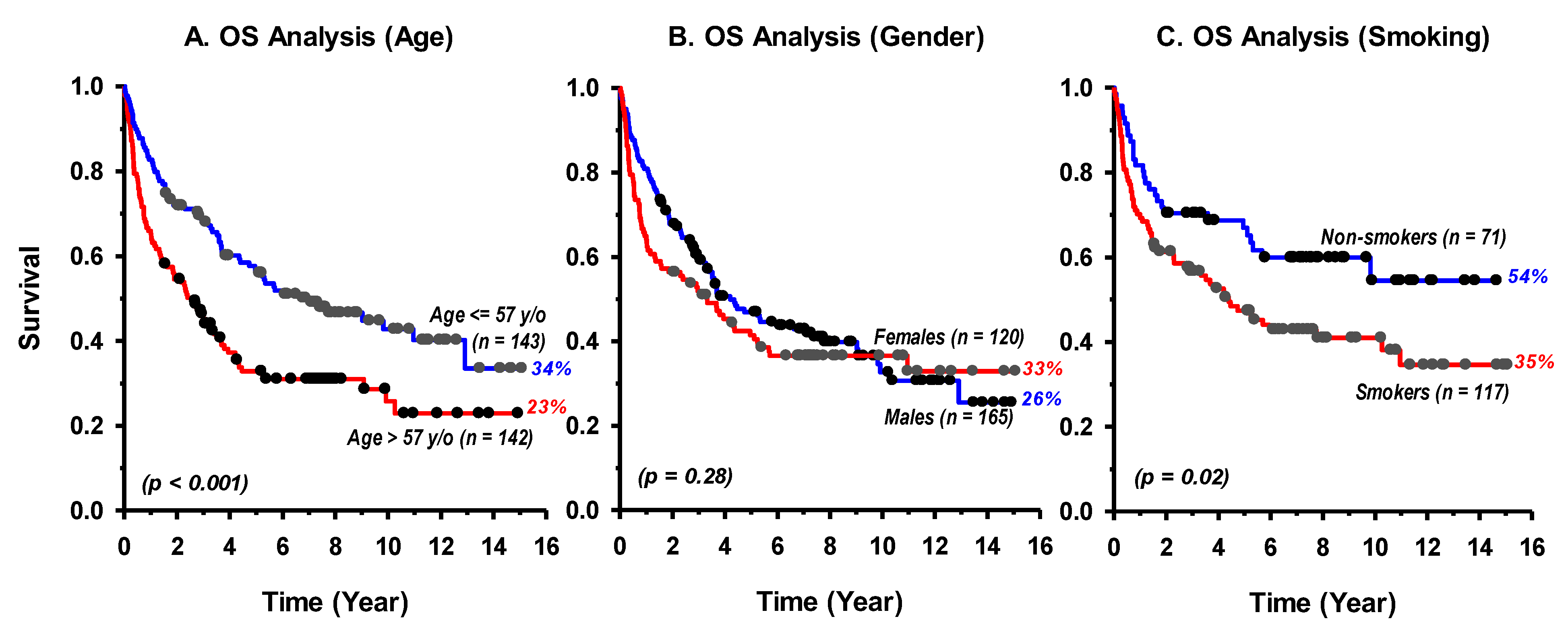
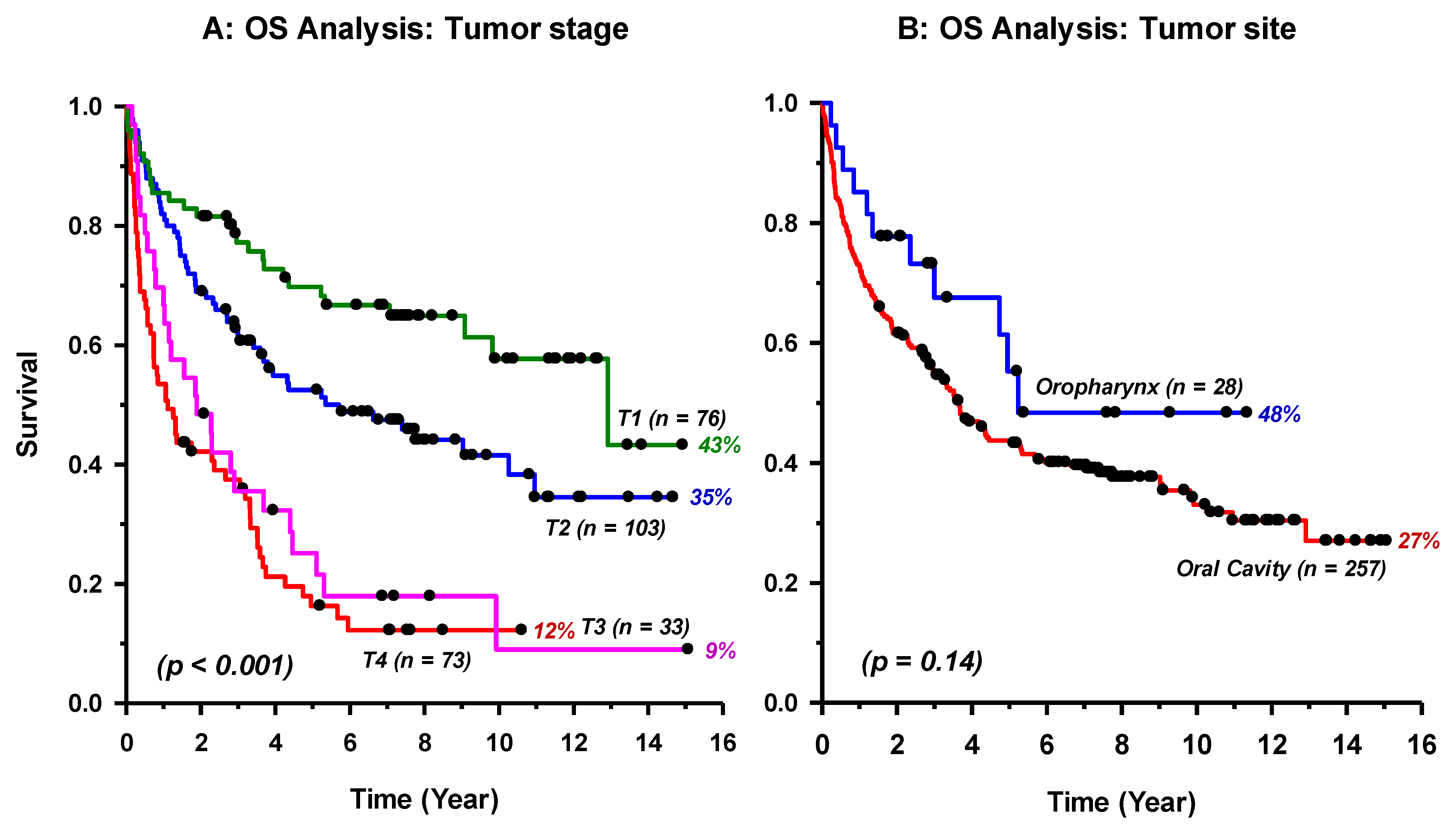
2. Results
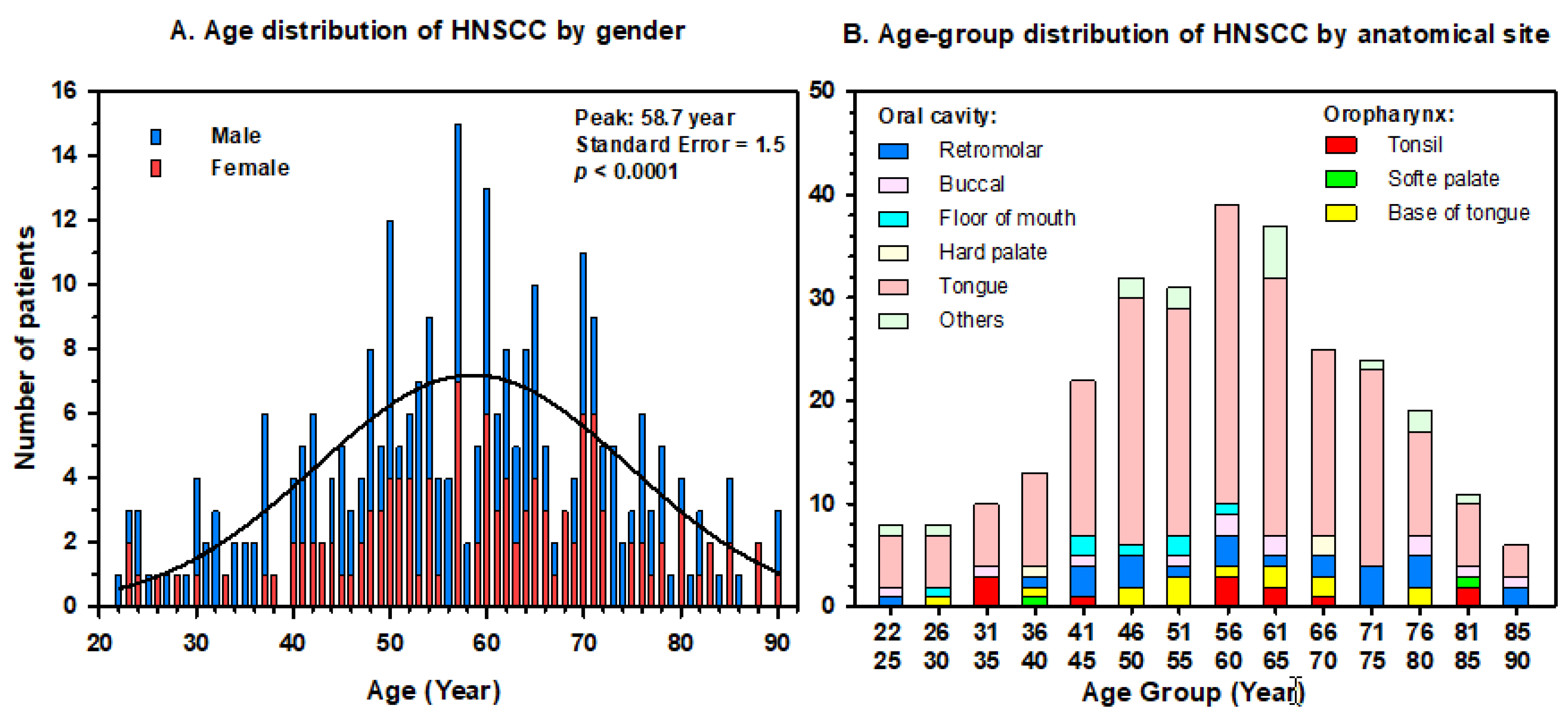
2.1. Patients and Clinical Data
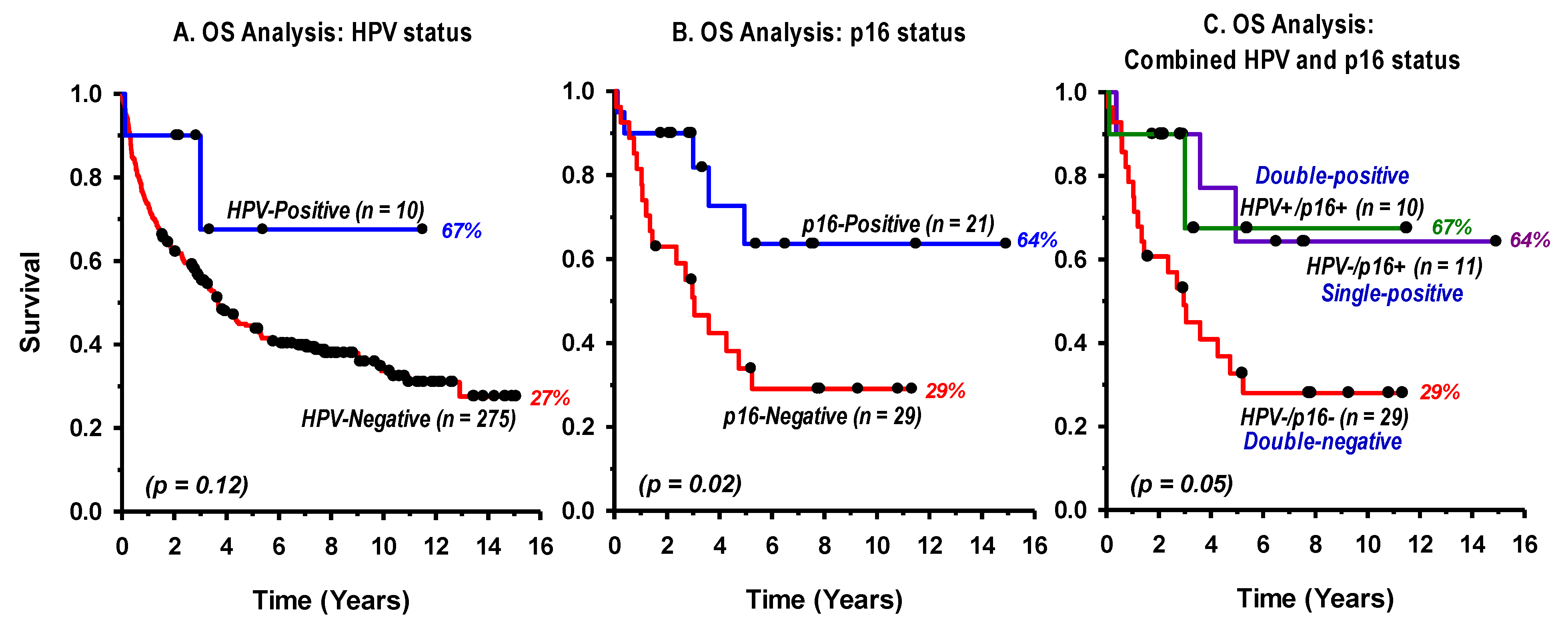
2.2. Detection of HPV Infection and Genotyping
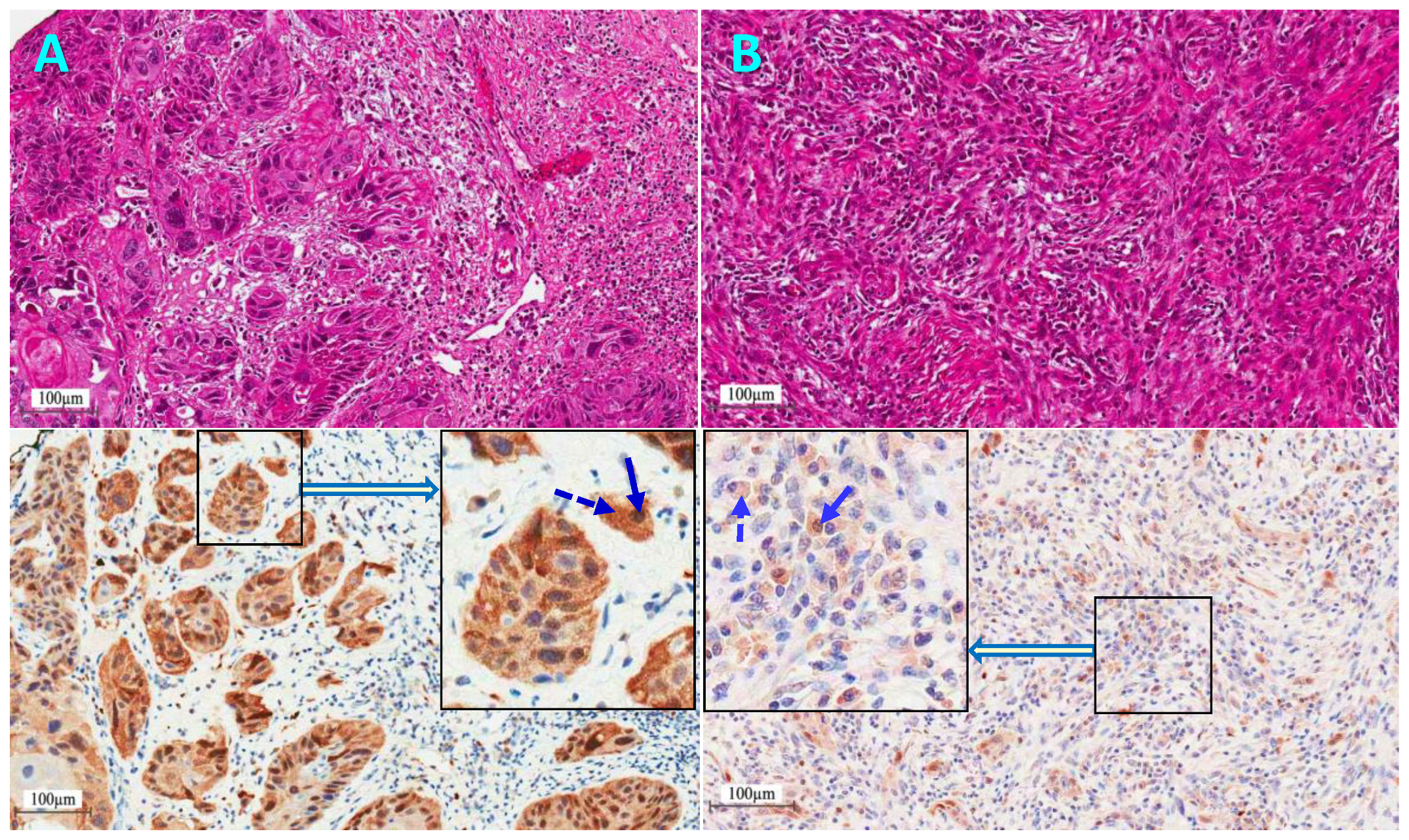
2.3. p16Ink4a Protein Immunohistochemical (IHC) Staining
3. Discussion
4. Materials and Methods
4.1. Ethical Considerations
4.2. Clinical Specimens
4.3. DNA Extraction
4.4. HPV Detection and Genotyping
4.5. Immunohistochemical (IHC) Staining of p16 Protein Expression
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Preston, R.; Lawson, F.; Rodriguez-Torres, S.; Noordhuis, M.G.; Pirini, F.; Manuel, L.; Valle, B.L.; Hadar, T.; Rivera, B.; Folawiyo, O.; et al. JAK3 Variant, Immune Signatures, DNA Methylation, and Social Determinants Linked to Survival Racial Disparities in Head and Neck Cancer Patients. Cancer Prev. Res. 2019, 12, 255–270. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Zanetti, R.; Ferlay, J. Cancer Incidence in Five Continents (2008-2012), electronic version; International Agency for Research on Cancer: Lyon, France, 2017; Volume XI. [Google Scholar]
- Cruz-Gregorio, A.; Martinez-Ramirez, I.; Pedraza-Chaverri, J.; Lizano, M. Reprogramming of Energy Metabolism in Response to Radiotherapy in Head and Neck Squamous Cell Carcinoma. Cancers 2019, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Al-Jaber, A.; Al-Nasser, L.; El-Metwally, A. Epidemiology of oral cancer in Arab countries. Saudi Med. J. 2016, 37, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Isayeva, T.; Li, Y.; Maswahu, D.; Brandwein-Gensler, M. Human papillomavirus in non-oropharyngeal head and neck cancers: A systematic literature review. Head. Neck. Pathol. 2012, 6 (Suppl. 1), S104–S120. [Google Scholar] [CrossRef]
- Termine, N.; Panzarella, V.; Falaschini, S.; Russo, A.; Matranga, D.; Lo Muzio, L.; Campisi, G. HPV in oral squamous cell carcinoma vs. head and neck squamous cell carcinoma biopsies: A meta-analysis (1988–2007). Ann. Oncol. 2008, 19, 1681–1690. [Google Scholar] [CrossRef]
- Serrano, B.; Brotons, M.; Bosch, F.X.; Bruni, L. Epidemiology and burden of HPV-related disease. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 14–26. [Google Scholar] [CrossRef]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV-associated head and neck cancer: A virus-related cancer epidemic. Lancet Oncol. 2010, 11, 781–789. [Google Scholar] [CrossRef]
- Ngan, H.L.; Wang, L.; Lo, K.W.; Lui, V.W.Y. Genomic Landscapes of EBV-Associated Nasopharyngeal Carcinoma vs. HPV-Associated Head and Neck Cancer. Cancers 2018, 10, 210. [Google Scholar] [CrossRef]
- Syrjanen, K.; Syrjanen, S.; Lamberg, M.; Pyrhonen, S.; Nuutinen, J. Morphological and immunohistochemical evidence suggesting human papillomavirus (HPV) involvement in oral squamous cell carcinogenesis. Int. J. Oral Surg. 1983, 12, 418–424. [Google Scholar] [CrossRef]
- Loning, T.; Ikenberg, H.; Becker, J.; Gissmann, L.; Hoepfer, I.; zur Hausen, H. Analysis of oral papillomas, leukoplakias, and invasive carcinomas for human papillomavirus type related DNA. J. Investig. Dermatol. 1985, 84, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Chaturvedi, A.K.; Anderson, W.F.; Fakhry, C. Epidemiology of Human Papillomavirus-Positive Head and Neck Squamous Cell Carcinoma. J. Clin. Oncol. 2015, 33, 3235–3242. [Google Scholar] [CrossRef] [PubMed]
- Sturgis, E.M.; Cinciripini, P.M. Trends in head and neck cancer incidence in relation to smoking prevalence: An emerging epidemic of human papillomavirus-associated cancers? Cancer 2007, 110, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, N.; Williams, M.D. Epidemiologic trends in head and neck cancer and aids in diagnosis. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 123–141. [Google Scholar] [CrossRef] [PubMed]
- Ndiaye, C.; Mena, M.; Alemany, L.; Arbyn, M.; Castellsague, X.; Laporte, L.; Bosch, F.X.; de Sanjose, S.; Trottier, H. HPV DNA, E6/E7 mRNA, and p16INK4a detection in head and neck cancers: A systematic review and meta-analysis. Lancet Oncol. 2014, 15, 1319–1331. [Google Scholar] [CrossRef]
- Nauta, I.H.; Rietbergen, M.M.; van Bokhoven, A.; Bloemena, E.; Witte, B.I.; Heideman, D.A.M.; Baatenburg de Jong, R.J.; Brakenhoff, R.H.; Leemans, C.R. Evaluation of the 8th TNM classification on p16-positive oropharyngeal squamous cell carcinomas in the Netherlands, and the importance of additional HPV DNA-testing. Ann. Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Fung, N.; Faraji, F.; Kang, H.; Fakhry, C. The role of human papillomavirus on the prognosis and treatment of oropharyngeal carcinoma. Cancer Metastasis Rev. 2017, 36, 449–461. [Google Scholar] [CrossRef]
- Dok, R.; Nuyts, S. HPV Positive Head and Neck Cancers: Molecular Pathogenesis and Evolving Treatment Strategies. Cancers 2016, 8, 41. [Google Scholar] [CrossRef]
- Wagner, S.; Sharma, S.J.; Wuerdemann, N.; Knuth, J.; Reder, H.; Wittekindt, C.; Klussmann, J.P. Human Papillomavirus-Related Head and Neck Cancer. Oncol. Res. Treat. 2017, 40, 334–340. [Google Scholar] [CrossRef]
- Lassen, P.; Eriksen, J.G.; Hamilton-Dutoit, S.; Tramm, T.; Alsner, J.; Overgaard, J. Effect of HPV-associated p16INK4A expression on response to radiotherapy and survival in squamous cell carcinoma of the head and neck. J. Clin. Oncol. 2009, 27, 1992–1998. [Google Scholar] [CrossRef]
- Deschuymer, S.; Dok, R.; Laenen, A.; Hauben, E.; Nuyts, S. Patient Selection in Human Papillomavirus Related Oropharyngeal Cancer: The Added Value of Prognostic Models in the New TNM 8th Edition Era. Front. Oncol. 2018, 8, 273. [Google Scholar] [CrossRef] [PubMed]
- Alsbeih, G. Exploring the Causes of the Low Incidence of Cervical Cancer in Western Asia. Asian Pac. J. Cancer Prev. 2018, 19, 1425–1429. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; Franklin, N.; Compton, N.; Robinson, M.; Powell, N.; Biswas-Baldwin, N.; Paleri, V.; Hartley, A.; Fresco, L.; Al-Booz, H.; et al. Geographic variation in human papillomavirus-related oropharyngeal cancer: Data from 4 multinational randomized trials. Head Neck 2016, 38 (Suppl. 1), E1863–E1869. [Google Scholar] [CrossRef]
- Al-Shahrani, Z.S.; Al-Rawaji, A.I.; Al-Madouj, A.N.; Hayder, M.S. Saudi Cancer Registry: Cancer Incidence Report Saudi Arabia 2014; Saudi Health Council: Riyadh, Saudi Arabia, 2017; pp. 1–82. [Google Scholar]
- Alsbeih, G. HPV Infection in Cervical and Other Cancers in Saudi Arabia: Implication for Prevention and Vaccination. Front. Oncol. 2014, 4, 65. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhang, H.; Xue, Y.; Wen, J.; Zhou, J.; Yang, X.; Wei, J. A systematic investigation of the association between HPV and the clinicopathological parameters and prognosis of oral and oropharyngeal squamous cell carcinomas. Cancer Med. 2017, 6, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Hesham, A.; Syed, K.; Jamal, B.; Alqahtani, A.; Alfaqih, A.; Alshehry, H.; Hameed, M.; Mustafa, A. Incidence, clinical presentation, and demographic factors associated with oral cancer patients in the southern region of Saudi Arabia: A 10-year retrospective study. J. Int. Oral Health 2017, 9, 105–109. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: A systematic review. Cancer Epidemiol. Prev. Biomarkers 2005, 14, 467–475. [Google Scholar] [CrossRef]
- Vidal Loustau, A.C.; Dulguerov, N.; Curvoisier, D.; McKee, T.; Lombardi, T. Low prevalence of HPV-induced oral squamous cell carcinoma in Geneva, Switzerland. Oral Dis. 2019. [Google Scholar] [CrossRef]
- Alsbeih, G.A.; Al-Harbi, N.M.; Bin Judia, S.S.; Khoja, H.A.; Shoukri, M.M.; Tulbah, A.M. Reduced rate of human papillomavirus infection and genetic overtransmission of TP53 72C polymorphic variant lower cervical cancer incidence. Cancer 2017, 123, 2459–2466. [Google Scholar] [CrossRef] [Green Version]
- Santegoets, L.A.; van Seters, M.; Heijmans-Antonissen, C.; Kleinjan, A.; van Beurden, M.; Ewing, P.C.; Kuhne, L.C.; Beckmann, I.; Burger, C.W.; Helmerhorst, T.J.; et al. Reduced local immunity in HPV-related VIN: Expression of chemokines and involvement of immunocompetent cells. Int. J. Cancer 2008, 123, 616–622. [Google Scholar] [CrossRef]
- Weinberger, P.M.; Yu, Z.; Haffty, B.G.; Kowalski, D.; Harigopal, M.; Brandsma, J.; Sasaki, C.; Joe, J.; Camp, R.L.; Rimm, D.L.; et al. Molecular classification identifies a subset of human papillomavirus—Associated oropharyngeal cancers with favorable prognosis. J. Clin. Oncol. 2006, 24, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tan, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Mehra, R.; Ang, K.K.; Burtness, B. Management of human papillomavirus-positive and human papillomavirus-negative head and neck cancer. Semin. Radiat. Oncol. 2012, 22, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Bussu, F.; Ragin, C.; Boscolo-Rizzo, P.; Rizzo, D.; Gallus, R.; Delogu, G.; Morbini, P.; Tommasino, M. HPV as a marker for molecular characterization in head and neck oncology: Looking for a standardization of clinical use and of detection method(s) in clinical practice. Head Neck 2019, 41, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Combes, J.D.; Franceschi, S. Role of human papillomavirus in non-oropharyngeal head and neck cancers. Oral Oncol. 2014, 50, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Zafereo, M.E.; Xu, L.; Dahlstrom, K.R.; Viamonte, C.A.; El-Naggar, A.K.; Wei, Q.; Li, G.; Sturgis, E.M. Squamous cell carcinoma of the oral cavity often overexpresses p16 but is rarely driven by human papillomavirus. Oral Oncol. 2016, 56, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albers, A.E.; Qian, X.; Kaufmann, A.M.; Coordes, A. Meta analysis: HPV and p16 pattern determines survival in patients with HNSCC and identifies potential new biologic subtype. Sci. Rep. 2017, 7, 16715. [Google Scholar] [CrossRef] [PubMed]
- Lop, J.; Garcia, J.; Lopez, M.; Taberna, M.; Mena, M.; Alemany, L.; Quer, M.; Leon, X. Competing mortality in oropharyngeal carcinoma according to human papillomavirus status. Head Neck 2019, 41, 1328–1334. [Google Scholar] [CrossRef]
- Lassen, P.; Primdahl, H.; Johansen, J.; Kristensen, C.A.; Andersen, E.; Andersen, L.J.; Evensen, J.F.; Eriksen, J.G.; Overgaard, J.; Danish, H.; et al. Impact of HPV-associated p16-expression on radiotherapy outcome in advanced oropharynx and non-oropharynx cancer. Radiother. Oncol. 2014, 113, 310–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.S.; Bindra, R.S.; Mo, A.; Hayman, T.; Husain, Z.; Contessa, J.N.; Gaffney, S.G.; Townsend, J.P.; Yu, J.B. CDKN2A Copy Number Loss Is an Independent Prognostic Factor in HPV-Negative Head and Neck Squamous Cell Carcinoma. Front. Oncol 2018, 8, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, G.; Vishnoi, K.; Tyagi, A.; Jadli, M.; Singh, T.; Goel, A.; Sharma, A.; Agarwal, K.; Prasad, S.C.; Pandey, D.; et al. Characterization of key transcription factors as molecular signatures of HPV-positive and HPV-negative oral cancers. Cancer Med. 2017, 6, 591–604. [Google Scholar] [CrossRef]
- Taberna, M.; Torres, M.; Alejo, M.; Mena, M.; Tous, S.; Marquez, S.; Pavon, M.A.; Leon, X.; Garcia, J.; Guix, M.; et al. The Use of HPV16-E5, EGFR, and pEGFR as Prognostic Biomarkers for Oropharyngeal Cancer Patients. Front. Oncol. 2018, 8, 589. [Google Scholar] [CrossRef] [PubMed]
- De Felice, F.; Polimeni, A.; Valentini, V.; Brugnoletti, O.; Cassoni, A.; Greco, A.; de Vincentiis, M.; Tombolini, V. Radiotherapy Controversies and Prospective in Head and Neck Cancer: A Literature-Based Critical Review. Neoplasia 2018, 20, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Chakravarthy, A.R.; Walter, V.; Masterson, L.; Feber, A.; Jay, A.; Weinberger, P.M.; McIndoe, R.A.; Forde, C.T.; Chester, K.; et al. Frequent HPV-independent p16/INK4A overexpression in head and neck cancer. Oral Oncol. 2018, 83, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mena, M.; Taberna, M.; Tous, S.; Marquez, S.; Clavero, O.; Quiros, B.; Lloveras, B.; Alejo, M.; Leon, X.; Quer, M.; et al. Double positivity for HPV-DNA/p16(ink4a) is the biomarker with strongest diagnostic accuracy and prognostic value for human papillomavirus related oropharyngeal cancer patients. Oral Oncol. 2018, 78, 137–144. [Google Scholar] [CrossRef]
- Gregoire, V.; Lefebvre, J.L.; Licitra, L.; Felip, E.; EHNS–ESMO–ESTRO guidelines working group. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21 (Suppl. 5), v184–v186. [Google Scholar] [CrossRef] [PubMed]
- Alsbeih, G.; Ahmed, R.; Al-Harbi, N.; Venturina, L.A.; Tulbah, A.; Balaraj, K. Prevalence and genotypes’ distribution of human papillomavirus in invasive cervical cancer in Saudi Arabia. Gynecol. Oncol. 2011, 121, 522–526. [Google Scholar] [CrossRef]
- Barasch, S.; Mohindra, P.; Hennrick, K.; Hartig, G.K.; Harari, P.M.; Yang, D.T. Assessing p16 Status of Oropharyngeal Squamous Cell Carcinoma by Combined Assessment of the Number of Cells Stained and the Confluence of p16 Staining: A Validation by Clinical Outcomes. Am. J. Surg. Pathol. 2016, 40, 1261–1269. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Site (ICD Code) | Number of Cases | Age Median (Range) | Gender | Smoking * | Tumor Stage | Treatment | HPV | p16 |
|---|---|---|---|---|---|---|---|---|
| Oropharynx: | ||||||||
| Tonsil (C09) | 12 | 60 (31–83) | M: 9 F: 3 | Yes: 4 No: 5 N/A: 3 | T1–2: 6 (N0: 2, N+: 4, M0: 6) T3–4: 6 (N0: 5, N+: 1, M0: 6) | S: 1, S+RT: 5 CRT: 4, S+RT: 2 | P: 3 (HPV16) N: 9 | P: 4 N: 8 N/A: 0 |
| Soft palate (C05.1) | 2 | 61 (37–85) | M: 2 F: 0 | Yes: 1 No: 0 N/A: 1 | T1–2: 0 (N0: 0, N+: 0, M0: 0) T3–4: 2 (N0: 2, N+: 0, M0:2) | S+CRT: 2 | P: 0 N: 2 | P: 0 N: 2 N/A: 0 |
| Base of tongue C01 | 14 | 54 (27–78) | M: 7 F: 7 | Yes: 7 No: 5 N/A: 2 | T1–2: 8 (N0: 3, N+: 5, M0: 8) T3–4: 6 (N0: 0, N+: 6, M0: 6) | S: 2, S+RT: 5, S+CRT: 1 S+RT: 1, CRT: 3, S+CRT: 2 | P: 3 (HPV16) N: 11 | P: 7 N: 7 N/A: 0 |
| Oral Cavity: | ||||||||
| Retromolar C06.2 | 24 | 62 (24–90) | M: 16 F: 8 | Yes: 11 No: 8 N/A: 5 | T1–2: 11 (N0: 6, N+: 5, M0: 11) T3–4: 13 (N0: 1, N+: 12, M0: 13) | S: 3, S+RT: 5, CRT: 1, S+CRT: 2 S+RT: 1, CRT: 1, S+CRT: 11 | P: 2 (HPV16) N: 22 | P: 5 N: 5 N/A: 14 |
| Tongue C02 | 198 | 57 (22–90) | M: 113 F: 85 | Yes: 82 No: 45 N/A: 71 | T1–2: 134 (N0: 84, N+: 51, M0: 134) T3–4: 64 (N0: 24, N+: 39, M0: 64) | S: 62, S+RT: 56, S+CRT: 16 CRT: 1, S+RT: 13, S+CRT: 50 | P: 1 (HPV33) N: 197 | P: 4 N: 6 N/A: 188 |
| Buccal (C06) | 19 | 62 (24–90) | M: 9 F: 10 | Yes: 7 No: 3 N/A: 9 | T1–2: 11 (N0: 6, N+: 5, M0: 11) T3–4: 8 (N0: 4, N+: 4, M0: 8) | S: 4, S+RT: 7 S+RT: 3, S+CRT: 5 | P: 1 (HPV16) N: 18 | P: 1 N: 1 N/A: 17 |
| Floor of mouth (C04) | 13 | 49 (25–82) | M: 7 F: 6 | Yes: 4 No: 5 N/A: 4 | T1–2: 8 (N0: 6, N+: 2, M0: 8) T3–4: 5 (N0:2, N+: 3, M0: 5) | S: 5, S+RT: 3 S+RT: 1, S+CRT: 4 | P: 0 N: 13 | N/A: 13 |
| Hard palate (C05.0) | 3 | 66 (37–69) | M: 2 F: 1 | Yes: 1 No: 0 N/A: 2 | T1–2: 1 (N0: 1, N+: 0, M0: 1) T3–4: 2 (N0: 2, N+: 0, M0: 2) | S+RT: 1 S+RT: 1, S+CRT: 1 | P: 0 N: 3 | P: 0 N: 0 N/A: 3 |
| All cases | 285 | 57 (22–90) | M: 165 F: 120 | Yes: 117 No: 71 N/A: 97 | T1–2: 179 (N0: 107, N+: 72, M0: 179) T3–4: 106 (N0: 41, N+: 65, M0: 106) | S: 77, CRT: 1, S+RT: 82, S+CRT: 19 CRT: 9, S+RT: 22, S+CRT: 75 | P: 10 (3.5%) N: 275 (96.5%) | P: 21 (42%) ** N: 29 (58 %) ** N/A: 238 |
| Risk Factors | Categories | HR | 95%CI | p Value |
|---|---|---|---|---|
| Age | Younger * | 0.57 | 0.38–0.87 | 0.009 |
| Gender | Females | 1.01 | 0.66–1.55 | 0.963 |
| Smoking | Non-smokers | 0.77 | 0.48–1.22 | 0.258 |
| Tumor site | Oropharynx | 0.71 | 0.31–1.63 | 0.422 |
| Tumor stage | Early (T1–2) | 0.53 | 0.33–0.83 | 0.005 |
| Treatment | Surgery ** | 0.40 | 0.20–0.77 | 0.006 |
| HPV/p16 status | Positive | 0.38 | 0.11–1.28 | 0.118 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsbeih, G.; Al-Harbi, N.; Bin Judia, S.; Al-Qahtani, W.; Khoja, H.; El-Sebaie, M.; Tulbah, A. Prevalence of Human Papillomavirus (HPV) Infection and the Association with Survival in Saudi Patients with Head and Neck Squamous Cell Carcinoma. Cancers 2019, 11, 820. https://doi.org/10.3390/cancers11060820
Alsbeih G, Al-Harbi N, Bin Judia S, Al-Qahtani W, Khoja H, El-Sebaie M, Tulbah A. Prevalence of Human Papillomavirus (HPV) Infection and the Association with Survival in Saudi Patients with Head and Neck Squamous Cell Carcinoma. Cancers. 2019; 11(6):820. https://doi.org/10.3390/cancers11060820
Chicago/Turabian StyleAlsbeih, Ghazi, Najla Al-Harbi, Sara Bin Judia, Wejdan Al-Qahtani, Hatim Khoja, Medhat El-Sebaie, and Asma Tulbah. 2019. "Prevalence of Human Papillomavirus (HPV) Infection and the Association with Survival in Saudi Patients with Head and Neck Squamous Cell Carcinoma" Cancers 11, no. 6: 820. https://doi.org/10.3390/cancers11060820