Influence of Vitamin D in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
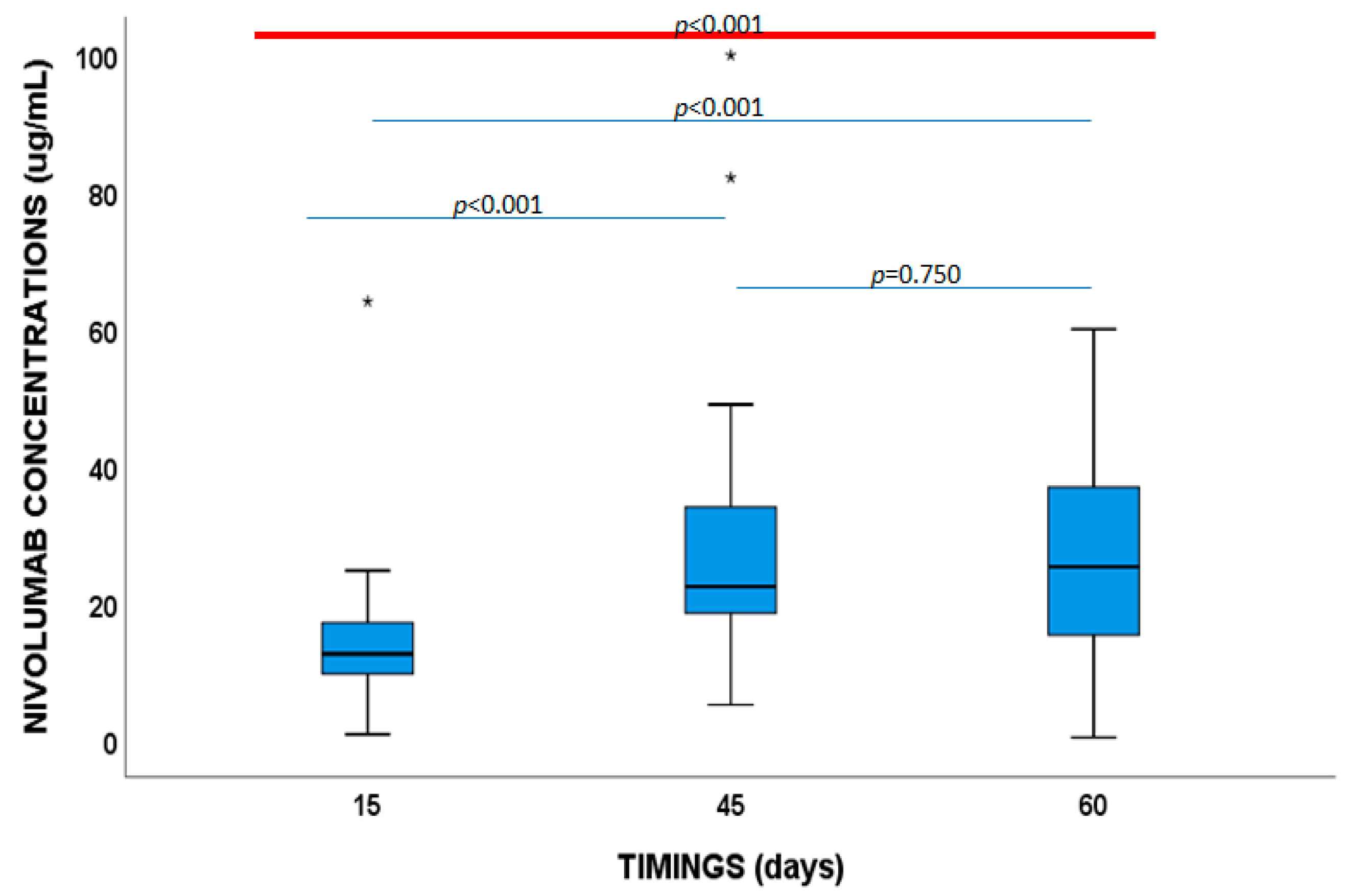
2.2. Nivolumab and Vitamin D Concentrations
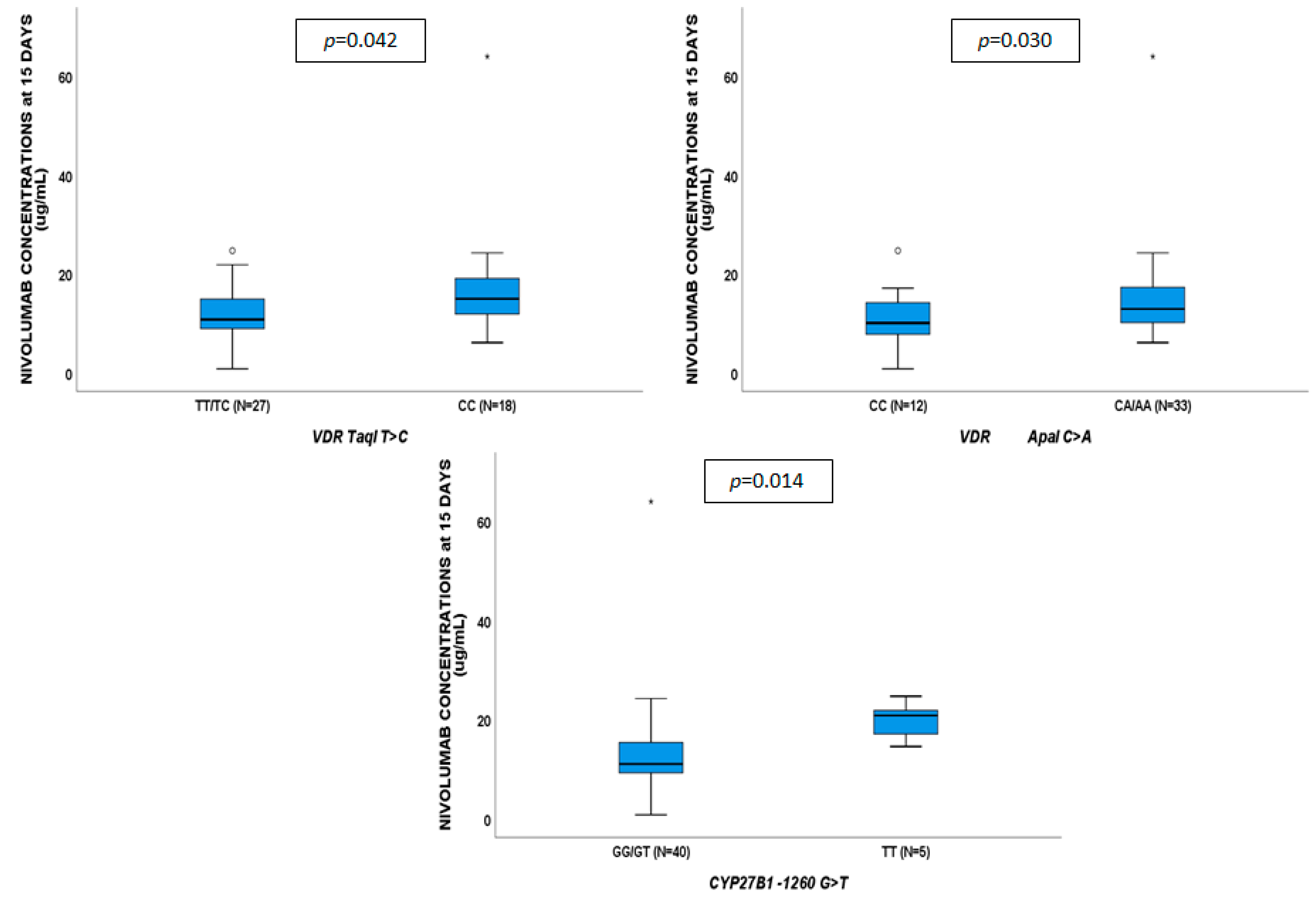
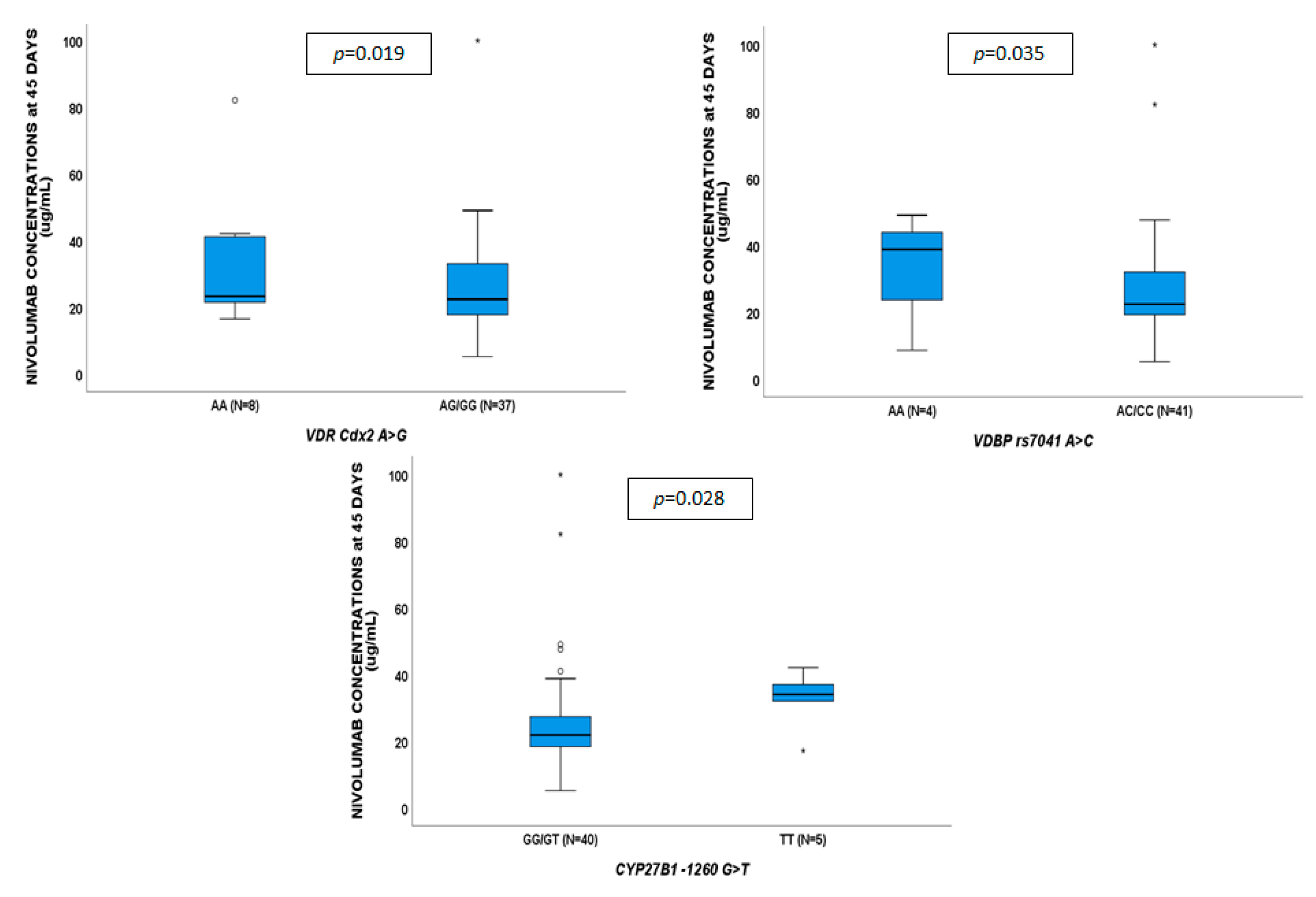
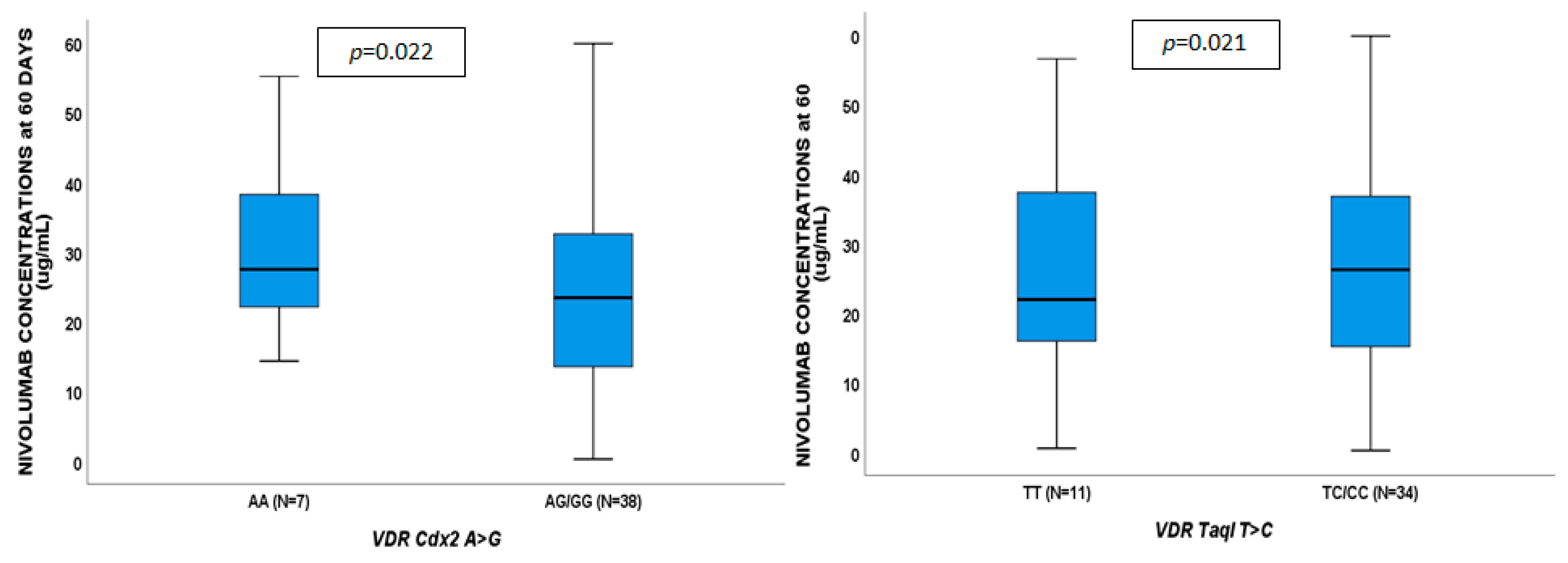
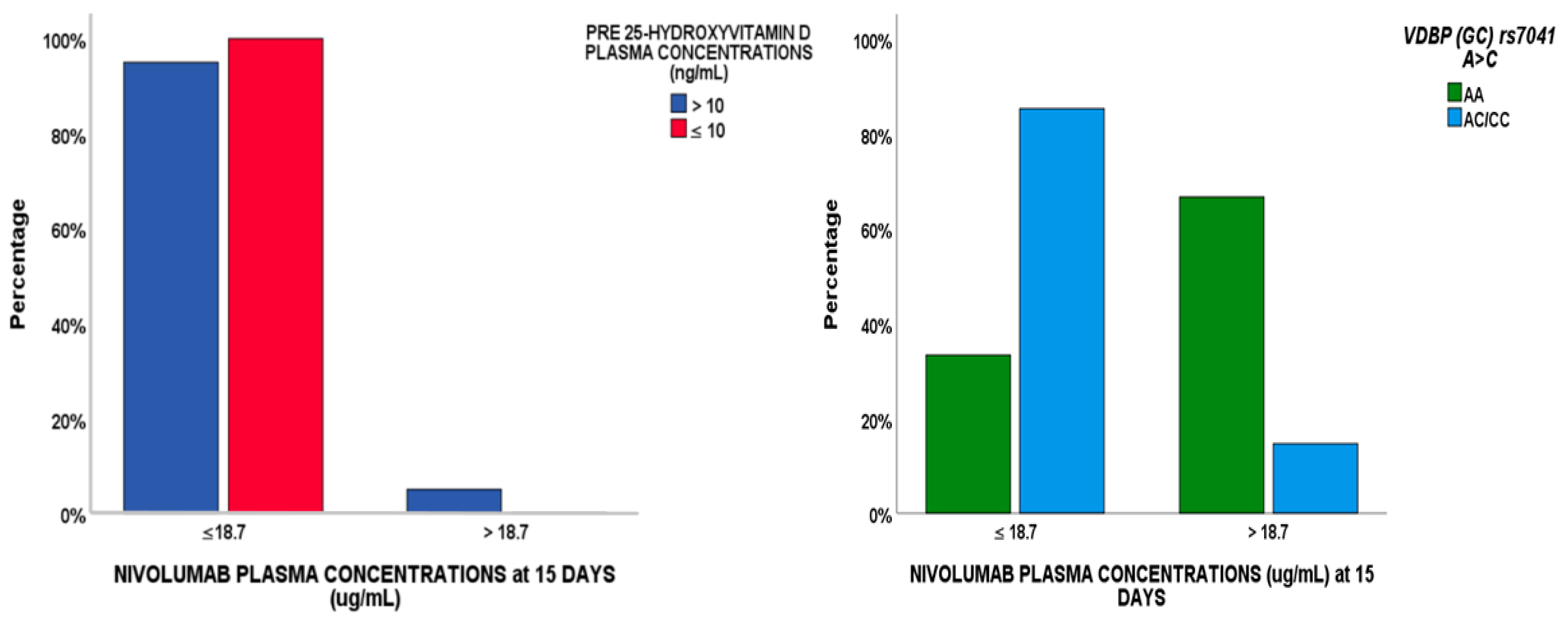
2.3. Pharmacogenetics
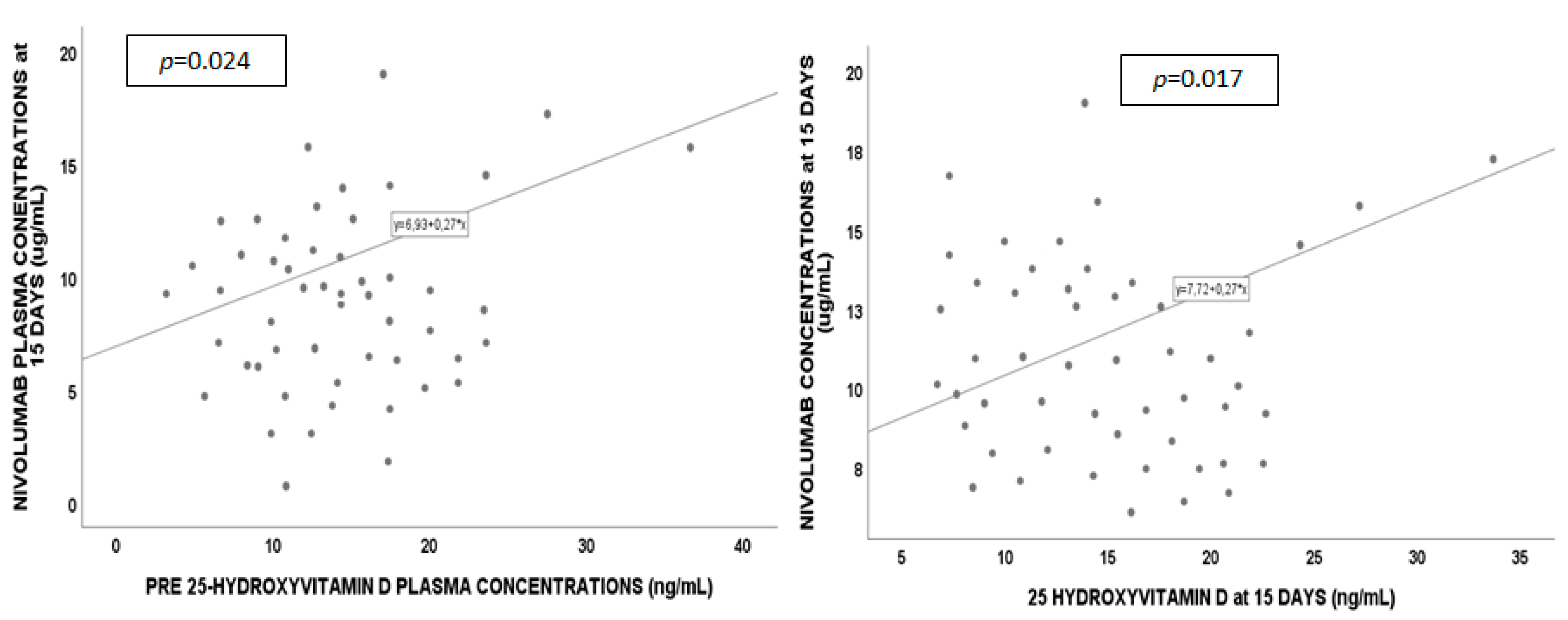
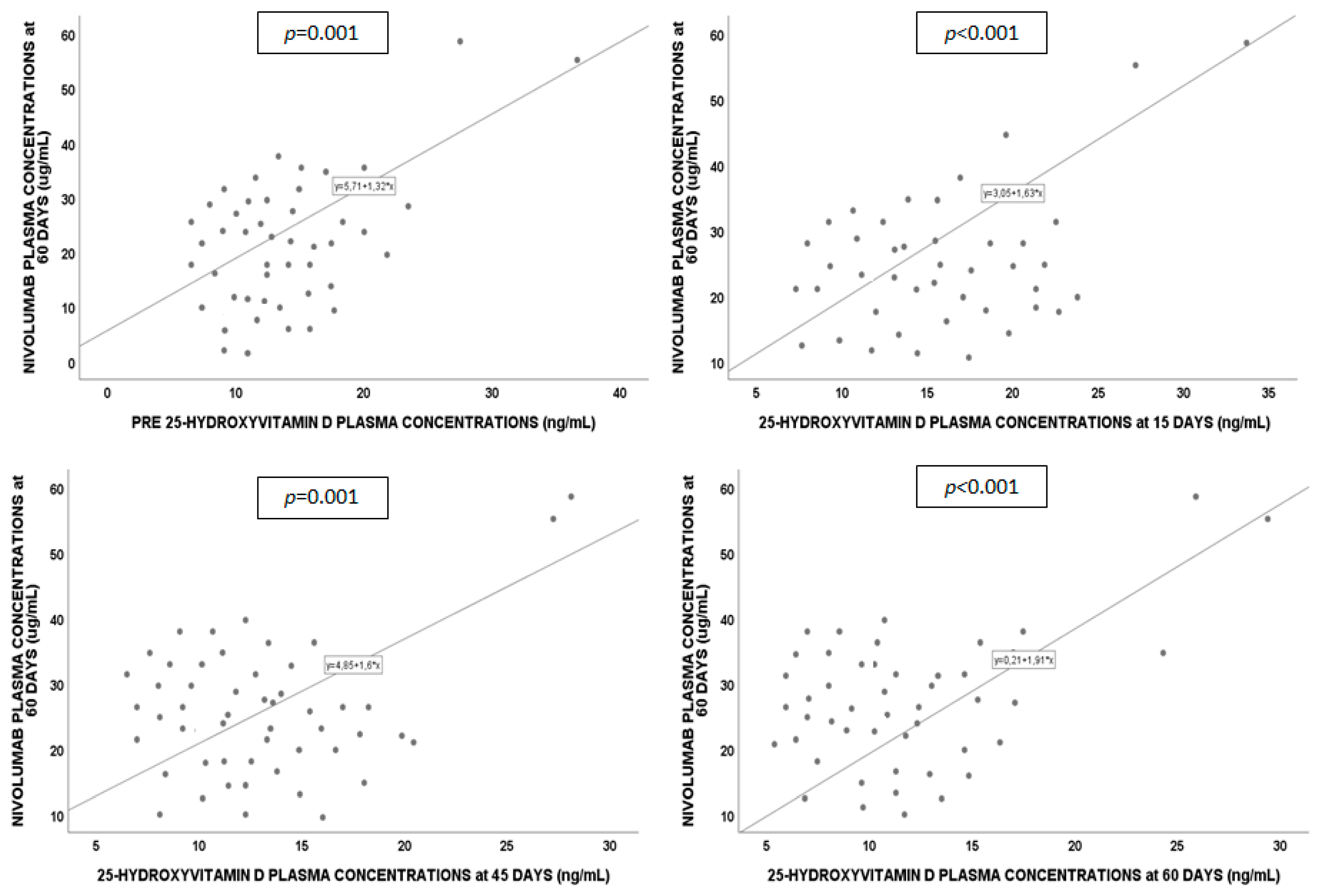
2.4. Regression Analysis
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Couzin-Frankel, J. Breakthrough of the year 2013. Cancer immunotherapy. Science 2013, 342, 1432–1433. [Google Scholar] [CrossRef] [PubMed]
- Alsaab, H.O.; Sau, S.; Alzhrani, R.; Tatiparti, K.; Bhise, K.; Kashaw, S.K.; Iyer, A.K. PD-1 and PD-L1 checkpoint signaling inhibition for cancer immunotherapy: Mechanism, combinations, and clinical outcome. Front. Pharm. 2017, 8, 561. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Lin, J.; Liao, G.; Tian, Y.; Liang, Y.; Li, R.; Liu, M.; Yuan, Y. Comparative analysis of immune checkpoint inhibitors and chemotherapy in the treatment of advanced non-small cell lung cancer: A meta-analysis of randomized controlled trials. Medicine (Baltimore) 2018, 97, e11936. [Google Scholar] [CrossRef] [PubMed]
- Tykodi, S.S.; Schadendorf, D.; Cella, D.; Reck, M.; Harrington, K.; Wagner, S.; Shaw, J.W. Patient-reported outcomes with nivolumab in advanced solid cancers. Cancer Treat. Rev. 2018, 70, 75–87. [Google Scholar] [CrossRef] [PubMed]
- (FDA) FaDA. FDA Grants Nivolumab Accelerated Approval for Third-Line Treatment of Metastatic Small Cell Lung Cancer; Food and Drug Administration: Silver Spring, MD, USA, 2015.
- Koolen, S.L.W.; Basak, E.A.; Hurkmans, D.; Schreurs, M.W.J.; Bins, S.; Oomen De Hoop, E.; Wijkhuis, A.J.M.; Den Besten, I.; Sleijfer, S.; Debets, R.; et al. Correlation between nivolumab exposure and treatment outcome in NSCLC. In Proceedings of the 2018 ASCO Annual Meeting, Chicago, IL, USA, 1–5 June 2018. [Google Scholar]
- Michot, J.M.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel-Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur. J. Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Statkevich, P.; Bajaj, G.; Feng, Y.; Saeger, S.; Desai, D.D.; Park, J.S.; Waxman, I.M.; Roy, A.; Gupta, M. Evaluation of immunogenicity of nivolumab monotherapy and its clinical relevance in patients with metastatic solid tumors. J. Clin. Pharmacol. 2017, 57, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Bersanelli, M.; Leonetti, A.; Buti, S. The link between calcitriol and anticancer immunotherapy: vitamin D as the possible balance between inflammation and autoimmunity in the immune-checkpoint blockade. Immunotherapy 2017, 9, 1127–1131. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Zhang, F.; Richards, J.B.; Kestenbaum, B.; Van Meurs, J.B.; Berry, D.; Kiel, D.P.; Streeten, E.A.; Ohlsson, C.; Koller, D.L.; et al. Common genetic determinants of vitamin D insufficiency: A genome-wide association study. Lancet 2010, 376, 180–188. [Google Scholar] [CrossRef]
- Ma, K.; Xu, W.; Wang, C.; Li, B.; Su, K.; Li, W. Vitamin D deficiency is associated with a poor prognosis in advanced non-small cell lung cancer patients treated with platinum-based first-line chemotherapy. Cancer Biomark. 2017, 18, 297–303. [Google Scholar] [CrossRef]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: Two-year outcomes from two randomized, open-label, phase III trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef]
- Aguiar, P.N., Jr.; Perry, L.A.; Penny-Dimri, J.; Babiker, H.; Tadokoro, H.; De Mello, R.A.; Lopes, G.L., Jr. The effect of PD-L1 testing on the cost-effectiveness and economic impact of immune checkpoint inhibitors for the second-line treatment of NSCLC. Ann. Oncol. 2017, 28, 2256–2263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matter-Walstra, K.; Schwenkglenks, M.; Aebi, S.; Dedes, K.; Diebold, J.; Pietrini, M.; Klingbiel, D.; Von Moos, R.; Gautschi, O. A cost-effectiveness analysis of nivolumab versus docetaxel for advanced nonsquamous NSCLC including PD-L1 testing. J. Thorac. Oncol. 2016, 11, 1846–1855. [Google Scholar] [CrossRef] [PubMed]
- Bochen, F.; Balensiefer, B.; Korner, S.; Bittenbring, J.T.; Neumann, F.; Koch, A.; Bumm, K.; Marx, A.; Wemmert, S.; Papaspyrou, G.; et al. Vitamin D deficiency in head and neck cancer patients-prevalence, prognostic value and impact on immune function. Oncoimmunology 2018, 7, e1476817. [Google Scholar] [CrossRef]
- Feng, Q.; Zhang, H.; Dong, Z.; Zhou, Y.; Ma, J. Circulating 25-hydroxyvitamin D and lung cancer risk and survival: A dose-response meta-analysis of prospective cohort studies. Medicine (Baltimore) 2017, 96, e8613. [Google Scholar] [CrossRef] [PubMed]
- Smolders, J.; Menheere, P.; Thewissen, M.; Peelen, E.; Tervaert, J.W.; Hupperts, R.; Damoiseaux, J. Regulatory T cell function correlates with serum 25-hydroxyvitamin D, but not with 1,25-dihydroxyvitamin D, parathyroid hormone and calcium levels in patients with relapsing remitting multiple sclerosis. J. Steroid Biochem. Mol. Biol. 2010, 121, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Fu, L.; Juras, D.J.; Karmali, M.; Wong, B.Y.; Gozdzik, A.; Cole, D.E. Common variants of the vitamin D binding protein gene and adverse health outcomes. Crit. Rev. Clin. Lab. Sci. 2013, 50, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, T.O.; Zhang, J.H.; Parra, E.; Ellis, B.K.; Simpson, C.; Lee, W.M.; Balko, J.; Fu, L.; Wong, B.Y.; Cole, D.E. Vitamin D binding protein is a key determinant of 25-hydroxyvitamin D levels in infants and toddlers. J. Bone Miner. Res. 2013, 28, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.N.; Cotterchio, M.; Cole, D.E.; Knight, J.A. Vitamin D-related genetic variants, interactions with vitamin D exposure, and breast cancer risk among Caucasian women in Ontario. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1708–1717. [Google Scholar] [CrossRef]
- Lafi, Z.M.; Irshaid, Y.M.; El-Khateeb, M.; Ajlouni, K.M.; Hyassat, D. Association of rs7041 and rs4588 polymorphisms of the vitamin D binding protein and the rs10741657 polymorphism of CYP2R1 with vitamin D status among Jordanian patients. Genet. Test Mol. Biomar. 2015, 19, 629–636. [Google Scholar] [CrossRef]
- Daffara, V.; Verdoia, M.; Rolla, R.; Nardin, M.; Marino, P.; Bellomo, G.; Carriero, A.; De Luca, G. Impact of polymorphism rs7041 and rs4588 of Vitamin D Binding Protein on the extent of coronary artery disease. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 775–783. [Google Scholar] [CrossRef]
- Schmid, S.; Diem, S.; Li, Q.; Krapf, M.; Flatz, L.; Leschka, S.; Desbiolles, L.; Klingbiel, D.; Jochum, W.; Fruh, M. Organ-specific response to nivolumab in patients with non-small cell lung cancer (NSCLC). Cancer Immunol. Immunother. 2018, 67, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Du Prel, J.B.; Rohrig, B.; Hommel, G.; Blettner, M. Choosing statistical tests: Part 12 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2010, 107, 343–348. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%), Median (IQR) | |
|---|---|---|
| n | 45 | |
| Age (years) | 73 (65–79.5) | |
| Male sex | 31 (69) | |
| BMI (Kg/m2) | 23.4 (20.1–26.4) | |
| Caucasian | 45 (100) | |
| NSCLC type | Adenocarcinoma | 34 (52.3) |
| Squamous cell carcinoma | 9 (13.8) | |
| Poorly differentiated carcinoma | 1 (1.5) | |
| Large-cell neuroendocrine carcinoma | 1 (1.5) | |
| Concomitant drugs | Cardiovascular | 24 (36.9) |
| Diabetes | 4 (6.2) | |
| Opioids | 9 (13.8) | |
| Protease inhibitors | 20 (30.8) | |
| Corticosteroid | 12 (18.5) | |
| Vitamin D | 2 (3.1) | |
| Pre-treatment drugs | Cisplatine | 24 (53.3) |
| Docetaxel | 10 (22.2) | |
| Carboplatine | 24 (53.3) | |
| Gemcitabine | 12 (26.7) | |
| Gefitinib | 2 (4.4) | |
| Pemetrexed | 30 (66.7) | |
| Afatinib | 1 (2.2) | |
| Osimertinib | 1 (2.2) | |
| Erlotinib | 20 (44.4) | |
| Vinorelbine | 10 (22.2) | |
| Paclitaxel | 3 (6.7) | |
| Bevacizumab | 3 (6.7) | |
| Etoposide | 4 (8.9) | |
| Zoledronic acid | 1 (2.2) | |
| Bavicizumab | 1 (2.2) | |
| Farletuzumab | 1 (2.2) | |
| Radiotherapy | 1 (2.2) | |
| Single Nucleotide Polymorphism (SNP) | % Homozigous Wild Type | % Heterozygous | % Homozygous Mutant |
|---|---|---|---|
| CYP27B1 +2838 C > T | 20 CC | 2.2 CT | 77.8 TT |
| CYP27B1 −1260 G > T | 73.3 CC | 15.6 CT | 11.1 TT |
| CYP24A1 rs2248359 T > C | 42.2 TT | 40 TC | 17.8 CC |
| CYP24A1 rs927650 C > T | 33.3 CC | 22.2 CT | 44.5 TT |
| CYP24A1 rs2585428 A > G | 31.1 AA | 28.9 AC | 40 CC |
| VDR Cdx2 A > G | 17.8 AA | 13.3 AG | 68.9 GG |
| VDR TaqI T > C | 33.3 TT | 26.7 TC | 40 CC |
| VDR FokI T > C | 11.1 TT | 42.2 TC | 46.7 CC |
| VDR BsmI G > A | 42.2 GG | 57.8 GA | - |
| VDR ApaI C > A | 26.7 CC | 28.9 CA | 44.4 AA |
| VDBP rs7041 T > G | 6.7 TT | 62.2 TG | 31.1 GG |
| Variables | Nivolumab Concentrations ≤ 18.7 μg/mL | |||
|---|---|---|---|---|
| Univariate | Multivariate | |||
| p-Value | OR (95% IC) | p-Value | OR (95% IC) | |
| BMI < 25 Kg/m2 | 0.766 | 1.270 (0.392–6.112) | ||
| Age > 60 years | 0.939 | 0.970 (0.091–9.145) | ||
| Gender (male) | 0.213 | 2.260 (0.692–12.419) | ||
| Drug dosage < 200 mg | 0.945 | 1.056 (0.099–4.867) | ||
| VDBP (GC) AC/CC | 0.059 | 11.667 (0.909–149.700) | 0.049 | 10.667 (0.830–137.145) |
| CYP24A1 3999 CC | NC | |||
| VDR TaqI TC/CC | 0.164 | 3.077 (0.632–14.976) | ||
| CYP27B1 -1260 GG | 0.148 | 3.250 (0.658–16.040) | ||
| Pre 25-hydroxyvitamin D levels | NC | NC | ||
| Pre 1,25-hydroxyvitamin D levels | 0.124 | 3.840 (0.692–21.312) | ||
| Adenocarcinoma NSCLC type | NC | |||
| Squamous cell carcinoma | NC | |||
| Cisplatine pre-treatment | 0.093 | 4.442 (0.852–24.853) | ||
| Carboplatine pre-treatment | 0.190 | 0.300 (0.051–1.854) | ||
| Pemetrexed pre-treatment | NC | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cusato, J.; Genova, C.; Tomasello, C.; Carrega, P.; Ottonello, S.; Pietra, G.; Mingari, M.C.; Cossu, I.; Rijavec, E.; Leggieri, A.; et al. Influence of Vitamin D in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab. Cancers 2019, 11, 125. https://doi.org/10.3390/cancers11010125
Cusato J, Genova C, Tomasello C, Carrega P, Ottonello S, Pietra G, Mingari MC, Cossu I, Rijavec E, Leggieri A, et al. Influence of Vitamin D in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab. Cancers. 2019; 11(1):125. https://doi.org/10.3390/cancers11010125
Chicago/Turabian StyleCusato, Jessica, Carlo Genova, Cristina Tomasello, Paolo Carrega, Selene Ottonello, Gabriella Pietra, Maria Cristina Mingari, Irene Cossu, Erika Rijavec, Anna Leggieri, and et al. 2019. "Influence of Vitamin D in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab" Cancers 11, no. 1: 125. https://doi.org/10.3390/cancers11010125