Associations of Epstein-Barr Virus-Positive Gastric Adenocarcinoma with Circulating Mediators of Inflammation and Immune Response

 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Patients and Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuzushima, K.; Nakamura, S.; Nakamura, T.; Yamamura, Y.; Yokoyama, N.; Fujita, M.; Kiyono, T.; Tsurumi, T. Increased frequency of antigen-specific CD8(+) cytotoxic t lymphocytes infiltrating an epstein-barr virus-associated gastric carcinoma. J. Clin. Investig. 1999, 104, 163–171. [Google Scholar] [CrossRef] [PubMed]
- van Beek, J.; zur Hausen, A.; Kranenbarg, E.K.; van de Velde, C.J.H.; Middeldorp, J.M.; van den Brule, A.J.C.; Meijer, C.J.L.M.; Bloemena, E. EBV-positive gastric adenocarcinomas: A distinct clinicopathologic entity with a low frequency of lymph node involvement. J. Clin. Oncol. 2004, 22, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Gourzones, C.; Barjon, C.; Busson, P. Host-tumor interactions in nasopharyngeal carcinomas. Semin. Cancer Biol. 2012, 22, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.P.; Hao, S.P.; Chang, J.H.; Wu, C.C.; Tsang, N.M.; Lee, Y.S.; Hsu, C.L.; Ueng, S.H.; Liu, S.C.; Liu, Y.L.; et al. Macrophage inflammatory protein-3alpha is a novel serum marker for nasopharyngeal carcinoma detection and prediction of treatment outcomes. Clin. Cancer Res. 2008, 14, 6979–6987. [Google Scholar] [CrossRef] [PubMed]
- Hsin, L.J.; Kao, H.K.; Chen, I.H.; Tsang, N.M.; Hsu, C.L.; Liu, S.C.; Chang, Y.S.; Chang, K.P. Serum CXCL9 levels are associated with tumor progression and treatment outcome in patients with nasopharyngeal carcinoma. PLoS ONE 2013, 8, e80052. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.J.; Chapuy, B.; Jing, O.Y.; Sun, H.H.; Roemer, M.G.M.; Xu, M.L.; Yu, H.B.; Fletcher, C.D.M.; Freeman, G.J.; Shipp, M.A.; et al. PD-L1 expression is characteristic of a subset of aggressive B-cell lymphomas and virus-associated malignancies. Clin. Cancer Res. 2013, 19, 3462–3473. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.; Zhang, J.; Hong, S.; Zhan, J.; Chen, N.; Qin, T.; Tang, Y.; Zhang, Y.; Kang, S.; Zhou, T.; et al. EBV-driven LMP1 and IFN-gamma up-regulate PD-L1 in nasopharyngeal carcinoma: Implications for oncotargeted therapy. Oncotarget 2014, 5, 12189–12202. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Yeh, T.H.; Lai, H.C.; Wu, S.Y.; Su, I.J.; Takada, K.; Chang, Y. Epstein-Barr virus Zta-induced immunomodulators from nasopharyngeal carcinoma cells upregulate interleukin-10 production from monocytes. J. Virol. 2011, 85, 7333–7342. [Google Scholar] [CrossRef] [PubMed]
- Incrocci, R.; Barse, L.; Stone, A.; Vagvala, S.; Montesano, M.; Subramaniam, V.; Swanson-Mungerson, M. Epstein-barr virus latent membrane protein 2A (LMP2A) enhances IL-10 production through the activation of bruton’s tyrosine kinase and STAT3. Virology 2016, 500, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.P.; Chang, Y.T.; Wu, C.C.; Liu, Y.L.; Chen, M.C.; Tsang, N.M.; Hsu, C.L.; Chang, Y.S.; Yu, J.S. Multiplexed immunobead-based profiling of cytokine markers for detection of nasopharyngeal carcinoma and prognosis of patient survival. Head Neck 2011, 33, 886–897. [Google Scholar] [CrossRef] [PubMed]
- Teruya-Feldstein, J.; Jaffe, E.S.; Burd, P.R.; Kingma, D.W.; Setsuda, J.E.; Tosato, G. Differential chemokine expression in tissues involved by hodgkin’s disease: Direct correlation of eotaxin expression and tissue eosinophilia. Blood 1999, 93, 2463–2470. [Google Scholar] [PubMed]
- Rahal, E.A.; Hajjar, H.; Rajeh, M.; Yamout, B.; Abdelnoor, A.M. Epstein-barr virus and human herpes virus 6 type a DNA enhance IL-17 production in mice. Viral Immunol. 2015, 28, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.L.; Morgan, D.R.; Dominguez, R.L.; Thorne, L.B.; Elmore, S.H.; Mino-Kenudson, M.; Lauwers, G.Y.; Booker, J.K.; Gulley, M.L. High levels of Epstein-Barr virus DNA in latently infected gastric adenocarcinoma. Lab. Investig. 2009, 89, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Assarsson, E.; Lundberg, M.; Holmquist, G.; Bjorkesten, J.; Thorsen, S.B.; Ekman, D.; Eriksson, A.; Rennel Dickens, E.; Ohlsson, S.; Edfeldt, G.; et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS ONE 2014, 9, e95192. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
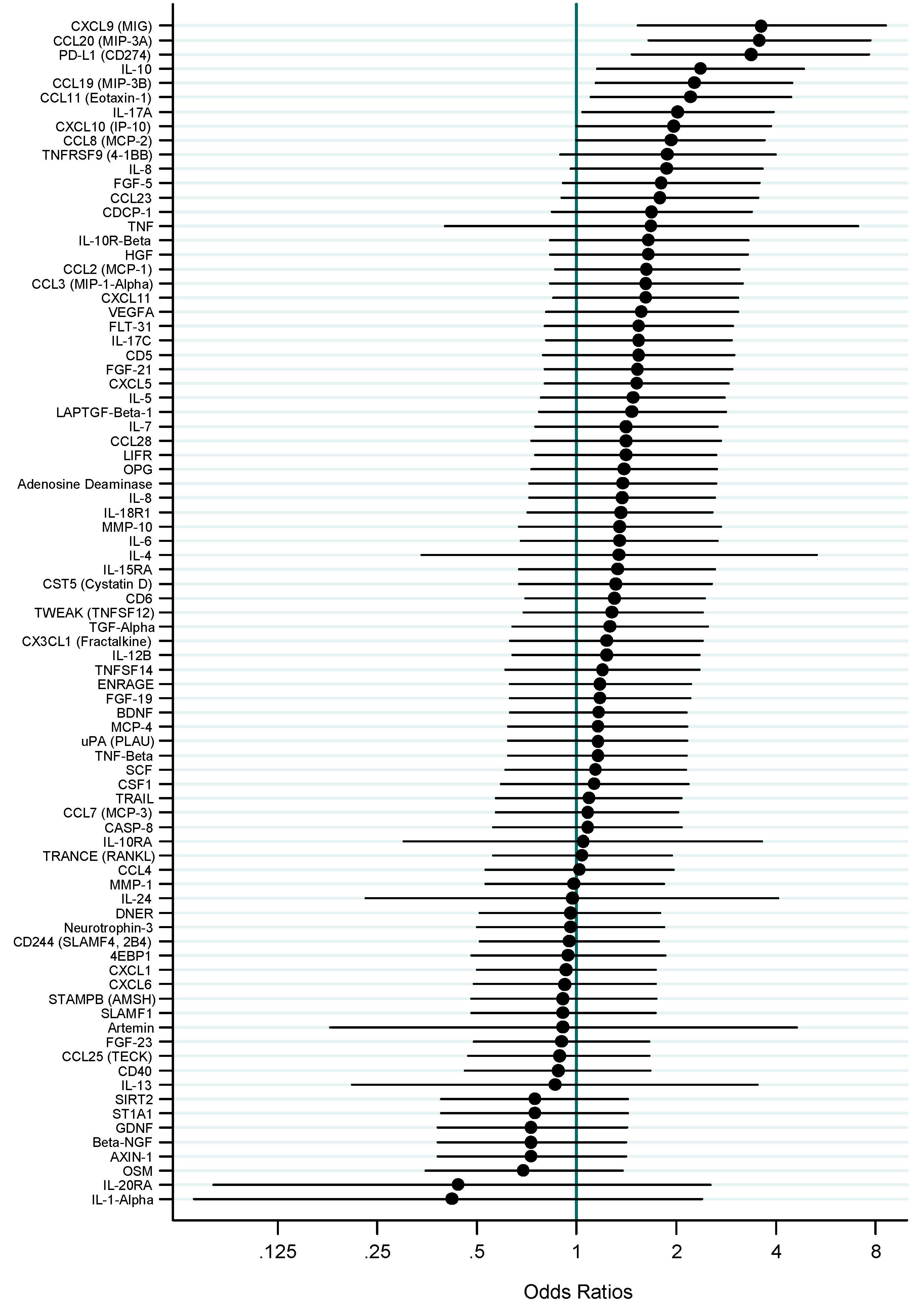
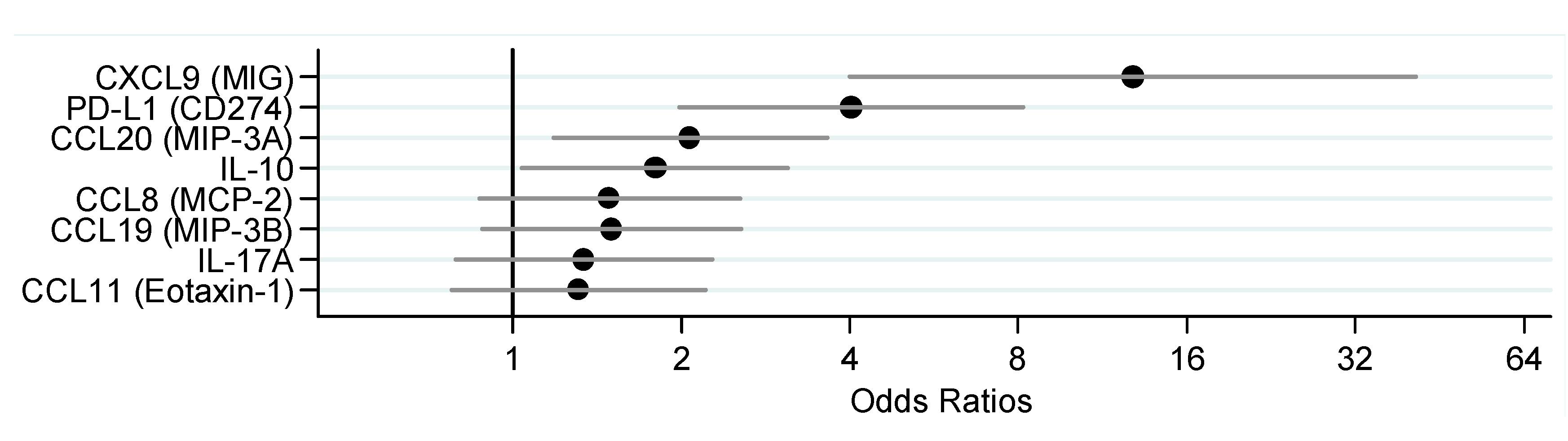
| Protein (Other Names) | Marker Level Tertile | Age- and Sex-Adjusted OR (95% CI) |
|---|---|---|
| CCL20 (MIP-3A) | 1 | 1.0 |
| 2 | 2.33 (0.57–9.49) | |
| 3 | 12.30 (2.68–56.36) | |
| p-trend | 0.001 | |
| AUC | 0.76 | |
| CXCL9 (MIG, EBV-induced molecule 1 ligand chemokine) | 1 | 1.0 |
| 2 | 2.17 (0.44–10.81) | |
| 3 | 11.49 (2.08–63.55) | |
| p-trend | 0.003 | |
| AUC | 0.74 | |
| PD-L1 (CD274) | 1 | 1.0 |
| 2 | 5.80 (0.96–35.18) | |
| 3 | 13.73 (2.21–85.07) | |
| p-trend | 0.004 | |
| AUC | 0.73 | |
| IL-10 | 1 | 1.0 |
| 2 | 2.91 (0.73–11.61) | |
| 3 | 5.72 (1.33–24.65) | |
| p-trend | 0.019 | |
| AUC | 0.67 | |
| CCL19 (MIP-3B) | 1 | 1.0 |
| 2 | 1.12 (0.30–4.20) | |
| 3 | 5.03 (1.30–19.49) | |
| p-trend | 0.019 | |
| AUC | 0.67 | |
| CCL11 (Eotaxin-1) | 1 | 1.0 |
| 2 | 1.57 (0.41–6.09) | |
| 3 | 4.74 (1.18–19.02) | |
| p-trend | 0.026 | |
| AUC | 0.70 | |
| IL-17A | 1 | 1.0 |
| 2 | 4.29 (1.11–16.64) | |
| 3 | 4.28 (1.09–16.80) | |
| p-trend | 0.038 | |
| AUC | 0.67 | |
| CCL8 (MCP-2) | 1 | 1.0 |
| 2 | 2.10 (0.56–7.88) | |
| 3 | 3.72 (1.01–13.75) | |
| p-trend | 0.049 | |
| AUC | 0.67 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camargo, M.C.; Sivins, A.; Isajevs, S.; Folkmanis, V.; Rudzīte, D.; Gulley, M.L.; Offerhaus, G.J.; Leja, M.; Rabkin, C.S. Associations of Epstein-Barr Virus-Positive Gastric Adenocarcinoma with Circulating Mediators of Inflammation and Immune Response. Cancers 2018, 10, 284. https://doi.org/10.3390/cancers10090284
Camargo MC, Sivins A, Isajevs S, Folkmanis V, Rudzīte D, Gulley ML, Offerhaus GJ, Leja M, Rabkin CS. Associations of Epstein-Barr Virus-Positive Gastric Adenocarcinoma with Circulating Mediators of Inflammation and Immune Response. Cancers. 2018; 10(9):284. https://doi.org/10.3390/cancers10090284
Chicago/Turabian StyleCamargo, M. Constanza, Armands Sivins, Sergejs Isajevs, Valdis Folkmanis, Dace Rudzīte, Margaret L. Gulley, G. Johan Offerhaus, Marcis Leja, and Charles S. Rabkin. 2018. "Associations of Epstein-Barr Virus-Positive Gastric Adenocarcinoma with Circulating Mediators of Inflammation and Immune Response" Cancers 10, no. 9: 284. https://doi.org/10.3390/cancers10090284