Inadequate Vitamin C Status in Prediabetes and Type 2 Diabetes Mellitus: Associations with Glycaemic Control, Obesity, and Smoking


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Design
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Demographic Information
2.4. Anthropometric Measures
2.5. Blood Parameters
2.5.1. Plasma Vitamin C
2.5.2. Plasma Ghrelin, Leptin, and Adiponectin
2.5.3. Plasma Insulin
2.6. Dietary Intake of Vitamin C, Macronutrients, and Fibre
2.7. Physical Activity
2.8. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Metabolic and Inflammatory Plasma Biomarkers
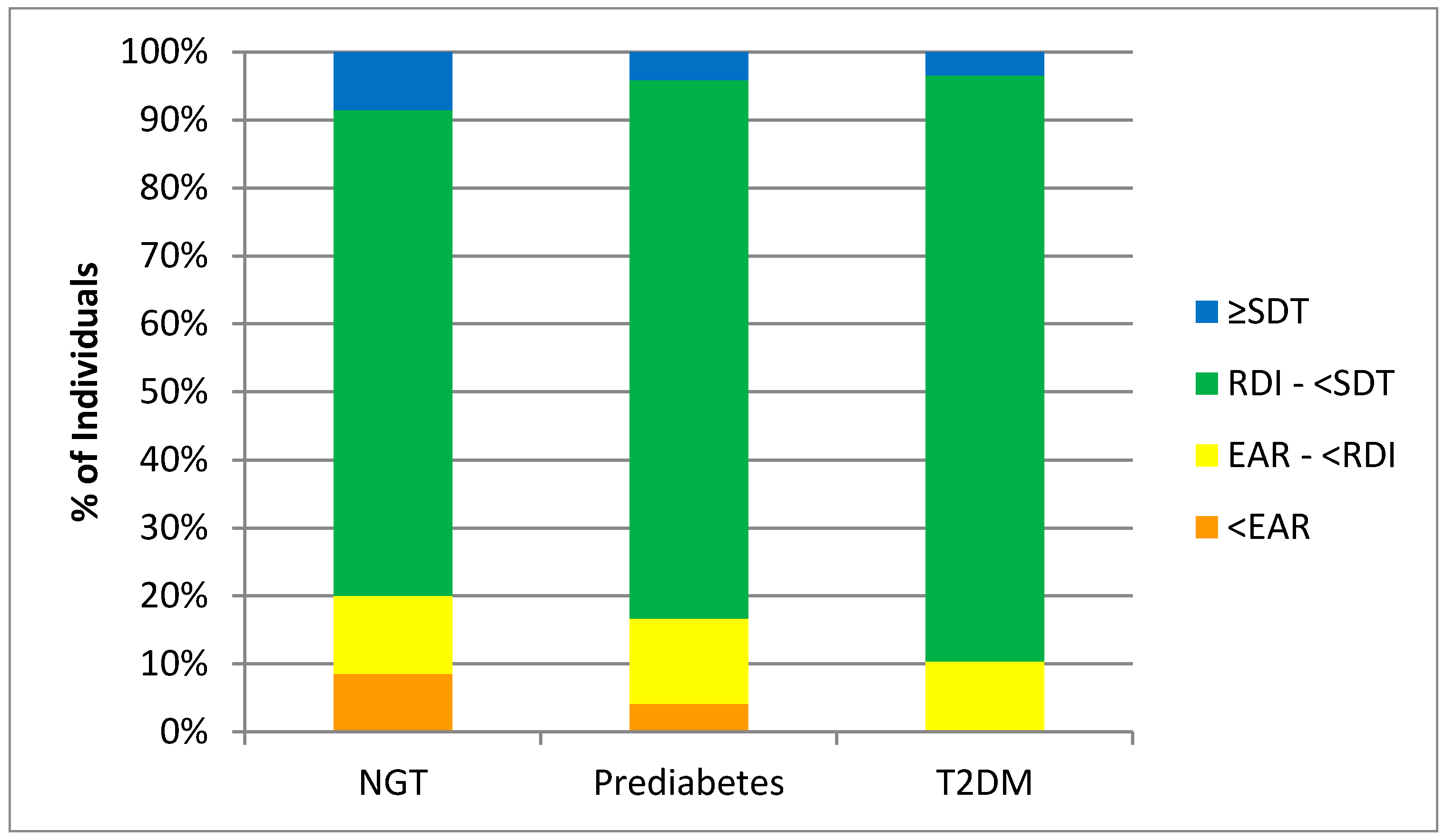
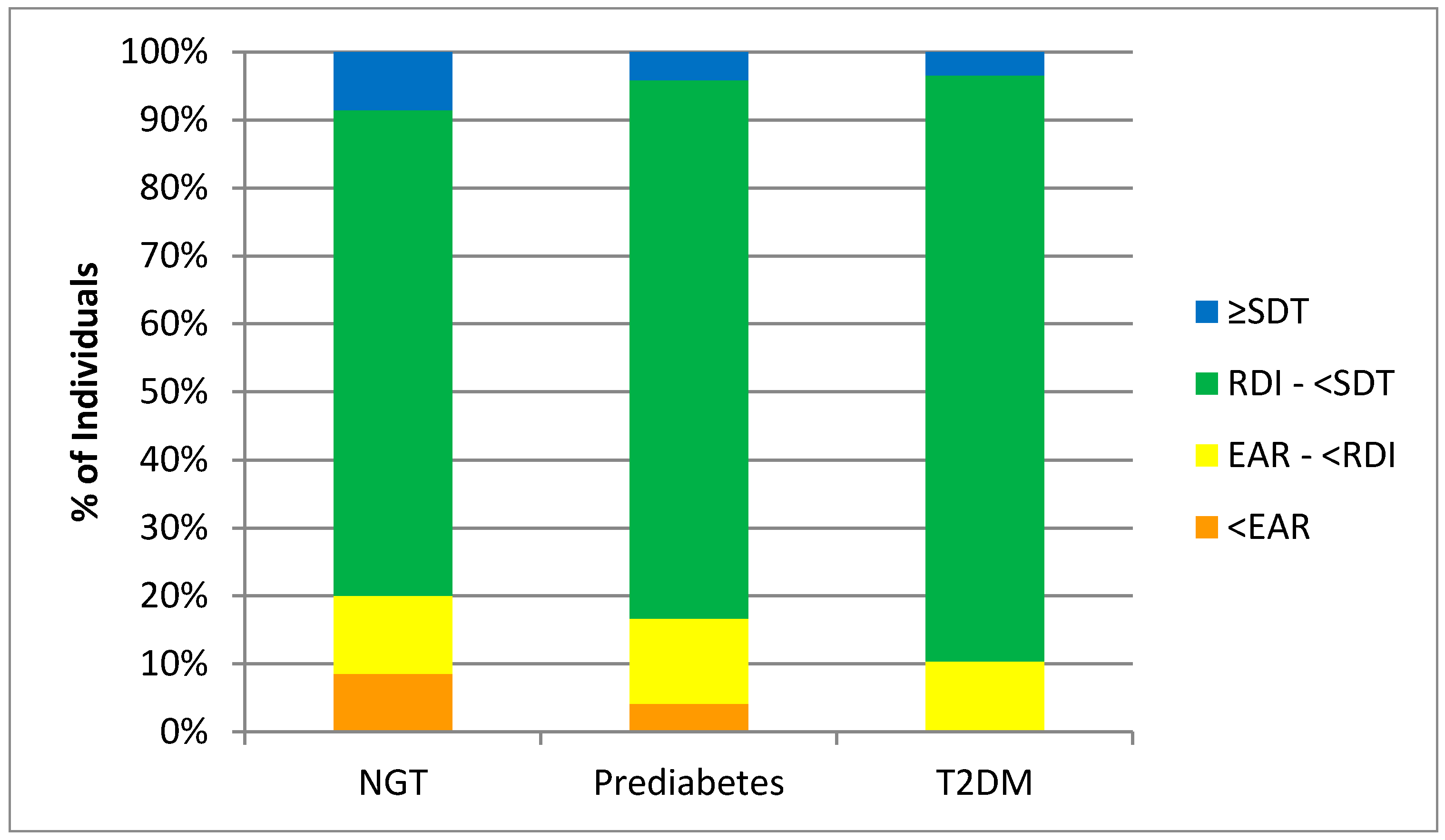
3.3. Dietary Intake of Vitamin C, Macronutrients, and Fibre
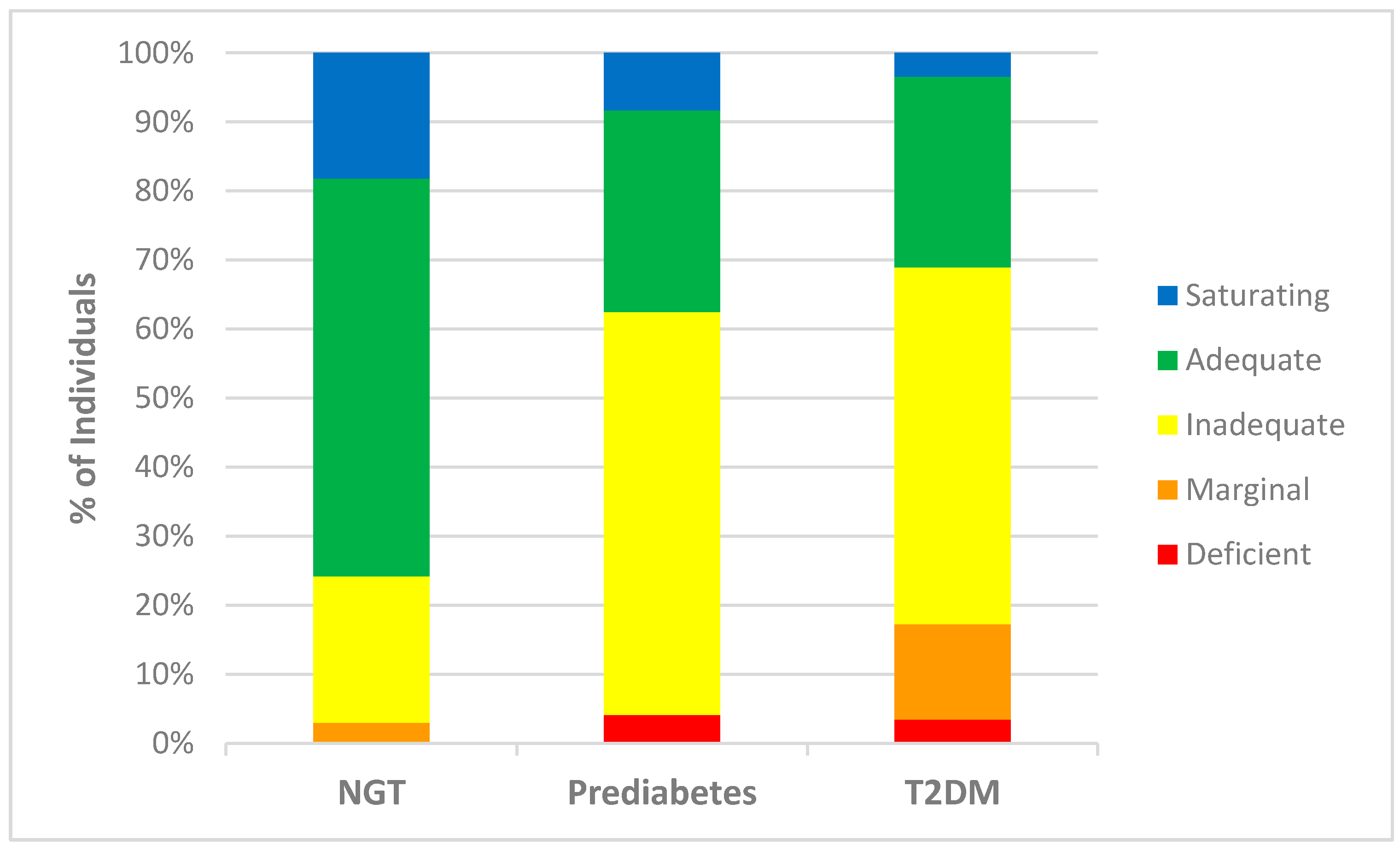
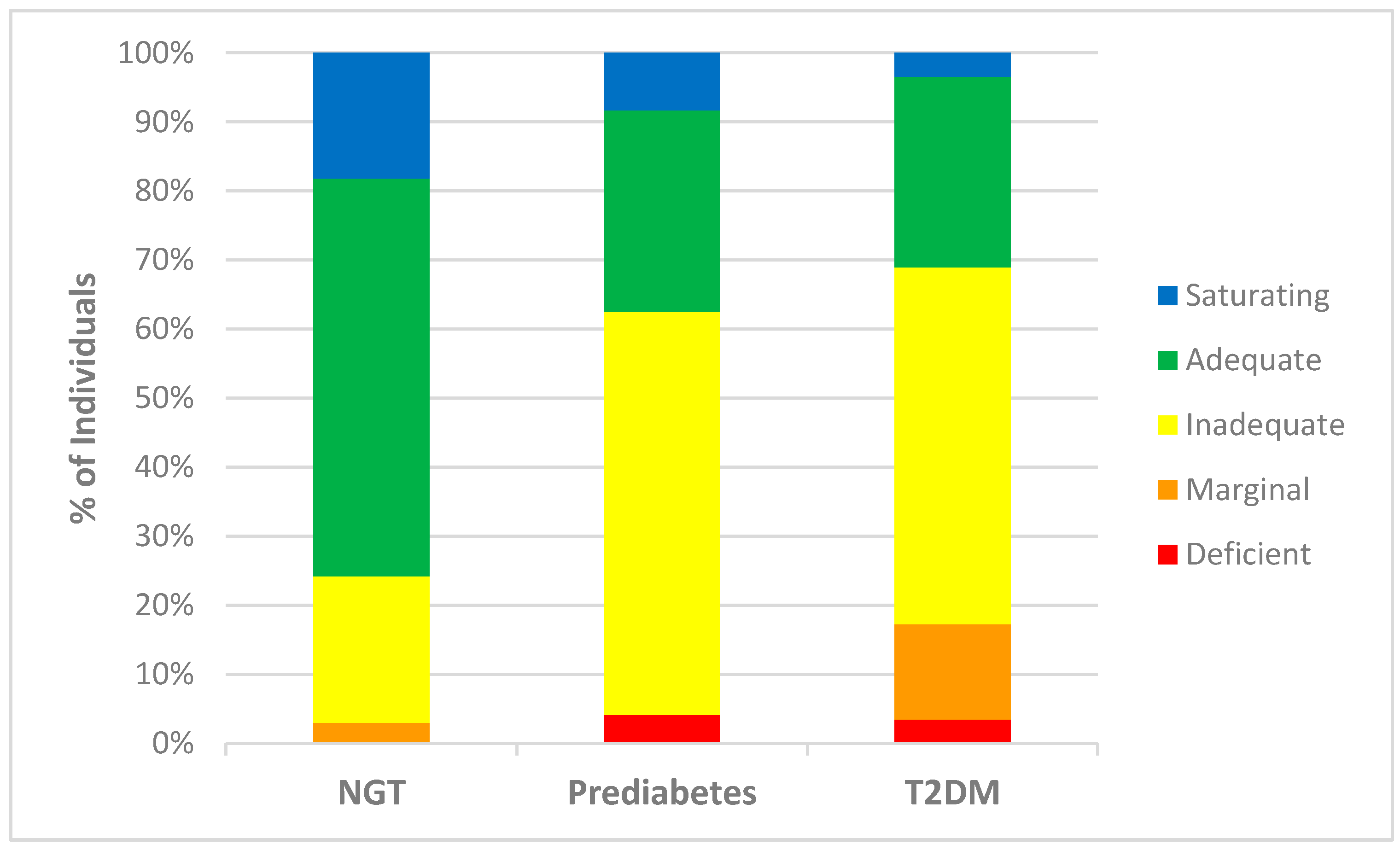
3.4. Plasma Vitamin C Status and Dietary Vitamin C Intakes
3.5. Plasma Vitamin C Correlations
4. Discussion
4.1. Predictors of Plasma Vitamin C
4.2. Metabolic Hormones
4.3. Clinical Significance
4.4. Study Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014, 37, S81–S90. [Google Scholar]
- International Diabetes Federation. IDF diabetes atlas 2015. Available online: http://www.diabetesatlas.org. (accessed on 5 June 2017).
- Ministry of Health. Virtual diabetes register 2017. Available online: http://www.health.govt.nz/our-work/diseases-and-conditions/diabetes/about-diabetes/virtual-diabetes-register-vdr. (accessed on 11 June 2017).
- Primary Care Domain NHS Digital. Quality and outcomes framework-prevalence, achievements and exceptions report 2016. Available online: http://www.content.digital.nhs.uk/catalogue/PUB22266 (accessed on 25 June 2017).
- McArdle, M.; Finucane, O.; Connaughton, R.; McMorrow, A.; Roche, H. Mechanisms of obesity-induced inflammation and insulin resistance: insights into the emerging role of nutritional strategies. Front. Endocrinol. (Lausanne). 2013, 4, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Frei, B. Toward a new recommended dietary allowance for vitamin C based on antioxidant and health effects in humans. Am. J. Clin. Nutr. 1999, 69, 1086–1107. [Google Scholar] [PubMed]
- Carr, A.; Frei, B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J. 1999, 13, 1007–1024. [Google Scholar] [PubMed]
- Will, J.C.; Byers, T. Does diabetes mellitus increase the requirement for vitamin C? Nutr. Rev. 1996, 54, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Sargeant, L.; Wareham, N.; Bingham, S.; Day, N. Vitamin C and hyperglycemia in the European prospective investigation into cancer-Norfolk (EPIC-Norfolk) study: A population-based study. Diabetes Care. 2000, 23, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Kositsawat, J.; Freeman, V.L. Vitamin C and A1c relationship in the National Health and Nutrition Examination Survey (NHANES) 2003–2006. J. Am. Coll. Nutr. 2011, 30, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.; Li, H.; Wang, Y.; Niyyati, M.; Wang, Y.; Leshin, J.; Levine, M. Low red blood cell vitamin C concentrations induce red blood cell fragility: A link to diabetes via glucose, glucose transporters, and dehydroascorbic Acid. EBioMedicine 2015, 2, 1735–1750. [Google Scholar] [CrossRef] [PubMed]
- Olofsson, C.; Discacciati, A.; Akesson, A.; Orsini, N.; Brismar, K.; Wolk, A. Changes in fruit, vegetable and juice consumption after the diagnosis of type 2 diabetes: A prospective study in men. Br. J. Nutr. 2017, 117, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Feskens, E.J.M.; Virtanen, S.M.; Räsänen, L.; Tuomilehto, J.; Stengård, J.; Pekkanen, J.; Nissinen, A.; Kromhout, D. Dietary factors determining diabetes and impaired glucose tolerance: A 20-year follow-up of the Finnish and Dutch cohorts of the Seven Countries Study. Diabetes Care. 1995, 18, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Harding, A.H.; Wareham, N.J.; Bingham, S.A.; Khaw, K.; Luben, R.; Welch, A.; Forouhi, N.G. Plasma vitamin C level, fruit and vegetable consumption, and the risk of new-onset type 2 diabetes mellitus: The European prospective investigation of cancer-Norfolk prospective study. Arch. Intern. Med. 2008, 168, 1493. [Google Scholar] [CrossRef] [PubMed]
- Som, S.; Basu, S.; Mukherjee, D.; Deb, S.; Choudhury, P.R.; Mukherjee, S.; Chatterjee, S.N.; Chatterjee, I.B. Ascorbic acid metabolism in diabetes mellitus. Metabolism 1981, 30, 572–577. [Google Scholar] [CrossRef]
- Will, J.; Ford, E.; Bowman, B. Serum vitamin C concentrations and diabetes: Findings from the third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Clin. Nutr. 1999, 70, 49–52. [Google Scholar] [PubMed]
- World Health Organization. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. 2000. Available online: http://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/ (accessed on 10 June 2017).
- World Health Organization. Section 5: Collecting step 2 data: Physical measurements 2017. Available online: http://www.who.int/chp/steps/Part3_Section5.pdf?ua=1 (accessed on 19 June 2017).
- Carr, A.C.; Pullar, J.M.; Moran, S.; Vissers, M.C. Bioavailability of vitamin C from kiwifruit in non-smoking males: Determination of ‘healthy’ and ‘optimal’ intakes. J. Nutr. Sci. 2012, 1, e14. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Uchiki, T.; Iwama, M.; Kishimoto, Y.; Takahashi, R.; Ishigami, A. Determination of dehydroascorbic acid in mouse tissues and plasma by using tris(2-carboxyethyl)phosphine hydrochloride as reductant in metaphosphoric acid/ethylenediaminetetraacetic acid solution. Biol. Pharm Bull. 2010, 33, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Bang, A.S.; Soule, S.G.; Yandle, T.G.; Richards, A.M.; Pemberton, C.J. Characterisation of proghrelin peptides in mammalian tissue and plasma. J. Endocrinol. 2007, 192, 313–323. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Nutrient reference values for Australia and New Zealand including recommended dietary intakes Canberra: ACT: National Health and Medical Research Council. 2006. Available online: https://www.nhmrc.gov.au/_files_nhmrc/file/publications/17122_nhmrc_nrv_update-dietary_intakes-web.pdf (accessed on 12 June 2017).
- New Zealand Society for the Study of Diabetes. NZSSD position statement on the diagnosis of, and screening for, type 2 diabetes 2011. Available online: http://www.nzssd.org.nz/HbA1c/1.%20NZSSD%20position%20statement%20on%20screening%20for%20type%202%20diabetes%20final%20Sept%202011.pdf (accessed on 20 June 2017).
- Lykkesfeldt, J.; Poulsen, H.E. Is vitamin C supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2010, 103, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Girgis, C.; Christie-David, D.; Gunton, J. Effects of vitamins C and D in type 2 diabetes mellitus. Nutr Diet Suppl. 2015, 7, 21–28. [Google Scholar] [CrossRef]
- Johnston, C.S.; Beezhold, B.L.; Mostow, B.; Swan, P.D. Plasma vitamin C is inversely related to body mass index and waist circumference but not to plasma adiponectin in nonsmoking adults. J. Nutr. 2007, 137, 1757–1762. [Google Scholar] [PubMed]
- Block, G.; Mangels, A.R.; Patterson, B.H.; Levander, O.A.; Norkus, E.P.; Taylor, P.R. Body weight and prior depletion affect plasma ascorbate levels attained on identical Vitamin C intake: A controlled-diet study. J. Am. Coll. Nutr. 1999, 18, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Pullar, J.M.; Bozonet, S.M.; Vissers, M.C. Marginal ascorbate status (hypovitaminosis C) results in an attenuated response to vitamin C supplementation. Nutrients 2016, 8, 341. [Google Scholar] [CrossRef] [PubMed]
- Lamb, R.E.; Goldstein, B.J. Modulating an oxidative-inflammatory cascade: Potential new treatment strategy for improving glucose metabolism, insulin resistance, and vascular function. Int. J. Clin. Pract. 2008, 62, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Calle, M.C.; Fernandez, M.L. Inflammation and type 2 diabetes. Diabetes Metab. 2012, 38, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Bailo, B.; El-Sohemy, A.; Haddad, P.S.; Arora, P.; Benzaied, F.; Karmali, M.; Badawi, A. Vitamins D, C, and E in the prevention of type 2 diabetes mellitus: Modulation of inflammation and oxidative stress. Biologics 2011, 5, 7–19. [Google Scholar] [PubMed]
- Schectman, G.; Byrd, J.; Gruchow, H. The influence of smoking on vitamin C status in adults. Am. J. Public Health. 1989, 79, 158. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.M.; Sternberg, M.R.; Schleicher, R.L.; Rybak, M.E. Dietary supplement use and smoking are important correlates of biomarkers of water-soluble vitamin status after adjusting for sociodemographic and lifestyle variables in a representative sample of U.S. adults. J. Nutr. 2013, 143, 957S–965S. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J.; Michels, A.J.; Frei, B. Vitamin C. Adv. Nutr. 2014, 5, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Klok, M.D.; Jakobsdottir, S.; Drent, M.L. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Werner, A.D.; Lara, J.; Willis, N.D.; Mathers, J.C.; Siervo, M. Effects of vitamin C supplementation on glycaemic control: a systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Gillani, S.W.; Sulaiman, S.A.S.; Abdul, M.I.M.; Baig, M.R. Combined effect of metformin with ascorbic acid versus acetyl salicylic acid on diabetes-related cardiovascular complication a 12-month single blind multicenter randomized control trial. Cardiovasc. Diabetol. 2017, 16, 103. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine, Panel on Dietary Antioxidants Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids: A Report of the Panel on Dietary Antioxidants and Related Compounds, Subcommittees on Upper Reference Levels of Nutrients and of Interpretation and Use of Dietary Reference Intakes, and the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- Zebrowski, E.J.; Bhatnagar, P.K. Urinary excretion pattern of ascorbic acid in streptozotocin diabetic and insulin treated rats. Pharmacol. Res. Commun. 1979, 11, 95–103. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | NGT | Prediabetes | T2DM | Total |
|---|---|---|---|---|
| Age * (years) | 55 ± 13 a | 63 ± 9 b | 61 ± 11 b | 59 ± 11 |
| Sex * | ||||
| Female % (n) | 74 (26) a | 52 (13) ab | 35 (10) b | 55% (49) |
| Male % (n) | 26 (9) | 48 (12) | 66 (19) | 45% (40) |
| Ethnicity | ||||
| European % (n) | 86 (30) | 88 (22) | 97 (28) | 90% (80) |
| Maori % (n) | 9 (3) | 4 (1) | 3 (1) | 6% (5) |
| Pacific Island % (n) | 0 (0) | 4 (1) | 0 (0) | 1% (1) |
| Asian % (n) | 3 (1) | 4 (1) | 0 (0) | 2% (2) |
| Other % (n) | 3 (1) | 0 (0) | 0 (0) | 1% (1) |
| Qualification | ||||
| No Qualification % (n) | 96 (3) | 20 (5) | 25 (7) | 17% (15) |
| Secondary School % (n) | 20 (7) | 24 (6) | 32 (9) | 25% (22) |
| Post-Secondary Certificate, Diploma or Trade Diploma % (n) | 43 (15) | 20 (5) | 25 (7) | 31% (27) |
| University % (n) | 27 (10) | 36 (9) | 18 (5) | 27% (24) |
| Physical Activity (MET min/week) | 1723 ± 1687 | 2496 ± 3671 | 1320 ± 1490 | 1772 ± 2327 |
| Anthropometry | ||||
| Weight * (kg) | 76 ± 18 a | 89 ± 19 b | 96 ± 20 b | 86 ± 21 |
| BMI * (kg/m2) | 28 ± 6 a | 30 ± 7 ab | 33 ± 6 b | 30 ± 7 |
| Fat Mass (%) | 32 ± 8 | 33 ± 8 | 35 ± 7 | 33 ± 8 |
| Waist Circumference * (cm) | 89 ± 16 a | 99 ± 14 b | 110 ± 15 c | 99 ± 17 |
| Waist-to-Hip Ratio * | 0.9 ± 0.1 a | 0.9 ± 0.1 b | 1.0 ± 0.1 b | 0.9 ± 0.1 |
| Blood Pressure Diastolic (mmHg) | 78 ± 9 | 83 ± 8 | 79 ± 9 | 80 ± 9 |
| Blood Pressure Systolic * (mmHg) | 125 ± 14 a | 132 ± 14 ab | 135 ± 15 b | 130 ± 15 |
| Smoking Status | ||||
| Current Smoker % (n) | 7 (2) | 5 (1) | 3 (1) | 5% (4) |
| Ex-smoker % (n) | 28 (8) | 439 (9) | 38 (11) | 35% (28) |
| Non-smoker % (n) | 66 (19) | 52 (11) | 59 (17) | 60% (47) |
| Laboratory Measures | NGT | Prediabetes | T2DM | Total |
|---|---|---|---|---|
| Fasting Glucose * (mmol/L) | 5.0 ± 0.4 a | 6.2 ± 0.4 b | 7.2 ± 1.3 c | 6.0 ± 1.2 |
| HbA1c * (mmol/mol) | 35 ± 4 a | 40 ± 5 b | 47 ± 9 c | 41 ± 8 |
| hs-CRP (mg/L) Mean (95% CI) | 1.2 (0.9–1.6) | 1.6 (1.0–2.3) | 2.1 (1.4–2.8) | 1.6 (1.31.9) |
| Total Cholesterol * (mmol/L) | 5.3 ± 0.9 a | 5.9 ± 1.2 a | 4.3 ± 1.1 b | 5.0 ± 1.1 |
| Cholesterol HDL * (mmol/L) | 1.5 ± 0.4 a | 1.3 ± 0.3 b | 1.1 ± 0.2 b | 1.3 ± 0.3 |
| Cholesterol LDL * (Calc) (mmol/L) | 3.4 ± 0.8 a | 3.3 ± 1.0 a | 2.5 ± 1.0 b | 3.1 ± 1.0 |
| Triglycerides * (mmol/L) | 1.1 ± 0.4 a | 1.3 ± 0.7 ab | 1.4 ± 0.6 b | 1.3 ± 0.6 |
| Cholesterol (total/HDL) (ratio) | 3.8 ± 0.8 | 4.2 ± 0.8 | 3.9 ± 1.1 | 4.0 ± 0.9 |
| Fasting Insulin * (pmol/L) | 53 ± 37 a | 89 ± 53 b | 95 ± 48 b | 77 ± 49 |
| Ghrelin * (pmol/L) Mean (95% CI) | 171 (142–207) a | 111 (88–140) b | 112 (91–139) b | 132 (117–150) |
| Leptin (ng/mL) Mean (95% CI) | 27 (20–38) | 33 (20–54) | 33 (23–47) | 31 (25–38) |
| Adiponectin * (µg/mL) Mean (95% CI) | 11 (9–13) a | 9 (7–11) a | 7 (6–8) b | 9 (8–10) |
| Plasma vitamin C * (µmol/L) | 57 ± 14 a | 48 ± 16 b | 41 ± 18 b | 49 ± 17 |
| Total Daily Dietary intake | NGT | Prediabetes | T2DM | Total |
|---|---|---|---|---|
| Energy (KJ) | 8192 ± 2336 | 8430 ± 2260 | 8033 ± 2416 | 8204 ± 2321 |
| Fibre (g) | 24 ± 9 | 25 ± 8 | 27 ± 9 | 25 ± 9 |
| Protein (% of Energy) | 17 ± 3 | 18 ± 4 | 17 ± 3 | 17 ± 3 |
| Fat (% of Energy) | 37 ± 6 | 39 ± 8 | 36 ± 7 | 37 ± 7 |
| Carbohydrate (% of Energy) | 44 ± 6 | 40 ± 8 | 44 ± 8 | 43 ± 7 |
| Dietary Vitamin C Intake (mg) | 103 ± 76 | 94 ± 58 | 101 ± 61 | 100 ± 66 |
| Measure | Pearson Correlation |
|---|---|
| Fasting Glucose (mmol/L) | −0.411 *** |
| HbA1c (mmol/mol) | −0.334 *** |
| Total Cholesterol (mmol/L) | 0.093 |
| Triglycerides (mmol/L) | −0.322 ** |
| Cholesterol (HDL) | 0.295 ** |
| Cholesterol (total/HDL) | −0.214 * |
| Cholesterol (LDL) calculated | 0.086 |
| Insulin (pmol/L) | −0.353 ** |
| hs-CRP (mg/L) | −0.333 ** |
| Ghrelin (pmol/L) | 0.295 ** |
| Leptin (ng/mL) | −0.183 |
| Adiponectin (ng/mL) | 0.202 |
| BMI (kg/m2) | −0.446 *** |
| Waist-to-Hip Ratio | −0.274 * |
| Fat Mass (%) | −0.295 ** |
| Measure | B | Lower 95% CI | Upper 95% CI | p Value |
|---|---|---|---|---|
| BMI | −0.9 | −1.4 | −0.4 | 0.001 |
| Current Smoker | −21.9 | −35.8 | −7.9 | 0.003 |
| Ex-Smoker | −4.9 | −11.2 | 1.5 | 0.128 |
| Fasting Glucose | −4.4 | −7.1 | −1.8 | 0.001 |
| Dietary vitamin C | 0.05 | 0.01 | 0.10 | 0.032 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, R.; Willis, J.; Gearry, R.; Skidmore, P.; Fleming, E.; Frampton, C.; Carr, A. Inadequate Vitamin C Status in Prediabetes and Type 2 Diabetes Mellitus: Associations with Glycaemic Control, Obesity, and Smoking. Nutrients 2017, 9, 997. https://doi.org/10.3390/nu9090997
Wilson R, Willis J, Gearry R, Skidmore P, Fleming E, Frampton C, Carr A. Inadequate Vitamin C Status in Prediabetes and Type 2 Diabetes Mellitus: Associations with Glycaemic Control, Obesity, and Smoking. Nutrients. 2017; 9(9):997. https://doi.org/10.3390/nu9090997
Chicago/Turabian StyleWilson, Renée, Jinny Willis, Richard Gearry, Paula Skidmore, Elizabeth Fleming, Chris Frampton, and Anitra Carr. 2017. "Inadequate Vitamin C Status in Prediabetes and Type 2 Diabetes Mellitus: Associations with Glycaemic Control, Obesity, and Smoking" Nutrients 9, no. 9: 997. https://doi.org/10.3390/nu9090997