Lifestyle Patterns and Weight Status in Spanish Adults: The ANIBES Study

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurements
2.1.1. Lifestyle Factors
Diet
Physical Activity
Sleep Duration
Smoking
2.1.2. Body Measurements
2.1.3. Covariates
Education
Geographical Area
2.2. Data Cleaning
2.3. Data Analysis
2.3.1. Dietary Patterns
2.3.2. Lifestyle Patterns
3. Results
3.1. Sample Characteristics
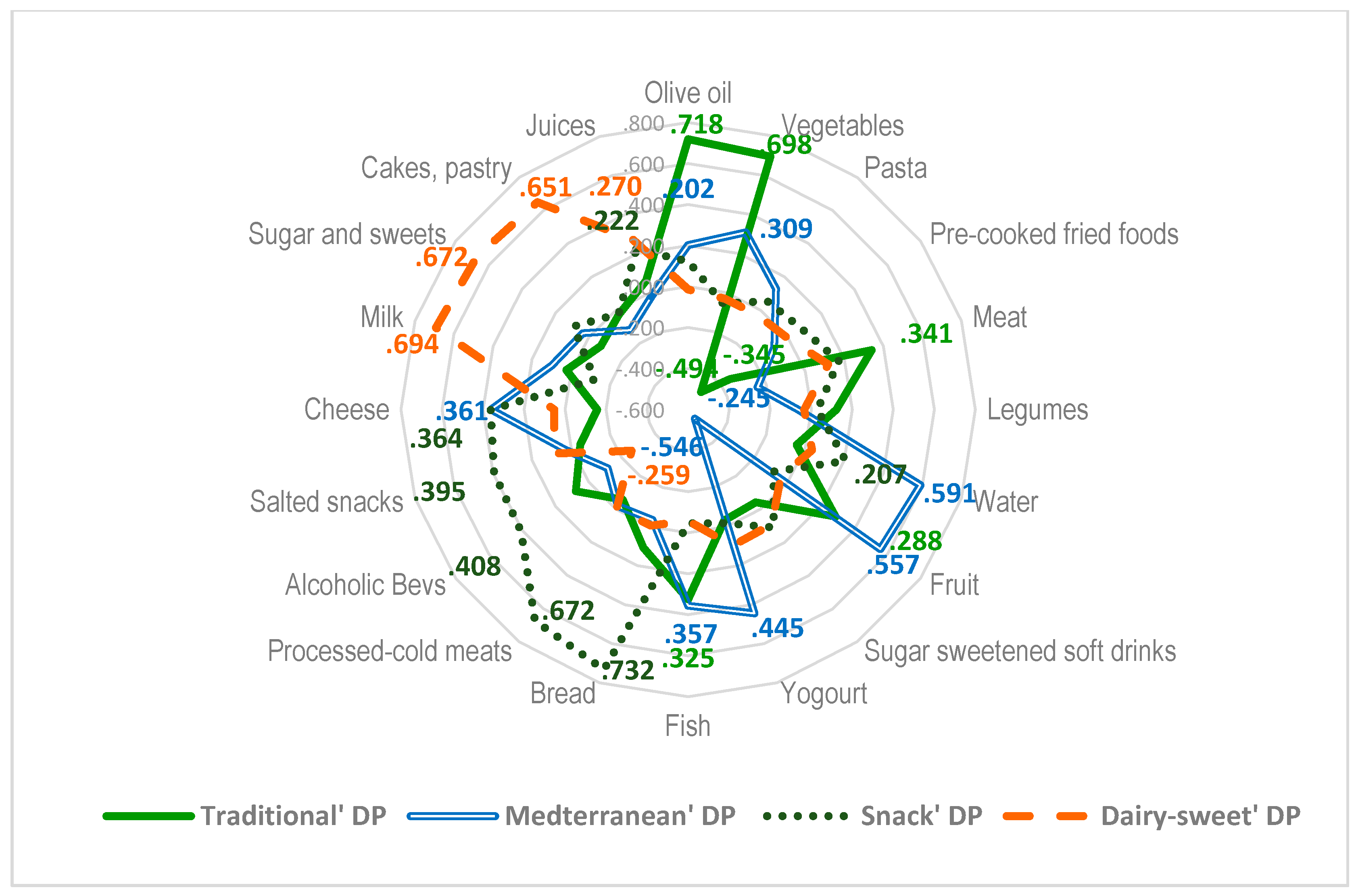
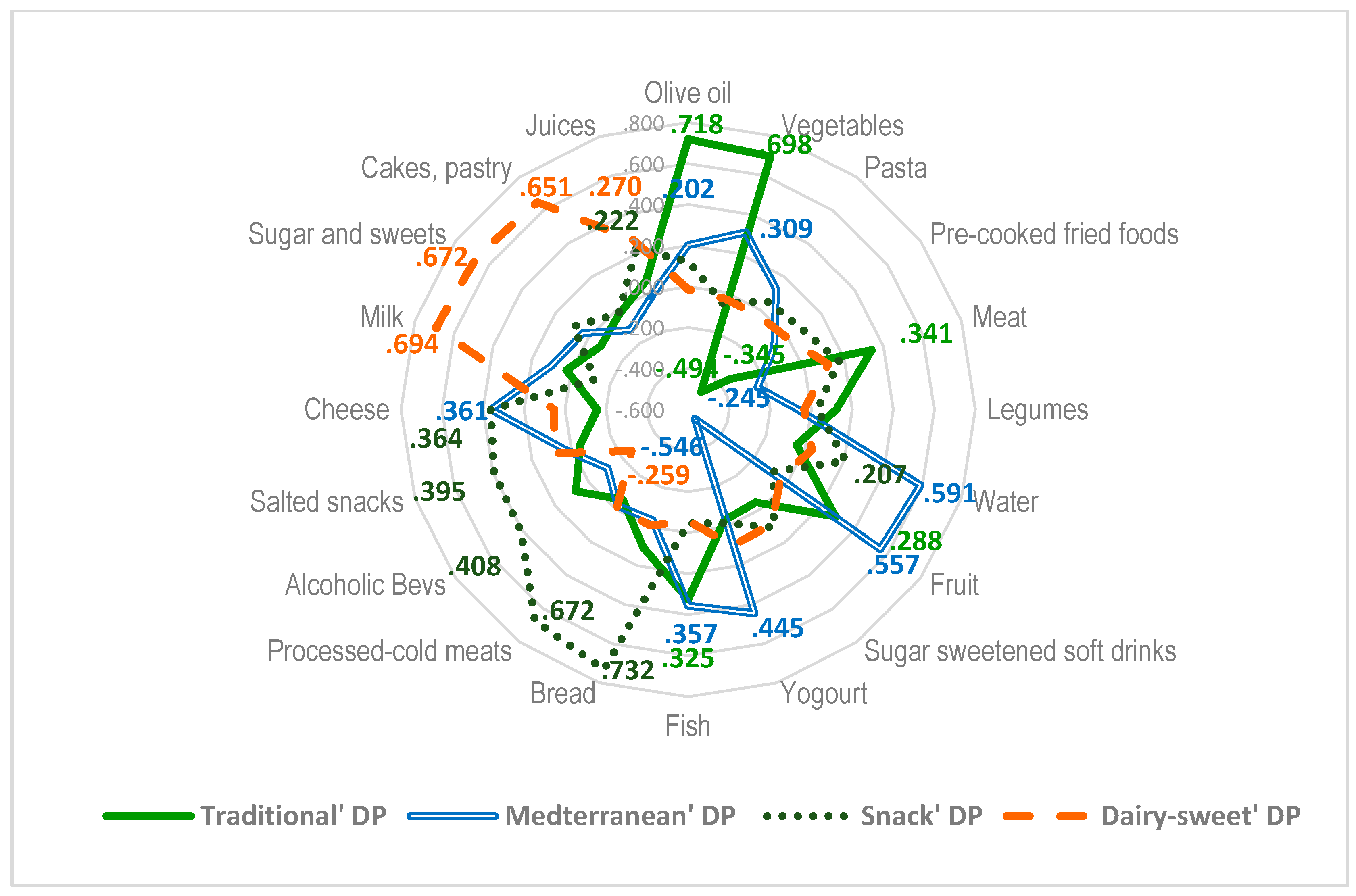
3.2. Dietary Patterns
3.3. Lifestyle Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Margetts, B. Feedback on WHO/FAO global report on diet, nutrition and prevention of chronic diseases (NCD). Public Health Nutr. 2003, 6, 423–424. [Google Scholar] [CrossRef] [PubMed]
- Jessri, M.; Wolfinger, R.D.; Lou, W.Y.; L’Abbé, M.R. Identification of dietary patterns associated with obesity in a nationally representative survey of Canadian adults: Application of a priori, hybrid, and simplified dietary pattern techniques. Am. J. Clin. Nutr. 2017, 105, 669–684. [Google Scholar] [CrossRef] [PubMed]
- López-Sobaler, A.M.; Aparicio, A.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. Overweight and General and Abdominal Obesity in a Representative Sample of Spanish Adults: Findings from the ANIBES Study. Biomed Res. Int. 2016, 2016, 8341487. [Google Scholar] [CrossRef] [PubMed]
- Basterra-Gortari, F.J.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Gea, A.; Martinez-Gonzalez, M.A. Prevalencia de obesidad y diabetes en adultos españoles, 1987–2012. Med. Clin. 2017, 148, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Eguaras, S.; Toledo, E.; Hernández-Hernández, A.; Cervantes, S.; Martínez-González, M.A. Better Adherence to the Mediterranean Diet Could Mitigate the Adverse Consequences of Obesity on Cardiovascular Disease: The SUN Prospective Cohort. Nutrients 2015, 7, 9154–9162. [Google Scholar] [CrossRef] [PubMed]
- Lacoppidan, S.A.; Kyrø, C.; Loft, S.; Helnæs, A.; Christensen, J.; Hansen, C.P.; Dahm, C.C.; Overvad, K.; Tjønneland, A.; Olsen, A. Adherence to a Healthy Nordic Food Index Is Associated with a Lower Risk of Type-2 Diabetes—The Danish Diet, Cancer and Health Cohort Study. Nutrients 2015, 7, 8633–8644. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioral, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar]
- San-Cristobal, R.; Navas-Carretero, S.; Celis-Morales, C.; Brennan, L.; Walsh, M.; Lovegrove, J.A.; Daniel, H.; Saris, W.H.M.; Traczyk, I.; Manios, Y.; et al. Analysis of Dietary Pattern Impact on Weight Status for Personalised Nutrition through On-Line Advice: The Food4Me Spanish Cohort. Nutrients 2015, 7, 9523–9537. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.C.; Tey, S.L.; Gray, A.R.; Chisholm, A.; Smith, C.; Fleming, E.; Parnell, W. Association of Nut Consumption with Cardiometabolic Risk Factors in the 2008/2009 New Zealand Adult Nutrition Survey. Nutrients 2015, 7, 7523–7542. [Google Scholar] [CrossRef] [PubMed]
- Kremers, S.P. Theory and practice in the study of influences on energy balance-related behaviors. Patient Educ. Couns. 2010, 79, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The Cardiovascular Risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N.P.; Anderson, L.H.; Crain, A.L.; Martinson, B.C.; O’Connor, P.J.; Sherwood, N.E.; Whitebird, R.R. Meeting recommendations for multiple healthy lifestyle factors. Prevalence, clustering, and predictors among adolescent, adult, and senior health plan members. Am. J. Prev. Med. 2004, 27, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Ayuso, J.; Aparicio-Ugarriza, R.; Castillo, A.; Ruiz, E.; Ávila, J.M.; Aranceta-Batrina, J.; Gil, Á.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; et al. Physical Activity Patterns of the Spanish Population Are Mostly Determined by Sex and Age: Findings in the ANIBES Study. PLoS ONE 2016, 11, e0149969. [Google Scholar] [CrossRef] [PubMed]
- Hunsberger, M.; Mehlig, K.; Börnhorst, C.; Hebestreit, A.; Moreno, L.; Veidebaum, T.; Kourides, Y.; Siani, A.; Molnar, D.; Sioen, I.; et al. Dietary Carbohydrate and Nocturnal Sleep Duration in Relation to Children’s BMI: Findings from the IDEFICS Study in Eight European Countries. Nutrients 2015, 7, 10223–10236. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Wittert, G.; Taylor, A.W.; Adams, R.; Shi, Z. Associations between Macronutrient Intake and Obstructive Sleep Apnoea as Well as Self-Reported Sleep Symptoms: Results from a Cohort of Community Dwelling Australian Men. Nutrients 2016, 8, 207. [Google Scholar] [CrossRef] [PubMed]
- El Ansari, W.; Suominen, S.; Berg-Beckhoff, G. Is Healthier Nutrition Behaviour Associated with Better Self-Reported Health and Less Health Complaints? Evidence from Turku, Finland. Nutrients 2015, 7, 8478–8490. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.M.; Castillo, A.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; et al. The ANIBES Study on Energy Balance in Spain: Design, protocol and methodology. Nutrients 2015, 7, 970–998. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.M.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; et al. Energy Intake, Profile, and Dietary Sources in the Spanish Population: Findings of the ANIBES Study. Nutrients 2015, 7, 4739–4762. [Google Scholar] [CrossRef] [PubMed]
- Aranceta Bartrina, J.; Pérez-Rodrigo, C.; Serra-Majem, L.; Tur Marí, J.A.; Mataix Verdú, J.; Tojo Sierra, R.; Ribas Barba, L.; Martinez de Vitoria, E.; Millán Núñez-Cortés, J. Dieta y riesgo cardiovascular en España: Estudio DORICA (III). In Dieta y Riesgo Cardiovascular. Estudio DORICA II; Aranceta, J., Foz, M., Gil, B., Jover, E., Mantilla, T., Millán, J., Monereo, S., Moreno, B., Eds.; Médica Panamericana: Madrid, Spain, 2007; pp. 121–162. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 15th ed.; Pirámide: Madrid, Spain, 2011. [Google Scholar]
- Roman-Viñas, B.; Serra-Majem, L.; Hagströmer, M.; Ribas-Barba, L.; Sjöström, M.; Segura-Cardona, R. International physical activity questionnaire: Reliability and validity in a Spanish population. Eur. J. Sport Sci. 2010, 10, 297–304. [Google Scholar] [CrossRef]
- IPAQ. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. November 2005. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 27 October 2015).
- Bauman, A.; Ainsworth, B.E.; Bull, F.; Craig, C.L.; Hagströmer, M.; Sallis, J.F.; Pratt, M.; Sjöström, M. Progress and Pitfalls in the Use of the International Physical Activity Questionnaire (IPAQ) for Adult Physical Activity Surveillance. J. Phys. Act. Health 2009, 6, S5–S8. [Google Scholar] [CrossRef] [PubMed]
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, L. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2006; pp. 1–137. [Google Scholar]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Everitt, B.S.; Landau, S.; Leese, M.; Stahl, D. Cluster Analysis, 5th ed.; JohnWiley & Sons, Ltd.: West Sussex, UK, 2011. [Google Scholar]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.; Bassett, J. What can we learn from dietary pattern analysis? Public Health Nutr. 2016, 19, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Varraso, R.; Garcia-Aymerich, J.; Monier, F.; Le Moual, N.; De Batlle, J.; Miranda, G.; Pison, C.; Romieu, I.; Kauffmann, F.; Maccario, J. Assessment of dietary patterns in nutritional epidemiology: Principal component analysis compared with confirmatory factor analysis. Am. J. Clin. Nutr. 2012, 96, 1079–1092. [Google Scholar] [CrossRef] [PubMed]
- Wadolowska, L.; Kowalkowska, J.; Czarnocinska, J.; Jezewska-Zychowicz, M.; Babicz-Zielinska, E. Comparing dietary patterns derived by two methods and their associations with obesity in Polish girls aged 13–21 years: The cross-sectional GEBaHealth study. Perspect. Public Health 2017, 137, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Wirfalt, A.K.; Jeffery, R.W. Using cluster analysis to examine dietary patterns: Nutrient intakes, gender, and weight status differ across food pattern clusters. J. Am. Diet. Assoc. 1997, 97, 272–279. [Google Scholar] [CrossRef]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodrigo, C.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients 2016, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Allès, B.; Samieri, C.; Lorrain, S.; Jutand, M.A.; Carmichael, P.H.; Shatenstein, B.; Gaudreau, P.; Payette, H.; Laurin, D.; Barberger-Gateau, P. Nutrient Patterns and Their Food Sources in Older Persons from France and Quebec: Dietary and Lifestyle Characteristics. Nutrients 2016, 8, 225. [Google Scholar] [CrossRef] [PubMed]
- Blondin, S.A.; Mueller, M.P.; Bakun, P.J.; Choumenkovitch, S.F.; Tucker, K.L.; Economos, C.D. Cross-Sectional Associations between Empirically-Derived Dietary Patterns and Indicators of Disease Risk among University Students. Nutrients 2016, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Appannah, G.; Pot, G.K.; Huang, R.C.; Oddy, W.H.; Beilin, L.J.; Mori, T.A.; Jebb, S.A.; Ambrosini, G.L. Identification of a dietary pattern associated with greater cardiometabolic risk in adolescence. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.K.; Edwards, S.; Grieger, J.A. The Relationship between Dietary Patterns and Metabolic Health in a Representative Sample of Adult Australians. Nutrients 2015, 7, 6491–6505. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Zheng, P.F.; Zhang, X.Y.; Si, C.J.; Yu, X.L.; Gao, W.; Zhang, L.; Liao, D. Association between Dietary Patterns and the Indicators of Obesity among Chinese: A Cross-Sectional Study. Nutrients 2015, 7, 7995–8009. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Muller, D.; Hallfrisch, J.; Andres, R.; Tucker, K.L. Food patterns measured by factor analysis and anthropometric changes in adults. Am. J. Clin. Nutr. 2004, 80, 504–513. [Google Scholar] [PubMed]
- Johns, D.J.; Lindroos, A.K.; Jebb, S.A.; Sjostrom, L.; Carlsson, L.M.; Ambrosini, G.L. Dietary patterns, cardiometabolic risk factors, and the incidence of cardiovascular disease in severe obesity. Obesity 2015, 23, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.D.; Brage, S.; Forouhi, N.G.; Griffin, S.J.; Wareham, N.J.; Monsivais, P. Does the importance of dietary costs for fruit and vegetable intake vary by socioeconomic position? Br. J. Nutr. 2015, 114, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- de Azevedo Barros, M.B.; Guimarães Lima, M.; Barbosa Medina, L.P.; Landman Szwarcwald, C.; Carvalho Malta, D. Social inequalities in health behaviors among Brazilian adults: National Health Survey, 2013. Int. J. Equity Health 2016, 15, 148. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, S.; Chau, J.Y.; Catt, M.; Bauman, A.; Trenell, M.I. Low physical activity, high television viewing and poor sleep duration cluster in overweight and obese adults; a cross-sectional study of 398,984 participants from the UK Biobank. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health 2016, 16, 657. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Mixed Diet-Physically Active-Low Sedentary Lifestyle Pattern | Not Poor Diet-Low Physical Activity-Low Sedentary Lifestyle Pattern | Poor Diet-Low Physical Activity-Sedentary Lifestyle Pattern | All | χ2 | p | |||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | |||
| All | 210 | 13.0 | 1020 | 63.3 | 381 | 23.6 | 1611 | ||
| Gender | |||||||||
| Men | 151 | 71.9 | 423 | 41.5 | 204 | 53.5 | 778 | 70.1 | 0.000 |
| Women | 59 | 28.1 | 597 | 58.5 | 177 | 46.5 | 833 | ||
| Age group | |||||||||
| 18–30 years | 61 | 29.0 | 213 | 20.9 | 139 | 36.5 | 413 | 60.3 | 0.000 |
| 31–49 years | 110 | 52.4 | 487 | 47.7 | 183 | 48.0 | 780 | ||
| 50–64 years | 39 | 18.6 | 320 | 31.4 | 59 | 15.5 | 418 | ||
| Educational level | 27.8 | 0.000 | |||||||
| Primary or less | 55 | 26.2 | 304 | 29.8 | 73 | 19.2 | 432 | ||
| Secondary | 95 | 45.2 | 507 | 49.7 | 189 | 49.6 | 791 | ||
| Higher | 60 | 28.6 | 209 | 20.5 | 119 | 31.2 | 388 | ||
| Geographical area | |||||||||
| North-northwest | 36 | 17.1 | 166 | 16.3 | 74 | 19.4 | 276 | 4.7 | 0.577 |
| Eastern-Mediterranean | 70 | 33.3 | 350 | 34.3 | 127 | 33.3 | 547 | ||
| Center | 48 | 22.9 | 233 | 22.8 | 96 | 25.2 | 377 | ||
| South | 56 | 26.7 | 271 | 26.6 | 84 | 22.0 | 411 | ||
| BMI status | |||||||||
| Normal weight | 88 | 41.9 | 385 | 37.7 | 177 | 46.5 | 650 | 17.3 | 0.002 |
| Overweight | 90 | 42.9 | 386 | 37.8 | 136 | 35.7 | 612 | ||
| Obese | 32 | 15.2 | 249 | 24.4 | 68 | 17.8 | 349 | ||
| Mixed Diet-Physically Active-Low Sedentary Lifestyle Pattern | Not Poor Diet-Low Physical Activity-Low Sedentary Lifestyle Pattern | Poor Diet-Low Physical Activity-Sedentary Lifestyle Pattern | F | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Mean | SD | Median | Mean | SD | Median | |||
| Men | n = 151 | n = 423 | n = 204 | ||||||||
| “Traditional DP” score | 0.04 | 1.03 | 0.00 | 0.05 | 1.04 | 0.00 | −0.03 | 0.95 | 0.00 | 1.2 | 0.314 |
| “Mediterranean DP” score | 0.25 | 1.35 | 0.06 | −0.17 | 1.00 | −0.23 | −0.12 | 0.96 | −0.09 | 8.0 | 0.000 |
| “Snack DP” score | 0.66 | 1.29 | 0.52 | 0.14 | 0.95 | 0.07 | 0.46 | 1.14 | 0.31 | 9.9 | 0.000 |
| “Dairy-sweet DP” score | −0.05 | 0.99 | −0.11 | −0.49 | 0.61 | −0.51 | 1.03 | 1.21 | 0.88 | 126.9 | 0.000 |
| Walking (min/week) | 447.8 | 434.4 | 240.0 | 284.7 | 291.7 | 210.0 | 240.7 | 274.9 | 150.0 | 20.3 | 0.000 |
| Moderate PA (min/week) | 478.4 | 426.9 | 360.0 | 321.1 | 360.1 | 180.0 | 174.1 | 234.8 | 112.5 | 32.8 | 0.000 |
| Vigorous PA (min/week) | 706.4 | 291.7 | 720.0 | 81.8 | 127.3 | 0.0 | 102.3 | 155.4 | 0.0 | 734.1 | 0.000 |
| Sedentary time (h/day) | 3.6 | 2.0 | 3.0 | 4.4 | 2.3 | 4.0 | 7.1 | 3.7 | 6.4 | 96.8 | 0.000 |
| Sleeping (h/day) | 6.6 | 2.3 | 7.0 | 7.1 | 1.9 | 7.5 | 7.0 | 2.0 | 7.0 | 3.9 | 0.021 |
| Smoking (cig/day) | 4.3 | 6.9 | 0.0 | 6.4 | 8.7 | 0.0 | 3.1 | 6.0 | 0.0 | 10.2 | 0.000 |
| Women | n = 59 | n = 597 | n = 177 | ||||||||
| “Traditional DP” score | −0.30 | 1.02 | −0.20 | 0.02 | 0.96 | −0.02 | −0.12 | 1.00 | −0.10 | 7.2 | 0.001 |
| “Mediterranean DP” score | 0.33 | 1.06 | 0.45 | 0.03 | 0.89 | 0.05 | 0.09 | 0.92 | 0.09 | 7.2 | 0.001 |
| “Snack DP” score | −0.20 | 0.94 | −0.37 | −0.38 | 0.75 | −0.49 | −0.12 | 0.82 | −0.29 | 7.2 | 0.001 |
| Dairy-sweet DP’ score | 0.03 | 0.74 | −0.02 | −0.33 | 0.60 | −0.36 | 1.16 | 0.89 | 1.09 | 203.0 | 0.000 |
| Walking (min/week) | 528.6 | 364.1 | 420.0 | 267.0 | 270.2 | 180.0 | 247.5 | 263.0 | 180.0 | 25.6 | 0.000 |
| Moderate PA (min/week) | 740.3 | 399.6 | 750.0 | 545.8 | 442.9 | 420.0 | 316.9 | 332.2 | 210.0 | 25.2 | 0.000 |
| Vigorous PA (min/week) | 692.0 | 325.3 | 630.0 | 45.9 | 92.2 | 0.0 | 57.8 | 120.2 | 0.0 | 685.4 | 0.000 |
| Sedentary time (h/day) | 3.6 | 2.1 | 3.0 | 4.0 | 2.2 | 4.0 | 6.6 | 4.1 | 6.0 | 60.5 | 0.000 |
| Sleeping (h/day) | 6.2 | 2.5 | 7.0 | 7.1 | 1.9 | 7.5 | 7.0 | 2.2 | 7.5 | 6.3 | 0.002 |
| Smoking (cig/day) | 2.5 | 5.6 | 0.0 | 3.9 | 7.0 | 0.0 | 2.3 | 5.2 | 0.0 | 4.5 | 0.011 |
| Mixed Diet-Physically Active-Low Sedentary Lifestyle Pattern | Not Poor Diet-Low Physical Activity-Low Sedentary Lifestyle Pattern | Poor Diet-Low Physical Activity-Sedentary Lifestyle Pattern | F | p | |||||||
| Mean | SD | Median | Mean | SD | Median | Mean | SD | Median | |||
| Men (n = 781) | (n = 151) | (n = 423) | (n = 204) | ||||||||
| Vegetables (g/day) | 184.9 | 110.9 | 165.4 | 185.1 | 112.4 | 162.5 | 178.2 | 97.2 | 165.0 | 0.98 | 0.374 |
| Fruit (g/day) | 183.1 | 231.0 | 136.7 | 145.0 | 172.7 | 97.5 | 139.5 | 144.0 | 103.9 | 3.24 | 0.040 |
| Legumes (g/day) | 16.7 | 23.1 | 7.5 | 16.2 | 19.1 | 10.5 | 13.6 | 18.2 | 7.1 | 2.19 | 0.113 |
| Meat (g/day) | 127.2 | 92.3 | 111.7 | 109.8 | 75.3 | 95.8 | 124.9 | 77.4 | 116.3 | 0.56 | 0.573 |
| Processed and cold meats (g/day) | 55.8 | 46.6 | 44.3 | 42.5 | 36.0 | 34.2 | 50.3 | 39.1 | 45.9 | 2.46 | 0.086 |
| Fish (g/day) | 73.6 | 90.8 | 47.7 | 62.5 | 66.9 | 39.3 | 55.8 | 57.1 | 35.4 | 3.01 | 0.050 |
| Eggs (g/day) | 40.8 | 46.4 | 31.3 | 32.5 | 33.4 | 21.3 | 28.3 | 30.4 | 20.0 | 9.58 | 0.000 |
| Milk (mL/day) | 155.5 | 122.9 | 139.7 | 125.6 | 100.7 | 115.0 | 267.5 | 178.5 | 249.4 | 60.42 | 0.000 |
| Cheese (g/day) | 25.4 | 41.4 | 15.2 | 15.8 | 20.0 | 10.0 | 19.2 | 22.2 | 12.9 | 4.39 | 0.013 |
| Yoghourt (g/day) | 62.3 | 74.5 | 41.7 | 42.3 | 64.2 | 0.0 | 46.2 | 62.0 | 20.8 | 3.62 | 0.027 |
| Pasta (g/day) | 22.6 | 27.5 | 12.5 | 16.2 | 20.0 | 11.7 | 17.7 | 20.2 | 11.7 | 3.08 | 0.047 |
| Bread (g/day) | 94.4 | 57.4 | 83.3 | 83.6 | 44.6 | 80.0 | 97.5 | 58.2 | 85.0 | 1.15 | 0.318 |
| Cakes and pastry (g/day) | 30.3 | 36.1 | 16.7 | 21.1 | 25.7 | 11.7 | 57.8 | 46.3 | 50.2 | 44.80 | 0.000 |
| Sugar and sweets (g/day) | 15.0 | 15.4 | 10.0 | 10.0 | 9.8 | 7.5 | 24.7 | 18.5 | 21.8 | 43.23 | 0.000 |
| Pre-cooked foods (g/day) | 73.0 | 83.0 | 50.0 | 76.3 | 86.9 | 45.8 | 80.0 | 91.3 | 46.3 | 3.45 | 0.032 |
| Savory snacks (g/day) | 6.1 | 12.1 | 0.0 | 4.7 | 10.1 | 0.0 | 7.5 | 14.3 | 0.0 | 0.51 | 0.603 |
| Olive oil (mL/day) | 20.0 | 8.9 | 20.2 | 18.0 | 8.8 | 16.7 | 17.3 | 7.5 | 18.0 | 6.40 | 0.002 |
| Juices (mL/day) | 71.0 | 123.9 | 0.0 | 40.0 | 79.8 | 0.0 | 88.6 | 175.4 | 0.0 | 1.51 | 0.221 |
| Sugar sweetened soft drinks (mL/day) | 104.2 | 151.5 | 41.7 | 97.7 | 186.7 | 0.0 | 127.2 | 192.2 | 47.5 | 2.44 | 0.088 |
| Water (mL/day) | 843.4 | 647.7 | 695.8 | 638.0 | 537.2 | 513.3 | 757.4 | 582.2 | 685.0 | 3.62 | 0.027 |
| Alcoholic beverages (mL/day) | 186.1 | 259.4 | 71.7 | 176.4 | 241.2 | 58.3 | 102.7 | 181.9 | 0.0 | 14.33 | 0.000 |
| Low alcohol content bevs (mL/day) | 1.6 | 5.7 | 0.0 | 2.8 | 11.6 | 0.0 | 3.4 | 19.4 | 0.0 | 2.95 | 0.05 |
| High alcohol content bevs (mL/day) | 184.5 | 257.6 | 71.7 | 173.6 | 238.8 | 55.8 | 99.3 | 177.3 | 0.0 | 14.31 | 0.00 |
| Mixed Diet-Physically Active-Low Sedentary Lifestyle Pattern | Not Poor Diet-Low Physical Activity-Low Sedentary Lifestyle Pattern | Poor Diet-Low Physical Activity-Sedentary Lifestyle Pattern | F | p | |||||||
| Mean | SD | Median | Mean | SD | Median | Mean | SD | Median | |||
| Women (n = 833) | n = 59 | n = 597 | n = 177 | ||||||||
| Vegetables (g/day) | 168.5 | 90.6 | 156.2 | 195.3 | 115.3 | 168.8 | 174.4 | 110.4 | 162.6 | 5.197 | 0.006 |
| Fruit (g/day) | 186.5 | 175.6 | 152.5 | 162.4 | 173.0 | 111.5 | 143.8 | 147.0 | 110.0 | 0.929 | 0.395 |
| Legumes (g/day) | 10.9 | 13.8 | 5.0 | 14.7 | 18.7 | 10.0 | 13.6 | 24.2 | 3.3 | 1.433 | 0.239 |
| Meat (g/day) | 78.8 | 63.1 | 66.7 | 90.9 | 63.4 | 82.5 | 101.6 | 70.1 | 89.2 | 2.054 | 0.129 |
| Processed and cold meats (g/day) | 37.1 | 31.5 | 29.7 | 33.5 | 30.1 | 26.7 | 37.5 | 32.2 | 29.2 | 1.582 | 0.206 |
| Fish (g/day) | 55.4 | 50.4 | 45.0 | 59.8 | 62.9 | 40.0 | 58.1 | 65.9 | 38.3 | 0.142 | 0.868 |
| Eggs (g/day) | 25.9 | 26.3 | 21.3 | 25.0 | 24.7 | 20.7 | 24.5 | 24.2 | 19.5 | 1.497 | 0.224 |
| Milk (mL/day) | 175.0 | 104.7 | 175.0 | 148.2 | 103.1 | 141.7 | 271.2 | 138.3 | 255.0 | 72.001 | 0.000 |
| Cheese (g/day) | 20.1 | 20.5 | 12.5 | 15.1 | 17.1 | 10.0 | 18.7 | 21.3 | 13.3 | 1.289 | 0.276 |
| Yoghourt (g/day) | 53.9 | 56.7 | 30.8 | 43.7 | 57.2 | 20.8 | 51.4 | 58.7 | 22.5 | 2.550 | 0.079 |
| Pasta (g/day) | 18.7 | 20.5 | 11.7 | 14.5 | 19.1 | 8.3 | 15.4 | 19.7 | 10.8 | 1.768 | 0.171 |
| Bread (g/day) | 64.8 | 38.4 | 56.7 | 65.7 | 39.6 | 60.0 | 66.7 | 33.7 | 64.2 | 11.989 | 0.000 |
| Cakes and pastry (g/day) | 31.6 | 37.1 | 20.7 | 20.9 | 22.6 | 15.0 | 56.3 | 40.9 | 50.0 | 54.345 | 0.000 |
| Sugar and sweets (g/day) | 15.6 | 12.4 | 13.7 | 11.3 | 11.3 | 8.2 | 30.2 | 25.0 | 25.3 | 52.816 | 0.000 |
| Pre-cooked foods (g/day) | 63.1 | 77.6 | 41.7 | 61.1 | 71.6 | 41.7 | 58.0 | 61.5 | 41.7 | 4.561 | 0.011 |
| Savory snacks (g/day) | 5.9 | 9.6 | 0.0 | 3.4 | 7.4 | 0.0 | 9.0 | 14.8 | 2.0 | 7.045 | 0.001 |
| Olive oil (mL/day) | 17.2 | 8.2 | 15.8 | 17.9 | 7.8 | 17.3 | 17.3 | 8.5 | 17.0 | 6.580 | 0.001 |
| Juices (mL/day) | 51.0 | 80.5 | 0.0 | 32.5 | 60.0 | 0.0 | 61.3 | 86.8 | 13.3 | 3.348 | 0.036 |
| Sugar sweetened soft drinks (mL/day) | 60.5 | 130.2 | 0.0 | 77.9 | 149.7 | 0.0 | 96.4 | 159.7 | 33.3 | 3.543 | 0.029 |
| Water (mL/day) | 764.2 | 563.1 | 658.3 | 649.0 | 474.2 | 550.0 | 753.6 | 560.2 | 641.7 | 4.689 | 0.009 |
| Alcoholic beverages (mL/day) | 84.4 | 132.5 | 30.0 | 68.5 | 141.6 | 0.0 | 47.0 | 100.4 | 0.0 | 8.842 | 0.000 |
| Low alcohol content bevs (mL/day) | 1.1 | 4.1 | 0.0 | 1.4 | 10.5 | 0.0 | 1.6 | 7.3 | 0.0 | 1.518 | 0.220 |
| High alcohol content bevs (mL/day) | 83.3 | 131.2 | 30.0 | 67.2 | 140.5 | 0.0 | 45.5 | 97.8 | 0.0 | 8.516 | 0.000 |
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| POR | 95% C.I.POR | p | POR | 95% C.I.POR | p | |||
| Lower | Upper | Lower | Upper | |||||
| Age group | ||||||||
| 50–64 years | 0.000 | 0.000 | ||||||
| 18–30 years | 0.29 | 0.17 | 0.48 | 0.000 | 0.29 | 0.16 | 0.52 | 0.000 |
| 31–49 years | 0.61 | 0.42 | 0.89 | 0.011 | 0.52 | 0.35 | 0.78 | 0.002 |
| Level of education | ||||||||
| High | 0.293 | 0.000 | ||||||
| Primary or less | 1.41 | 0.87 | 2.28 | 0.162 | 3.11 | 1.74 | 5.58 | 0.000 |
| Secondary | 1.08 | 0.69 | 1.69 | 0.730 | 1.85 | 1.06 | 3.24 | 0.031 |
| Geographical area | ||||||||
| South | 0.017 | 0.704 | ||||||
| North-northwest | 1.13 | 0.65 | 1.99 | 0.658 | 0.83 | 0.45 | 1.50 | 0.532 |
| Eastern-Mediterranean | 1.99 | 1.25 | 3.16 | 0.003 | 1.11 | 0.70 | 1.76 | 0.672 |
| Center | 1.45 | 0.88 | 2.40 | 0.141 | 0.88 | 0.51 | 1.52 | 0.649 |
| Lifestyle pattern | ||||||||
| Poor diet-low physical activity-sedentary lifestyle pattern | 0.058 | 0.648 | ||||||
| Mixed diet-physically active-low sedentary lifestyle pattern | 0.52 | 0.29 | 0.93 | 0.027 | 1.16 | 0.48 | 2.80 | 0.738 |
| Not poor diet-low physical activity-low sedentary lifestyle pattern | 0.92 | 0.59 | 1.44 | 0.726 | 1.30 | 0.75 | 2.25 | 0.358 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Rodrigo, C.; Gianzo-Citores, M.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Lifestyle Patterns and Weight Status in Spanish Adults: The ANIBES Study. Nutrients 2017, 9, 606. https://doi.org/10.3390/nu9060606
Pérez-Rodrigo C, Gianzo-Citores M, Gil Á, González-Gross M, Ortega RM, Serra-Majem L, Varela-Moreiras G, Aranceta-Bartrina J. Lifestyle Patterns and Weight Status in Spanish Adults: The ANIBES Study. Nutrients. 2017; 9(6):606. https://doi.org/10.3390/nu9060606
Chicago/Turabian StylePérez-Rodrigo, Carmen, Marta Gianzo-Citores, Ángel Gil, Marcela González-Gross, Rosa M. Ortega, Lluis Serra-Majem, Gregorio Varela-Moreiras, and Javier Aranceta-Bartrina. 2017. "Lifestyle Patterns and Weight Status in Spanish Adults: The ANIBES Study" Nutrients 9, no. 6: 606. https://doi.org/10.3390/nu9060606