Pre-Pregnancy Body Mass Index Is Associated with Dietary Inflammatory Index and C-Reactive Protein Concentrations during Pregnancy

 ,
,
Abstract
:1. Introduction
2. Material and Methods
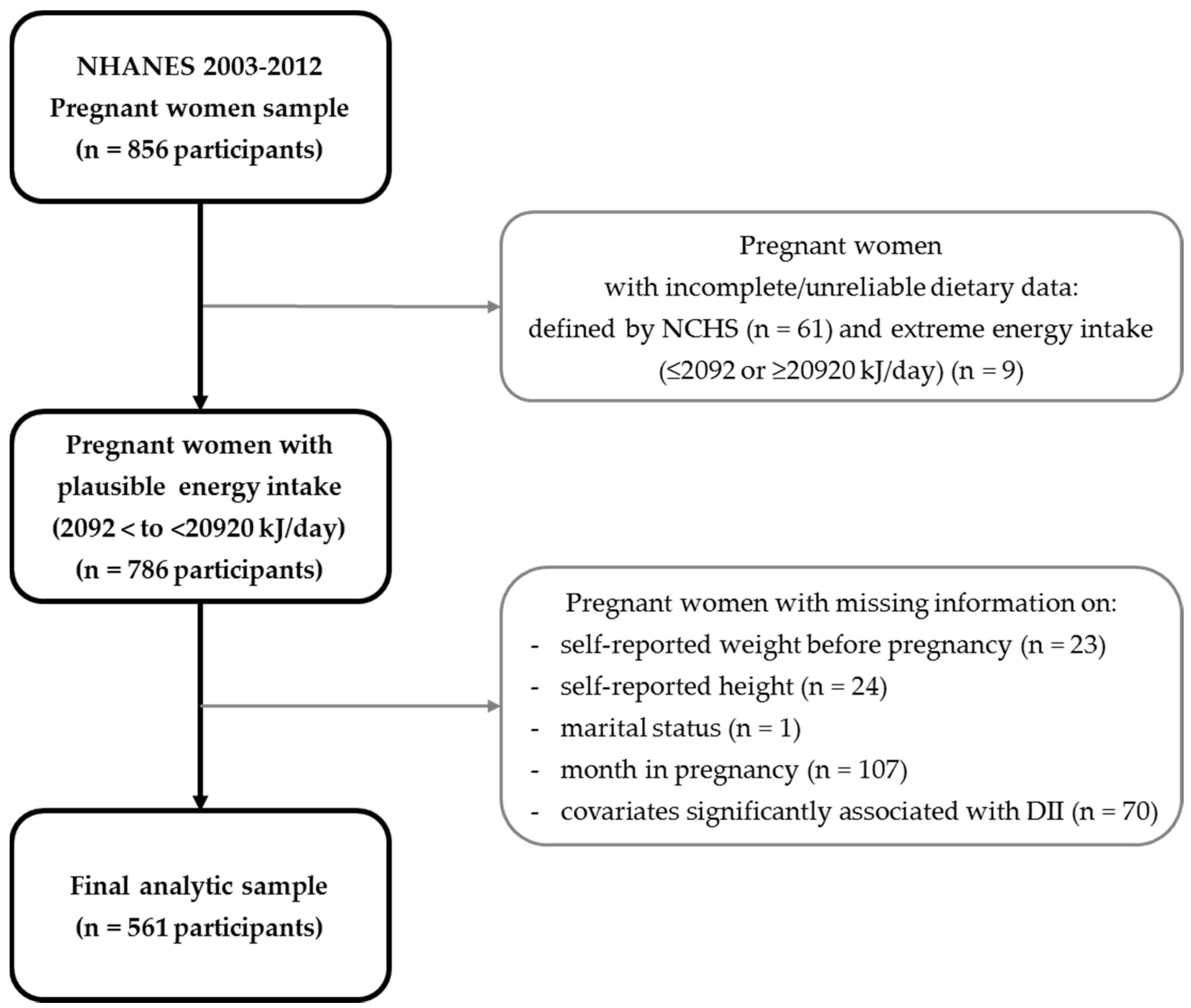
2.1. Study Population
2.2. Exposure Variable
2.3. Outcome Variables
2.3.1. Dietary Inflammatory Index (DII)
2.3.2. C-Reactive Protein (CRP)
2.4. Covariates
2.5. Statistical Analyses
3. Results
4. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Shin, D.; Song, W.O. Prepregnancy body mass index is an independent risk factor for gestational hypertension, gestational diabetes, preterm labor, and small- and large-for-gestational-age infants. J. Matern. Fetal Neonatal Med. 2015, 28, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.; Sandler, L.; Hsu, K.; Vossen-Smirnakis, K.; Ecker, J.L.; Thadhani, R. First-trimester C-reactive protein and subsequent gestational diabetes. Diabetes Care 2003, 26, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Qiu, C.; Sorensen, T.K.; Luthy, D.A.; Williams, M.A. A prospective study of maternal serum C-reactive protein (CRP) concentrations and risk of gestational diabetes mellitus. Paediatr. Perinat. Epidemiol. 2004, 18, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Bullen, B.L.; Jones, N.M.; Holzman, C.B.; Tian, Y.; Senagore, P.K.; Thorsen, P.; Skogstrand, K.; Hougaard, D.M.; Sikorskii, A. C-reactive protein and preterm delivery: Clues from placental findings and maternal weight. Reprod. Sci. 2013, 20, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Teran, E.; Escudero, C.; Moya, W.; Flores, M.; Vallance, P.; Lopez-Jaramillo, P. Elevated C-reactive protein and pro-inflammatory cytokines in Andean women with pre-eclampsia. Int. J. Gynaecol. Obstet. 2001, 75, 243–249. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Ness, R.B.; Harger, G.F.; Roberts, J.M. Inflammation and triglycerides partially mediate the effect of prepregnancy body mass index on the risk of preeclampsia. Am. J. Epidemiol. 2005, 162, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Pre-pregnancy weight status is associated with diet quality and nutritional biomarkers during pregnancy. Nutrients 2016, 8, 162. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.A.; Bodnar, L.M.; Siega-Riz, A.M. Pregravid body mass index is negatively associated with diet quality during pregnancy. Public Health Nutr. 2007, 10, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Tsigga, M.; Filis, V.; Hatzopoulou, K.; Kotzamanidis, C.; Grammatikopoulou, M.G. Healthy Eating Index during pregnancy according to pre-gravid and gravid weight status. Public Health Nutr. 2011, 14, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Esmaillzadeh, A.; Kimiagar, M.; Mehrabi, Y.; Azadbakht, L.; Hu, F.B.; Willett, W.C. Fruit and vegetable intakes, C-reactive protein, and the metabolic syndrome. Am. J. Clin. Nutr. 2006, 84, 1489–1497. [Google Scholar] [PubMed]
- Ma, Y.; Griffith, J.A.; Chasan-Taber, L.; Olendzki, B.C.; Jackson, E.; Stanek, E.J.; Li, W.; Pagoto, S.L.; Hafner, A.R.; Ockene, I.S. Association between dietary fiber and serum C-reactive protein. Am. J. Clin. Nutr. 2006, 83, 760–766. [Google Scholar] [PubMed]
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. 2013, 4, 384S–392S. [Google Scholar] [CrossRef] [PubMed]
- Hermsdorff, H.H.M.; Barbosa, K.B.; Volp, A.C.P.; Puchau, B.; Bressan, J.; Zulet, M.A.; Martínez, J.A. Vitamin C and fibre consumption from fruits and vegetables improves oxidative stress markers in healthy young adults. Br. J. Nutr. 2012, 107, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Cavicchia, P.P.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Hébert, J.R. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J. Nutr. 2009, 139, 2365–2372. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hebert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L.; et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hussey, J.R.; Ma, Y.; Hebert, J.R. Inflammatory potential of diet and all-cause, cardiovascular, and cancer mortality in National Health and Nutrition Examination Survey III Study. Eur. J. Nutr. 2015, 56, 683. [Google Scholar] [CrossRef] [PubMed]
- Deng, F.E.; Shivappa, N.; Tang, Y.; Mann, J.R.; Hebert, J.R. Association between diet-related inflammation, all-cause, all-cancer, and cardiovascular disease mortality, with special focus on prediabetics: Findings from NHANES III. Eur. J. Nutr. 2016, 56, 1085. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Arellano, A.; Ramallal, R.; Ruiz-Canela, M.; Salas-Salvado, J.; Corella, D.; Shivappa, N.; Schroder, H.; Hebert, J.R.; Ros, E.; Gomez-Garcia, E.; et al. Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the PREDIMED Study. Nutrients 2015, 7, 4124–4138. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.M.; Bassett, J.K.; Shivappa, N.; Hebert, J.R.; English, D.R.; Giles, G.G.; Severi, G. Dietary inflammatory index, Mediterranean diet score, and lung cancer: A prospective study. Cancer Causes Control 2016, 27, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Rosato, V.; Serraino, D.; La Vecchia, C. Inflammatory potential of diet and risk of laryngeal cancer in a case-control study from Italy. Cancer Causes Control 2016, 27, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Kesse-Guyot, E.; Assmann, K.E.; Andreeva, V.A.; Touvier, M.; Neufcourt, L.; Shivappa, N.; Hebert, J.R.; Wirth, M.D.; Hercberg, S.; Galan, P.; et al. Long-term association between the dietary inflammatory index and cognitive functioning: Findings from the SU.VI.MAX study. Eur. J. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary patterns during pregnancy are associated with gestational weight gain. Matern. Child Health J. 2016, 20, 2527–2538. [Google Scholar] [CrossRef] [PubMed]
- Grieger, J.A.; Grzeskowiak, L.E.; Clifton, V.L. Preconception dietary patterns in human pregnancies are associated with preterm delivery. J. Nutr. 2014, 144, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.M.; Wall, C.; Becroft, D.M.; Robinson, E.; Wild, C.J.; Mitchell, E.A. Maternal dietary patterns in pregnancy and the association with small-for-gestational-age infants. Br. J. Nutr. 2010, 103, 1665–1673. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.A.; Maslova, E.; Halldorsson, T.I.; Olsen, S.F. Characterization of dietary patterns in the danish national birth cohort in relation to preterm birth. PLoS ONE 2014, 9, e93644. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary patterns during pregnancy are associated with risk of gestational diabetes mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef] [PubMed]
- Vujkovic, M.; Steegers, E.A.; Looman, C.W.; Ocke, M.C.; van der Spek, P.J.; Steegers-Theunissen, R.P. The maternal Mediterranean dietary pattern is associated with a reduced risk of spina bifida in the offspring. BJOG Int. J. Obstet. Gynaecol. 2009, 116, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Obermann-Borst, S.A.; Vujkovic, M.; de Vries, J.H.; Wildhagen, M.F.; Looman, C.W.; de Jonge, R.; Steegers, E.A.; Steegers-Theunissen, R.P. A maternal dietary pattern characterised by fish and seafood in association with the risk of congenital heart defects in the offspring. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 1205–1215. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Murakami, K.; Hirota, Y.; Kanzaki, H.; Kitada, M.; Horikoshi, Y.; Ishiko, O.; et al. Maternal dietary patterns in pregnancy and fetal growth in Japan: The Osaka Maternal and Child Health Study. Br. J. Nutr. 2012, 107, 1526–1533. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.A.; McAuliffe, F.M. Maternal dietary patterns and associated nutrient intakes during each trimester of pregnancy. Public Health Nutr. 2013, 16, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Pick, M.E.; Edwards, M.; Moreau, D.; Ryan, E.A. Assessment of diet quality in pregnant women using the Healthy Eating Index. J. Am. Diet. Assoc. 2005, 105, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary quality during pregnancy varies by maternal characteristics in Project Viva: A US cohort. J. Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Bianchi, L.; Chung, H.; Weatherspoon, L.; Song, W.O. Is gestational weight gain associated with diet quality during pregnancy? Matern. Child Health J. 2014, 18, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Sotres-Alvarez, D.; Herring, A.H.; Siega-Riz, A.M. Latent class analysis is useful to classify pregnant women into dietary patterns. J. Nutr. 2010, 140, 2253–2259. [Google Scholar] [CrossRef] [PubMed]
- Sotres-Alvarez, D.; Siega-Riz, A.M.; Herring, A.H.; Carmichael, S.L.; Feldkamp, M.L.; Hobbs, C.A.; Olshan, A.F. Maternal dietary patterns are associated with risk of neural tube and congenital heart defects. Am. J. Epidemiol. 2013, 177, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health/objectives (accessed on 10 November 2016).
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey 2003–2004 Data Documentation, Codebook, and Frequency: Demographic Variables and Sample Weights (DEMO_C). Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2003–2004/DEMO_C.htm#Component_Description (accessed on 27 February 2016).
- Johnson, C.L.; Paulose-Ram, R.; Ogden, C.E.; Carroll, M.D.; Kruszon-Moran, D.; Dohrmann, S.M.; Curtin, L.R. National Health and Nutrition Examination Survey: Analytic guidelines, 1999–2010; National Center for Health Statistics, Vital and Health Statistics: Washington, DC, USA, 2013; Volume 2.
- Centers for Disease Control and Prevention, National Center for Health Statistic. Dietary Interview—Total nutrient Intakes, First Day. Available online: http://wwwn.cdc.gov/Nchs/Nhanes/2011–2012/DR1TOT_G.htm#DR1DRSTZ (accessed on 29 September 2016).
- Shin, D.; Chung, H.; Weatherspoon, L.; Song, W.O. Validity of prepregnancy weight status estimated from self-reported height and weight. Matern. Child Health J. 2014, 18, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organization Technical Report Series; World Health Organization: Geneva, Switzerland, 1995; Volume 854, pp. 1–452. [Google Scholar]
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey 2003–2004 Data Documentation, Codebook, and Frequency: C-Reactive Protein (CRP), Bone Alkaline Phosphatase (BAP) & Parathyroid Hormone (PTH) (L11_C). Available online: http://wwwn.cdc.gov/Nchs/Nhanes/2003–2004/L11_C.htm (accessed on 10 November 2016).
- Centers for Disease Control and Prevention; National Center for Health Statistic. National Health and Nutiriton Examination Survey 2005–2006 Data Documentation, Codebook, and Frequencies: C-Reactive Protein (CRP) (CRP_D). Available online: http://wwwn.cdc.gov/Nchs/Nhanes/2005–2006/CRP_D.htm#LBXCRP (accessed on 10 November 2016).
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey 2007–2008 Data Documentation, Codebook, and Frequencies: C-Reactive Protein (CRP) (CRP_E). Available online: http://wwwn.cdc.gov/Nchs/Nhanes/2007-2008/CRP_E.htm (accessed on 10 November 2016).
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey 2009–2010 Data Documentation, Codebook, and Frequencies: C-Reactive Protein (CRP) (CRP_F). Available online: http://wwwn.cdc.gov/Nchs/Nhanes/2009-2010/CRP_F.htm (accessed on 10 November 2016).
- Panagos, P.G.; Vishwanathan, R.; Penfield-Cyr, A.; Matthan, N.R.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Sen, S. Breastmilk from obese mothers has pro-inflammatory properties and decreased neuroprotective factors. J. Perinatol. 2016, 36, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Nettleton, J.A.; Steffen, L.M.; Mayer-Davis, E.J.; Jenny, N.S.; Jiang, R.; Herrington, D.M.; Jacobs, D.R., Jr. Dietary patterns are associated with biochemical markers of inflammation and endothelial activation in the Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2006, 83, 1369–1379. [Google Scholar] [PubMed]
- North, C.J.; Venter, C.S.; Jerling, J.C. The effects of dietary fibre on C-reactive protein, an inflammation marker predicting cardiovascular disease. Eur. J. Clin. Nutr. 2009, 63, 921–933. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Shipley, M.; Armitage, J.; Collins, R.; Harris, W. Plasma phospholipid fatty acids and CHD in older men: Whitehall study of London civil servants. Br. J. Nutr. 2009, 102, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Timpson, N.J.; Nordestgaard, B.G.; Harbord, R.M.; Zacho, J.; Frayling, T.M.; Tybjaerg-Hansen, A.; Smith, G.D. C-reactive protein levels and body mass index: Elucidating direction of causation through reciprocal Mendelian randomization. Int. J. Obes. 2011, 35, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Rawson, E.S.; Freedson, P.S.; Osganian, S.K.; Matthews, C.E.; Reed, G.; Ockene, I.S. Body mass index, but not physical activity, is associated with C-reactive protein. Med. Sci. Sports Exerc. 2003, 35, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Galuska, D.A.; Gillespie, C.; Will, J.C.; Giles, W.H.; Dietz, W.H. C-reactive protein and body mass index in children: Findings from the Third National Health and Nutrition Examination Survey, 1988–1994. J. Pediatr. 2001, 138, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Challier, J.C.; Basu, S.; Bintein, T.; Minium, J.; Hotmire, K.; Catalano, P.M.; Hauguel-de Mouzon, S. Obesity in pregnancy stimulates macrophage accumulation and inflammation in the placenta. Placenta 2008, 29, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, J.E.; Ferrell, W.R.; Crawford, L.; Wallace, A.M.; Greer, I.A.; Sattar, N. Maternal obesity is associated with dysregulation of metabolic, vascular, and inflammatory pathways. J. Clin. Endocrinol. Metab. 2002, 87, 4231–4237. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Wirth, M.D.; Hurley, T.G.; Hebert, J.R. Association between the dietary inflammatory index (DII) and telomere length and C-reactive protein from the National Health and Nutrition Examination Survey-1999–2002. Mol. Nutr. Food Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Von Zglinicki, T. Oxidative stress shortens telomeres. Trends Biochem. Sci. 2002, 27, 339–344. [Google Scholar] [CrossRef]
- Borzychowski, A.; Sargent, I.; Redman, C. Inflammation and Pre-Eclampsia. Semin. Fetal Neonatal Med. 2006, 11, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Basiotis, P.P.; Welsh, S.O.; Cronin, F.J.; Kelsay, J.L.; Mertz, W. Number of days of food intake records required to estimate individual and group nutrient intakes with defined confidence. J. Nutr. 1987, 117, 1638–1641. [Google Scholar] [PubMed]

{kind=link}
| Socio-Demographics and Lifestyle Factors | Pre-Pregnancy BMI 1 | DII | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obese | p Value | Tertile 1 | Tertile 2 | Tertile 3 | p Value | ||||||||
| (n = 31) | (n = 311) | (n = 153) | (n = 136) | (n = 210) | (n = 211) | (n = 210) | ||||||||||
| Mean | SEM | Mean | SEM | Mean | SEM | Mean | SEM | Mean | SEM | Mean | SEM | Mean | SEM | |||
| Maternal Age (years) | 27.5 | 1.4 | 28.1 | 0.6 | 28.5 | 0.9 | 28.1 | 0.8 | 0.8520 | 30.2 | 0.8 | 27.4 | 0.6 | 26.5 | 0.6 | <0.0001 |
| Family Poverty Income Ratio (n = 601) | 2.5 | 0.5 | 3.1 | 0.2 | 2.7 | 0.3 | 2.3 | 0.2 | 0.0013 | 3.1 | 0.2 | 2.7 | 0.2 | 2.6 | 0.2 | 0.0775 |
| Month in Pregnancy | 5.2 | 0.7 | 5.9 | 0.3 | 5.6 | 0.3 | 4.7 | 0.3 | 0.0037 | 5.8 | 0.3 | 5.2 | 0.2 | 5.5 | 0.3 | 0.3511 |
| n | (Wt’d % 2) | n | (Wt’d %) | n | (Wt’d %) | n | (Wt’d %) | n | (Wt’d %) | n | (Wt’d %) | n | (Wt’d %) | |||
| Race/Ethnicity | ||||||||||||||||
| Hispanic | 4 | 2.0 | 93 | 47.4 | 52 | 26.7 | 48 | 23.9 | <0.0001 | 80 | 43.4 | 75 | 35.0 | 42 | 21.6 | 0.0002 |
| Non-Hispanic white | 17 | 3.3 | 152 | 55.8 | 67 | 18.9 | 48 | 22.0 | 91 | 36.3 | 85 | 28.3 | 108 | 35.4 | ||
| Non-Hispanic black | 4 | 5.0 | 39 | 25.8 | 25 | 19.4 | 37 | 49.8 | 17 | 15.4 | 39 | 38.9 | 49 | 45.7 | ||
| Other (including multi-racial) | 6 | 16.6 | 27 | 63.2 | 9 | 15.8 | 3 | 4.4 | 22 | 56.7 | 12 | 31.4 | 11 | 11.9 | ||
| Education | ||||||||||||||||
| ≤High school graduate | 12 | 4.4 | 140 | 42.8 | 85 | 24.5 | 77 | 28.4 | 0.2622 | 91 | 29.5 | 108 | 34.0 | 115 | 36.5 | 0.2086 |
| ≥College | 19 | 4.5 | 171 | 54.6 | 68 | 17.9 | 59 | 23.0 | 119 | 40.4 | 103 | 30.2 | 95 | 29.4 | ||
| Marital Status | ||||||||||||||||
| Married/living with partner | 26 | 4.6 | 244 | 51.4 | 122 | 21.2 | 94 | 22.8 | 0.3537 | 181 | 38.6 | 168 | 32.0 | 137 | 29.4 | 0.2410 |
| Widowed/divorced/separated/single | 5 | 3.8 | 67 | 45.8 | 31 | 16.8 | 42 | 33.5 | 29 | 27.7 | 43 | 29.8 | 73 | 42.5 | ||
| Smoking Status during Pregnancy 3 (n = 585) | ||||||||||||||||
| No | 26 | 4.0 | 255 | 53.5 | 127 | 18.2 | 109 | 24.3 | 0.4225 | 185 | 38.7 | 173 | 29.5 | 159 | 31.8 | 0.0016 |
| Yes | 3 | 8.5 | 38 | 42.9 | 12 | 28.0 | 15 | 20.5 | 8 | 10.1 | 22 | 35.0 | 38 | 54.9 | ||
| Physical Activity (n = 354) | ||||||||||||||||
| Light (0–500 MET 4-min/week) | 10 | 3.8 | 88 | 53.8 | 48 | 20.4 | 41 | 22.0 | 0.8083 | 72 | 39.6 | 47 | 24.3 | 68 | 36.1 | 0.9646 |
| Moderate (500–1000 MET-min/week) | 3 | 2.9 | 49 | 54.2 | 12 | 28.6 | 12 | 14.3 | 30 | 44.2 | 28 | 26.5 | 18 | 29.3 | ||
| Active (≥1000 MET-min/week) | 3 | 2.4 | 53 | 64.0 | 21 | 18.2 | 14 | 15.4 | 36 | 45.7 | 30 | 20.5 | 25 | 33.8 | ||
| Parity (n = 297) | ||||||||||||||||
| None | 0 | . | 11 | 77.2 | 2 | 8.1 | 3 | 14.7 | n/a | 3 | 11.6 | 5 | 39.5 | 8 | 48.9 | 0.2143 |
| 1 | 7 | 3.0 | 73 | 49.1 | 37 | 23.1 | 31 | 24.8 | 53 | 28.7 | 55 | 41.0 | 40 | 30.4 | ||
| 2 | 3 | 4.3 | 35 | 56.1 | 25 | 15.7 | 21 | 23.9 | 33 | 49.1 | 26 | 24.1 | 25 | 26.8 | ||
| ≥3 | 0 | . | 26 | 61.5 | 15 | 29.2 | 8 | 9.3 | 16 | 43.0 | 14 | 22.3 | 19 | 34.7 | ||
| DII (n = 631 1; 561 2) | CRP 3 (n = 551 1; 528 2) | |
|---|---|---|
| Beta (95% CIs) | Beta (95% CIs) | |
| Pre-pregnancy BMI 4 | ||
| Unadjusted | 0.03 (−0.35–0.90) | 0.06 (0.05–0.07) |
| Multivariable 5 | 0.02 (−0.03–4.05) | 0.07 (0.05–0.08) |
| CRP (n = 551 1; 528 2) | ||
|---|---|---|
| OR (95% CIs) 3 | Beta (95% CIs) 4 | |
| DII continuous | ||
| Unadjusted | 0.97 (0.77–1.22) | 0.01 (−0.04–0.06) |
| Multivariable 5 | 0.94 (0.75–1.19) | 0.01 (−0.03–0.06) |
| Unadjusted (n = 631) | 1 Adjusted (n = 561) | ||||||
|---|---|---|---|---|---|---|---|
| Tertile 3 vs. Tertile 1 (Reference) | Tertile 3 vs. Tertile 1 (Reference) | ||||||
| ORs | 95% CIs | AORs | 95% CIs | ||||
| Pre-pregnancy BMI | Pre-pregnancy BMI | ||||||
| Underweight | 2.26 | 0.58 | 8.85 | Underweight | 3.11 | 0.85 | 11.45 |
| Normal | 1.00 | Normal | 1.00 | ||||
| Overweight | 1.31 | 0.56 | 3.11 | Overweight | 1.44 | 0.56 | 3.73 |
| Obese | 2.15 | 0.96 | 4.83 | Obese | 2.40 | 1.01 | 5.71 |
| p trend 2 | 0.4112 | p trend 2 | 0.009 | ||||
| p trend 3 | 0.116 | p trend 3 | 0.037 | ||||
| Age (continuous) | 0.89 | 0.83 | 0.96 | ||||
| Family Poverty Income Ratio (continuous) (n = 601) | 1.11 | 0.81 | 1.53 | ||||
| Month in Pregnancy (continuous) | 0.98 | 0.81 | 1.18 | ||||
| Race/Ethnicity | |||||||
| Hispanic | 0.45 | 0.15 | 1.32 | ||||
| Non-Hispanic white | 1.00 | ||||||
| Non-Hispanic black | 2.30 | 0.63 | 8.45 | ||||
| Other (including multi-racial groups) | 0.37 | 0.11 | 1.18 | ||||
| Education | |||||||
| ≤High school graduate | 1.68 | 0.60 | 4.71 | ||||
| ≥College | 1.00 | ||||||
| Smoking Status during Pregnancy 4 (n = 585) | |||||||
| Yes | 4.25 | 1.25 | 14.51 | ||||
| No | 1.00 | ||||||
| Unadjusted (n = 551) | Adjusted 1 (n = 528) | ||||||
|---|---|---|---|---|---|---|---|
| Tertile 3 vs. Tertile 1 (Reference) | Tertile 3 vs. Tertile 1 (Reference) | ||||||
| ORs | 95% CIs | AORs | 95% CIs | ||||
| Pre-pregnancy BMI | Pre-pregnancy BMI | ||||||
| Underweight | 0.25 | 0.06 | 1.08 | Underweight | 0.36 | 0.08 | 1.56 |
| Normal | 1.00 | Normal | 1.00 | ||||
| Overweight | 3.69 | 1.21 | 11.24 | Overweight | 3.95 | 1.49 | 10.45 |
| Obese | 14.67 | 4.80 | 44.83 | Obese | 24.84 | 6.19 | 99.67 |
| p-trend 2 | <0.0001 | p-trend 2 | <0.0001 | ||||
| p-trend 3 | <0.0001 | p-trend 3 | <0.0001 | ||||
| Age (continuous) | 1.02 | 0.95 | 1.10 | ||||
| Family Poverty Income Ratio (continuous) (n = 528) | 1.41 | 1.07 | 1.85 | ||||
| Month in Pregnancy (continuous) | 1.13 | 0.98 | 1.30 | ||||
| Race/Ethnicity | |||||||
| Hispanic | 2.62 | 1.14 | 6.03 | ||||
| Non-Hispanic white | 1.00 | ||||||
| Non-Hispanic black | 2.04 | 0.76 | 5.47 | ||||
| Other (including multi-racial groups) | 1.88 | 0.22 | 16.12 | ||||
| Education | |||||||
| ≤High school graduate | 3.45 | 1.17 | 10.20 | ||||
| ≥College | 1.00 | ||||||
| Smoking Status during Pregnancy 4 | |||||||
| Yes | 1.91 | 0.61 | 6.00 | ||||
| No | 1.00 | ||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.; Hur, J.; Cho, E.-H.; Chung, H.-K.; Shivappa, N.; Wirth, M.D.; Hébert, J.R.; Lee, K.W. Pre-Pregnancy Body Mass Index Is Associated with Dietary Inflammatory Index and C-Reactive Protein Concentrations during Pregnancy. Nutrients 2017, 9, 351. https://doi.org/10.3390/nu9040351
Shin D, Hur J, Cho E-H, Chung H-K, Shivappa N, Wirth MD, Hébert JR, Lee KW. Pre-Pregnancy Body Mass Index Is Associated with Dietary Inflammatory Index and C-Reactive Protein Concentrations during Pregnancy. Nutrients. 2017; 9(4):351. https://doi.org/10.3390/nu9040351
Chicago/Turabian StyleShin, Dayeon, Junguk Hur, Eun-Hee Cho, Hae-Kyung Chung, Nitin Shivappa, Michael D. Wirth, James R. Hébert, and Kyung Won Lee. 2017. "Pre-Pregnancy Body Mass Index Is Associated with Dietary Inflammatory Index and C-Reactive Protein Concentrations during Pregnancy" Nutrients 9, no. 4: 351. https://doi.org/10.3390/nu9040351