Eating at Food Outlets and “On the Go” Is Associated with Less Healthy Food Choices in Adults: Cross-Sectional Data from the UK National Diet and Nutrition Survey Rolling Programme (2008–2014)

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Dietary Data
2.3. Other Variables
2.4. Defining Eating Occasions
- Home: bedroom, dining room, garden, kitchen, living room, home/other, home/unspecified
- Work: all work canteen categories, desk, work/other. Eating occasions at university (all university canteen categories, university/other) were combined with work due to the small number of eating occasions in this location (0.2% of all occasions) which did not allow for meaningful interpretation
- Leisure places: sports clubs, sports leisure venue, leisure activity place /cinema/shopping centre/place of interest, attractions, community/day centre, public hall, function room
- Food outlets: restaurant/pub/night club, fast food outlet, coffee shop/cafe/deli/sandwich bar
- “On the go”: bus, car or train outside/other, street
2.5. Dietary Variables and Classification of Foods as Core or Non-Core
2.6. Data Analysis
3. Results
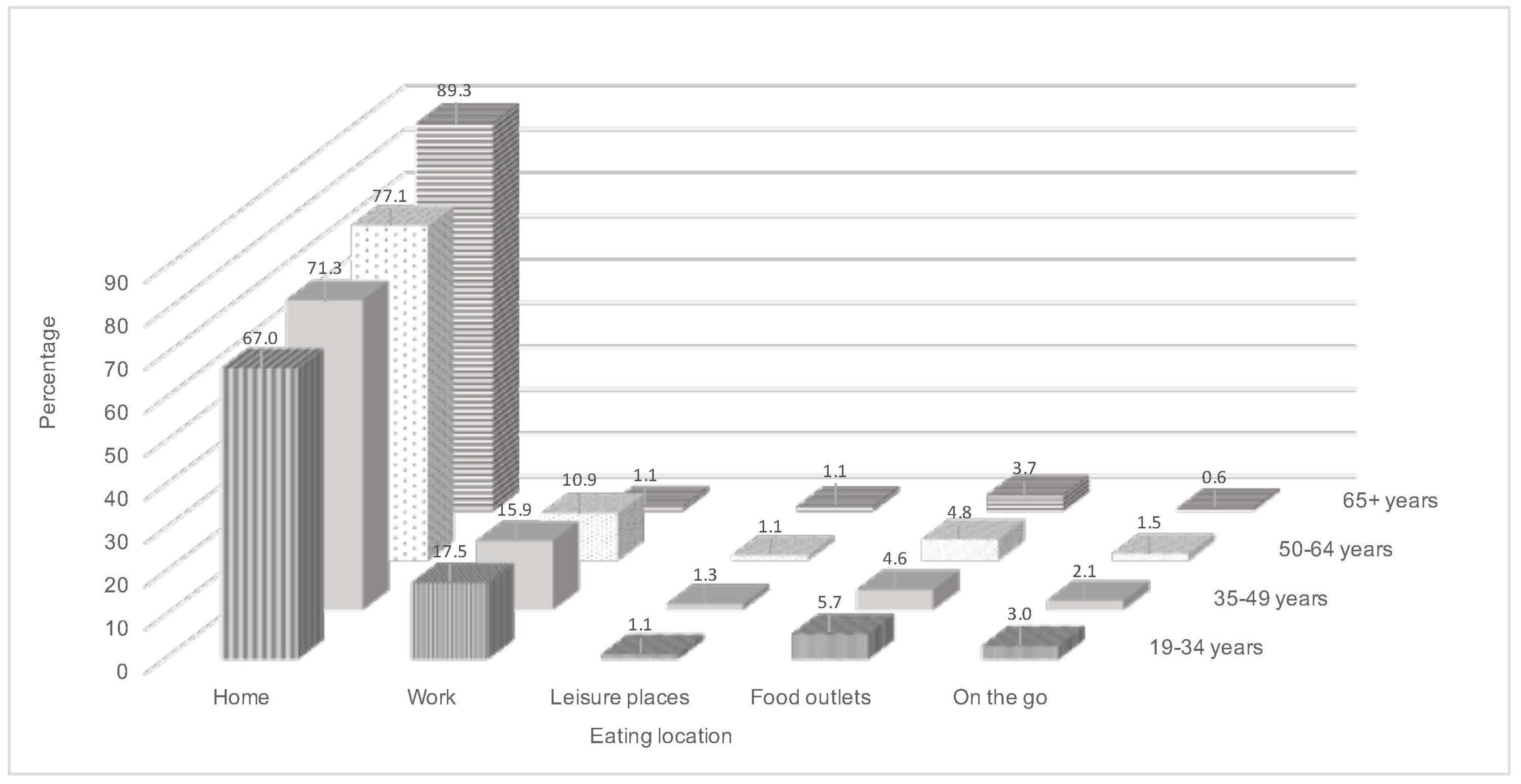
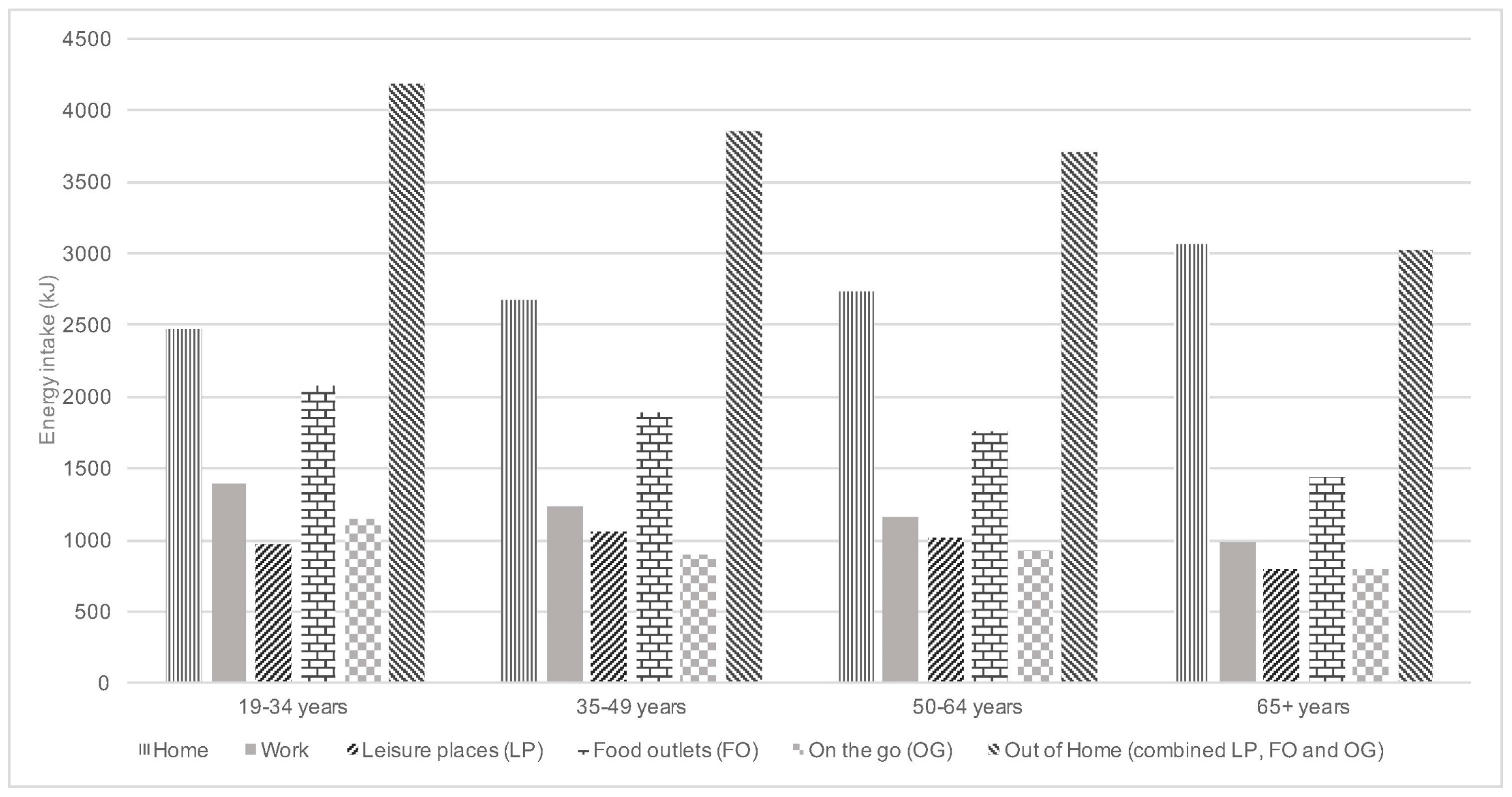
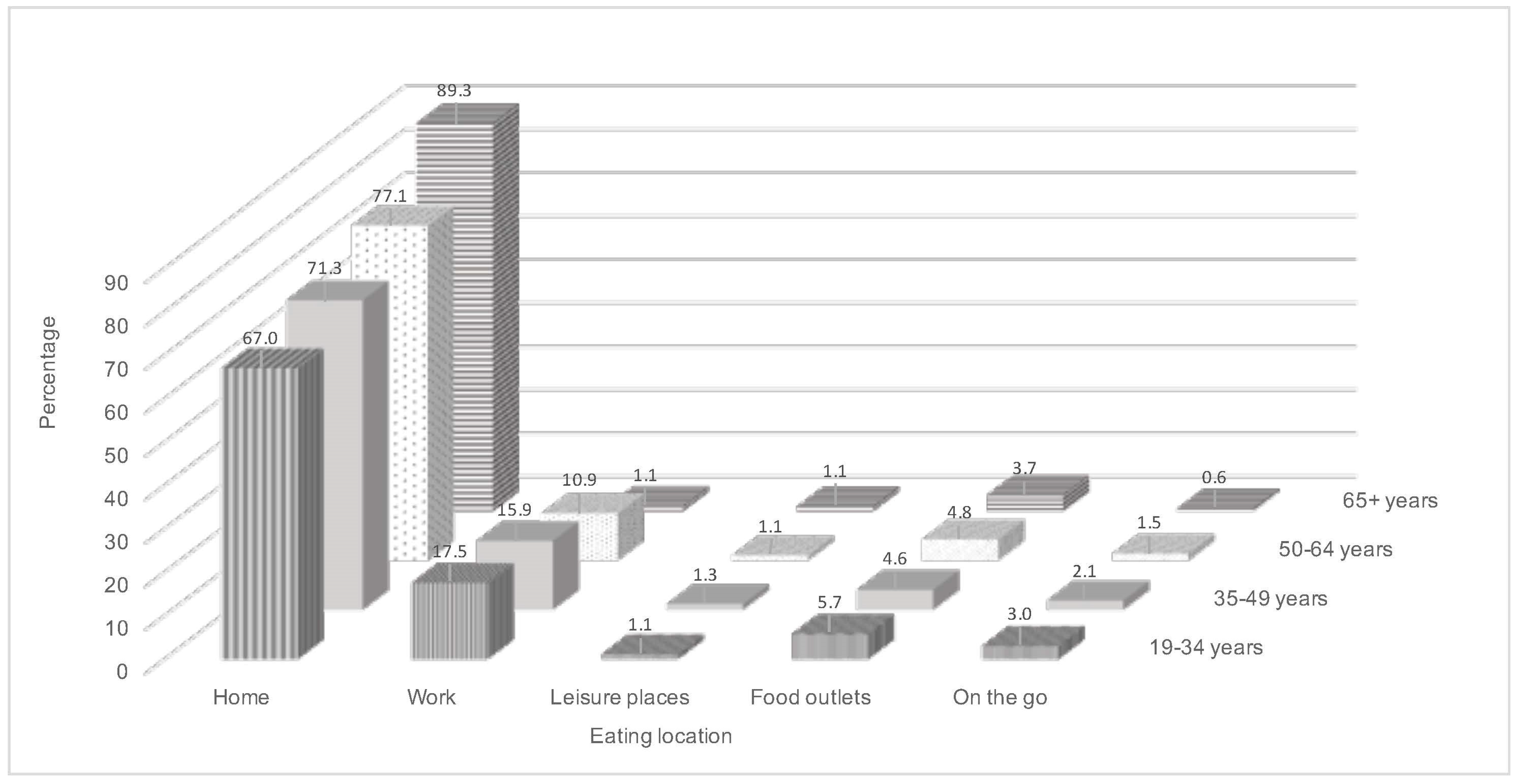
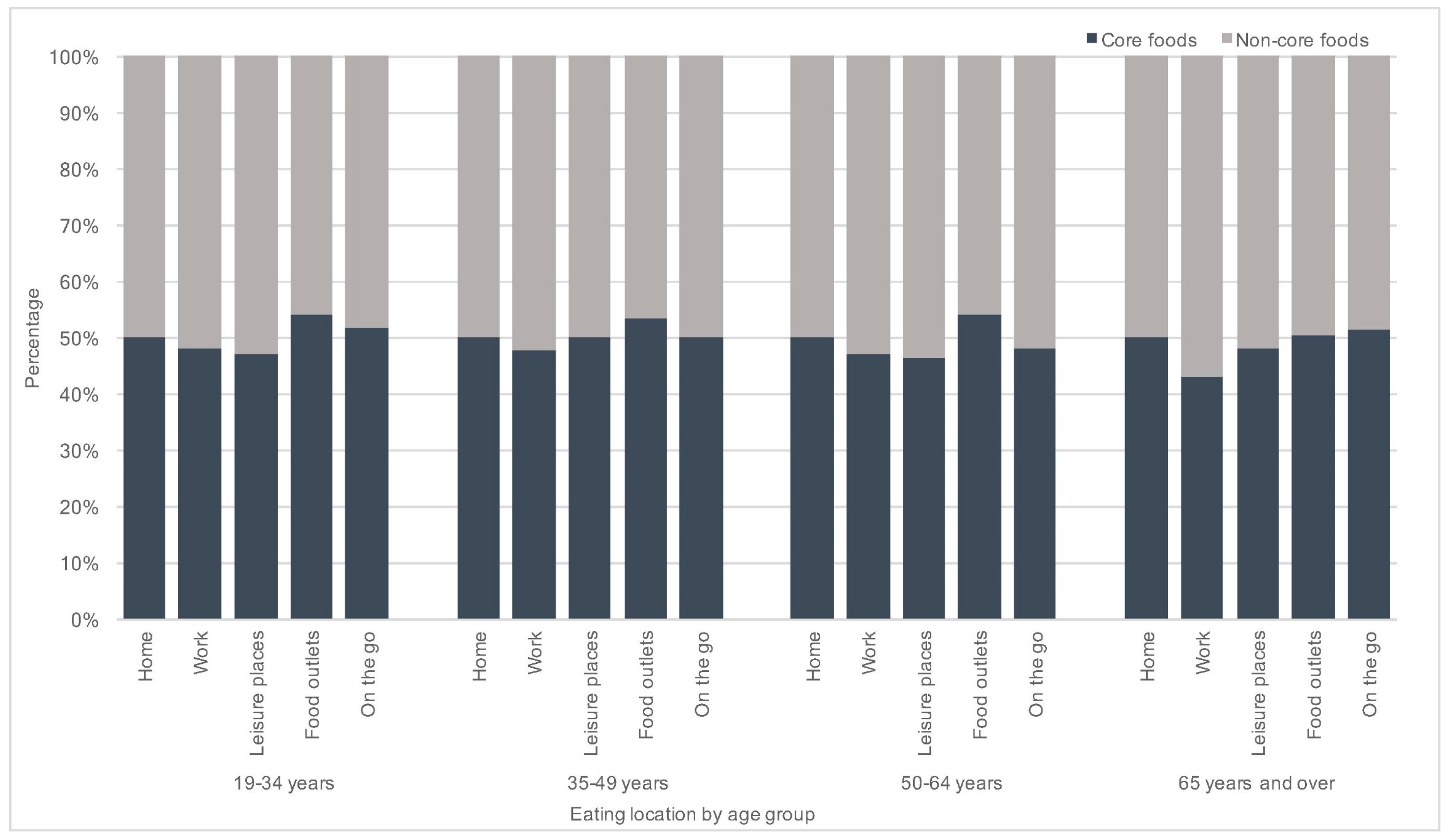
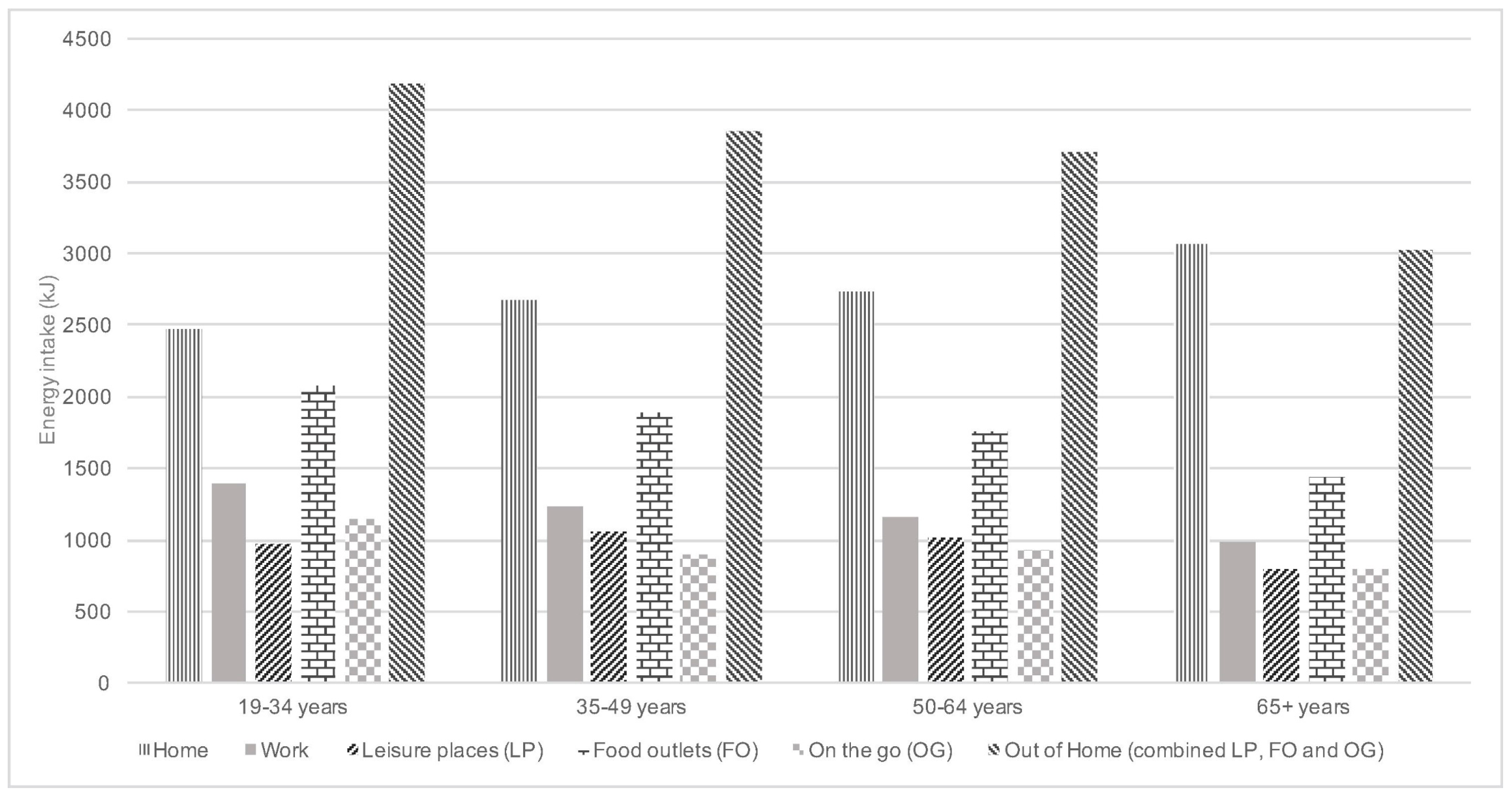
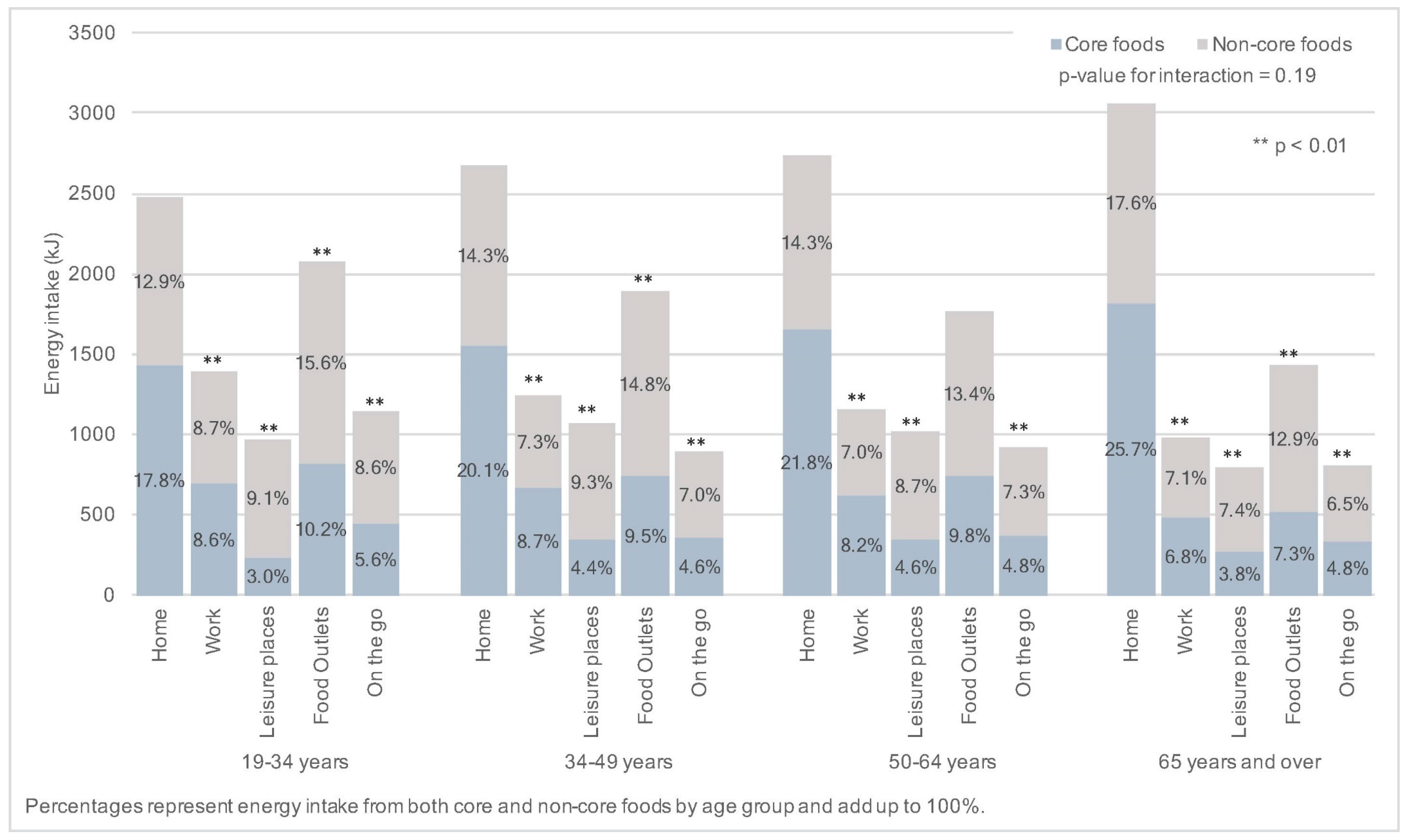
3.1. Intakes of Selected Foods and Nutrients by Eating Location
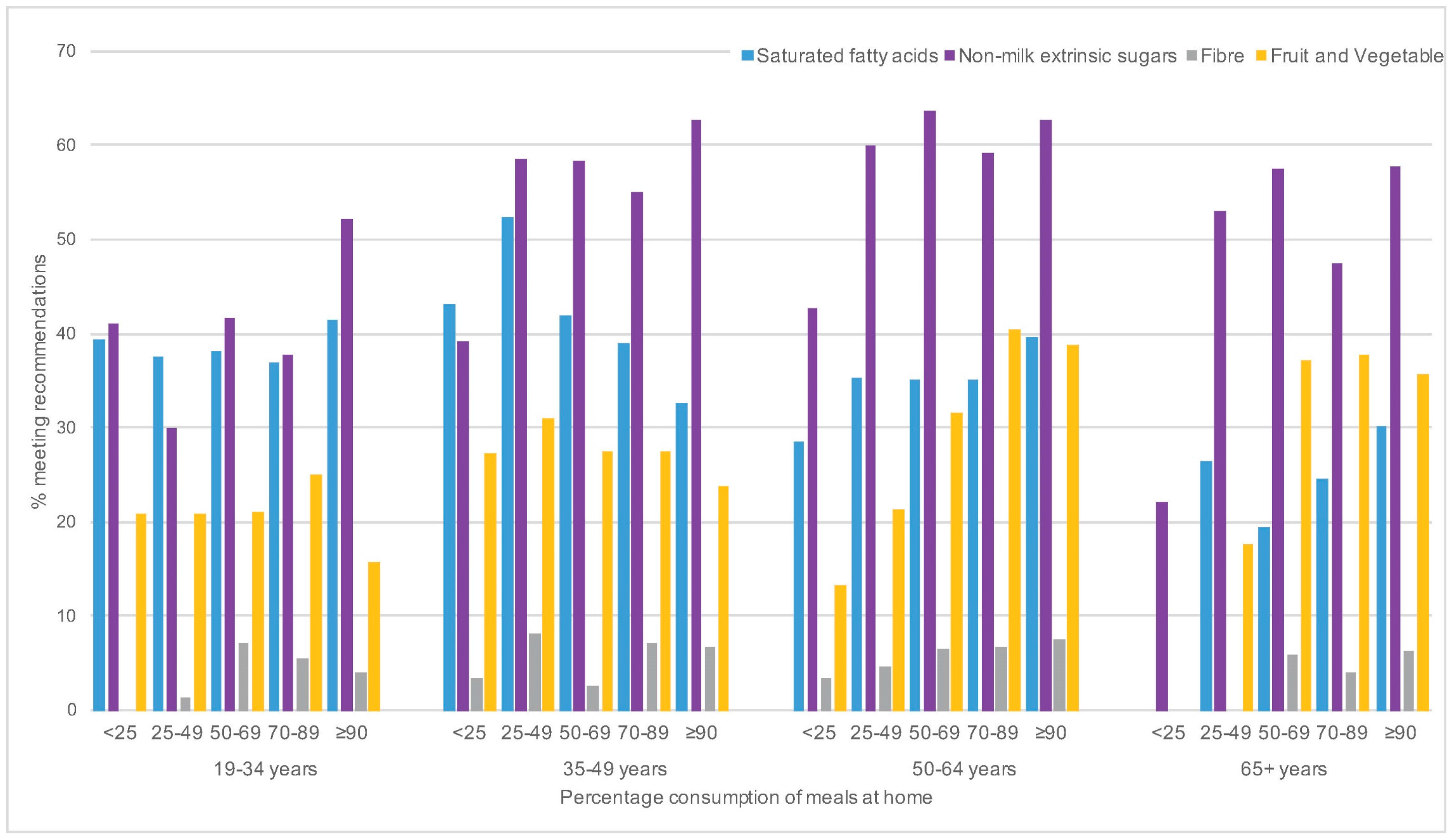
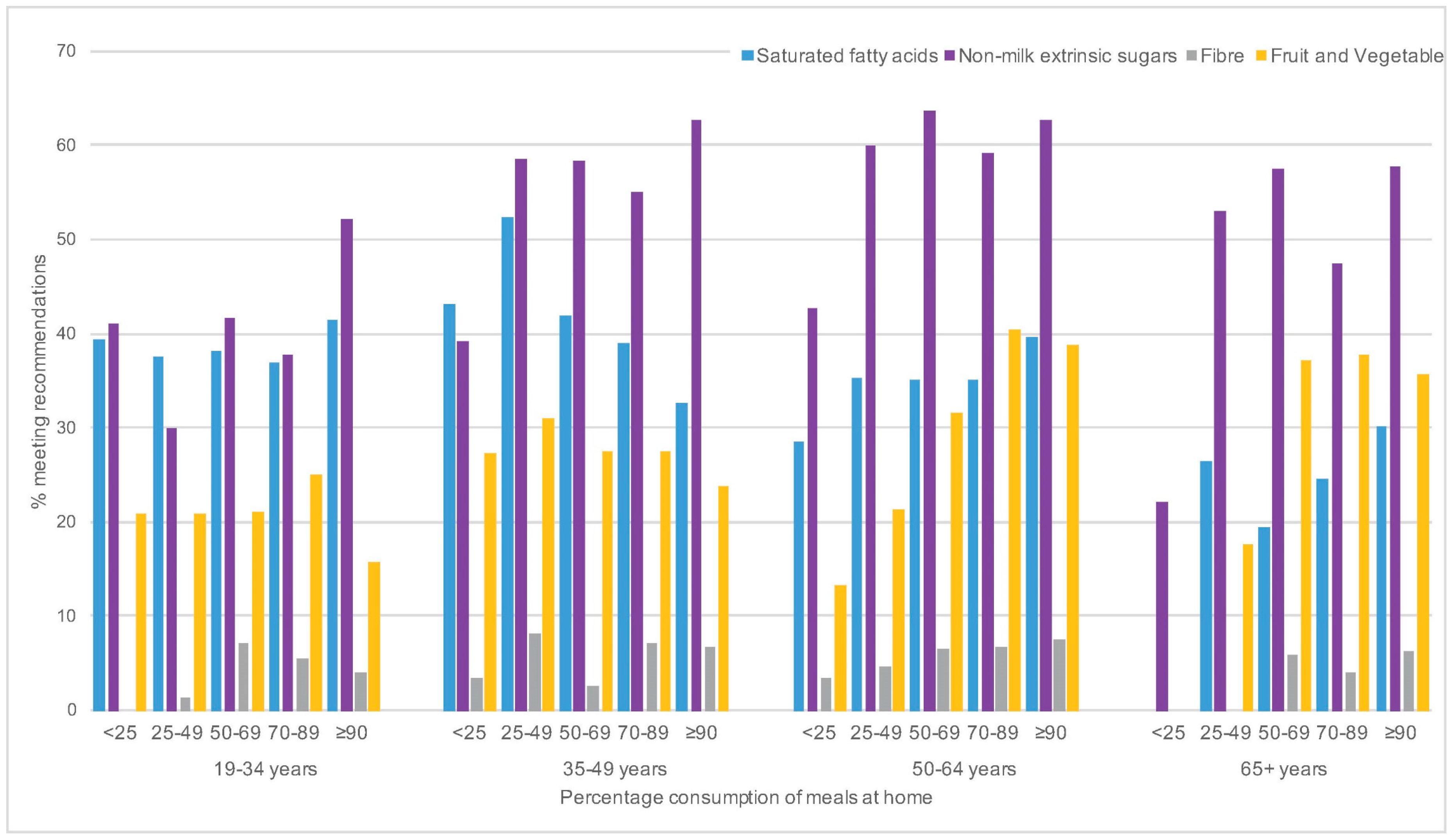
3.2. Home Eating Consumption Patterns and Impact of Modulatory Factors
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Disease; Joint WHO/FAO Expert Consultation: Geneva, Switzerland, 2003. [Google Scholar]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Manson, J.E.; Lee, I.M.; Cole, S.R.; Hennekens, C.H.; Willett, W.C.; Buring, J.E. Fruit and vegetable intake and risk of cardiovascular disease: The Women’s Health Study. Am. J. Clin. Nutr. 2000, 72, 922–928. [Google Scholar] [PubMed]
- Harding, A.H.; Wareham, N.J.; Bingham, S.A.; Khaw, K.; Luben, R.; Welch, A.; Forouhi, N.G. Plasma Vitamin C Level, Fruit and Vegetable Consumption, and the Risk of New-Onset Type 2 Diabetes Mellitus. Arch. Intern. Med. 2008, 168, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fruit, Vegetables and NCD Prevention; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Vergnaud, A.C.; Norat, T.; Romaguera, D.; Mouw, T.; May, A.M.; Romieu, I.; Freisling, H.; Slimani, N.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; et al. Fruit and vegetable consumption and prospective weight change in participants of the European Prospective Investigation into Cancer and Nutrition-Physical Activity, Nutrition, Alcohol, Cessation of Smoking, Eating Out of Home, and Obesity study. Am. J. Clin. Nutr. 2012, 95, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Caterson, I.; Seidell, J.C.; James, W.P. Diet, nutrition and the prevention of excess weight gain and obesity. Public Health Nutr. 2004, 7, 123–146. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, 132–142. [Google Scholar] [CrossRef]
- Allender, S.; Gleeson, E.; Crammond, B.; Sacks, G.; Lawrence, M.; Peeters, A.; Loff, B.; Swinburn, B. Policy change to create supportive environments for physical activity and healthy eating: Which options are the most realistic for local government? Health Promot. Int. 2012, 27, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Brownson, R.C.; Haire-Joshu, D.; Luke, D.A. Shaping the context of health: A review of environmental and policy approaches in the prevention of chronic diseases. Annu. Rev. Public Health 2006, 27, 341–370. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; Tseng, M. Towards comprehensive global monitoring of food environments and policies to reduce diet-related non-communicable diseases. Public Health Nutr. 2013, 16, 2101–2104. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.E.; Sorensen, G.; Subramanian, S.V.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.B.; Evenson, K.R. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef] [PubMed]
- Lachat, C.; Nago, E.; Verstraeten, R.; Roberfroid, D.; Van Camp, J.; Kolsteren, P. Eating out of home and its association with dietary intake: A systematic review of the evidence. Obes. Rev. 2012, 13, 329–346. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, I.N.; Curioni, C.; Sichieri, R. Association between eating out of home and body weight. Nutr. Rev. 2012, 70, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.A.; Burgoine, T.; Stamp, E.; Grieve, R. The foodscape: Classification and field validation of secondary data sources across urban/rural and socio-economic classifications in England. Int. J. Behav. Nutr. Phys. Act. 2012, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabs, J.; Devine, C.M. Time scarcity and food choices: An overview. Appetite 2006, 47, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Department for Environment Food and Rural Affairs. Family Food 2012; Department for Environment Food and Rural Affairs: London, UK, 2013.
- Adams, J.; Goffe, L.; Brown, T.; Lake, A.A.; Summerbell, C.; White, M.; Wrieden, W.; Adamson, A.J. Frequency and socio-demographic correlates of eating meals out and take-away meals at home: Cross-sectional analysis of the UK national diet and nutrition survey, waves 1–4 (2008–12). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bezerra, I.N.; Junior, E.V.; Pereira, R.A.; Sichieri, R. Away-from-home eating: Nutritional status and dietary intake among Brazilian adults. Public Health Nutr. 2015, 18, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, N.A.; Gibney, M.J.; Burke, S.J.; McCarthy, S.N. The influence of eating location on nutrient intakes in Irish adults: Implications for developing food-based dietary guidelines. Public Health Nutr. 2005, 8, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Katsoulis, M.; Orfanos, P.; Lachat, C.; Gedrich, K.; Rodrigues, S.S.; Freisling, H.; Kolsteren, P.; Engeset, D.; Lopes, C.; et al. HECTOR Consortium. Eating out is different from eating at home among individuals who occasionally eat out. A cross-sectional study among middle-aged adults from eleven European countries. Br. J. Nutr. 2015, 113, 1951–1964. [Google Scholar] [CrossRef] [PubMed]
- Nicklas, T.; O’Neil, C. Development of the SoFAS (solid fats and added sugars) concept: The 2010 Dietary Guidelines for Americans. Adv. Nutr. 2015, 6, 368S–375S. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.A. Do diets high in sugars compromise micronutrient intakes? Micronutrient intakes in the Dietary and Nutritional Survey of British Adults according to dietary concentration of ‘added’, ‘non-milk extrinsic’ or ‘total’ sugars. J. Hum. Nutr. Diet. 1997, 10, 125–133. [Google Scholar] [CrossRef]
- Myhre, J.B.; Løken, E.B.; Wandel, M.; Andersen, L.F. Eating location is associated with the nutritional quality of the diet in Norwegian adults. Public Health Nutr. 2013, 17, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; McNaughton, S.A.; Gall, S.A.; Blizzard, L.; Dwyer, T.; Venn, A.J. Takeaway food consumption and its associations with diet quality and abdominal obesity: A cross-sectional study of young adults. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Neckerman, K.M. Takeaway food and health. BMJ 2014, 348, g1817. [Google Scholar] [CrossRef] [PubMed]
- Burgoine, T.; Forouhi, N.G.; Griffin, S.J.; Wareham, N.J.; Monsivais, P. Associations between exposure to takeaway food outlets, takeaway food consumption, and body weight in Cambridgeshire, UK: Population based, cross sectional study. BMJ 2014, 348, g1464. [Google Scholar] [CrossRef] [PubMed]
- Seguin, R.A.; Aggarwal, A.; Vermeylen, F.; Drewnowski, A. Consumption Frequency of Foods Away from Home Linked with Higher Body Mass Index and Lower Fruit and Vegetable Intake among Adults: A Cross-Sectional Study. J. Environ. Public Health 2016, 2016, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Whitley, M.I.; Graubard, B.I. Away from home meals: Associations with biomarkers of chronic disease and dietary intake in American adults, NHANES 2005–2010. Int. J. Obes. 2015, 39, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Nago, E.S.; Lachat, C.K.; Dossa, R.A.; Kolsteren, P.W. Association of out-of-home eating with anthropometric change: A systematic review of prospective studies. Crit. Rev. Food Sci. Nutr. 2014, 54, 1103–1116. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.S.; Ju, S.Y. Trends in nutrient intakes and consumption while eating-out among Korean adults based on Korea National Health and Nutrition Examination Survey (1998–2012) data. Nutr. Res. Pract. 2014, 8, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Nguyen, B.T.; Han, E. Energy intake from restaurants: Demographics and socioeconomics, 2003–2008. Am. J. Prev. Med. 2012, 43, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D. Energy intakes of US children and adults by food purchase location and by specific food source. Nutr. J. 2013, 12, 59. [Google Scholar] [CrossRef] [PubMed]
- NatCen Social Research, MRC Elsie Widdowson Laboratory, University College London Medical School. National Diet and Nutrition Survey Years 1–6, 2008/09–2013/14. [Data Collection], 8th ed.; UK Data Service: Colchester, UK, 2017; SN: 6533. [Google Scholar]
- Bates, B.; Lennox, A.; Prentice, A.; Bates, C.; Page, P.; Nicholson, S.; Swan, G. National Diet and Nutrition Survey Results from Years 1, 2, 3 and 4 (Combined) of the Rolling Programme (2008/2009–2011/2012); Public Health England: London, UK, 2014.
- Fitt, E.; Cole, D.; Ziauddeen, N.; Pell, D.; Stickley, E.; Harvey, A.; Stephen, A.M. DINO (Diet In Nutrients Out)—An integrated dietary assessment system. Public Health Nutr. 2015, 18, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Agency. Food Portion Sizes, 3rd ed.; Food Standards Agency, Ed.; The Stationary Office: London, UK, 2002.
- Duffey, K.J.; Popkin, B.M. Energy density, portion size, and eating occasions: Contributions to increased energy intake in the United States, 1977–2006. PLoS Med. 2011, 8, e1001050. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; van Jaarsveld, C.H.; Wardle, J. Individual and family environment correlates differ for consumption of core and non-core foods in children. Br. J. Nutr. 2011, 105, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Scientific Advisory Committee on Nutrition. The Nutritional Wellbeing of the British Population; TSO: London, UK, 2008.
- Scientific Advisory Committee on Nutrition. Carbohydrates and Health; TSO: London, UK, 2015.
- Fitt, E.; Mak, T.N.; Stephen, A.M.; Prynne, C.; Roberts, C.; Swan, G.; Farron-Wilson, M. Disaggregating composite food codes in the UK National Diet and Nutrition Survey food composition databank. Eur. J. Clin. Nutr. 2010, 64, S32–S36. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. 5 A Day 2015. Available online: http://www.nhs.uk/livewell/5aday/Pages/5ADAYhome.aspx (accessed on 4 November 2015).
- R Development Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008. [Google Scholar]
- Department of Health. Dietary reference values for food energy and nutrients for the United Kingdom. Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy. Rep. Health Soc. Subj. Lond. 1991, 41, 1–210. [Google Scholar]
- Cohen, D.A.; Babey, S.H. Contextual influences on eating behaviours: Heuristic processing and dietary choices. Obes. Rev. 2012, 13, 766–779. [Google Scholar] [CrossRef] [PubMed]
- Albertson, A.M.; Reicks, M.; Joshi, N.; Gugger, C.K. Whole grain consumption trends and associations with body weight measures in the United States: Results from the cross sectional National Health and Nutrition Examination Survey 2001–2012. Nutr. J. 2016, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Ziauddeen, N.; University of Southampton, Southampton, UK. Unpublished work. 2017.
- Mikkila, V.; Rasanen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- NHS Digital. National Child Measurement Programme England, 2015/16 School Year; NHS Digital: Leeds, UK, 2017. [Google Scholar]
- Patterson, R.; Risby, A.; Chan, M.Y. Consumption of takeaway and fast food in a deprived inner London Borough: Are they associated with childhood obesity? BMJ Open 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. Taste preferences and food intake. Annu. Rev. Nutr. 1997, 17, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Aggarwal, A.; Hurvitz, P.M.; Monsivais, P.; Moudon, A.V. Obesity and supermarket access: Proximity or price? Am. J. Public Health 2012, 102, e74–e80. [Google Scholar] [CrossRef] [PubMed]
- Monsivais, P.; Aggarwal, A.; Drewnowski, A. Are socio-economic disparities in diet quality explained by diet cost? J. Epidemiol. Community Health 2012, 66, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Pechey, R.; Jebb, S.A.; Kelly, M.P.; Almiron-Roig, E.; Conde, S.; Nakamura, R.; Shemilt, I.; Suhrcke, M.; Marteau, T.M. Socioeconomic differences in purchases of more vs. less healthy foods and beverages: Analysis of over 25,000 British households in 2010. Soc. Sci. Med. 2013, 92, 22–26. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Core foods | Non-core foods |
|---|---|
| Pasta, rice and other miscellaneous cereals | Biscuits |
| Bread (all types) | Buns, cakes, pastries and fruit pies |
| Breakfast cereals (all types) | Puddings |
| Milk (all types) | Ice cream |
| Cheese | Butter, spreads and oil |
| Yogurt and fromage frais | Dairy desserts |
| Eggs and egg dishes | |
| Beef, veal and dishes | Meat pies and pastries |
| Lamb and dishes | |
| Pork and dishes | Bacon and ham |
| Chicken and turkey dishes | Coated chicken and turkey |
| Liver products and dishes | |
| Burgers and kebabs | |
| Sausages | |
| Other meat and meat products | |
| White fish, shellfish and fish dishes | Coated or fried white fish |
| Oily fish | |
| Salad and other raw vegetables | |
| Vegetables (not raw) including beans and meat alternatives | |
| Other potatoes and potato salads | Chips, fried and roast potatoes and potato products |
| Nuts and seeds | |
| Fruit | |
| Smoothies | |
| Fruit juice (capped at maximum intake contribution to 5-a-day) | Soft drinks not diet |
| Tea, coffee and water | Soft drinks diet |
| Alcoholic beverages | |
| Sugar, preserves and sweet spreads | |
| Sugar confectionery | |
| Chocolate confectionery |
| Fruit and Vegetables | Red and Processed Meat | Sugar Sweetened Beverages | Fibre | Non-Milk Extrinsic Sugars (NMES) | Saturated Fatty Acids | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean % (Food Intake) | p | Mean % (Food Intake) | p | Mean % (Food Intake) | p | Mean % (Food Intake) | p | Mean % (Energy Intake) | p | Mean % (Energy Intake) | p | ||
| 19–34 years | Home | 10.4 | (ref) | 3.1 | (ref) | 12.6 | (ref) | 0.6 | (ref) | 12.0 | (ref) | 12.3 | (ref) |
| Work | 9.5 | 0.16 | 1.7 | 0.00 | 14.3 | 0.00 | 0.5 | 0.00 | 16.4 | 0.00 | 11.7 | 0.18 | |
| Leisure places | 4.2 | 0.00 | 2.1 | 0.12 | 13.9 | 0.00 | 0.5 | 0.27 | 23.8 | 0.00 | 8.4 | 0.00 | |
| Food outlets | 6.8 | 0.00 | 3.7 | 0.18 | 17.4 | 0.00 | 0.5 | 0.00 | 16.4 | 0.00 | 9.3 | 0.00 | |
| On the go | 12.3 | 0.16 | 2.7 | 0.38 | 21.2 | 0.00 | 0.7 | 0.00 | 23.3 | 0.00 | 11.1 | 0.04 | |
| 35–49 years | Home | 11.0 | (ref) | 2.9 | (ref) | 6.5 | (ref) | 0.6 | (ref) | 10.4 | (ref) | 12.1 | (ref) |
| Work | 10.6 | 0.40 | 1.7 | 0.00 | 5.8 | 0.00 | 0.5 | 0.00 | 13.8 | 0.00 | 12.0 | 0.71 | |
| Leisure places | 4.1 | 0.00 | 2.2 | 0.11 | 7.4 | 0.00 | 0.5 | 0.36 | 19.4 | 0.00 | 9.7 | 0.00 | |
| Food outlets | 6.9 | 0.00 | 4.0 | 0.00 | 8.6 | 0.00 | 0.4 | 0.00 | 14.8 | 0.00 | 10.0 | 0.00 | |
| On the go | 15.3 | 0.00 | 2.3 | 0.13 | 11.0 | 0.00 | 0.8 | 0.00 | 20.2 | 0.00 | 9.7 | 0.00 | |
| 50–64 years | Home | 12.2 | (ref) | 2.7 | (ref) | 3.6 | (ref) | 0.6 | (ref) | 9.9 | (ref) | 12.4 | (ref) |
| Work | 11.1 | 0.10 | 2.0 | 0.00 | 2.8 | 0.00 | 0.5 | 0.00 | 13.0 | 0.00 | 12.6 | 0.59 | |
| Leisure places | 6.6 | 0.00 | 2.2 | 0.44 | 6.4 | 0.00 | 0.4 | 0.05 | 19.1 | 0.00 | 11.5 | 0.28 | |
| Food outlets | 7.7 | 0.00 | 3.4 | 0.06 | 5.8 | 0.00 | 0.5 | 0.00 | 14.0 | 0.00 | 10.4 | 0.00 | |
| On the go | 18.6 | 0.00 | 1.7 | 0.00 | 7.7 | 0.00 | 0.9 | 0.00 | 19.7 | 0.00 | 10.4 | 0.01 | |
| ≥65 years | Home | 12.7 | (ref) | 2.6 | (ref) | 3.1 | (ref) | 0.6 | (ref) | 10.8 | (ref) | 13.2 | (ref) |
| Work | 7.3 | 0.00 | 1.3 | 0.00 | 0.2 | 0.06 | 0.4 | 0.00 | 11.7 | 0.61 | 13.6 | 0.71 | |
| Leisure places | 6.9 | 0.00 | 2.6 | 0.99 | 6.7 | 0.00 | 0.3 | 0.00 | 20.4 | 0.00 | 13.8 | 0.57 | |
| Food outlets | 7.5 | 0.00 | 3.4 | 0.04 | 4.9 | 0.00 | 0.4 | 0.00 | 13.6 | 0.00 | 12.3 | 0.08 | |
| On the go | 13.3 | 0.83 | 2.6 | 0.95 | 3.7 | 0.01 | 0.9 | 0.00 | 23.4 | 0.00 | 10.3 | 0.00 | |
| p for trend | 0.22 | 0.29 | 0.00 | 0.25 | 0.97 | 0.00 | |||||||
| Percentage Consumption of Meals at Home | p Value | ||||||
|---|---|---|---|---|---|---|---|
| <25 | 25–49 | 50–69 | 70–89 | >90 | |||
| n | 88 | 477 | 1047 | 1587 | 1537 | ||
| Age (years) (mean) | 37.9 | 37.2 | 41.0 | 49.4 | 56.5 | ||
| Sex (%) | Male | 65.3 | 55.0 | 56.2 | 43.6 | 44.8 | (ref) |
| Female | 34.7 | 45.0 | 43.8 | 56.4 | 55.2 | 0.01 | |
| Ethnicity (%) | White | 94.8 | 91.7 | 90.1 | 89.4 | 87.8 | (ref) |
| Non-white | 5.2 | 8.3 | 9.9 | 10.6 | 12.2 | 0.57 | |
| Income (quintile) (%) | ≤£12,300 | 6.6 | 6.2 | 9.3 | 16.8 | 23.6 | (ref) |
| >£12,300 ≤ £19,890 | 6.3 | 13.0 | 16.4 | 19.9 | 28.8 | 0.04 | |
| >£19,890 ≤ £28,615 | 22.0 | 17.6 | 19.3 | 18.7 | 16.3 | 0.00 | |
| >£28,615 ≤ £42,500 | 18.6 | 30.2 | 23.3 | 22.0 | 17.5 | 0.00 | |
| >£42,500 | 46.5 | 33.0 | 31.6 | 22.6 | 13.8 | 0.00 | |
| BMI (%) | Underweight | 0.6 | 2.2 | 1.3 | 0.6 | 2.3 | 0.85 |
| Normal weight | 39.7 | 38.8 | 34.2 | 35.4 | 33.8 | (ref) | |
| Overweight | 25.4 | 35.8 | 39.3 | 35.3 | 36.7 | 0.44 | |
| Obese | 30.5 | 19.5 | 22.9 | 26.0 | 25.0 | 0.66 | |
| Morbidly obese | 3.8 | 3.7 | 2.3 | 2.7 | 2.2 | 0.04 | |
| Frequency of eating out (%) | 5 or more times per week | 4.7 | 3.7 | 2.1 | 1.1 | 0.5 | 0.00 |
| 3–4 times per week | 8.2 | 5.3 | 5.3 | 2.8 | 2.4 | 0.00 | |
| 1–2 times per week | 30.1 | 27.6 | 26.1 | 24.3 | 15.3 | 0.00 | |
| 1–2 times per month | 38.3 | 47.9 | 45.6 | 44.9 | 39.2 | 0.00 | |
| Rarely or never | 18.7 | 15.5 | 21.0 | 26.9 | 42.6 | (ref) | |
| Frequency of takeaway meals (%) | 5 or more times per week | 0.8 | 0.5 | 0.1 | 0.2 | 0.6 | 0.47 |
| 3–4 times per week | 0.7 | 1.7 | 1.2 | 1.0 | 1.6 | 0.62 | |
| 1–2 times per week | 23.9 | 30.5 | 22.8 | 16.9 | 14.1 | 0.00 | |
| 1–2 times per month | 51.9 | 40.0 | 45.3 | 35.5 | 27.0 | 0.00 | |
| Rarely or never | 22.6 | 27.3 | 30.6 | 46.5 | 56.7 | (ref) | |
| Drinking (%) | Once a week or more | 75.4 | 63.2 | 57.2 | 51.1 | 38.7 | 0.00 |
| Once or twice a month | 11.0 | 16.9 | 17.3 | 17.6 | 16.0 | 0.34 | |
| Once every couple of months | 2.0 | 5.0 | 7.6 | 10.5 | 10.1 | 0.98 | |
| Few times a year | 5.2 | 5.4 | 6.9 | 8.4 | 12.7 | 0.60 | |
| Never drinks | 6.5 | 9.5 | 11.0 | 12.4 | 22.5 | (ref) | |
| Smoking (%) | No | 71.4 | 74.6 | 72.9 | 78.8 | 76.1 | (ref) |
| Yes | 28.6 | 25.4 | 27.1 | 21.2 | 23.9 | 0.06 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziauddeen, N.; Almiron-Roig, E.; Penney, T.L.; Nicholson, S.; Kirk, S.F.L.; Page, P. Eating at Food Outlets and “On the Go” Is Associated with Less Healthy Food Choices in Adults: Cross-Sectional Data from the UK National Diet and Nutrition Survey Rolling Programme (2008–2014). Nutrients 2017, 9, 1315. https://doi.org/10.3390/nu9121315
Ziauddeen N, Almiron-Roig E, Penney TL, Nicholson S, Kirk SFL, Page P. Eating at Food Outlets and “On the Go” Is Associated with Less Healthy Food Choices in Adults: Cross-Sectional Data from the UK National Diet and Nutrition Survey Rolling Programme (2008–2014). Nutrients. 2017; 9(12):1315. https://doi.org/10.3390/nu9121315
Chicago/Turabian StyleZiauddeen, Nida, Eva Almiron-Roig, Tarra L. Penney, Sonja Nicholson, Sara F. L. Kirk, and Polly Page. 2017. "Eating at Food Outlets and “On the Go” Is Associated with Less Healthy Food Choices in Adults: Cross-Sectional Data from the UK National Diet and Nutrition Survey Rolling Programme (2008–2014)" Nutrients 9, no. 12: 1315. https://doi.org/10.3390/nu9121315