Maternal Continuing Folic Acid Supplementation after the First Trimester of Pregnancy Increased the Risk of Large-for-Gestational-Age Birth: A Population-Based Birth Cohort Study

Abstract
:
1. Introduction
2. Research Design and Methods
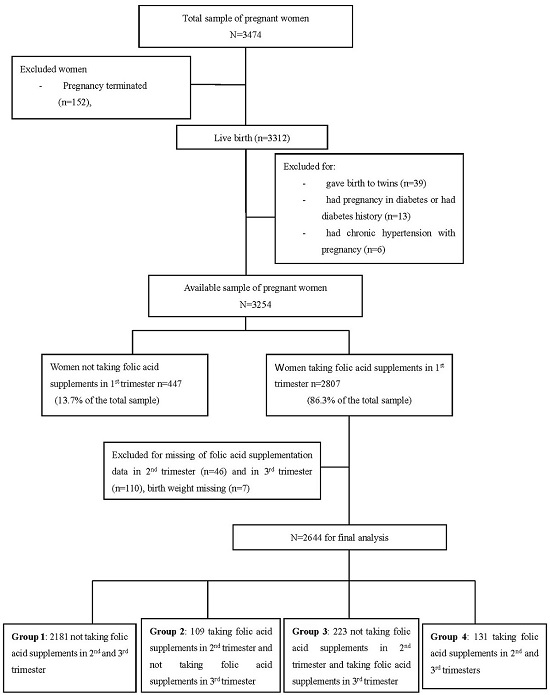
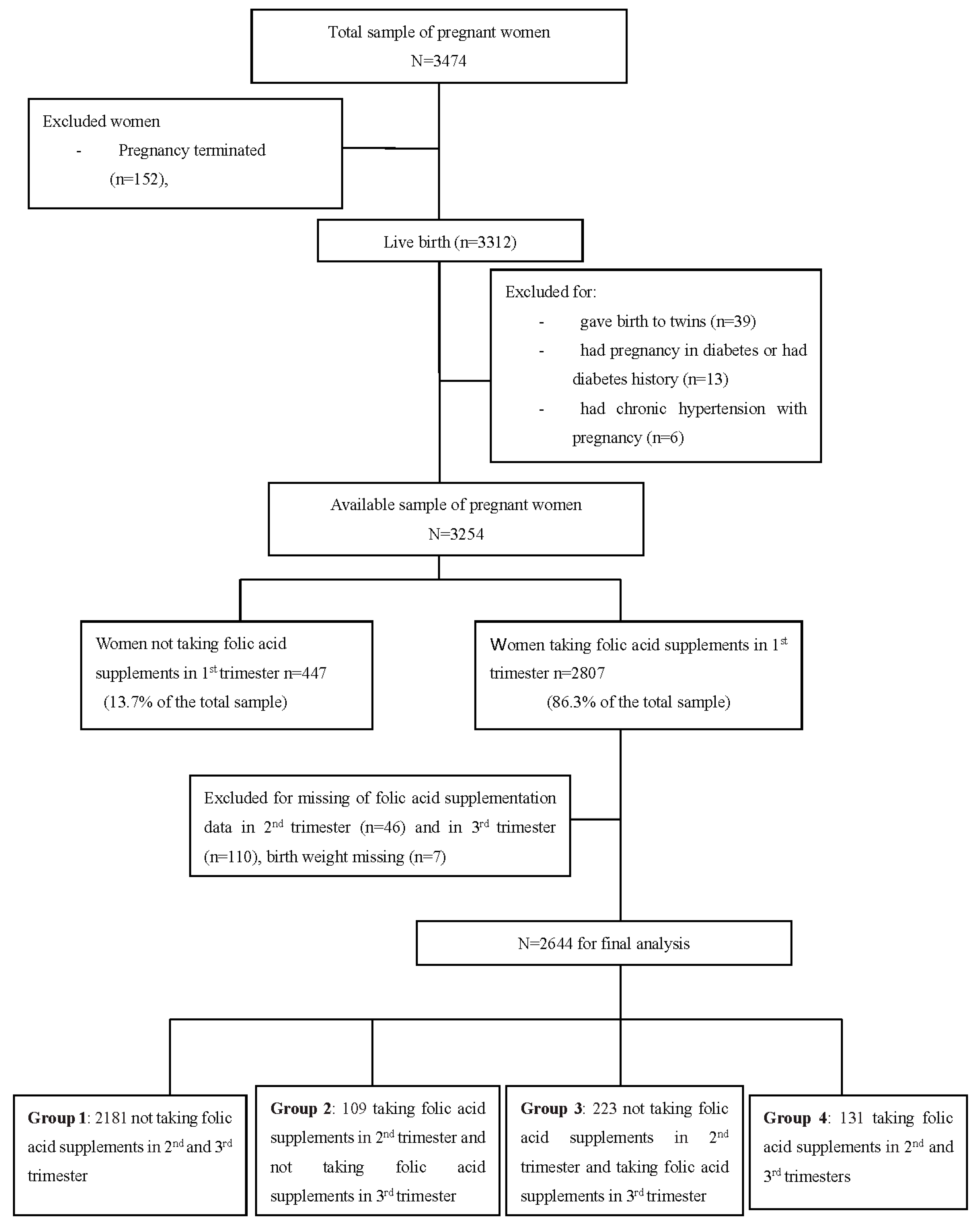
2.1. Cohort Study
2.2. Folic Acid Supplementation and Pregnancy Outcomes
2.3. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
Acknowledgment
Author Contributions
Conflicts of Interest
References
- Tamura, T.; Picciano, M.F. Folate and human reproduction. Am. J. Clin. Nutr. 2006, 83, 993–1016. [Google Scholar] [PubMed]
- Antony, A.C. In utero physiology: Role of folic acid in nutrient delivery and fetal development. Am. J. Clin. Nutr. 2007, 85, 598S–603S. [Google Scholar] [PubMed]
- Czeizel, A.E.; Dudas, I. Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N. Engl. J. Med. 1992, 327, 1832–1835. [Google Scholar] [CrossRef] [PubMed]
- Recommendations for the Use of Folic Acid to Reduce the Number of Cases of Spina Bifida and Other Neural Tube Defects. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00019479.htm (accessed on 11 September 1992).
- Higgins, J.R.; Quinlivan, E.P.; McPartlin, J.; Scott, J.M.; Weir, D.G.; Darling, M.R. The relationship between increased folate catabolism and the increased requirement for folate in pregnancy. BJOG 2000, 107, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Chanarin, I.; Rothman, D.; Ward, A.; Perry, J. Folate status and requirement in pregnancy. Br. Med. J. 1968, 2, 390–394. [Google Scholar] [CrossRef] [PubMed]
- McNulty, B.; McNulty, H.; Marshall, B.; Ward, M.; Molloy, A.M.; Scott, J.M.; Dornan, J.; Pentieva, K. Impact of continuing folic acid after the first trimester of pregnancy: Findings of a randomized trial of folic acid supplementation in the second and third trimesters. Am. J. Clin. Nutr. 2013, 98, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Ubeda, N.; Reyes, L.; Gonzalez-Medina, A.; Alonso-Aperte, E.; Varela-Moreiras, G. Physiologic changes in homocysteine metabolism in pregnancy: A longitudinal study in Spain. Nutrition 2011, 27, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Holmes, V.A.; Wallace, J.M.; Alexander, H.D.; Gilmore, W.S.; Bradbury, I.; Ward, M.; Scott, J.M.; McFaul, P.; McNulty, H. Homocysteine is lower in the third trimester of pregnancy in women with enhanced folate status from continued folic acid supplementation. Clin. Chem. 2005, 51, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczyk, R.T.; Zhang, J.; Betran, A.P.; Souza, J.P.; Mori, R.; Gulmezoglu, A.M.; Merialdi, M. A global reference for fetal-weight and birthweight percentiles. Lancet 2011, 377, 1855–1861. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes—2011. Diabetes Care 2011, 34, S11–S61. [Google Scholar]
- Fekete, K.; Berti, C.; Trovato, M.; Lohner, S.; Dullemeijer, C.; Souverein, O.W.; Cetin, I.; Decsi, T. Effect of folate intake on health outcomes in pregnancy: A systematic review and meta-analysis on birth weight, placental weight and length of gestation. Nutr. J. 2012, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O.; Hediger, M.L.; Schall, J.I.; Khoo, C.S.; Fischer, R.L. Dietary and serum folate: Their influence on the outcome of pregnancy. Am. J. Clin. Nutr. 1996, 63, 520–525. [Google Scholar] [PubMed]
- Pentieva, K.; Selhub, J.; Paul, L.; Molloy, A.M.; McNulty, B.; Ward, M.; Marshall, B.; Dornan, J.; Reilly, R.; Parle-McDermott, A.; et al. Evidence from a randomized trial that exposure to supplemental folic acid at recommended levels during pregnancy does not lead to increased unmetabolized folic acid concentrations in maternal or cord blood. J. Nutr. 2016, 146, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Ronnenberg, A.G.; Goldman, M.B.; Chen, D.; Aitken, I.W.; Willett, W.C.; Selhub, J.; Xu, X. Preconception homocysteine and b vitamin status and birth outcomes in chinese women. Am. J. Clin. Nutr. 2002, 76, 1385–1391. [Google Scholar] [PubMed]
- Smits, L.J.; Essed, G.G. Short interpregnancy intervals and unfavourable pregnancy outcome: Role of folate depletion. Lancet 2001, 358, 2074–2077. [Google Scholar] [CrossRef]
- Joubert, B.R.; den Dekker, H.T.; Felix, J.F.; Bohlin, J.; Ligthart, S.; Beckett, E.; Tiemeier, H.; van Meurs, J.B.; Uitterlinden, A.G.; Hofman, A.; et al. Maternal plasma folate impacts differential DNA methylation in an epigenome-wide meta-analysis of newborns. Nat. Commun. 2016, 7, 10577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Mil, N.H.; Bouwland-Both, M.I.; Stolk, L.; Verbiest, M.M.; Hofman, A.; Jaddoe, V.W.; Verhulst, F.C.; Eilers, P.H.; Uitterlinden, A.G.; Steegers, E.A.; et al. Determinants of maternal pregnancy one-carbon metabolism and newborn human DNA methylation profiles. Reproduction 2014, 148, 581–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steegers-Theunissen, R.P.; Obermann-Borst, S.A.; Kremer, D.; Lindemans, J.; Siebel, C.; Steegers, E.A.; Slagboom, P.E.; Heijmans, B.T. Periconceptional maternal folic acid use of 400 microg per day is related to increased methylation of the igf2 gene in the very young child. PLoS ONE 2009, 4, e7845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engel, S.M.; Joubert, B.R.; Wu, M.C.; Olshan, A.F.; Haberg, S.E.; Ueland, P.M.; Nystad, W.; Nilsen, R.M.; Vollset, S.E.; Peddada, S.D.; et al. Neonatal genome-wide methylation patterns in relation to birth weight in the norwegian mother and child cohort. Am. J. Epidemiol. 2014, 179, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Fryer, A.A.; Emes, R.D.; Ismail, K.M.; Haworth, K.E.; Mein, C.; Carroll, W.D.; Farrell, W.E. Quantitative, high-resolution epigenetic profiling of cpg loci identifies associations with cord blood plasma homocysteine and birth weight in humans. Epigenetics 2011, 6, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Oster, M.; Nuchchanart, W.; Trakooljul, N.; Murani, E.; Zeyner, A.; Wirthgen, E.; Hoeflich, A.; Ponsuksili, S.; Wimmers, K. Methylating micronutrient supplementation during pregnancy influences foetal hepatic gene expression and igf signalling and increases foetal weight. Eur. J. Nutr. 2015, 55, 1717–1727. [Google Scholar] [CrossRef] [PubMed]
- Wen, S.W.; Chen, X.K.; Rodger, M.; White, R.R.; Yang, Q.; Smith, G.N.; Sigal, R.J.; Perkins, S.L.; Walker, M.C. Folic acid supplementation in early second trimester and the risk of preeclampsia. Am. J. Obstet. Gynecol. 2008, 198, 45.e1–45.e7. [Google Scholar] [CrossRef] [PubMed]
- Roberfroid, D.; Huybregts, L.; Lanou, H.; Habicht, J.P.; Henry, M.C.; Meda, N.; Kolsteren, P. Prenatal micronutrient supplements cumulatively increase fetal growth. J. Nutr. 2012, 142, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Willett, W.C.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Changes in dietary intake from the first to the second trimester of pregnancy. Paediatr. Perinat. Epidemiol. 2006, 20, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.W.; Lim, A.L.; Colega, M.; Tint, M.T.; Aris, I.M.; Tan, C.S.; Chong, Y.S.; Gluckman, P.D.; Godfrey, K.M.; Kwek, K.; et al. Maternal folate status, but not that of vitamins b-12 or b-6, is associated with gestational age and preterm birth risk in a multiethnic asian population. J. Nutr. 2015, 145, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Blot, I.; Papiernik, E.; Kaltwasser, J.P.; Werner, E.; Tchernia, G. Influence of routine administration of folic acid and iron during pregnancy. Gynecol. Obstet. Investig. 1981, 12, 294–304. [Google Scholar] [CrossRef]
- Broekman, B.F.; Chan, Y.H.; Chong, Y.S.; Quek, S.C.; Fung, D.; Low, Y.L.; Ooi, Y.P.; Gluckman, P.D.; Meaney, M.J.; Wong, T.Y.; et al. The influence of birth size on intelligence in healthy children. Pediatrics 2009, 123, e1011–e1016. [Google Scholar] [CrossRef] [PubMed]
- Osmond, C.; Barker, D.J.; Winter, P.D.; Fall, C.H.; Simmonds, S.J. Early growth and death from cardiovascular disease in women. BMJ 1993, 307, 1519–1524. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Parental Characteristics | Group 1 | Group 2 | Group 3 | Group 4 | p |
|---|---|---|---|---|---|
| n = 2181 | n = 109 | n = 223 | n = 131 | ||
| Maternal characteristics | |||||
| Age (y, means ± SD) | 26.3 ± 3.4 | 27.0 ± 3.9 | 26.5 ± 3.2 | 28.3 ± 4.1 | 0 |
| ≤24 (n (%)) | 733 (33.6) | 30 (27.5) | 58 (26.0) | 20 (15.3) | |
| 25–29 (n (%)) | 1122 (51.4) | 59 (54.1) | 134 (60.1) | 66 (50.4) | 0 |
| ≥30 (n (%)) | 326 (14.9) | 20 (18.3) | 31 (13.9) | 45 (34.4) | |
| Ethnicity (Han) (%) | 98.4 | 95.4 | 97.3 | 99.2 | 0.127 |
| Residence (n (%)) | |||||
| Urban | 1714 (78.7) | 92 (86.0) | 185 (83.3) | 119 (90.8) | |
| Suburb | 286 (13.1) | 10 (9.3) | 26 (11.7) | 6 (4.6) | 0.009 |
| Rural | 177 (8.1) | 5 (4.7) | 11 (5.0) | 6 (4.6) | |
| BMI a (kg/m2, means ± SD) | 20.8 ± 2.8 | 20.8 ± 2.5 | 20.3 ± 2.3 | 20.7 ± 3.1 | 0.07 |
| <18.5(n (%)) | 419 (19.2) | 21 (19.3) | 39 (17.5) | 36 (27.5) | |
| 18.5–24.9 (n (%)) | 1594 (73.1) | 81 (74.3) | 174 (78.0) | 85 (64.9) | 0.134 |
| ≥25 (n (%)) | 168 (7.7) | 7 (6.4) | 10 (4.5) | 10 (7.6) | |
| Parity (n (%)) | |||||
| 1 | 1996 (91.5) | 99 (90.8) | 210 (94.2) | 119 (90.8) | 0.512 |
| ≥2 | 185 (8.5) | 10 (9.2) | 13 (5.8) | 12 (9.2) | |
| Educational (years) | 13.5 ± 3.1 | 13.7 ± 2.9 | 13.8 ± 3.0 | 14.6 ± 2.9 | 0.003 |
| ≤9 (n (%)) | 378 (17.3) | 13 (11.9) | 27 (2.1) | 14 (10.7) | |
| 10–15 (n (%)) | 1182 (54.2) | 65 (59.6) | 128 (57.4) | 63 (48.1) | 0.011 |
| >15 (n (%)) | 621 (28.5) | 31 (28.4) | 68 (30.5) | 54 (41.2) | |
| Monthly income (n (%)) | |||||
| Low income b | 544 (25.2) | 25 (23.1) | 43 (19.3) | 24 (18.3) | |
| Middle income b | 935 (43.2) | 48 (44.4) | 111 (49.8) | 55 (42.0) | 0.139 |
| High income b | 683 (31.6) | 35 (32.4) | 69 (30.9) | 52 (39.7) | |
| Smoking (n (%)) | 66 (3.0) | 0 | 4 (1.8) | 4 (3.1) | 0.22 |
| GDM (n (%)) | 276 (12.7) | 13 (11.9) | 31 (13.9) | 22 (16.8) | 0.538 |
| Pregnancy hypertension (n (%)) | 129 (5.9) | 5 (4.6) | 6 (2.7) | 12 (9.2) | 0.07 |
| Paternal characteristics | |||||
| Age (y, means ± SD) | 28.1 ± 4.4 | 29.2 ± 4.8 | 28.6 ± 4.7 | 30.3 ± 5.1 | 0 |
| ≤24 (n (%)) | 398 (18.3) | 15 (13.8) | 35 (15.7) | 8 (6.1) | |
| 25–29 (n (%)) | 1136 (52.1) | 49 (45.0) | 109 (48.9) | 61 (46.6) | 0 |
| ≥30 (n (%)) | 645 (29.6) | 45 (41.3) | 79 (35.4) | 62 (47.3) | |
| Educational (years) | |||||
| ≤9 (n (%)) | 304 (13.9) | 11 (10.1) | 18 (8.1) | 3 (2.3) | |
| 10–15 (n (%)) | 1206 (55.3) | 59 (54.1) | 126 (56.5) | 63 (48.1) | 0 |
| >15 (n (%)) | 671 (30.8) | 39 (35.8) | 79 (35.4) | 65 (49.6) | |
| BMI (kg/m2, means ± SD) | 23.4 ± 3.5 | 23.5 ± 5.1 | 23.4 ± 3.4 | 23.5 ± 3.3 | 0.984 |
| Newborn Characteristics | Group 1 | Group 2 | Group 3 | Group 4 | p |
|---|---|---|---|---|---|
| n = 2181 | n = 109 | n = 223 | n = 131 | ||
| Sex, M (%) | 1114 (51.1) | 57 (52.3) | 99 (44.6) | 76 (58) | 0.098 |
| Gestation week at labor | 39.5 ± 1.2 | 39.6 ± 1.1 | 39.6 ± 1.0 | 39.4 ± 1.2 | 0.411 |
| Birth weight (m ± SD in g) | 3359.2 ± 427.6 | 3432.6 ± 422.4 | 3453.0 ± 432.4 | 3435.1 ± 429.8 | 0.002 |
| Birth length (m ± SD in cm) | 50.0 ± 1.8 | 50.1 ± 1.6 | 50.4 ± 1.6 | 50.3 ± 1.5 | 0.02 |
| Head circumference (m ± SD in cm) | 34.0 ± 1.6 | 34.4 ± 1.8 | 34.1 ± 1.4 | 34.3 ± 1.3 | 0.024 |
| Chest circumference (m ± SD in cm) | 33.5 ± 1.5 | 33.8 ± 1.5 | 33.7 ± 1.5 | 33.8 ± 1.4 | 0.019 |
| LGA (n (%)) | 342 (15.7) | 17 (15.6) | 42 (18.8) | 34 (26.0) | 0.015 |
| SGA (n (%)) | 217 (10.0) | 6 (5.5) | 17 (7.6) | 12 (9.2) | 0.323 |
| LBW (n (%)) | 48 (2.2) | 0 | 2 (0.9) | 1 (0.9) | 0.158 |
| HBW (n (%)) | 165 (7.6) | 12 (11.0) | 24 (10.8) | 9 (6.9) | 0.216 |
| RRe | Group 1 | Group 2 | Group 3 | Group 4 |
|---|---|---|---|---|
| n = 2181 | n = 109 | n = 223 | n = 131 | |
| Risk of LGA birth | ||||
| model 1 | 1 | 0.99 (0.58, 1.69) | 1.25 (0.87, 1.78) | 1.88 (1.25, 2.83) ** |
| model 2 | 1 | 0.99 (0.58, 1.68) | 1.24 (0.86, 1.77) | 1.85 (1.23, 2.79) ** |
| model 3 | 1 | 0.98 (0.59, 1.70) | 1.26 (0.88, 1.80) | 1.97 (1.30, 2.98) ** |
| model 4 | 1 | 1.05 (0.61, 1.80) | 1.32 (0.92, 1.90) | 2.07 (1.36, 3.15) ** |
| model 5 | 1 | 1.05 (0.61, 1.80) | 1.29 (0.89, 1.87) | 1.98 (1.29, 3.04) ** |
| Risk of SGA birth | ||||
| model 1 | 1 | 0.53 (0.23, 1.21) | 0.75 (0.45, 1.25) | 0.91 (0.50, 1.68) |
| model 2 | 1 | 0.54 (0.23, 1.24) | 0.75 (0.45, 1.26) | 0.99 (0.54, 1.85) |
| model 3 | 1 | 0.53 (0.23, 1.22) | 0.74 (0.44, 1.25) | 0.92 (0.50, 1.71) |
| model 4 | 1 | 0.51 (0.22, 1.19) | 0.74 (0.44, 1.25) | 0.80 (0.43, 1.51) |
| Model 5 | 1 | 0.55 (0.23, 1.27) | 0.77 (0.45, 1.29) | 0.90 (0.48, 1.70) |
| RR Not Adjusting for Propensity Score | RR Adjusting for Propensity Score | |
|---|---|---|
| Risk of LGA birth | ||
| Group 1 | 1 | 1 |
| Group 2 | 0.97 (0.56, 1.69) | 1.05 (0.58, 1.88) |
| Group 3 | 1.32 (0.91, 1.90) | 1.35 (0.94, 1.96) |
| Group 4 | 1.92 (1.25, 2.98) | 1.87 (1.21, 2.87) ** |
| Risk of SGA birth | ||
| Group 1 | 1 | 1 |
| Group 2 | 0.54 (0.23, 1.26) | 0.50 (0.21, 1.21) |
| Group 3 | 0.70 (0.42, 1.18) | 0.71 (0.42, 1.18) |
| Group 4 | 0.86 (0.45, 1.64) | 0.67 (0.33, 1.32) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.; Ge, X.; Zhu, B.; Xuan, Y.; Huang, K.; Rutayisire, E.; Mao, L.; Huang, S.; Yan, S.; Tao, F. Maternal Continuing Folic Acid Supplementation after the First Trimester of Pregnancy Increased the Risk of Large-for-Gestational-Age Birth: A Population-Based Birth Cohort Study. Nutrients 2016, 8, 493. https://doi.org/10.3390/nu8080493
Wang S, Ge X, Zhu B, Xuan Y, Huang K, Rutayisire E, Mao L, Huang S, Yan S, Tao F. Maternal Continuing Folic Acid Supplementation after the First Trimester of Pregnancy Increased the Risk of Large-for-Gestational-Age Birth: A Population-Based Birth Cohort Study. Nutrients. 2016; 8(8):493. https://doi.org/10.3390/nu8080493
Chicago/Turabian StyleWang, Sufang, Xing Ge, Beibei Zhu, Yujie Xuan, Kun Huang, Erigene Rutayisire, Leijing Mao, Sanhuan Huang, Shuangqin Yan, and Fangbiao Tao. 2016. "Maternal Continuing Folic Acid Supplementation after the First Trimester of Pregnancy Increased the Risk of Large-for-Gestational-Age Birth: A Population-Based Birth Cohort Study" Nutrients 8, no. 8: 493. https://doi.org/10.3390/nu8080493