Effect of Chocolate and Yerba Mate Phenolic Compounds on Inflammatory and Oxidative Biomarkers in HIV/AIDS Individuals

Abstract
:1. Introduction
2. Experimental Section
2.1. Ethical Statement
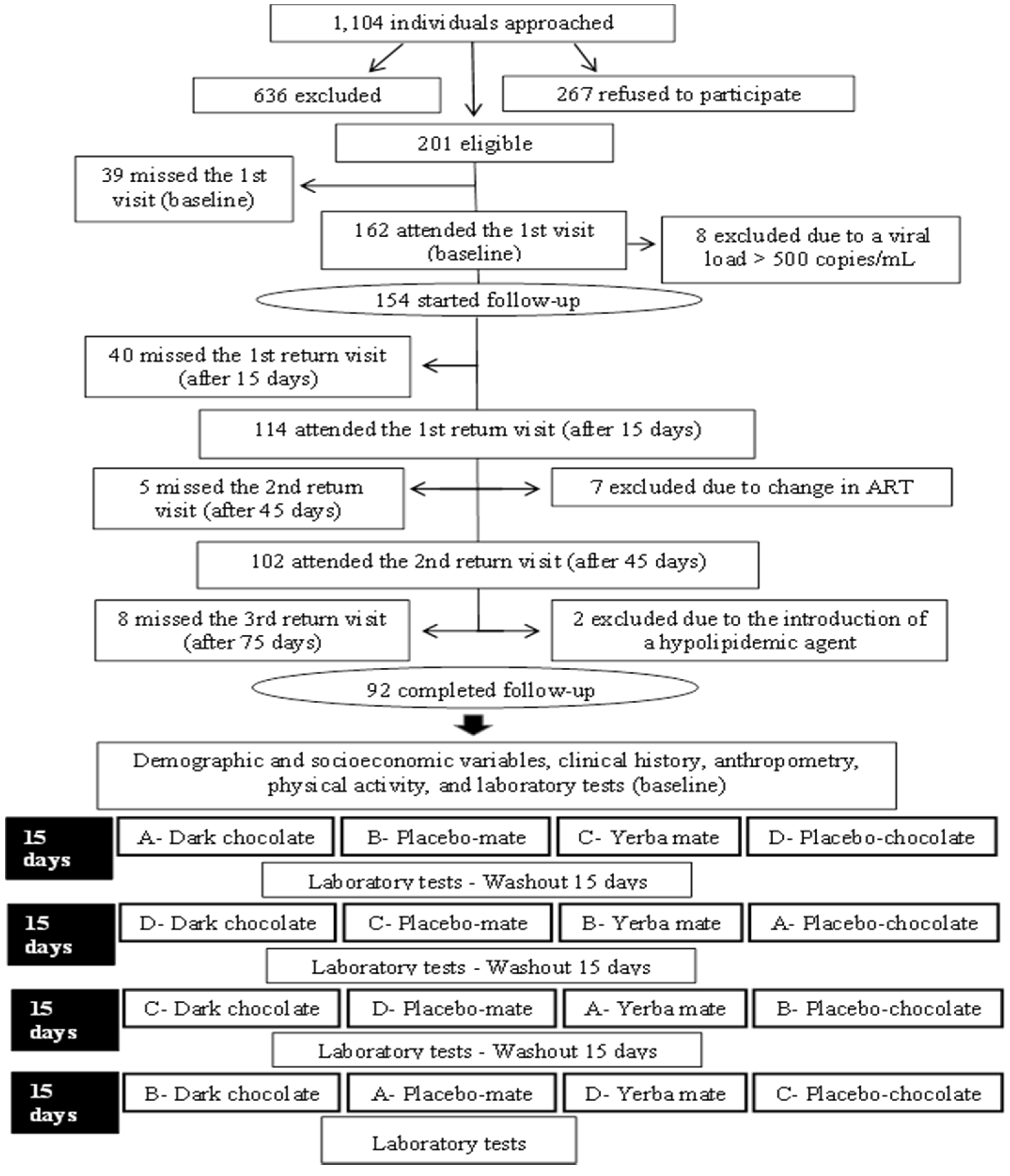
2.2. Experimental Design and Subjects
2.3. Data Collection
2.4. Supplementation
2.5. Anthropometry
2.6. Laboratory Tests
2.7. Statistical Analysis
3. Results
4. Discussion
4.1. Chocolate Consumption
4.2. Yerba Mate Consumption
4.3. hs-CRP
4.4. Fibrinogen
4.5. TBARS
4.6. White Blood Cell Count
4.7. Limitations of the Study
4.8. Forces of the Study
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Reisler, R.B.; Han, C.; Burman, W.J.; Tedaldi, E.M.; Neaton, J.D. Grade 4 events are as important as AIDS events in the era of HAART. J. Acquir. Immune Defic. Syndr. 2003, 34, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Price, T.O.; Ercal, N.; Nakaoke, R.; Banks, W.A. HIV-1 viral proteins gp 120 and Tat induce oxidative stress in brain endothelial cells. Brain Res. 2005, 1045, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Grinspoon, S.K.; Grunfeld, C.; Kotler, D.P.; Currier, J.S.; Lundgren, J.D.; Dubé, M.P.; Lipshultz, S.E.; Hsue, P.Y.; Squires, K.; Schambelan, M.; et al. State of the science conference: Initiative to decrease cardiovascular risk and increase quality of care for patients living with HIV/AIDS: Executive summary. Circulation 2008, 118, 198–210. [Google Scholar] [CrossRef] [PubMed]
- Currier, I.S. Updated on cardiovascular complications in HIV infection. Top. HIV Med. 2009, 17, 98–103. [Google Scholar] [PubMed]
- Baker, J.V.; Henry, W.K.; Neaton, J.D. The consequences of HIV infection and antiretroviral therapy use for cardiovascular disease risk: Shifting paradigms. Curr. Opin. HIV AIDS 2009, 4, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Mello, A.P.Q.; Silva, I.T.; Abdalla, D.S.P.; Damasceno, N.R.T. Electronegative low-density lipoprotein: Origin and impact on health and disease. Atherosclerosis 2011, 215, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Aukrust, P.; Muller, F.; Svardal, A.M.; Ueland, T.; Berge, R.K.; Froland, S.S. Disturbed glutathione metabolism and decreased antioxidants levels in human immunodeficiency virus-infected patients during highly active antiretroviral therapy—Potential immunomodulatory effects of antioxidants. J. Infect. Dis. 2003, 188, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Bacchetti, P.; Gripshover, B.; Grunfeld, C.; Heymsfield, S.; McCreath, H.; Osmond, D.; Saag, M.; Scherzer, R.; Shlipak, M.; Tien, P. Study of Fat Redistribution and Metabolic Change in HIV Infection (FRAM). Fat distribution in men with HIV infection. J. Acquir. Immune Defic. Syndr. 2005, 40, 121–131. [Google Scholar] [PubMed]
- Piche, M.E.; Lemieux, S.; Weisnagel, S.J.; Corneau, L.; Nadeau, A.; Bergeron, J. Relation of high-sensitivity C-reactive protein, interleukin-6, tumor necrosis factor-alpha, and fibrinogen to abdominal adipose tissue, blood pressure, and cholesterol and triglyceride levels in healthy postmenopausal women. Am. J. Cardiol. 2005, 96, 92–97. [Google Scholar] [CrossRef] [PubMed]
- FRAM-Study of Fat Redistribution and Metabolic Change in HIV Infection. Fat distribution in women with HIV infection. J. Acquir. Immune Defic. Syndr. 2006, 42, 562–571. [Google Scholar]
- Osakabe, N.; Natsume, M.; Adachi, T.; Yamagishi, M.; Hirano, R.; Takizawa, T.; Itakura, H.; Kondo, K. Effects of cacao liquor polyphenols on the susceptibility of low-density lipoprotein to oxidation in hypercholesterolemic rabbits. J. Atheroscler. Thromb. 2000, 7, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Giuseppe, R.; Castelnuovo, A.; Centritto, F.; Zito, F.; Curtis, A.; Costanzo, S.; Vohnout, B.; Sieri, S.; Krogh, V.; Donati, M.B.; et al. Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. J. Nutr. 2008, 138, 1939–1945. [Google Scholar] [PubMed]
- Pimentel, G.D.; Lira, F.S.; Rosa, J.C.; Caris, A.V.; Pinheiro, F.; Ribeiro, E.B.; Oller, C.M.; Oyama, L.M. Yerba mate extract (Ilex paraguariensis) attenuates both central and peripheral inflammatory effects of diet-induced obesity in rats. J. Nutr. Biochem. 2013, 24, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Efraim, P.; Tucci, M.L.; Pezoa-García, N.H.; Haddad, R.; Eberlin, M. Teores de compostos fenólicos de sementes de cacaueiro de diferentes genótipos. Brazilian J. Food Technol. 2006, 9, 229–236. [Google Scholar]
- Efraim, P.; Alves, A.B.; Jardim, D.C.P. Polyphenols in cocoa and derivatives: Factors of variation and health effects. J. Food Technol. 2011, 14, 181–201. [Google Scholar]
- Wollgast, J.; Anklan, E. Polyphenols in chocolate: Is there a contribution to human health? Food Res. Intern. 2000, 33, 449–459. [Google Scholar] [CrossRef]
- Bastos, D.H.M.; Fornari, A.C.; Queiroz, Y.S.; Soares, R.A.M.; Torres, E.A.F.S. The chlorogenic acid and caffeine content of yerba maté. (Ilex paraguariensis) beverages. Acta Farm. Bonaerense 2005, 24, 91–95. [Google Scholar]
- Mursu, J.; Voutilainen, S.; Nurmi, T.; Rissanen, T.H.; Virtanen, J.K.; Kaikkonen, J.; Nyyssönen, K.; Salonen, J.T. Dark chocolate consumption increase HDL cholesterol concentration and chocolate fatty acids may inhibit lipid peroxidation in healthy human. Free Rad. Biol. Med. 2004, 37, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Hamed, M.S.; Gambert, S.; Bliden, K.P.; Bailon, O.; Anand, S.; Antonino, M.J.; Hamed, F.; Tantry, U.S.; Gurbel, P.A. Dark chocolate effect on platelet activity, C-reactive protein and lipid profile: A pilot study. South Med. J. 2008, 101, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Morais, E.C.; Stefanuto, A.; Klein, G.A.; Boaventura, B.C.; Andrade, F.; Wazlawik, E.; Di Pietro, P.F.; Maraschin, M.; da Silva, E.L. Consumption of yerba mate (Ilex paraguariensis) improves serum lipid parameters in healthy dyslipidemic subjects and provides an additional LDL-cholesterol reduction in individuals on statin therapy. J. Agric. Food Chem. 2009, 57, 8316–8324. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Liu, X.; Bai, Y.Y.; Li, S.H.; Sun, K.; He, C.; Hui, R. Short-term effect of cocoa product consumption on lipid profile: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2010, 92, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Nemes, M.I.B.; Carvalho, H.B.; Souza, M.F.M. Antiretroviral therapy adherence in Brazil. AIDS 2004, 18 (Suppl. 3), S15–S20. [Google Scholar] [CrossRef] [PubMed]
- Mazzafera, P. Maté drinking: Caffeine and phenolic acid intake. Food Chem. 1997, 60, 67–71. [Google Scholar] [CrossRef]
- Osakabe, N.; Baba, S.; Yasuda, A.; Iwamoto, T.; Kamiyama, M.; Takizawa, T.; Itakura, H.; Kondo, K. Daily cocoa intake reduces the susceptibility of low-density lipoprotein to oxidation as demonstrated in healthy human volunteers. Free Radic. Res. 2001, 34, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O.; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Centers for Disease Control and Prevention; American Heart Association. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [PubMed]
- Handin, R.I. Disorders of coagulation and Thrombosis. In Harrison’s Principles of Internal Medicine, 14th ed.; Mc Graw Hill Interamericana do Brasil Ltda: Rio de Janeiro, Brazil, 1988; Volume 1, pp. 736–743. [Google Scholar]
- Antolovich, M.; Prenzler, P.D.; Patsalides, E.; McDonald, S.; Robards, K. Methods for testing antioxidant activity. Analyst. 2002, 127, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Cirico, T.L.; Omaye, S.T. Additive or synergic effects of phenolic compounds on human low density lipoprotein oxidation. Food Chem. Toxicol. 2006, 44, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Mursu, J.; Voutilainen, S.; Nurmi, T.; Helleranta, M.; Rissanen, T.; Nurmi, A.; Kaikkonen, J.; Porkkala-Sarataho, E.; Nyyssönen, K.; Virtanen, J.K.; et al. Polyphenol-rich phloem enhances the resistence of total serum lipids to oxidation in men. J. Agric. Food Chem. 2005, 53, 3017–3022. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.J.; Friedrickson, D.S. Estimation of the concentration of low-density-lipoprotein cholesterol in plasma, without use of the preparative ultra centrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [PubMed]
- National Cholesterol Education Program. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Hill, V.L.; Simpson, V.Z.; Higgins, J.M.; Hu, Z.; Stevens, R.A.; Metcalf, J.A.; Baseler, M. Evaluation of the performance of the Sysmex XT-2000i Hematology Analyzer with whole bloods stores at room temperature. Lab. Med. 2009, 40, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Mellors, J.W.; Rinaldo, C.R.; Gupta, P.; White, R.M.; Todd, J.A.; Kingsley, L.A. Prognosis in HIV-1 infection predicted by the quantity of virus in plasma. Science 1996, 272, 1167–1170. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Cesari, M.; Anton, S.; Marzetti, E.; Giovannini, S.; Seo, A.Y.; Carter, C.; Yu, B.P.; Leeuwenburgh, C. Molecular in flammation: Underpinnings of aging and age-related diseases. Ageing Res. Rev. 2009, 8, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Hegele, R.A. HIV-associated dyslipidemia: Pathogenesis and treatment. Lancet Infect Dis. 2007, 7, 787–796. [Google Scholar] [CrossRef]
- Almeida, L.B.; Giudici, K.V.; Jaime, P.C. Consumo alimentar e dyslipidemia decorrente da terapia antiretroviral combinada para infecção pelo HIV: Uma revisão sistemática. Arq. Bras. Endocrinol. Metabol. 2009, 53, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Agell, M.; Urpi-Sarda, M.; Sacanella, E.; Camino-López, S.; Chiva-Blanch, G.; Llorente-Cortés, V.; Tobias, E.; Roura, E.; Andres-Lacueva, C.; Lamuela-Raventós, R.M.; et al. Cocoa consumption reduces NF-κB activation in peripheral blood mononuclear cells in humans. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Baba, S.; Osakabe, N.; Kato, Y.; Natsume, M.; Yasuda, A.; Kido, T.; Fukuda, K.; Muto, Y.; Kondo, K. Continuous intake of polyphenolic compounds containing cocoa powder reduces LDL oxidative susceptibility and has beneficial effects on plasma HDL-cholesterol concentrations in humans. Am. J. Clin. Nutr. 2007, 85, 709–717. [Google Scholar] [PubMed]
- Mosimann, A.L.; Wilhem-Filho, D.; Silva, E.L. Aqueous extract of Ilex paraguariensis attenuates the progression of atherosclerosis in cholesterol-fed rabbits. Biol. Factors 2006, 26, 59–70. [Google Scholar]
- Matsumoto, R.L.; Bastos, D.H.; Mendonça, S.; Nunes, V.S.; Bartchewsky, W.; Ribeiro, M.L.; Oliveira, C.P. Effects of mate tea (Ilex paraguariensis) ingestion on mRNA expression of antioxidant enzymes, lipid peroxidation, and total antioxidant status in healthy young women. J. Agric. Food Chem. 2009, 57, 1775–1780. [Google Scholar] [CrossRef] [PubMed]
- Boaventura, B.C.; Di Pietro, P.F.; Stefanuto, A.; Klein, G.A.; de Morais, E.C.; de Andrade, F.; Wazlawik, E.; da Silva, E.L. Association of mate tea (Ilex paraguariensis) intake and dietary intervention and effects on oxidative stress biomarkers of dyslipidemic subjects. Nutrition 2012, 28, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Lau, B.; Sharrett, A.R.; Kingsley, L.A.; Post, W.; Palella, F.J.; Visscher, B.; Gange, S.J. C-reactive protein is a marker for human immunodeficiency virus disease progression. Arch. Intern. Med. 2006, 166, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Bo, M.; Raspo, S.; Morra, F.; Cassader, M.; Isaia, G.; Poli, L. Body fat is the main predictor of fibrinogen levels in healthy non-obese men. Metabolism 2004, 53, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Omoregie, R.; Adeghe, J.E.; Ogefere, H.O.; Omokaro, E.U.; Ekeh, C.C. Haemorheologic and fibrinolytic activity in Nigerian HIV infected patients. Afr. Health Sci. 2008, 8, 217–219. [Google Scholar] [PubMed]
- Walter, M.F.; Jacob, R.F.; Jeffers, B.; Ghadanfar, M.M.; Preston, G.; Buch, J.; Mason, R.P. Serum levels of thiobarbituric acid reactive substances predict cardiovascular events in patients with stable coronary artery disease : A longitudinal analysis of the PREVENT study. J. Am. Coll. Cardiol. 2004, 44, 1996–2002. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Miki, T.; Sha, S.; Hirata, K.; Ishikawa, Y.; Yokoyama, M. Serum levels of thiobarbituric acid-reactive substances are associated with risk of coronary heart disease. J. Atheroscler. Thromb. 2011, 18, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Junqueira, V.B.; Barros, S.B.; Chan, S.S.; Rodrigues, L.; Giavarotti, L.; Abud, R.L.; Deucher, G.P. Aging and oxidative stress. Mol. Aspects Med. 2004, 25, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Ngondi, J.L.; Oben, J.; Forkah, D.M.; Etame, L.H.; Mbanya, D. The effect of different combination therapies on oxidative stress markers in HIV infected patients in Cameroon. AIDS Res. Ther. 2006, 22, 3–19. [Google Scholar]
- Campillo-Gimenez, L.; Casulli, S.; Dudoit, Y.; Seang, S.; Carcelain, G.; Lambert-Niclot, S.; Appay, V.; Autran, B.; Tubiana, R.; Elbim, C. Neutrophilsin antiretroviral therapy-controlled HIV demonstrate hyperactivation associated with a specific IL-17/IL-22 environment. J. Allergy Clin. Immunol. 2014, 134, 1142–1152. [Google Scholar] [CrossRef] [PubMed]
- Kenny, T.; Shu, S.; Moritoki, Y.; Keen, C.L.; Gershwin, M.E. Cocoa flavanols and procyanidins can modulate the lipopolysaccharide activation of polymorphonuclear cells in vitro. J. Med. Food 2009, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Esser, D.; Mars, M.; Oosterink, E.; Stalmach, A.; Müller, M.; Afman, L.A. Dark chocolate consumption improves leukocyte adhesion factors and vascular function in overweight men. FASEB J. 2014, 28, 1464–1473. [Google Scholar] [CrossRef] [PubMed]
- Heptinstall, S.; May, J.; Fox, S.; Kwik-Uribe, C.; Zhao, L. Cocoa flavanols and platelet and leukocyte function: Recent in vitro and ex vivo studies in healthy adults. J. Cardiovasc. Pharmacol. 2006, 47, 197–205. [Google Scholar] [CrossRef]
- Davison, G.; Callister, R.; Williamson, G.; Cooper, K.A.; Gleeson, M. The effect of acute pre-exercise dark chocolate consumption on plasma antioxidant status, oxidative stress and immunoendocrine responses to prolonged exercise. Eur. J. Nutr. 2012, 51, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, M.S.; Kennedy, K.; Singhal, A.; Martin, R.M.; Ness, A.; Hadders-Algra, M.; Koletzko, B.; Lucas, A. How much loss to follow-up is acceptable in long-term randomized trialsand prospective studies? Arch. Dis. Child 2008, 93, 458–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: http://www.cochrane-handbook.org (accessed on 26 February 2016).



{kind=link}
{kind=link}
| Variable | Completed the Study N (%)Mean (SD) | Did Not Complete the Study N (%)Mean (SD) | p-Value | ||
|---|---|---|---|---|---|
| Gender | 0.63 | ||||
| Male | 58 (63.0) | 36 (58.1) | |||
| Female | 34 (37.0) | 26 (41.9) | |||
| Age (years) | 92 (100) | 45.0 (7.1) | 62 (100) | 41.0 (8.1) | 0.00 |
| Race/ethnicity | |||||
| White | 43 (46.7) | 39 (62.9) | 0.12 | ||
| Black | 16 (17.4) | 6 (9.7) | |||
| Mixed race | 31 (33.7) | 17 (27.4) | |||
| Schooling (years) | 92 (100) | 5.0 (1.6) | 62 (100) | 5.0 (1.7) | 0.92 |
| Per capita income (US$) | 92 (100) | 465.6 (477.4) | 62 (100) | 378.1 (321.0) | 0.50 |
| Smoking | 0.14 | ||||
| Yes | 16 (17.4) | 19 (30.7) | |||
| No | 61 (66.3) | 36 (58.1) | |||
| Ex | 15 (16.3) | 7 (11.3) | |||
| Alcohol ingestion | 0.56 | ||||
| Yes | 46 (50) | 28 (45.2) | |||
| No | 46 (50) | 34 (54.8) | |||
| BMI (kg/m2) | 92 (100) | 23.4 (3.9) | 62 (100) | 23.4 (3.4) | 0.96 |
| Body fat (%) | 92 (100) | 19.8 (9.1) | 62 (100) | 21.2 (9.5) | 0.33 |
| CD4+ T lymphocytes (cells/mm3) | 92 (100) | 596.1 (263.4) | 62 (100) | 547.1 (281.5) | |
| Time since HIV diagnosis (years) | 92 (100) | 13.32 (5.1) | 62 (100) | 11.9 (5.2) | 0.07 |
| Time since onset of ART (years) | 92 (100) | 10.7 (5.2) | 62 (100) | 9.4 (4.9) | 0.08 |
| Adherence to ART | 0.16 | ||||
| Yes | 88 (95.7) | 56 (90.3) | |||
| No | 4 (4.4) | 6 (9.7) | |||
| hs-CRP (mg/dL) | 3.0 (8.3) | 3.1 (8.5) | 0.74 | ||
| <1.0 (low risk) | 31 (33.7) | 19 (30.6) | |||
| 1.0│-│ 3.0 (average risk) | 40 (43.5) | 26 (41.9) | |||
| >3.0 (high risk) | 21 (22.8) | 17 (27.4) | |||
| Fibrinogen (mg/dL) | 350.6 (121.6) | 346.6 (116.6) | 0.18 | ||
| 150│-│ 400 (appropriate) | 66 (71.7) | 44 (70.9) | |||
| >400 (high) | 26 (28.3) | 18 (29.0) | |||
| Total cholesterol | 92 (100) | 193.2 (35.2) | 62 (100) | 188.7 (30.8) | 0.09 |
| HDL-c (mg/dL) | 49.8 (14.8) | 44.8 (14.5) | 0.06 | ||
| Men | |||||
| <40 (low) | 22 (37.9) | 15 (41.6) | |||
| ≥40 (appropriate) | 36 (62.1) | 21 (58.3) | |||
| Women | |||||
| <50 (low) | 13 (38.2) | 9 (34.6) | |||
| ≥50 (appropriate) | 21 (61.8) | 17 (65.3) | |||
| LDL-c (mg/dL) | 92 (100) | 114.4 (30.7) | 53 (85.5) | 117.9 (39.5) | 0.65 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrilli, A.A.; Souza, S.J.; Teixeira, A.M.; Pontilho, P.M.; Souza, J.M.P.; Luzia, L.A.; Rondó, P.H.C. Effect of Chocolate and Yerba Mate Phenolic Compounds on Inflammatory and Oxidative Biomarkers in HIV/AIDS Individuals. Nutrients 2016, 8, 132. https://doi.org/10.3390/nu8050132
Petrilli AA, Souza SJ, Teixeira AM, Pontilho PM, Souza JMP, Luzia LA, Rondó PHC. Effect of Chocolate and Yerba Mate Phenolic Compounds on Inflammatory and Oxidative Biomarkers in HIV/AIDS Individuals. Nutrients. 2016; 8(5):132. https://doi.org/10.3390/nu8050132
Chicago/Turabian StylePetrilli, Aline A., Suelen J. Souza, Andrea M. Teixeira, Patricia M. Pontilho, José M. P. Souza, Liania A. Luzia, and Patricia H. C. Rondó. 2016. "Effect of Chocolate and Yerba Mate Phenolic Compounds on Inflammatory and Oxidative Biomarkers in HIV/AIDS Individuals" Nutrients 8, no. 5: 132. https://doi.org/10.3390/nu8050132