Nigerian Honey Ameliorates Hyperglycemia and Dyslipidemia in Alloxan-Induced Diabetic Rats

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Animals
2.3. Honey
2.4. Induction of Diabetes Mellitus
2.5. Treatment
- Group 1: Non-diabetic rats administered 1 mL/kg BW of drinking water
- Group 2: Diabetic rats administered 1 mL/kg BW of drinking water
- Group 3: Diabetic rats treated with 1.0 g/kg BW of honey
- Group 4: Diabetic rats treated with 2.0 g/kg BW of honey
- Group 5: Diabetic rats treated with 3.0 g/kg BW of honey
2.6. Biochemical Analysis
2.7. Determination of Atherogenic Index (AI), Coronary Risk Index (CRI) and Cardiovascular Risk Index (CVRI)
2.8. Statistical Analysis
3. Results
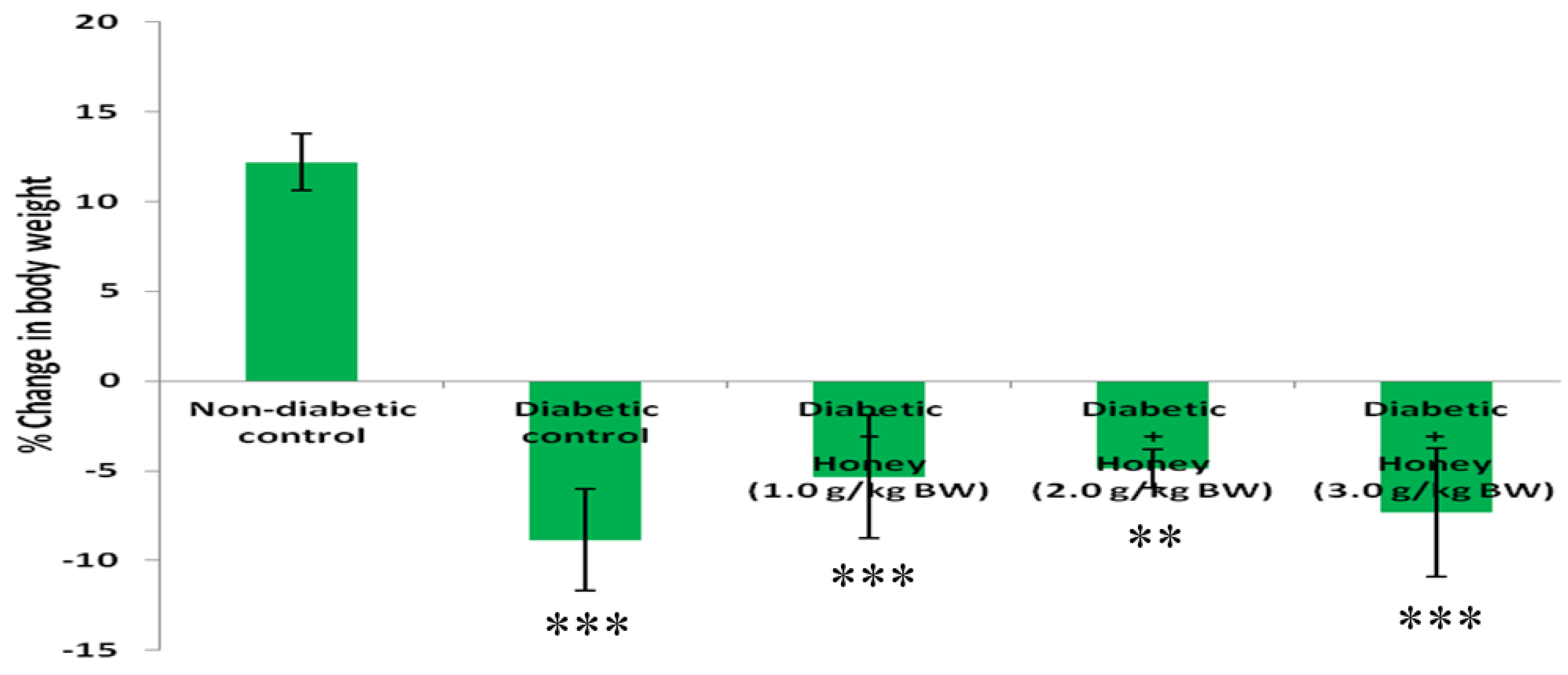
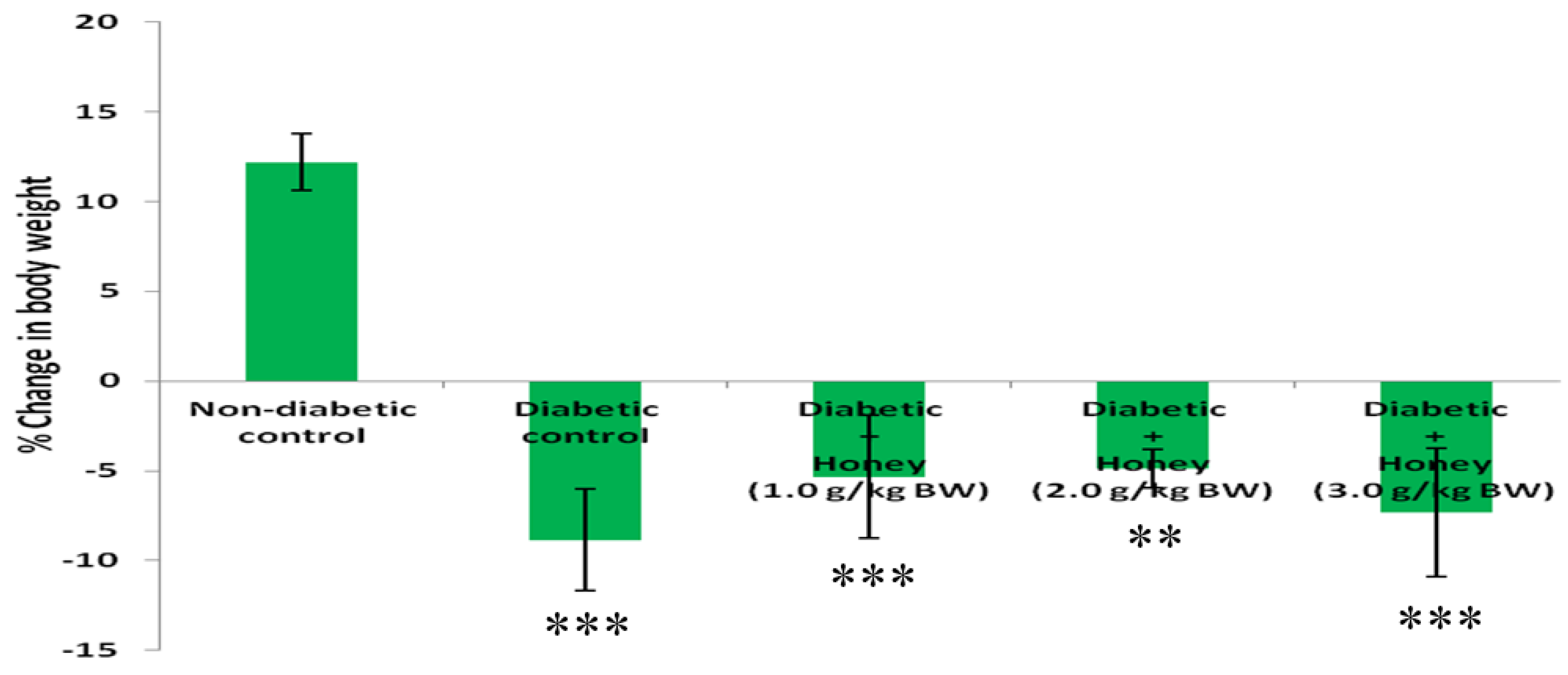
3.1. Effect of Honey on Percentage (%) Change in Body Weight (BW) of Diabetic Rats
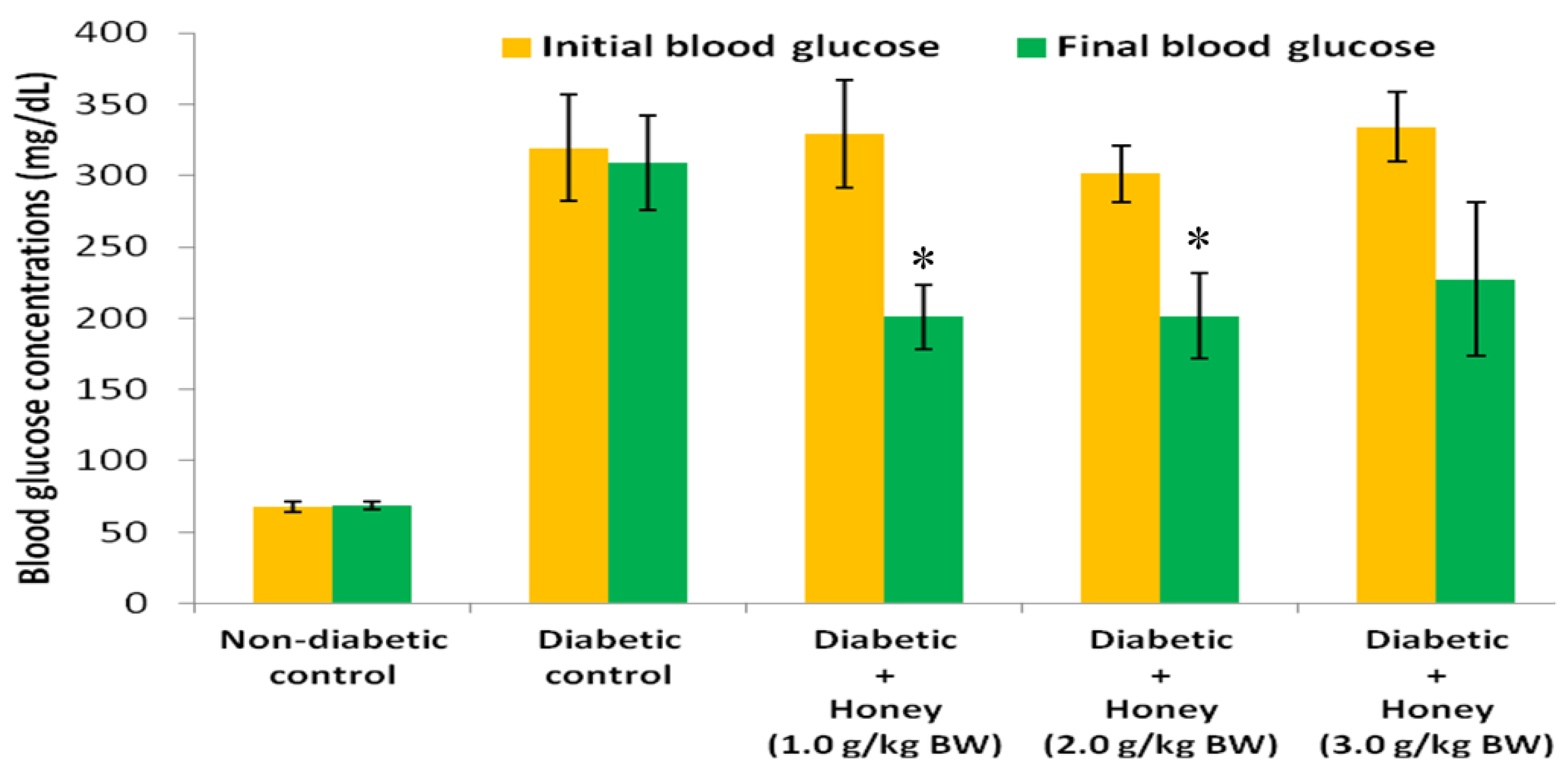
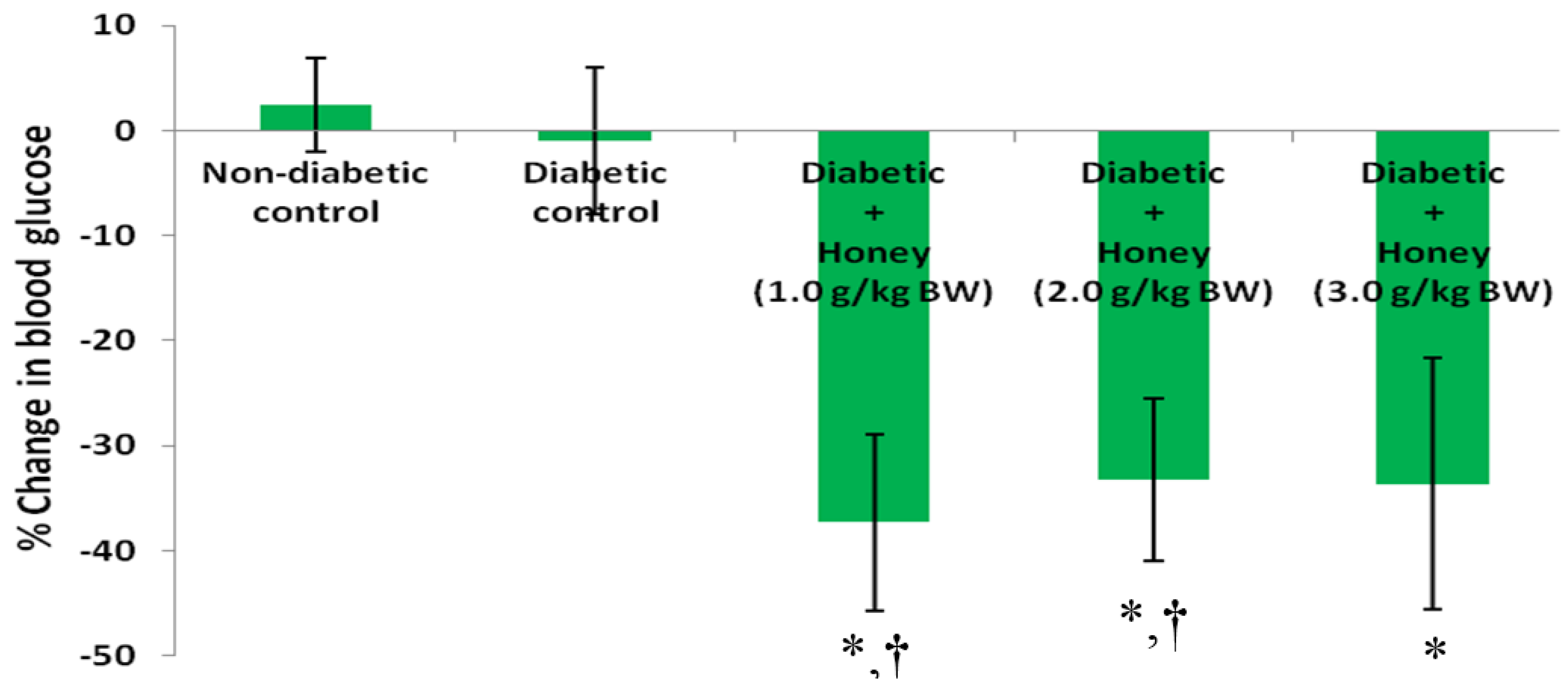
3.2. Effects of Honey on Blood Glucose (BG) Concentrations and Percentage (%) Change in BG of Diabetic Rats
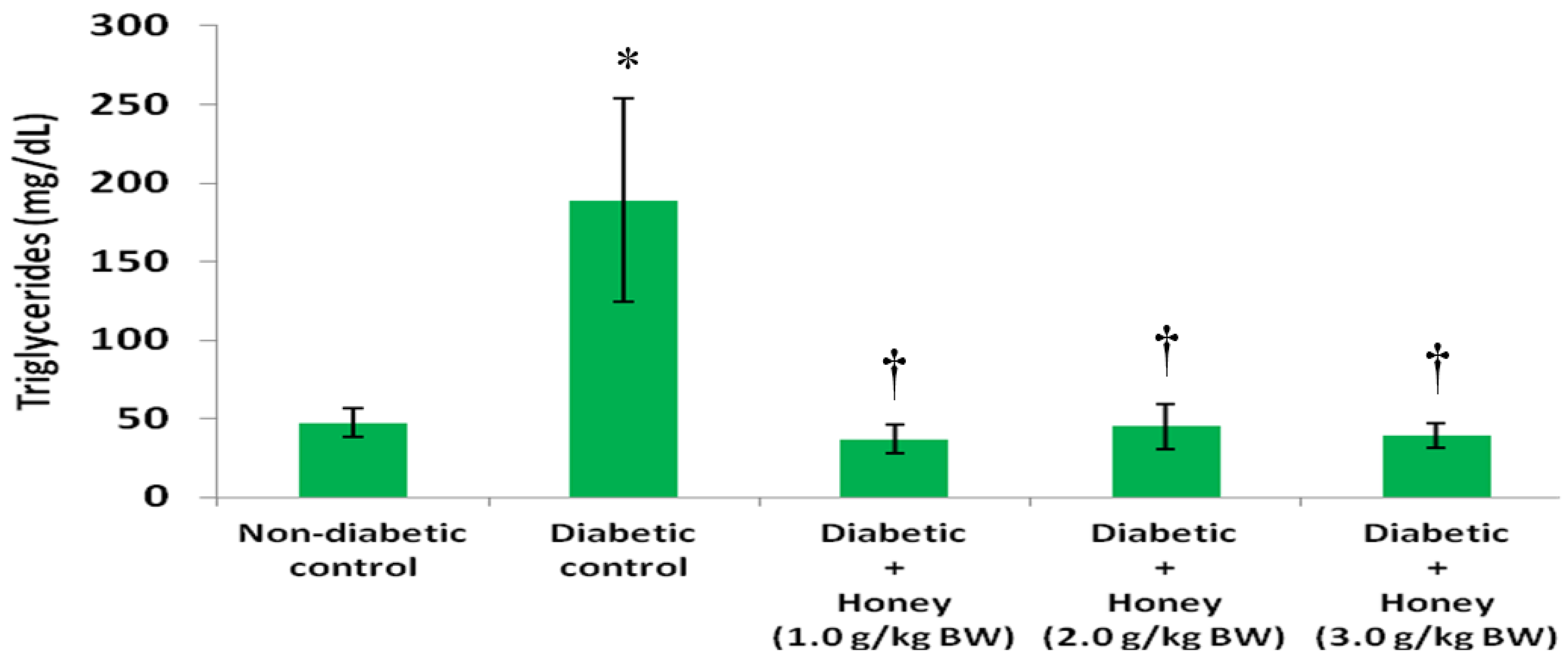
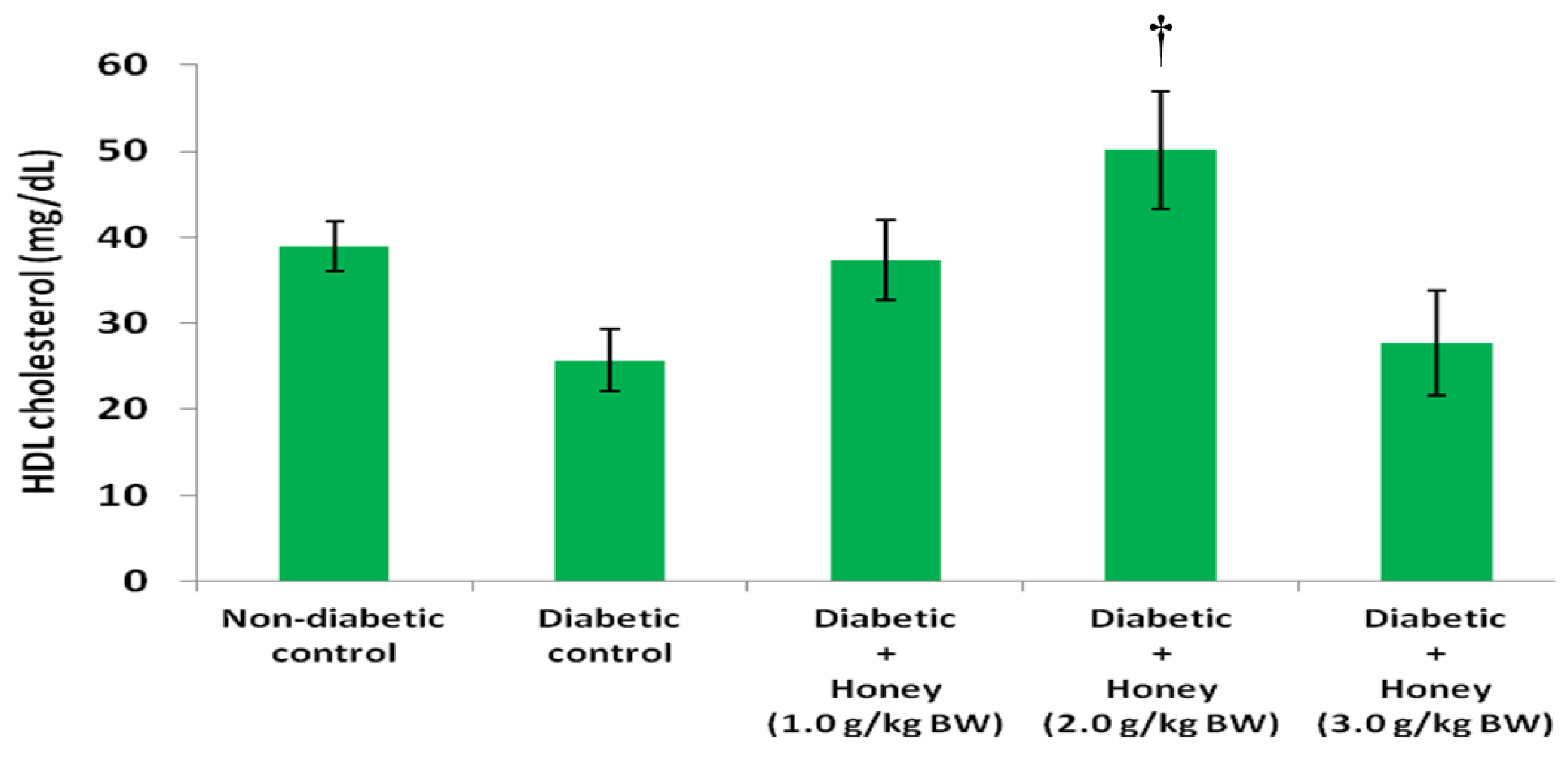
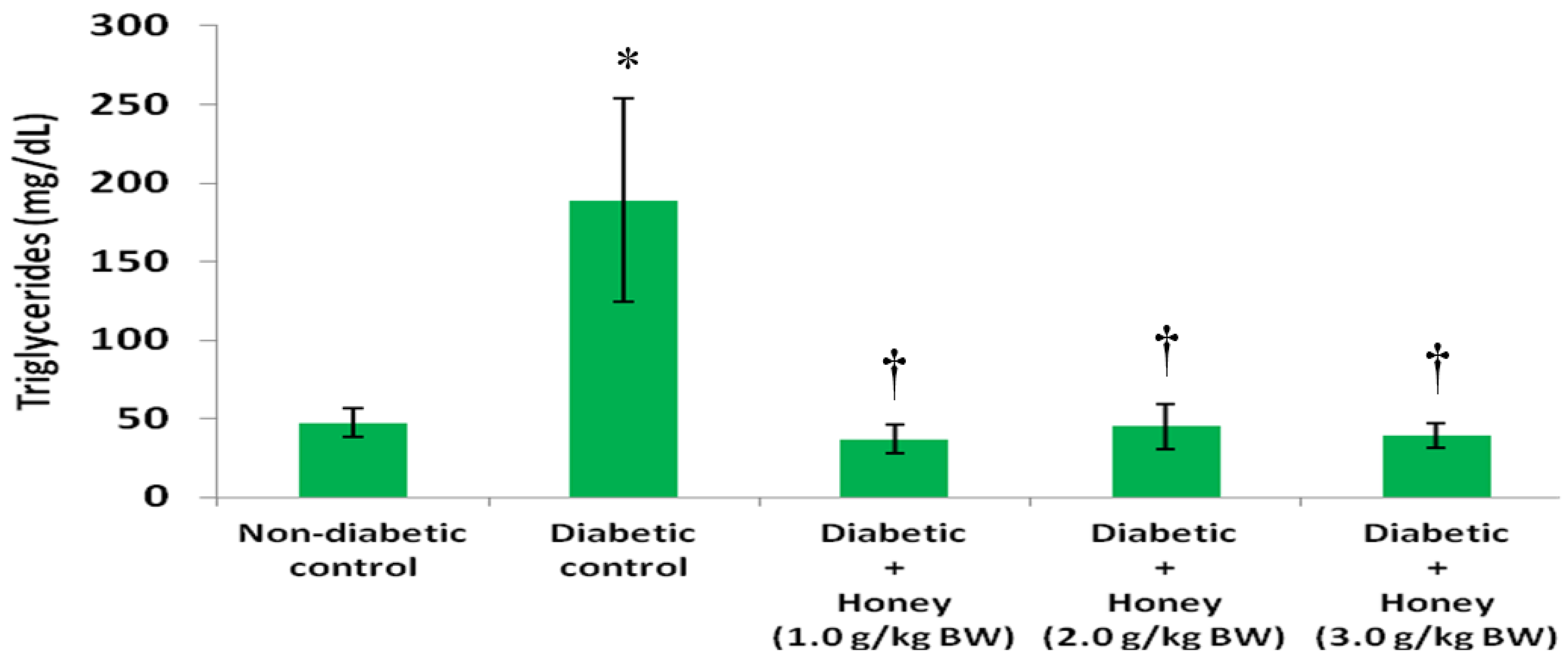
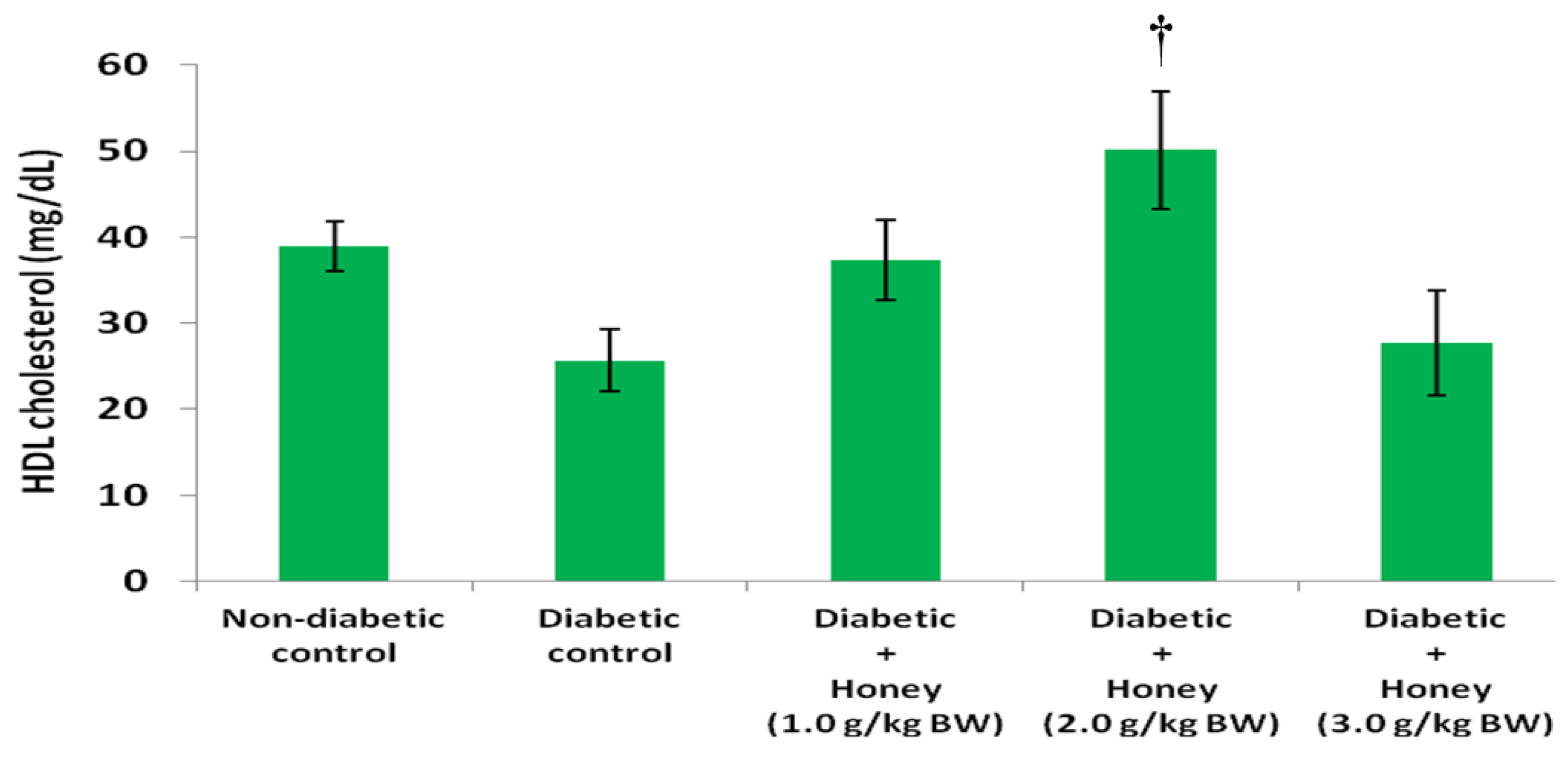
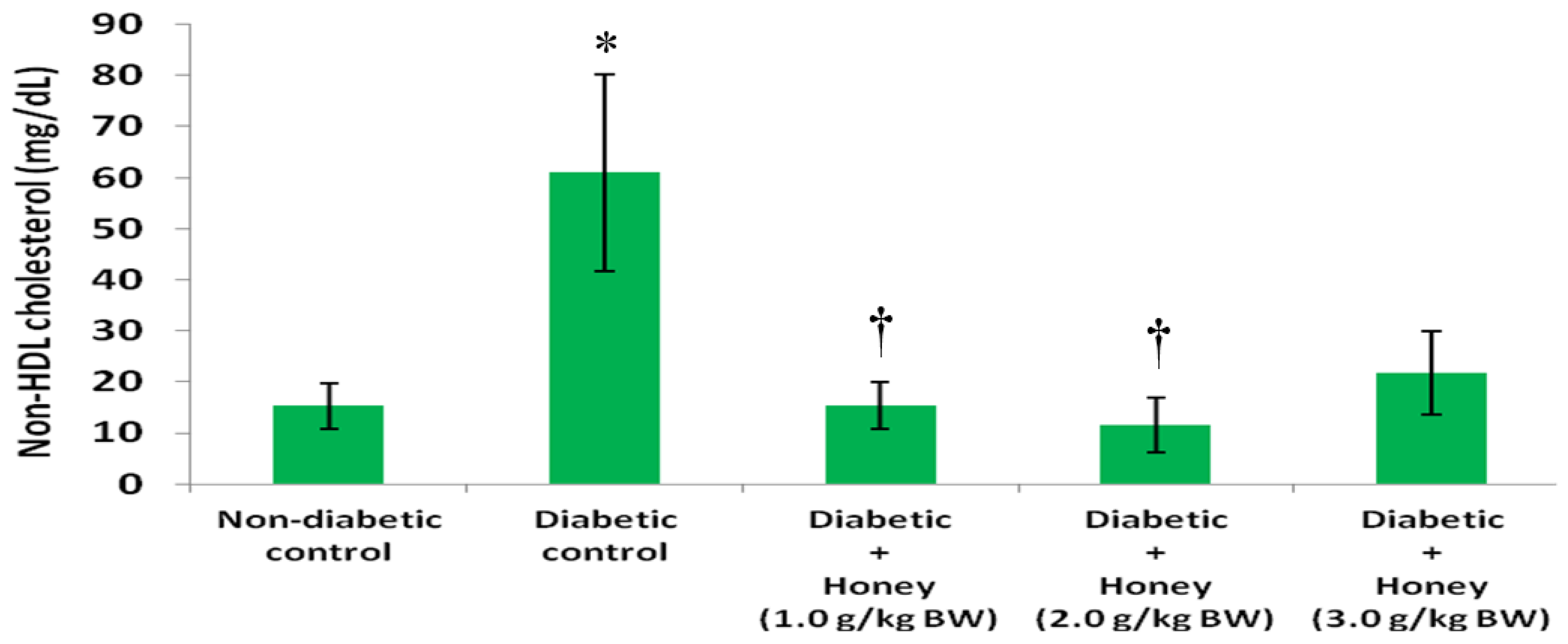
3.3. Effects of Honey on Triglycerides (TG), High Density Lipoprotein (HDL), Non-HDL and Very Low Density Lipoprotein (VLDL) Cholesterol of Diabetic Rats
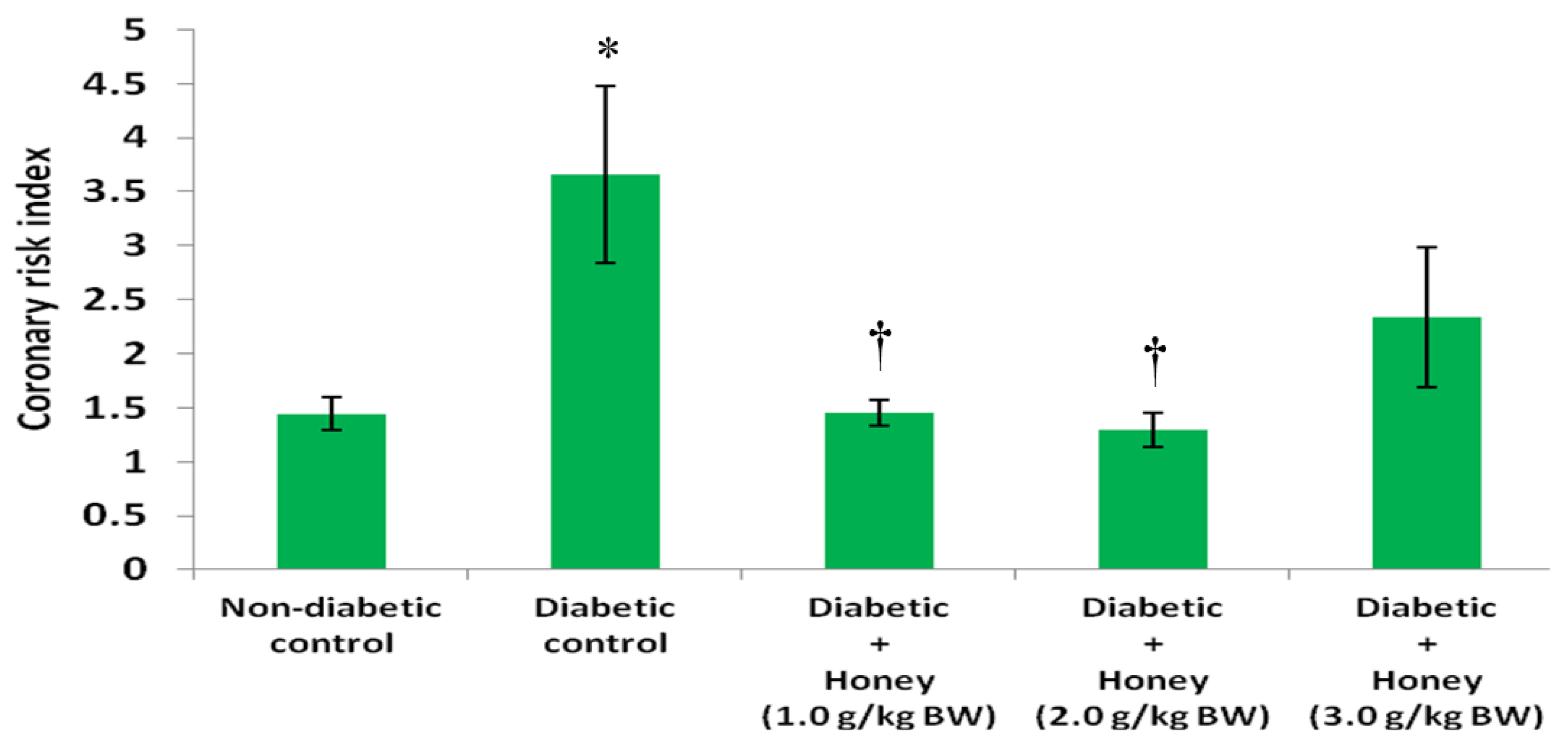
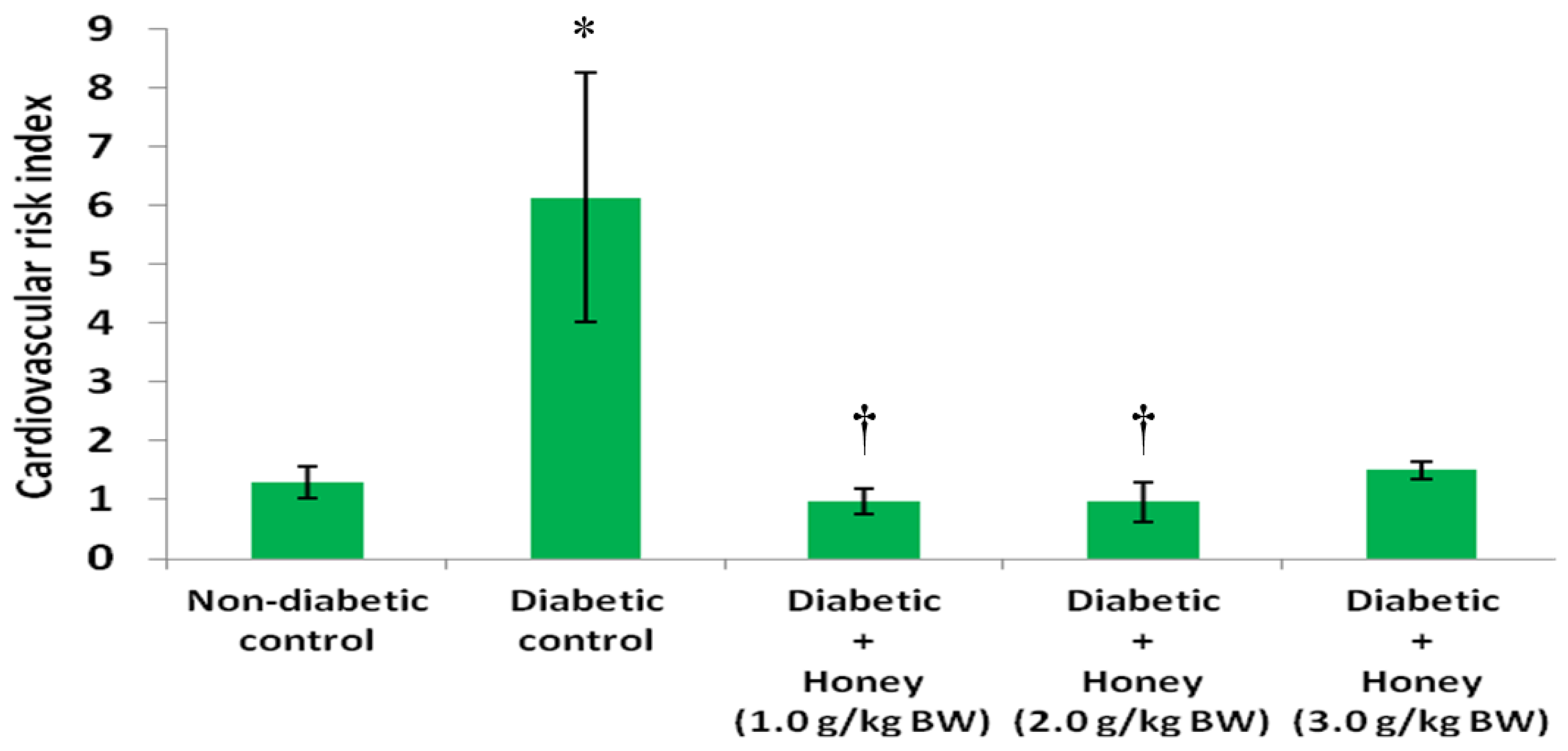
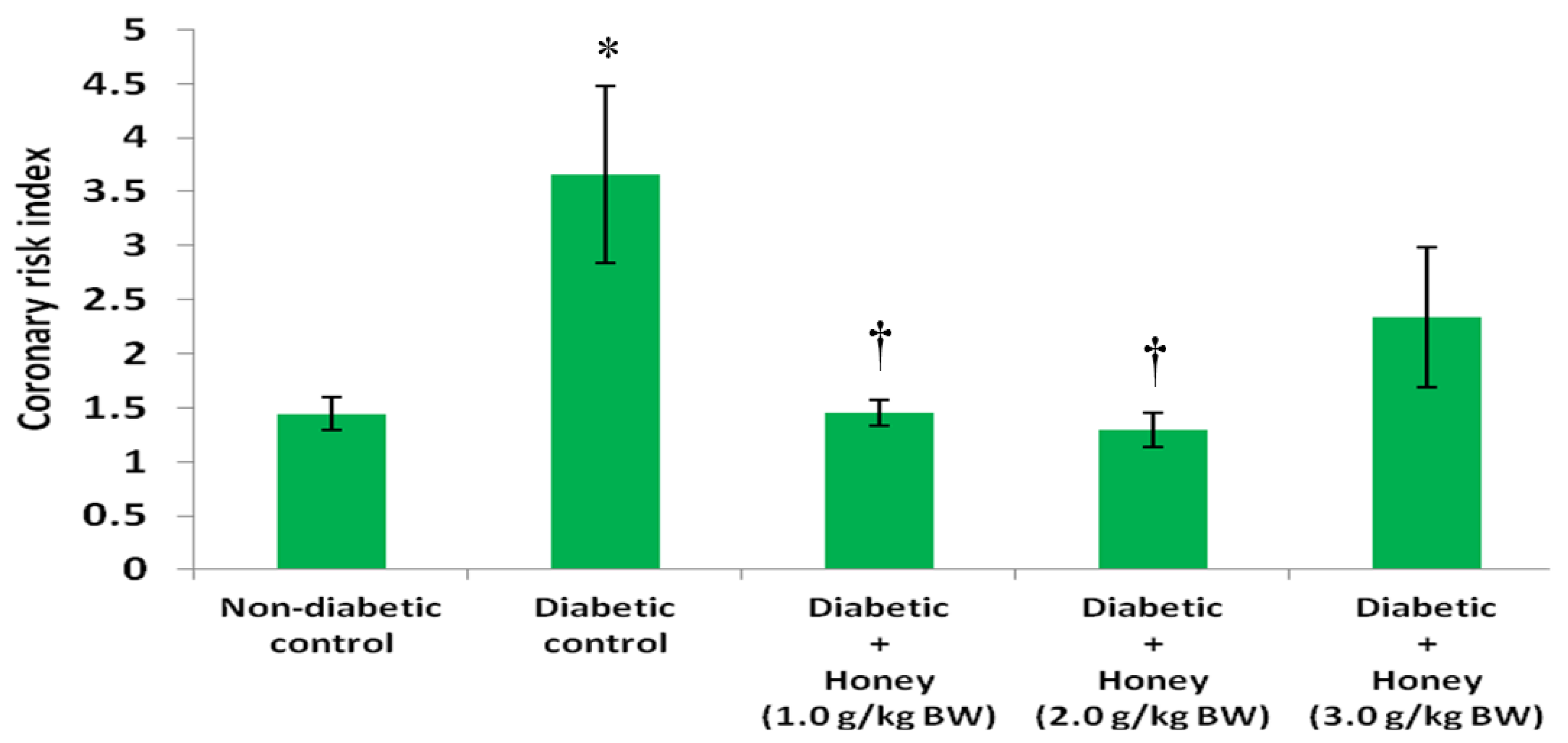
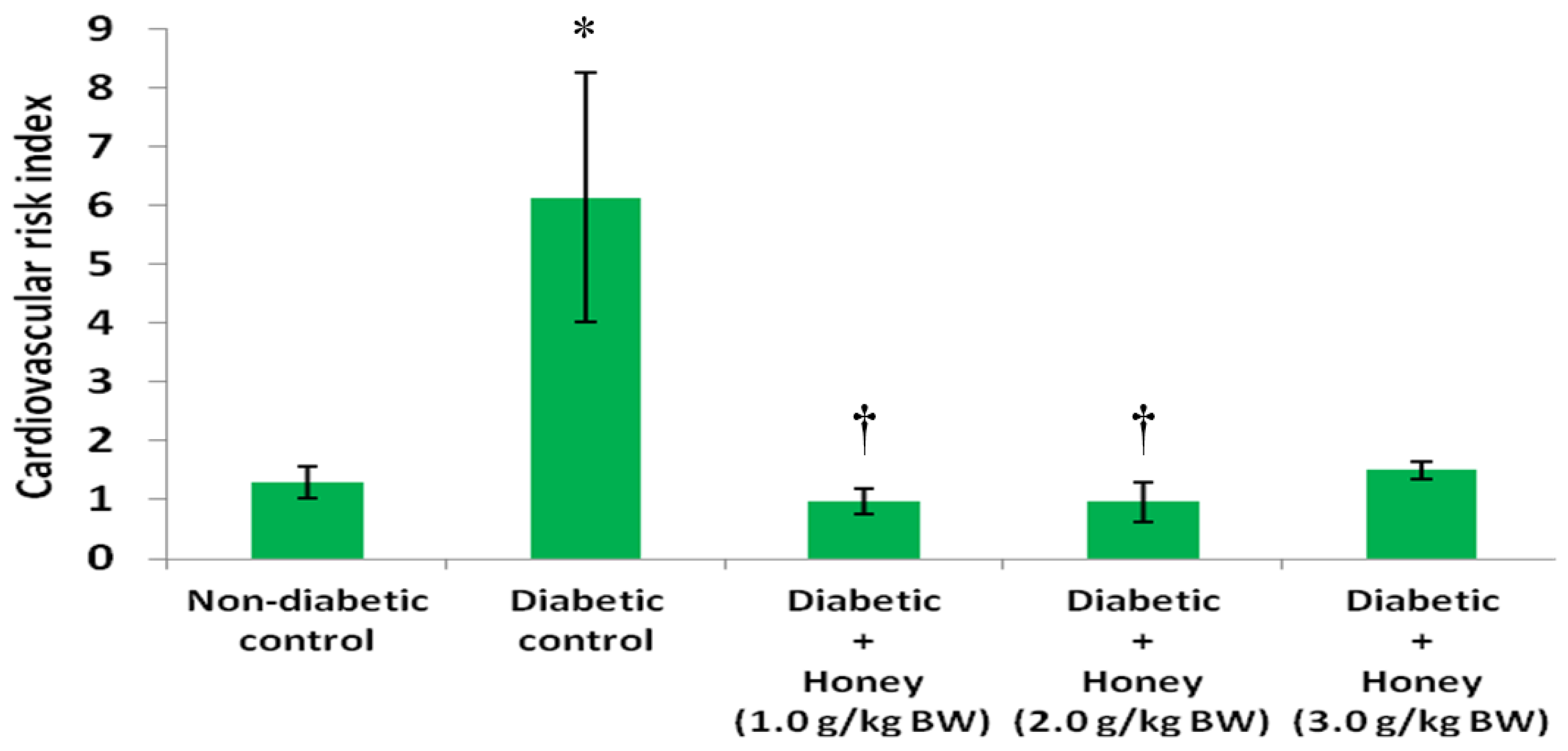
3.4. Effects of Honey on Coronary and Cardiovascular Risk Indices of Diabetic Rats
3.5. Effects of Honey on Total Cholesterol (TC), LDL Cholesterol and Atherogenic Index of Diabetic Rats
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CVD | cardiovascular disease |
| CHD | coronary heart disease |
| NAFDAC | National Agency for Food and Drug Administration Control |
| BW | body weight |
| BG | blood glucose |
| TC | total cholesterol |
| TGs | triglycerides |
| LDL | low density lipoprotein |
| VLDL | very low density lipoprotein |
| HDL | high density lipoprotein |
| Non-HDL | non-high density lipoprotein |
| AI | atherogenic index |
| CRI | coronary risk index |
| CVRI | cardiovascular risk index |
| SEM | standard error of mean |
| ANOVA | analysis of variance |
References
- Laing, S.P.; Swerdlow, A.J.; Slater, S.D.; Burden, A.C.; Morris, A.; Waugh, N.R.; Gatling, W.; Bingley, P.J.; Patterson, C.C. Mortality from heart disease in a cohort of 23,000 patients with insulin-treated diabetes. Diabetologia 2003, 46, 760–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Susanti, E.; Donosepoetro, M.; Patellongi, I.; Arif, M. Differences between several atherogenic parameters in patients with controlled and uncontrolled type 2 diabetes mellitus. Med. J. Indones. 2010, 19, 103–108. [Google Scholar] [CrossRef]
- Ballantyne, C.M. Treatment of dyslipidemia to reduce cardiovascular risk in patients with multiple risk factors. Clin. Cornerstone 2007, 8, S6–S13. [Google Scholar] [CrossRef]
- Williams, J.; Steers, W.N.; Ettner, S.L.; Mangione, C.M.; Duru, O.K. Cost-related nonadherence by medication type among medicare part D beneficiaries with diabetes. Med. Care 2013, 51, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Gupta, R.; Saraf, S.A. Herbs-are they safe enough? An overview. Crit. Rev. Food Sci. Nutr. 2012, 52, 876–898. [Google Scholar] [CrossRef] [PubMed]
- Crane, E. History of honey. In Honey, a Comprehensive Survey; Crane, E., Ed.; William Heinemann: London, UK, 1975; pp. 439–488. [Google Scholar]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S.; Sirajudeen, K.N.; Salleh, S.; Gurtu, S. Effects of Malaysian tualang honey supplementation on glycemia, free radical scavenging enzymes and markers of oxidative stress in kidneys of normal and streptozotocin-induced diabetic rats. Int. J. Cardiol. 2009, 137, S45. [Google Scholar] [CrossRef]
- Erejuwa, O.O.; Sulaiman, S.A.; Abdul Wahab, M.S. Honey: A novel antioxidant. Molecules 2012, 17, 4400–4423. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.T.; Rahman, R.A.; Gan, S.H.; Halim, A.S.; Hassan, S.A.; Sulaiman, S.A.; Kirnpal-Kaur, B. The antibacterial properties of Malaysian tualang honey against wound and enteric microorganisms in comparison to manuka honey. BMC Complement. Altern. Med. 2009, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gheldof, N.; Wang, X.H.; Engeseth, N.J. Identification and quantification of antioxidant components of honeys from various floral sources. J. Agric. Food Chem. 2002, 50, 5870–5877. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Q.X. Chemical composition, characterization, and differentiation of honey botanical and geographical origins. Adv. Food Nutr. Res. 2011, 62, 89–137. [Google Scholar] [PubMed]
- Erejuwa, O.O. Effect of honey in diabetes mellitus: Matters arising. J. Diabetes Metab. Disord. 2014, 13, 23. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, M.; Ataie-Jafari, A.; Hosseini, S.; Foruzanfar, M.H.; Rahmani, M.; Pajouhi, M. Effects of natural honey consumption in diabetic patients: An 8-week randomized clinical trial. Int. J. Food Sci. Nutr. 2009, 60, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O. The use of honey in diabetes mellitus: Is it beneficial or detrimental? Int. J. Endocrinol. Metab. 2012, 10, 444–445. [Google Scholar] [CrossRef]
- Bogdanov, S.; Jurendic, T.; Sieber, R.; Gallmann, P. Honey for nutrition and health: A review. J. Am. Coll. Nutr. 2008, 27, 677–689. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Health and Human Services, Public Health Service, National Institutes of Health. Guide for the Care and Use of Laboratory Animals; NIH Publication No. 85-23; National Institutes of Health: Bethesda, MD, USA, 1985.
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [PubMed]
- Abbott, R.D.; Wilson, P.W.; Kannel, W.B.; Castelli, W.P. High density lipoprotein cholesterol, total cholesterol screening and myocardial infarction. The Framingham Study. Arteriosclerosis 1988, 8, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Alladi, S.; Khada, A.; Shanmugan, M. Induction of hypercholesterolemia by simple soil protein with acetate generating amino acid. Nutr. Rep. Int. 1989, 40, 893–894. [Google Scholar]
- Erejuwa, O.O.; Gurtu, S.; Sulaiman, S.A.; Wahab, M.S.; Sirajudeen, K.N.; Salleh, M.S. Hypoglycemic and antioxidant effects of honey supplementation in streptozotocin-induced diabetic rats. Int. J. Vitam. Nutr. Res. 2010, 80, 74–82. [Google Scholar] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S.; Sirajudeen, K.N.; Salleh, M.S.; Gurtu, S. Glibenclamide or metformin combined with honey improves glycemic control in streptozotocin-induced diabetic rats. Int. J. Biol. Sci. 2011, 7, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Fasanmade, A.A.; Alabi, O.T. Differential effect of honey on selected variables in alloxan-induced and fructose-induced diabetic rats. Afr. J. Biomed. Res. 2008, 11, 191–196. [Google Scholar]
- Pamela, C.C.; Richard, A.H. Biochemistry, 2nd ed.; JP Lippincott: Philadelphia, PA, USA, 1994; pp. 248–251. [Google Scholar]
- Abdulrhman, M.M.; El-Hefnawy, M.H.; Aly, R.H.; Shatla, R.H.; Mamdouh, R.M.; Mahmoud, D.M.; Mohamed, W.S. Metabolic effects of honey in type 1 diabetes mellitus: A randomized crossover pilot study. J. Med. Food 2013, 16, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S. Honey—A novel antidiabetic agent. Int. J. Biol. Sci. 2012, 8, 913–934. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S. Oligosaccharides might contribute to the antidiabetic effect of honey: A review of the literature. Molecules 2011, 17, 248–266. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S. Fructose might contribute to the hypoglycemic effect of honey. Molecules 2012, 17, 1900–1915. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S. Effects of honey and its mechanisms of action on the development and progression of cancer. Molecules 2014, 19, 2497–2522. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S.; Sirajudeen, K.N.; Salleh, S.; Gurtu, S. Honey supplementation in spontaneously hypertensive rats elicits antihypertensive effect via amelioration of renal oxidative stress. Oxid. Med. Cell. Longev. 2012, 2012, 374037. [Google Scholar] [CrossRef] [PubMed]
- Kadir, E.A.; Sulaiman, S.A.; Yahya, N.K.; Othman, N.H. Inhibitory effects of tualang honey on experimental breast cancer in rats: A preliminary study. Asian Pac. J. Cancer Prev. 2013, 14, 2249–2254. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.; Sulaiman, S.A.; Jaafar, H.; Sirajudeen, K.N. Antioxidant protective effect of honey in cigarette smoke-induced testicular damage in rats. Int. J. Mol. Sci. 2011, 12, 5508–5521. [Google Scholar] [CrossRef] [PubMed]
- Nasrolahi, O.; Heidari, R.; Rahmani, F.; Farokhi, F. Effect of natural honey from ilam and metformin for improving glycemic control in streptozotocin-induced diabetic rats. Avicenna J. Phytomed. 2012, 2, 212–221. [Google Scholar] [PubMed]
- Zaid, S.S.; Sulaiman, S.A.; Sirajudeen, K.N.; Othman, N.H. The effects of tualang honey on female reproductive organs, tibia bone and hormonal profile in ovariectomised rats-animal model for menopause. BMC Complement. Altern. Med. 2011, 10, 82. [Google Scholar] [CrossRef] [PubMed]
- Vijan, S.; Hayward, R.A. Pharmacologic lipid-lowering therapy in type 2 diabetes mellitus: Background paper for the American college of physicians. Ann. Intern. Med. 2004, 140, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Ahmadvand, H.; Noori, A.; Dehnoo, M.G.; Bagheri, S.; Cheraghi, R.A. Hypoglycemic, hypolipidemic and antiatherogenic effects of oleuropein in alloxan-induced type 1 diabetic rats. Asian Pac. J. Trop. Dis. 2014, 4, S421–S425. [Google Scholar] [CrossRef]
- Ikewuchi, C.C. Effect of aqueous extract of sansevieria senegambica baker on plasma chemistry, lipid profile and atherogenic indices of alloxan-treated rats: Implications for the management of cardiovascular complications in diabetes mellitus. Pac. J. Sci. Technol. 2010, 11, 524–531. [Google Scholar]
- Szkudelski, T. The mechanism of alloxan and streptozotocin action in beta cells of the rat pancreas. Physiol. Res. 2001, 50, 537–546. [Google Scholar] [PubMed]
- Zheng, C.; Furtado, J.; Khoo, C. Apolipoprotein C-III and the metabolic basis for hypertriglyceridemia and the dense low-density lipoprotein phenotype. Circulation 2010, 121, 1722–1734. [Google Scholar] [CrossRef] [PubMed]
- Klop, B.; Elte, J.W.F.; Cabezas, C.M. Dyslipidemia in obesity: Mechanisms and potential targets. Nutrients 2013, 5, 1218–1240. [Google Scholar] [CrossRef] [PubMed]
- Winocour, P.H.; Durrington, P.N.; Bhatnagar, D.; Ishola, M.; Arrol, S.; Mackness, M. Abnormalities of VLDL, IDL, and LDL characterize insulin-dependent diabetes mellitus. Arterioscler. Thromb. 1992, 12, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Keevil, J.G.; Cullen, M.W.; Gangnon, R.; McBride, P.E.; Stein, J.H. Implications of cardiac risk and low-density lipoprotein cholesterol distributions in the United States for the diagnosis and treatment of dyslipidemia: Data from national health and nutrition examination survey 1999 to 2002. Circulation 2007, 115, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Katsilambros, N.L.; Philippides, P.; Touliatou, A. Metabolic effects of honey (alone or combined with other foods) in type II diabetics. Acta Diabetol. Lat. 1988, 25, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Bos, G.; Dekker, J.M.; Nijpels, G.; de Vegt, F.; Diamant, M.; Stehouwer, C.D.; Bouter, L.M.; Heine, R.J.; Hoorn, S. A combination of high concentrations of serum triglyceride and non-high-density-lipoprotein-cholesterol is a risk factor for cardiovascular disease in subjects with abnormal glucose metabolism—The hoorn study. Diabetologia 2003, 46, 910–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasevic, D.; Frohlich, J.; Mancini, G.B.; Lear, S.A. Clinical usefulness of lipid ratios to identify men and women with metabolic syndrome: A cross-sectional study. Lipids Health Dis. 2014, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Ingelsson, E.; Schaefer, E.; Contois, J.H.; McNamara, J.R.; Sullivan, L.; Keyes, M.J.; Pencina, M.J.; Schoonmaker, C.; Wilson, P.W.F.; D’Agostino, R.B.; et al. Clinical utility of different lipid measures for prediction of coronary heart disease in men and women. JAMA 2007, 298, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Salazar, M.R.; Carbajal, H.A.; Espeche, W.G.; Aizpurua, M.; Sisnieguez, C.E.; March, C.E.; Balbin, E.; Stavile, R.N.; Reaven, G.M. Identifying cardiovascular disease risk and outcome: Use of the plasma triglyceride/high-density lipoprotein cholesterol concentration ratio versus metabolic syndrome criteria. J. Intern. Med. 2013, 273, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Vega, G.L.; Barlow, C.E.; Grundy, S.M.; Leonard, D.; DeFina, L.F. Triglyceride-to high-density-lipoprotein-cholesterol ratio is an index of heart disease mortality and of incidence of type 2 diabetes mellitus in men. J. Investig. Med. 2014, 62, 345–349. [Google Scholar] [PubMed]
- Azmi, M.B.; Qureshi, S.A. Methanolic root extract of rauwolfia serpentina benth improves the glycemic, antiatherogenic, and cardioprotective indices in alloxan-induced diabetic mice. Adv. Pharm. Sci. 2012, 376429. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Berneis, K. Low-density lipoprotein size and cardiovascular risk assessment. QJM 2006, 99, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Brahm, A.; Hegele, R.A. Hypertriglyceridemia. Nutrients 2013, 5, 981–1001. [Google Scholar] [CrossRef] [PubMed]
- Al-Waili, N.S. Natural honey lowers plasma glucose, C-reactive protein, homocysteine, and blood lipids in healthy, diabetic, and hyperlipidemic subjects: Comparison with dextrose and sucrose. J. Med. Food 2004, 7, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S.; Salam, S.K.; Salleh, M.S.; Gurtu, S. Comparison of antioxidant effects of honey, glibenclamide, metformin, and their combinations in the kidneys of streptozotocin-induced diabetic rats. Int. J. Mol. Sci. 2011, 12, 829–843. [Google Scholar] [CrossRef] [PubMed]
- Erejuwa, O.O.; Sulaiman, S.A.; Wahab, M.S.; Sirajudeen, K.N.; Salleh, M.S.; Gurtu, S. Antioxidant protection of Malaysian tualang honey in pancreas of normal and streptozotocin-induced diabetic rats. Ann. Endocrinol. 2010, 71, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Ihara, Y.; Toyokuni, S.; Uchida, K.; Odaka, H.; Tanaka, T.; Ikeda, H.; Hiai, H.; Seino, Y.; Yamada, Y. Hyperglycemia causes oxidative stress in pancreatic-cells of GK rats, a model of type 2 diabetes. Diabetes 1999, 48, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Ebbert, J.O.; Jensen, M.D. Fat depots, free fatty acids, and dyslipidemia. Nutrients 2013, 5, 498–508. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | TC (mg/dL) | LDL Cholesterol (mg/dL) | Atherogenic Index |
|---|---|---|---|
| Non-diabetic control | 54.3 ± 2.4 | 8.0 ± 3.7 | 0.2 ± 0.1 |
| Diabetic control | 86.7 ± 18.1 | 23.2 ± 13.0 | 1.1 ± 0.7 |
| Diabetic + Honey (1.0 g/kg BW) | 52.6 ± 5.4 | 7.9 ± 2.9 | 0.2 ± 0.1 |
| Diabetic + Honey (2.0 g/kg BW) | 61.6 ± 5.6 | 4.4 ± 2.8 | 0.1 ± 0.1 |
| Diabetic + Honey (3.0 g/kg BW) | 49.4 ± 3.0 | 21.6 ± 7.5 | 1.0 ± 0.6 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erejuwa, O.O.; Nwobodo, N.N.; Akpan, J.L.; Okorie, U.A.; Ezeonu, C.T.; Ezeokpo, B.C.; Nwadike, K.I.; Erhiano, E.; Abdul Wahab, M.S.; Sulaiman, S.A. Nigerian Honey Ameliorates Hyperglycemia and Dyslipidemia in Alloxan-Induced Diabetic Rats. Nutrients 2016, 8, 95. https://doi.org/10.3390/nu8030095
Erejuwa OO, Nwobodo NN, Akpan JL, Okorie UA, Ezeonu CT, Ezeokpo BC, Nwadike KI, Erhiano E, Abdul Wahab MS, Sulaiman SA. Nigerian Honey Ameliorates Hyperglycemia and Dyslipidemia in Alloxan-Induced Diabetic Rats. Nutrients. 2016; 8(3):95. https://doi.org/10.3390/nu8030095
Chicago/Turabian StyleErejuwa, Omotayo O., Ndubuisi N. Nwobodo, Joseph L. Akpan, Ugochi A. Okorie, Chinonyelum T. Ezeonu, Basil C. Ezeokpo, Kenneth I. Nwadike, Erhirhie Erhiano, Mohd S. Abdul Wahab, and Siti A. Sulaiman. 2016. "Nigerian Honey Ameliorates Hyperglycemia and Dyslipidemia in Alloxan-Induced Diabetic Rats" Nutrients 8, no. 3: 95. https://doi.org/10.3390/nu8030095