A Pre and Post Survey to Determine Effectiveness of a Dietitian-Based Nutrition Education Strategy on Fruit and Vegetable Intake and Energy Intake among Adults

Abstract
:
1. Introduction
- To assess fruit and vegetable intake, energy intake, physical activity level, body mass index (BMI), nutrition knowledge and attitudes of adults before and after a nutrition education.
- To determine factors associated with nutrition knowledge.
- To evaluate the efficacy of the nutrition education strategy.
2. Materials and Methods
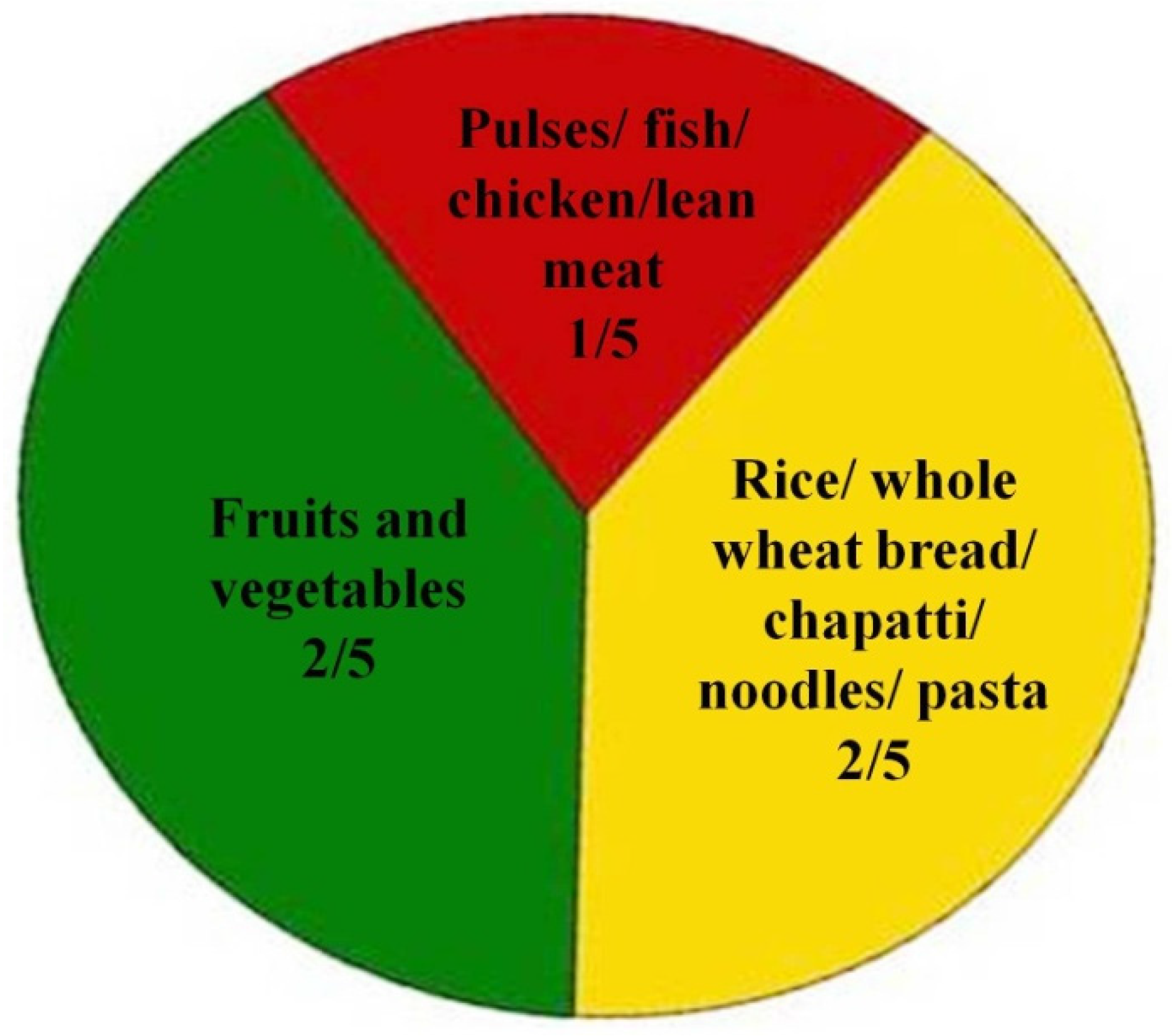
2.1. Nutrition Education Strategy
2.2. Ethical Approval
2.3. Statistical Analysis
3. Results
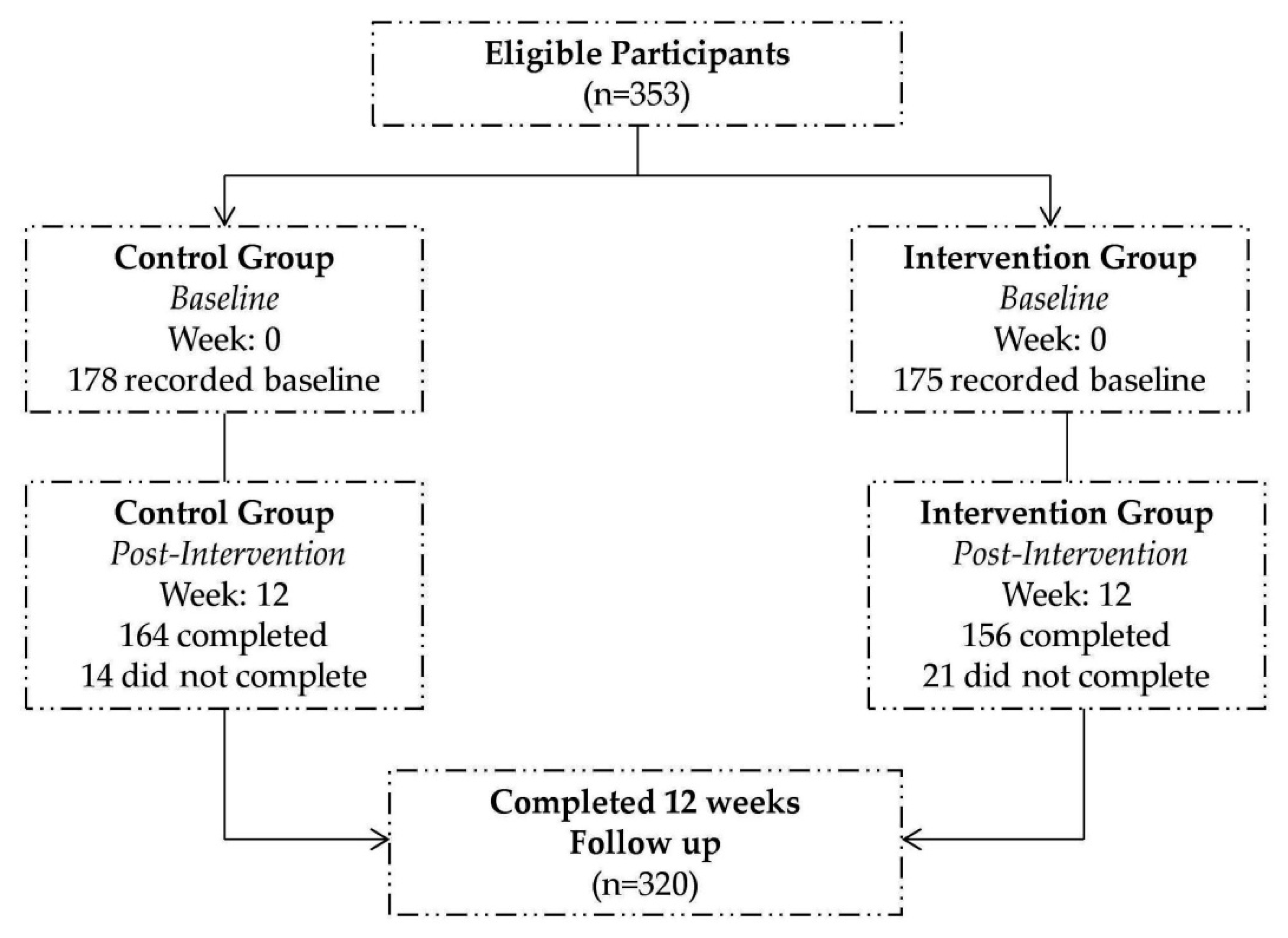
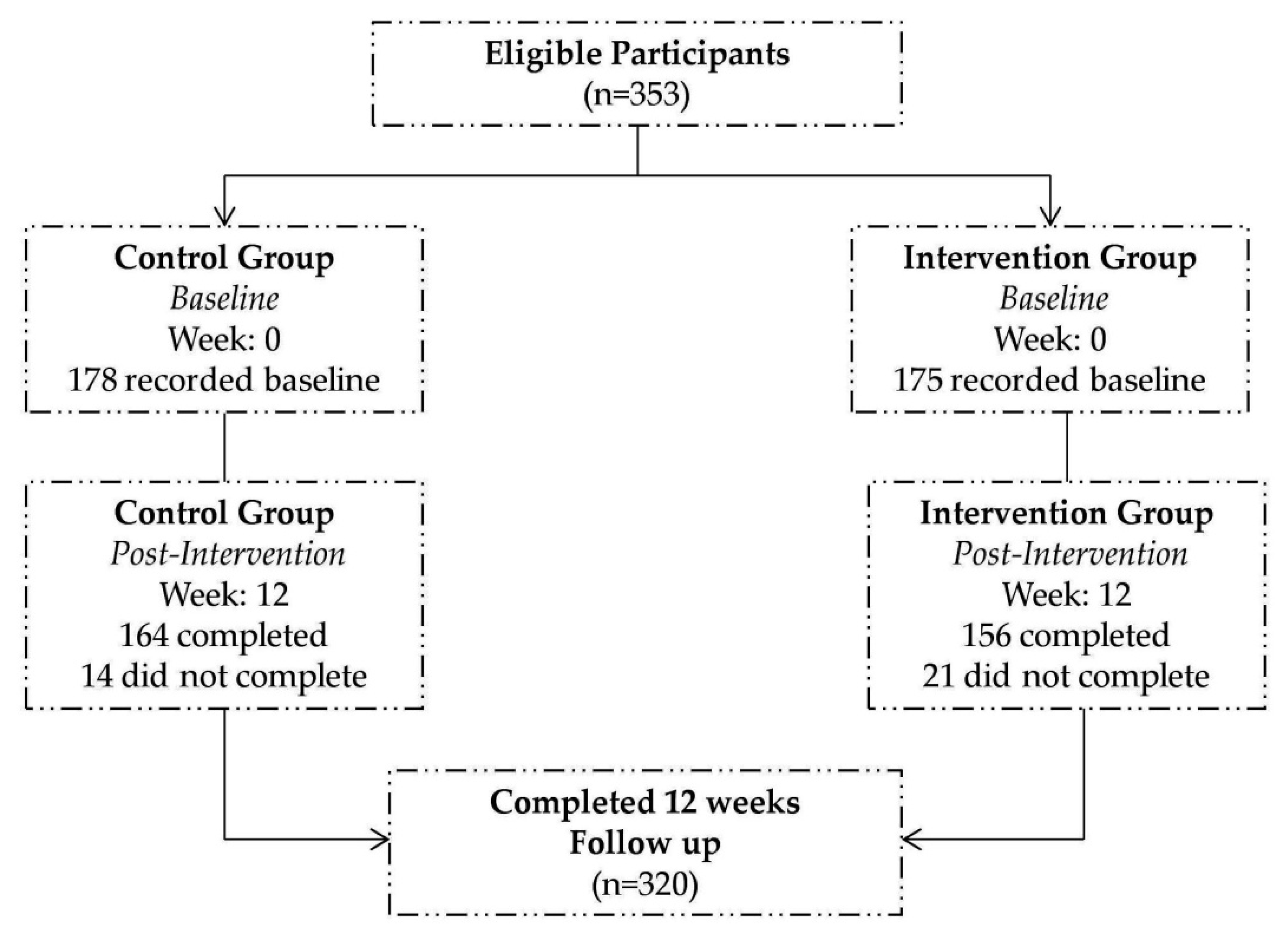
3.1. Participants’ Profiles
3.2. Intervention and Control Group at Baseline
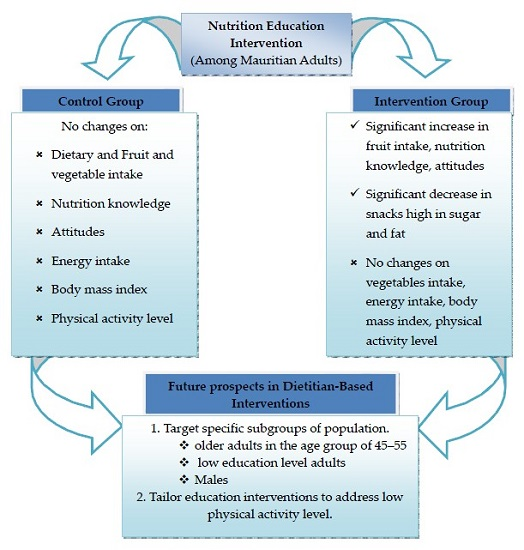
3.3. Post Intervention Changes
3.4. Opinions, Barriers and Motivators of the Nutrition Education Strategy
4. Discussion
4.1. Changes in Dietary Intake
4.2. Mean Energy Intake and BMI
4.3. Mean Nutritional Knowledge (NK)
4.4. Attitudes towards Healthier Eating
4.5. Barriers and Motivators to Nutrition Education Strategy
5. Limitations of the Study
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ministry of Health and Quality of Life. National Plan of Action for Nutrition 2009–2010. Available online: http://health.govmu.org/English/Documents/nut1-8.pdf (accessed on 17 August 2015).
- World Health Organisation. Country Corporation Strategy at a Glance, Mauritius. Available online: http://www.who.int/countryfocus/cooperation_strategy/ccsbrief_mus_en.pdf (accessed on 17 August 2015).
- Ministry of Health and Quality of Life. The Trends in Diabetes and Cardiovascular Disease Risk in Mauritius. The Mauritius Non Communicable Diseases Survey 2015. Available online: http://health.govmu.org/English/Statistics/Documents/Mauritius%20NCD%20Survey%202015%20Report.pdf (accessed on 17 January 2016).
- Ministry of Health and Quality of Life. Mauritius Salt Intake Study 2012. Available online: http://ncd.health.govmu.org/English/NCD%20Mobile%20Service/Documents/Mauritius%20Salt%20Intake%20Study%202012.pdf (accessed on 17 August 2015).
- Kimmons, J.; Gillespie, C.; Seymour, J.; Serdula, M.D.; Blanck, H.M. Fruit and vegetable intake among adolescents and adults in the United States: Percentage meeting individualized recommendations. Medscape J. Med. 2009, 11, 26. [Google Scholar]
- Ledikwe, J.H.; Blanck, H.M.; Kettel, K.L.; Khan, L.K.; Serdula, M.K.; Seymour, J.D.; Tohill, B.C.; Rolls, B.J. Dietary energy density is associated with energy intake and weight status in US adults. Am. J. Clin. Nutr. 2006, 83, 1362–1368. [Google Scholar] [PubMed]
- Joint FAO/WHO Workshop on Fruit and Vegetables for Health (2004: Kobe, Japan); World Health Organization; Deptartment of Chronic Diseases and Health Promotion. Fruit and Vegetable for Health; Report of a Joint FAO/WHO Workshop: Kobe, Japan; 1–3 September 2004. Available online: http://apps.who.int/iris/handle/10665/43143 (accessed on 17 August 2015).
- Li, Y.; Li, D.; Ma, C.Y.; Liu, C.Y.; Ding, H.; Wen, Z.M.; Peng, L.P. Consumption of and factors influencing consumption of, fruit and vegetables among elderly Chinese people. Nutrients 2012, 28, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Izzah, N.A.; Aminah, A.; Pauzi, M.A.; Lee, Y.H.; Wan, R.W.M.; Fatimah, D.S. Patterns of fruits and vegetable consumption among adults of different ethnics in Selangor, Malaysia. Int. Food Res. J. 2012, 19, 1095–1107. [Google Scholar]
- Garriguet, D. Nutrition: Findings from the Canadian Community Health Survey. Overview of Canadians’ Eating Habits. Available online: http://publications.gc.ca/Collection/Statcan/82-620-M/82-620- MIE2006002.pdf (accessed on 20 August 2015).
- Food and Agriculture Organization of the United Nations. Promotion of Fruit and Vegetables for Health: African Regional Workshop. Available online: http://www.fao.org/fileadmin/templates/agphome/documents/horticulture/WHO/arusha/PROFAV_2011_programme.pdf (accessed on 17 January 2015).
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Ganry, J. Current status of fruits and vegetables production and consumption in Francophone African countries—Potential impact on health. Acta Hort. 2009, 841, 249–256. [Google Scholar] [CrossRef]
- Comprehensive Africa Agriculture Development Programme (CAADP). CAADP Nutrition Capacity Development Workshop for the Southern Africa Region Nutrition Country Paper—Mauritius. Available online: http://www.fao.org/fileadmin/user_upload/wa_workshop/country-paper/Mauritius_NCP.pdf (accessed on 15 August 2015).
- Coulter, A.; Parsons, S.; Askham, J. Where Are the Patients in Decision-Making about Their Own Care? World Health Organization 2008 and World Health Organization, on Behalf of the European Observatory on Health Systems and Policies 2008. Available online: http://www.who.int/management/general/decisionmaking/WhereArePatientsinDecisionMaking.pdf (accessed on 15 August 2015).
- Hosmer, C.; Dwyer, J.T.; Villarroel, A. Training Needs for Nutrition Education: Guidelines for In-Service Training of Nutrition Educators. Food and Agriculture Organisation. Available online: http://www.fao.org/docrep/w3733e/w3733e05.htm (accessed on 22 August 2015).
- Abela, J. Adult learning theories and medical education: A review. Malta Med. J. 2009, 21, 11–18. [Google Scholar]
- Braeckman, L.; Bacquer, D.D.; Maes, L.; de Backer, G. Effects of a low-intensity worksite-based nutrition intervention. J. Occup. Med. Toxicol. 1999, 49, 549–555. [Google Scholar] [CrossRef]
- Hendrix, S.J.; Fischer, J.G.; Reddy, R.D.; Lommel, T.S.; Speer, E.M.; Stephens, H.; Park, S.; Johnson, M.A. Fruit and vegetable intake and knowledge increased following a community-based intervention in older adults in Georgia senior centers. J. Nutr. Elder. 2008, 27, 155–178. [Google Scholar] [CrossRef] [PubMed]
- Lowe, M.R.; Tappe, A.K.; Butryn, M.L.; Annunziato, R.A.; Coletta, M.C.; Ochner, C.N.; Rolls, B.J. An intervention study targeting energy and nutrient intake in worksite cafeterias. J. Eat Behav. 2010, 11, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.L.; Sheriff, J.L.; Dhaliwal, S.S.; Mamo, J.C.L. Tailored, iterative, printed dietary feedback is as effective as group education in improving dietary behaviours: Results from a randomised control trial in middle-aged adults with cardiovascular risk factors. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Amy, B.J.; George, G.; Pradhan, V. Cost-benefit analysis conducted for nutrition education in California. Calif. Agric. 2006, 60, 185–191. [Google Scholar]
- Booth, A.; Nowson, C.; Worsley, A.; Margerison, C.; Jorna, M. Dietary approaches for weight loss with increased intakes of fruit, vegetables and dairy products. Nutr. Diet. 2008, 65, 115–120. [Google Scholar] [CrossRef]
- Chapman, J.; Armitage, C.J. Do techniques that increase fruit intake also increase vegetable intake? Evidence from a comparison of two implementation intention interventions. Appetite 2012, 58, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Gans, K.M.; Risica, P.M.; Strolla, L.O.; Fournier, L.; Kirtania, U.; Upequi, D.; Zhao, J.; George, T.; Acgaryya, S. Effectiveness of different methods for delivering tailored nutrition education to low income, ethnically diverse adults. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.; Flaherty, S.J.; Jenner, D.; Davies, C.; Ells, L. A Review and Needs Assessment of Local Level Diet and Nutrition Data, EMPHO, United Kingdom. Available online: www.healthyweight4children.org.uk/resource/view.aspx?RID=60116 (accessed on 31 July 2014).
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey, 2003–2004 Data Documentation, Codebook, and Frequencies. Available online: http://www.cdc.gov/nchs/nhanes/nhanes2003-2004/FFQDC_C.htm#Component_Description (accessed on 18 August 2015).
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. Eur. J. Clin. Nutr. 1999, 53, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Galobardes, B.; Morabia, A. Measuring the habitat as an indicator of socioeconomic position: Methodology and its association with hypertension. J. Epidemiol. Community Health 2003, 57, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Agency. Attitudes and Behaviours towards Healthy Eating and Food Safety: A Scoping Study. Available online: http://www.food.gov.uk/sites/default/files/multimedia/pdfs/foodandyouscoping.pdf (accessed on 27 August 2015).
- Global Physical Activity Questionnaire Analysis Guide. Available online: http://www.who.int/chp/steps/resources/GPAQ_Analysis_Guide.pdf (accessed on 16 October 2014).
- Epic-Norfolk: Nutritional Methods (2014). University of Cambridge. Available online: http://www.srl.cam.ac.uk/epic/nutmethod/24hr.shtml (accessed on 17 August 2014).
- Lukmanji, Z.; Hertzmark, E.; Mlingi, N.; Mlingi, N.; Assey, V.; Ndossi, G.; Fawzi, W. Tanzania Food Composition Table; MUHAS-TFNC, HSPH: Dares Sallam, Tanzania, 2008. [Google Scholar]
- World Health Organisation. Obesity and Overweight. Fact Sheet No. 311. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 14 October 2014).
- Liu, N.; Mao, L.; Sun, X.; Liu, L.; Yao, P.; Chen, B. The effect of health and nutrition education intervention on women’s postpartum beliefs and practices: A randomized controlled trial. BMC Public Health 2009, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Finance & Economic Development. Statistics Mauritius 2015. Producer Price Index Agriculture—4th Quarter 2014. 2015. Available online: http://statsmauritius.govmu.org/English/Publications/Pages/ppia4thyr14.aspx (accessed on 26 October 2014). [Google Scholar]
- Luximon, Y.; Nowbuth, M.D. As status of food security in Mauritius in face of climate change. J. Eur. Water 2010, 32, 3–14. [Google Scholar]
- Ministry of Agro Industry and Fisheries. Strategic Options in Crop Diversification and Livestock Sector (2007–2015). 2007. Available online: http://www.areu.mu/files/pub/areunssp.pdf (accessed on 15 August 2015).
- Emanuel, A.S.; McCully, S.N.; Gallangher, K.M.; Updegraff, J.A. Theory of planned behavior explains gender difference in fruit and vegetable consumption. Appetite 2012, 59, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Arganini, C.; Saba, A.; Comitato, R.; Virgili, F.; Turrini, A. Gender Differences in Food Choice and Dietary Intake in Modern Western Societies. In Public Health—Social and Behavioral Health, 3rd ed.; Maddock, J., Ed.; In Tech Europe: Rijeka, Croatia; pp. 83–102. Available online: http://cdn.intechopen.com/pdfs-wm/36935.pdf (accessed on 28 August 2015).
- Chambers, S.; Lobb, A.; Butler, L.T.; Trail, W.B. The influence of age and gender on food choice: A focus group exploration. Int. J. Consumer Stud. 2008, 32, 356–365. [Google Scholar] [CrossRef]
- Knudsen, V.K.; Mathiessen, J.; Biltoft-Jensen, A.; Sorensen, M.R.; Groth, M.V.; Trolle, E.; Christensen, T.; Faqt, S. Identifying dietary patterns and associated health-related lifestyle factors in the adult Danish population. Eur. J. Clin. Nutr. 2014, 68, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Organization for Economic Cooperation and Development. Fruit and Vegetable Consumption among Adults. Health at a Glance 2013: OECD Indicators. Available online: http://dx.doi.org/10.1787/health_glance-2013–22-en (accessed on 17 August 2015).
- Simunaniemi, A.M.; Andersson, A.; Nydahl, M. Fruit and vegetable consumption close to recommendations. A partly web-based nationwide dietary survey in Swedish adults. Food Nutr. Res. 2009, 53, 10. [Google Scholar] [CrossRef] [PubMed]
- Webber, K.H.; Lee, E. The diet quality of adult women participating in a behavioural weight-loss programme. J. Hum. Nutr. Diet. 2011, 24, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Lhakhang, P.; Godinho, C.; Knoll, N.; Schwarzer, R. A brief intervention increases fruit and vegetable intake. A comparison of two intervention sequences. Appetite 2014, 82, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Kothe, E.J.; Mullan, B.A. Perceptions of fruit and vegetable dietary guidelines among Australian young adults. J. Nutr. Diet. 2011, 68, 262–266. [Google Scholar] [CrossRef]
- De Silva-Sanigorski, A.M.; Bell, A.C.; Kremer, P.; Nichols, M.; Crellin, M.; Smith, M.; Sharp, S.; de Groot, F.; Carpenter, L.; Boak, R.; et al. Reducing obesity in early childhood: Results from Romp & Chomp, an Australian community-wide intervention program. Am. J. Clin. Nutr. 2010, 91, 831–840. [Google Scholar] [PubMed]
- James, D.C.; Pobee, J.; Oxidine, D.; Brown, L.; Joshi, G. Using the health belief model to develop culturally appropriate weight-management materials for African-American women. J. Acad. Nutr. Diet. 2012, 112, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Rangan, A.M.; Schindeler, S.; Hector, D.J.; Gill, T.P. Assessment of typical food portion sizes consumed among Australian adults. Nutr. Diet. 2009, 66, 227–233. [Google Scholar] [CrossRef]
- Garduno-Diaz, S.D.; Khokhar, S. Eating habits and nutrient intake of migrant South Asians in the UK. J. Public Health 2014, 128, 1043–1046. [Google Scholar] [CrossRef] [PubMed]
- Kazoka, D.; Vetra, J. Relationship between age at menarche and adult body mass index. Pap. Anthropol. XVI 2007, 16, 170–179. [Google Scholar]
- Cooke, R.; Papadaki, A. Nutrition label use mediates the positive relationship between nutrition knowledge and attitudes towards healthy eating with dietary quality among university students in the UK. Appetite 2014, 83, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A.; Gearon, E.; Backholer, K.; Carstensen, B. Trends in the skewness of the body mass index distribution among urban Australian adults, 1980 to 2007. Ann. Epidemiol. 2015, 25, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Kriaucioniene, V.; Petkeviciene, J.; Klumbiene, J.; Sakyte, E.; Raskiliene, A. The prevalence and trends of overweight and obesity among Lithuanian adults, 1994–2012. J. Public Health 2014, 128, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Penman, A.D.; Johnson, W.D. The changing shape of the body mass index distribution curve in the population: Implications for public health policy to reduce the prevalence of adult obesity. Prev. Chronic Dis. 2006, 3, A74. [Google Scholar] [PubMed]
- Du, T.; Sun, X.; Yin, P.; Huo, R.; Ni, C.; Yu, X. Increasing trends in central obesity among Chinese adults with normal body mass index, 1993–2009. BMC Public Health 2013, 13, 327. [Google Scholar] [CrossRef] [PubMed]
- Nooritajer, M. The effect of education on physical activity style and body mass index on employed women in Iran University of Medical Sciences. World Appl. Sci. J. 2010, 9, 619–623. [Google Scholar]
- Sharma, S.V.; Gernand, A.D.; Day, R.S. Nutrition knowledge predicts eating behavior of all food groups except fruits and vegetables among adults in the Paso del Norte region: Qué Sabrosa Vida. J. Nutr. Educ. Behav. 2008, 40, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Dunneram, Y.; Jeewon, R. A scientific assessment of socio-demographic factors, physical activity level, and nutritional knowledge as determinants of dietary quality among Indo-Mauritian women. J. Nutr. Met. 2013, 9. [Google Scholar] [CrossRef]
- Rezaee, A.G.; Azizi, M.; Hoseini, R. A comparison of nutritional knowledge and food habits of physical education and non-physical education college students. J. Appl. Sci. 2012, 20, 1277–1282. [Google Scholar]
- De Vriendt, T.; Matthys, C.; Verbeke, W.; Pynaert, I.; de Henauw, S. Determinants of nutrition knowledge in young and middle-aged Belgian women and the association with their dietary behaviour. Appetite 2009, 52, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Zidenberg-Cherr, S. Exploring nutrition education resources and barriers, and nutrition knowledge in teachers in California. J. Nutr. Educ. Behav. 2014, 47, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, K.; van den Broucke, S.; Fullam, J. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Parmenter, K.; Waller, J. Nutrition knowledge and food intake. Appetite 2000, 34, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Wan-Lee, Y. Nutrition knowledge, attitudes, and dietary restriction behavior of the Taiwanese elderly. Asia Pac. J. Clin. Nutr. 2005, 14, 221–229. [Google Scholar] [PubMed]
- Allan, J.; Johnston, M.; Campbell, N. Why do people fail to turn good intentions into action? The role of executive control processes in the translation of healthy eating intentions into action in young Scottish adults. BMC Public Health 2008, 18, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearney, J.M.; Gibney, M.J.; Livingstone, B.E.; Robson, P.J.; Kiely, M.; Harrington, K. Attitudes towards and beliefs about nutrition and health among a random sample of adults in the Republic of Ireland and Northern Ireland. Public Health Nutr. 2001, 4, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Raats, M.M.; Sparks, P. Unrealistic optimism about diet-related risks: Implications for interventions. Proc. Nutr. Soc. 1995, 54, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Love, P.; Maunder, E.M.W.; Green, J.M. Are South African women willing and able to apply the new food-based dietary guidelines? Lessons for nutrition educators. Afr. J. Clin. Nutr. 2008, 21, 17–24. [Google Scholar]
- Seguin, R.; Connor, L.; Nelson, M.; LaCroix, A.; Eldrige, G. Understanding barriers and facilitators to healthy eating and active living in rural communities. Nutr. Met. 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fila, S.A.; Smith, C. Applying the theory of planned behavior to healthy eating behaviors in urban native American youth. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 11. [Google Scholar] [CrossRef] [PubMed]
- Eertmans, A.; Baeyen, F.; van den Bergh, O. Food likes and their relative importance in human eating behaviour: Review and preliminary suggestions for health promotion. Health Educ. Res. 2001, 16, 443–456. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Frequency | Score |
|---|---|
| Never or less than once per month | 0 |
| Monthly | 0.033 |
| Twice per month | 0.08 |
| Once per week | 0.14 |
| 2–3 times per week | 0.5 |
| Once daily | 1 |
| 2–3 times daily | 2 |
| Characteristics | Categories | * CG (n = 178) % | ** IG (n = 175) % |
|---|---|---|---|
| Age (years) | 19–25 | 16.1 | 16.0 |
| 25–45 | 66.1 | 66.3 | |
| 45–55 | 17.8 | 17.0 | |
| Gender | Male | 25.8 | 28.6 |
| Female | 74.2 | 71.4 | |
| Marital Status | Single | 20.2 | 28.6 |
| Married | 73.0 | 68.5 | |
| Separated | 1.1 | 0 | |
| Divorced | 2.2 | 0.6 | |
| Widowed | 3.4 | 2.3 | |
| Employment Status | Full time employed | 12.9 | 19.0 |
| Part time employed | 3.4 | 4.0 | |
| Self employed | 2.2 | 2.9 | |
| Unemployed | 78.8 | 72.0 | |
| Retired | 1.7 | 2.0 | |
| Education Level | Low | 7.5 | 7.4 |
| Medium | 46.6 | 45.7 | |
| High | 48.9 | 46.9 | |
| Total Household income | Low | 28.1 | 26.3 |
| Moderate | 57.3 | 56.2 | |
| high | 14.6 | 17.5 |
| Independent Variables | Mean ± SD | Std. Error of Mean | p Value | |
|---|---|---|---|---|
| Gender | Male | 6.32 ± 3.43 | 0.35 | 0.022 *,a |
| Female | 7.27 ± 3.49 | 0.22 | ||
| Age (years) | 19–25 | 6.92 ± 3.76 | 0.32 | 0.744 |
| 25–45 | 6.94 ± 3.38 | 0.30 | ||
| 45–55 | 7.25 ± 3.27 | 0.34 | ||
| Income Level | Low | 6.69 ± 3.61 | 0.36 | 0.534 |
| Moderate | 7.32 ± 3.45 | 0.40 | ||
| High | 7.10 ± 3.45 | 0.26 | ||
| Education Level | Low | 7.38 ± 4.11 | 0.90 | 0.272 |
| high | 6.73 ± 3.50 | 0.25 | ||
| Medium | 7.33 ± 3.39 | 0.28 | ||
| Nutrition Knowledge | Insufficient | 6.42 ± 3.73 | 1.03 | 0.792 |
| Good | 6.96 ± 3.62 | 0.34 | ||
| Quite Good | 7.07 ± 3.43 | 0.23 | ||
| Physical Activity Level | Low | 6.59 ± 3.39 | 0.25 | 0.051 |
| Moderate | 7.61 ± 3.73 | 0.36 | ||
| High | 7.18 ± 3.27 | 0.41 | ||
| Body Mass Index (BMI) | Underweight | 6.41 ± 3.21 | 0.50 | 0.424 |
| Overweight | 6.72 ± 3.48 | 0.39 | ||
| Normal | 7.17 ± 3.39 | 0.24 | ||
| Obese | 7.45 ± 4.25 | 0.68 | ||
| Access to Food Commodities | Easy | 7.02 ± 3.59 | 0.42 | 0.761 |
| Difficult | 6.83 ± 2.29 | 0.20 | ||
| Parameters | Categories | Mean ± SD | Std. Error of Mean | p Value |
|---|---|---|---|---|
| Age (years) | 19–25 | 2.42 ± 0.50 | 0.04 | 0.000 *,a |
| 25–45 | 2.29 ± 0.54 | 0.05 | ||
| 45–55 | 2.06 ± 0.49 | 0.05 | ||
| Gender | Male | 2.38 ± 0.55 | 0.06 | 0.039 *,b |
| Female | 2.25 ± 0.51 | 0.03 | ||
| Income Level | Low | 2.26 ± 0.54 | 0.05 | 0.311 |
| Moderate | 2.32 ± 0.50 | 0.04 | ||
| high | 2.21 ± 0.56 | 0.06 | ||
| Education Level | Low | 2.05 ± 0.38 | 0.08 | 0.000 *,a |
| Medium | 2.15 ± 0.52 | 0.04 | ||
| high | 2.40 ± 0.51 | 0.04 |
| Food Group Intakes | Mean ± SE | Adj. Mean a 95% CI | Adj. Mean Dif b (95% CI) | F-stat (df) | p Value a | |
|---|---|---|---|---|---|---|
| Baseline | After 12 Weeks | |||||
| Carbohydrates (Grains and tubers) | 0.17 (−0.79, 0.45) | 1.58 (11, 309) | 0.600 | |||
| Intervention | 3.84 ± 0.11 | 3.93 ± 1.87 | 3.74 (3.12, 4.14) | |||
| Control | 3.60 ± 0.11 | 3.61 ± 1.49 | 3.62 (3.09, 3.82) | |||
| Beans/Pulses | 0.001 (0.16, 0.17) | 1.39 (11, 309) | 0.990 | |||
| Intervention | 0.64 ± 0.39 | 0.67 ± 0.47 | 0.63 (0.7, 0.72) | |||
| Control | 0.64 ± 0.39 | 0.60 ± 0.46 | 0.64 (0.48, 0.71) | |||
| Meat and eggs | 0.14 (−0.40, 0.11) | 0.92 (11, 309) | 0.272 | |||
| Intervention | 0.95 ± 0.06 | 0.84 ± 0.86 | 0.98 (0.55, 1.03) | |||
| Control | 0.61 ± 0.56 | 0.59 ± 0.50 | 0.60 (0.53, 0.78) | |||
| Seafood | 0.15 (−0.34, 0.05) | 1.53 (11, 309) | 0.133 | |||
| Intervention | 0.52 ± 0.04 | 0.53 ± 0.63 | 0.52 (0.34, 0.68) | |||
| Control | 0.36 ± 0.40 | 0.35 ± 0.37 | 0.36 (0.26, 0.44) | |||
| Soybeans and products | 0.06 (−0.17, 0.29) | 2.59 (11, 309) | 0.590 | |||
| Intervention | 0.22 ± 0.47 | 0.23 ± 0.50 | 0.22 (0.05, 0.33) | |||
| Control | 0.26 ± 0.05 | 0.26 ± 0.74 | 0.26 (0.07, 0.43) | |||
| Dairy Products | 0.10 (−0.67, 0.47) | 2.56 (11, 309) | 0.726 | |||
| Intervention | 2.31 ± 1.11 | 2.12 ± 1.80 | 2.29 (1.46, 2.45) | |||
| Control | 2.19 + 1.11 | 2.08 ± 1.31 | 2.16 (1.55, 2.18) | |||
| Fruits | 0.58 (−1.20, 0.04) | 1.23 (11, 309) | <0.05 | |||
| Intervention | 2.96 ± 0.13 | 3.79 ± 1.85 | 2.95 (3.01, 4.01) | |||
| Control | 2.70 ± 0.12 | 2.94 ± 1.53 | 2.68 (2.61, 3.36) | |||
| Vegetables | 0.09 (−0.97, 0.78) | 1.74 (11, 309) | 0.837 | |||
| Intervention | 4.18 ± 0.17 | 4.23 ± 2.40 | 4.11 (3.56, 4.88) | |||
| Control | 4.19 ± 0.17 | 4.23 ± 2.40 | 4.11 (3.49, 4.65) | |||
| Processed Foods | 0.27 (−0.58, 0.04) | 1.49 (11, 309) | 0.08 | |||
| Intervention | 0.83 ± 0.08 | 0.71 ± 0.95 | 0.82 (0.42, 0.95) | |||
| Control | 0.48 ± 0.07 | 0.47 ± 0.72 | 0.46 (0.24, 0.60) | |||
| Snacks High in Sugar and Fat | 0.19 (−0.36, 0.74) | 1.15 (11, 309) | <0.05 | |||
| Intervention | 2.12 ± 0.13 | 1.64 ± 1.28 | 2.20 (0.99, 1.93) | |||
| Control | 1.70 ± 0.13 | 1.56 ± 1.69 | 1.66 (1.31, 1.94) | |||
| Beverages | 0.01 (−0.32, 0.30) | 2.71 (11, 309) | 0.953 | |||
| Intervention | 1.36 ± 0.07 | 1.34 ± 0.90 | 1.35 (0.99, 1.48) | |||
| Control | 1.30 ± 0.07 | 1.33 ± 0.80 | 1.28 (1.02, 1.41) | |||
| Questions | Post Intervention (n = 159) (%) | ||
|---|---|---|---|
| Liked session? | 71.2% very much | 28.8% slightly | 0% not |
| Opinions? It was: | 0% Annoying | 0% Difficult | 51.3%Encouraging |
| 0% Boring | 34.6% Simple | 71.2% Interesting | |
| 0% Confusing | 60.3% Healthy | 24.4% new | |
| 5.1% Time consuming | 42.9% Enjoyable | ||
| Heard new information? | 29.5% A lot | 64.1% A few things | 6.4% none |
| Important to have received the information? | 66.7% very | 32.1% slightly | 1.3% Not |
| Intend to change? | 80.8% Yes | 19.2% No | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pem, D.; Bhagwant, S.; Jeewon, R. A Pre and Post Survey to Determine Effectiveness of a Dietitian-Based Nutrition Education Strategy on Fruit and Vegetable Intake and Energy Intake among Adults. Nutrients 2016, 8, 127. https://doi.org/10.3390/nu8030127
Pem D, Bhagwant S, Jeewon R. A Pre and Post Survey to Determine Effectiveness of a Dietitian-Based Nutrition Education Strategy on Fruit and Vegetable Intake and Energy Intake among Adults. Nutrients. 2016; 8(3):127. https://doi.org/10.3390/nu8030127
Chicago/Turabian StylePem, Dhandevi, Suress Bhagwant, and Rajesh Jeewon. 2016. "A Pre and Post Survey to Determine Effectiveness of a Dietitian-Based Nutrition Education Strategy on Fruit and Vegetable Intake and Energy Intake among Adults" Nutrients 8, no. 3: 127. https://doi.org/10.3390/nu8030127