The Energy Content and Composition of Meals Consumed after an Overnight Fast and Their Effects on Diet Induced Thermogenesis: A Systematic Review, Meta-Analyses and Meta-Regressions


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search
2.2. Eligibility Criteria
2.2.1. Inclusion and Exclusion Criteria
2.2.2. Outcome Measures (Dependent Variables)
2.2.3. First Meal Consumed after an Overnight Fast (Independent Variables)
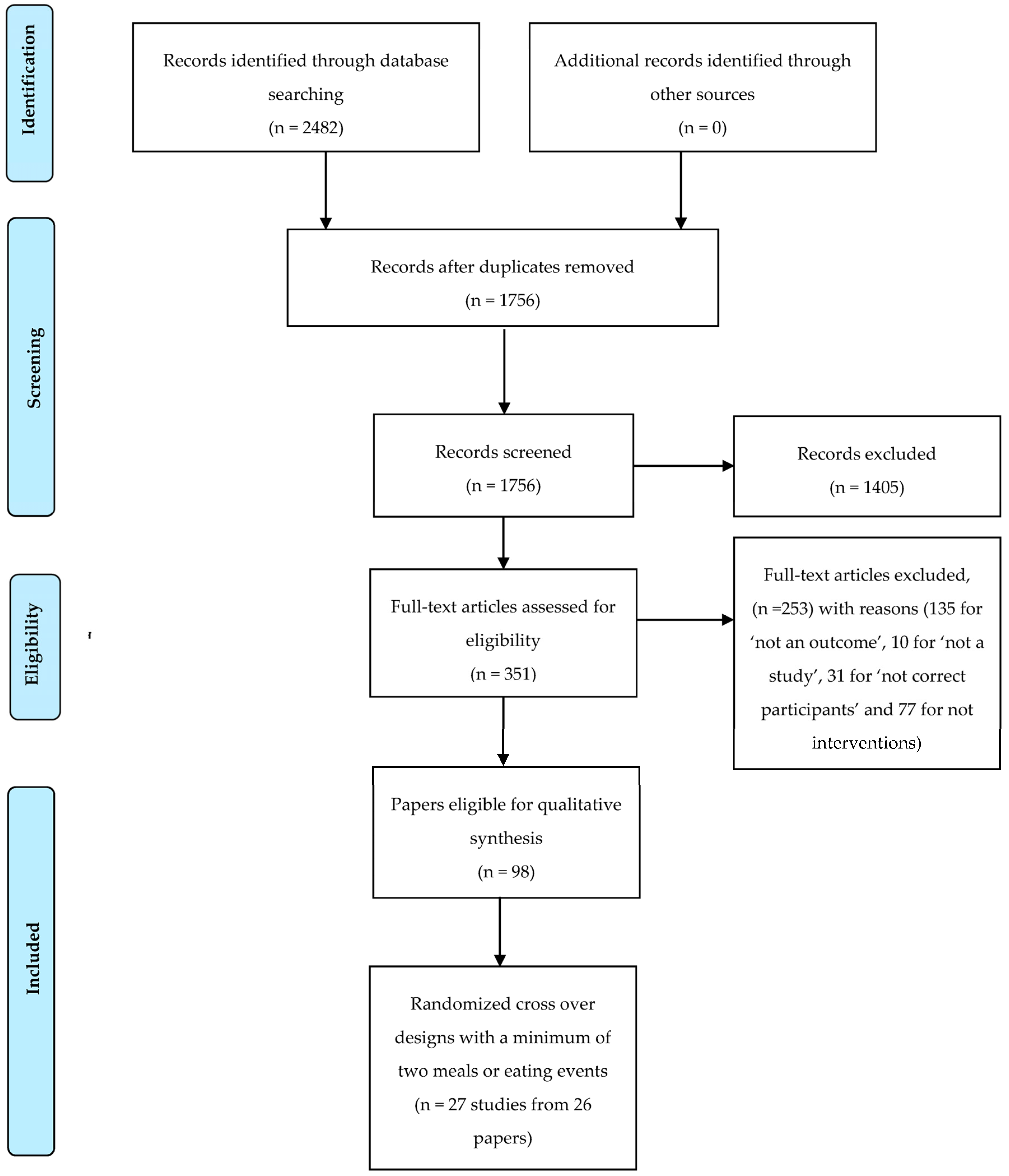
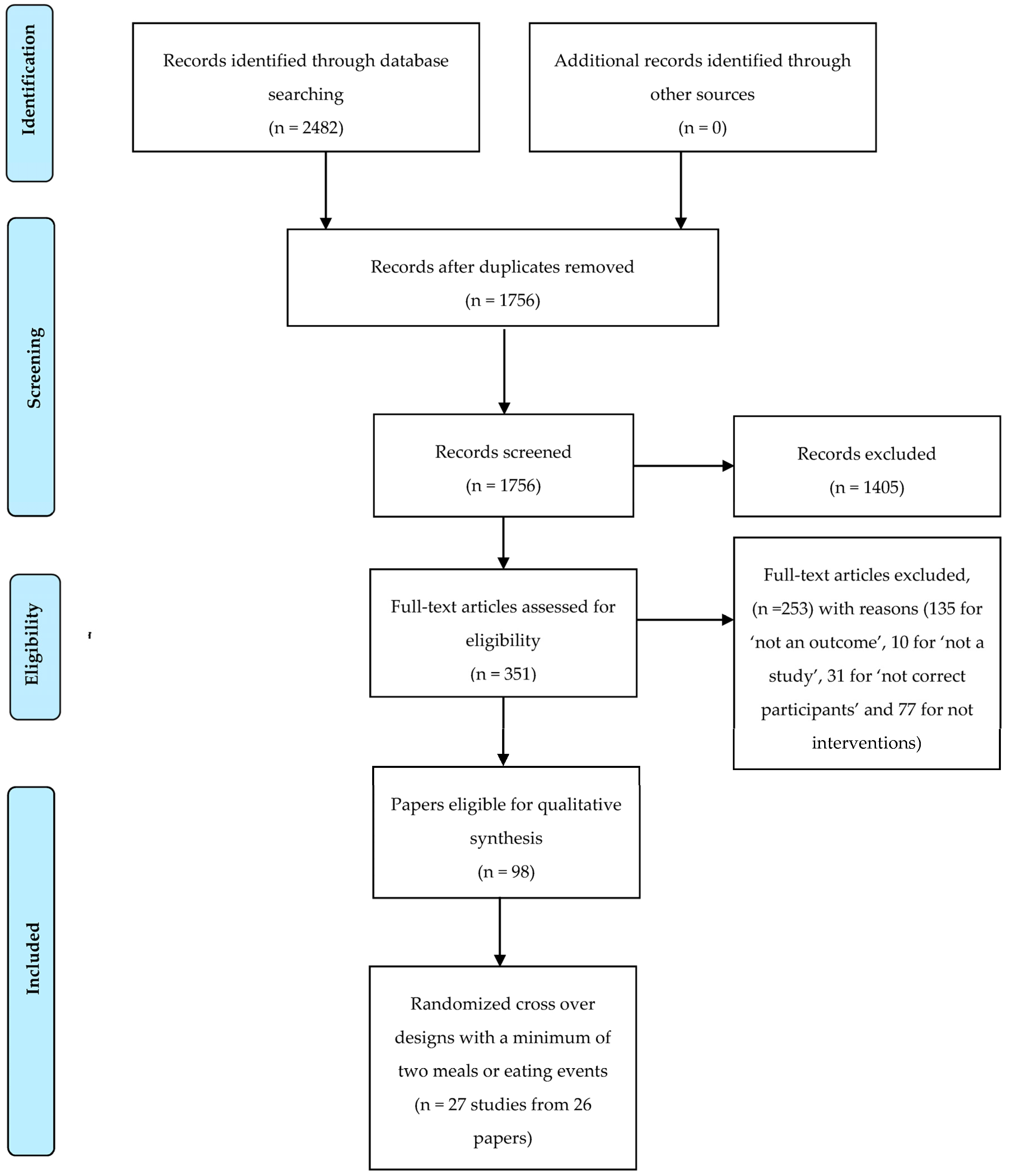
2.2.4. Systematic Review Process
2.2.5. Data Extraction
2.2.6. Participant Characteristics
2.2.7. Characteristics of the Meals
2.2.8. Outcome Characteristics
2.2.9. Meta-Regressions
2.9.10. Meta-Analyses
3. Results
3.1. Participant Characteristics
3.2. Interventions
3.3. Outcomes
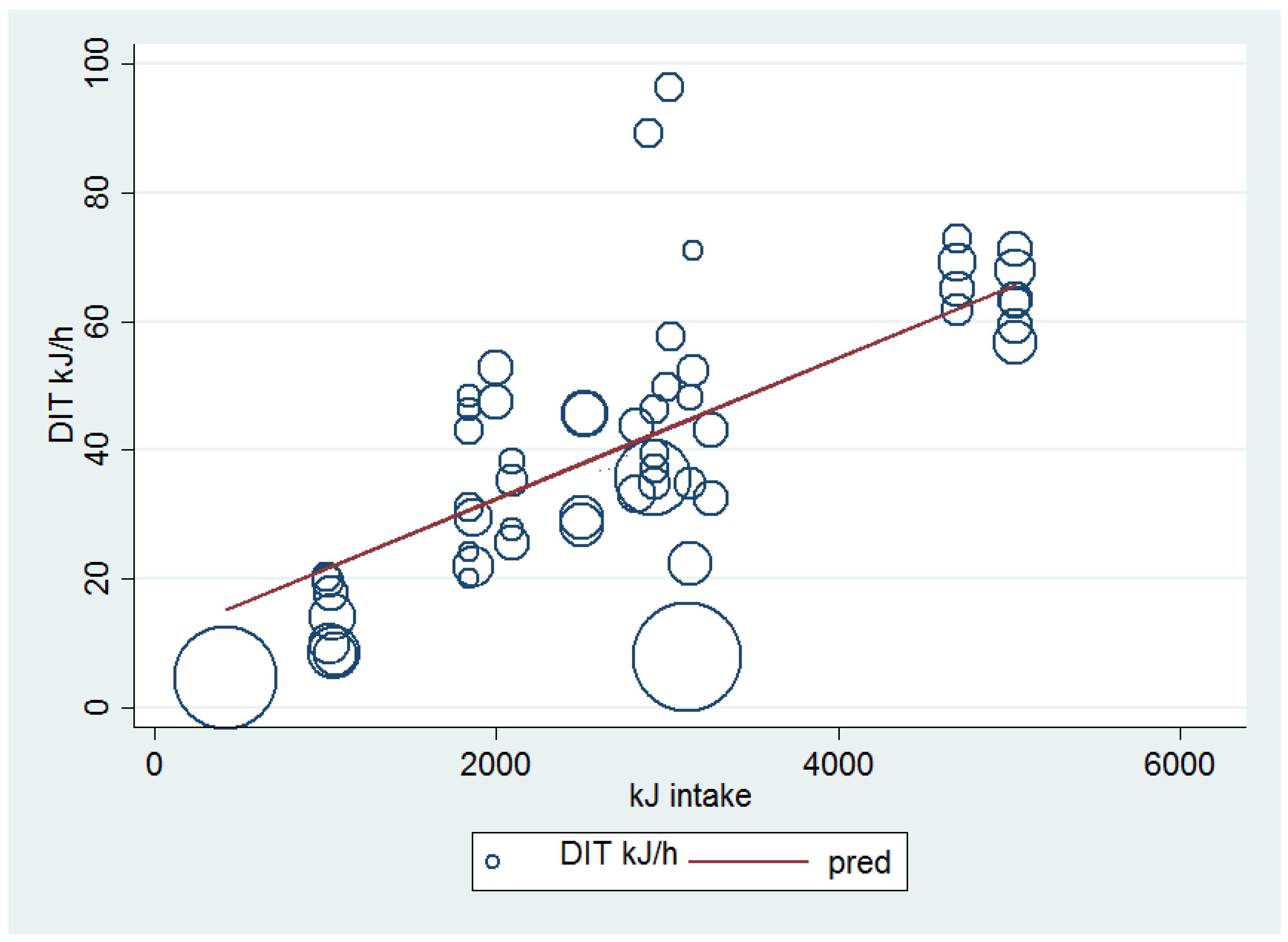
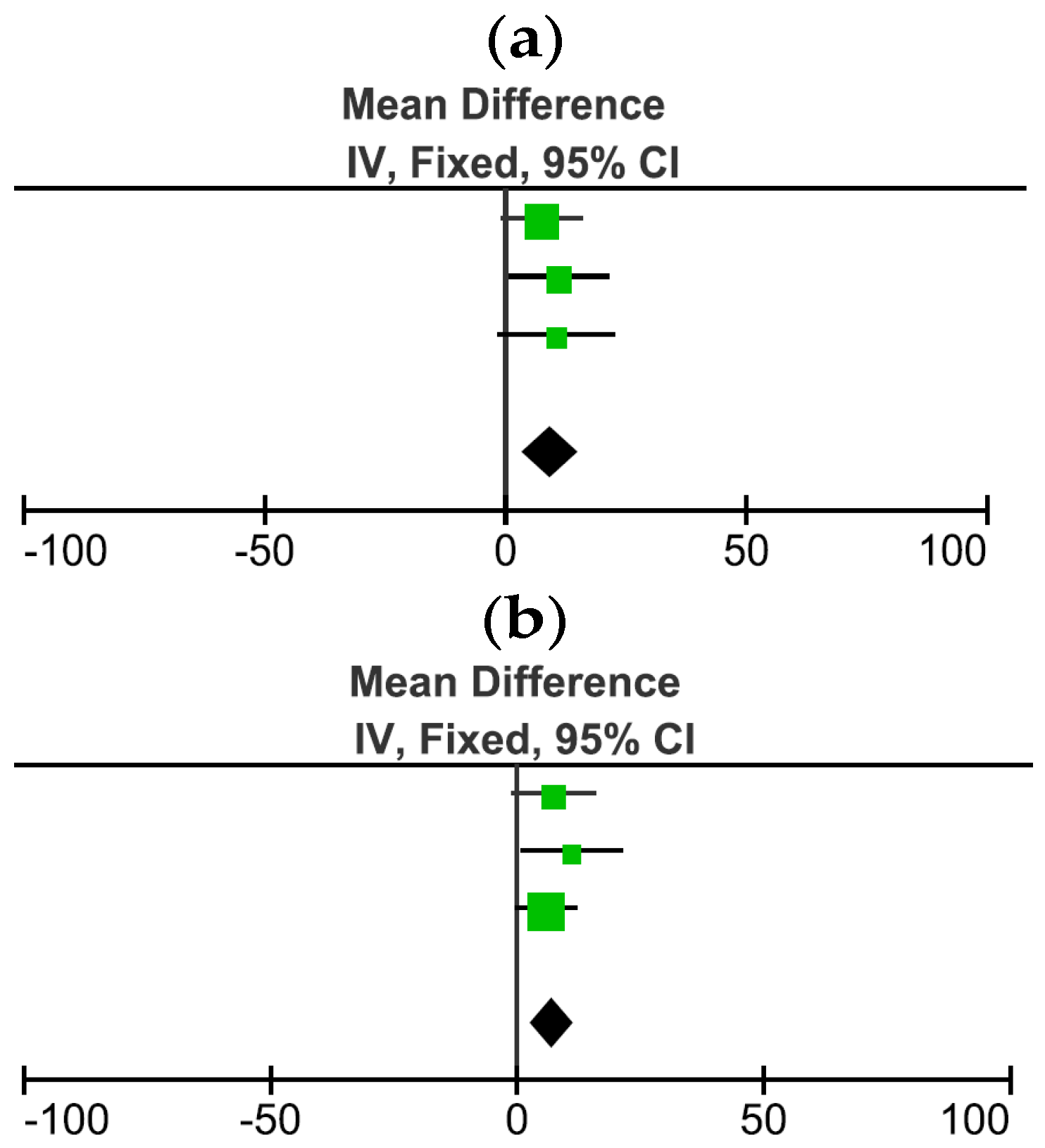
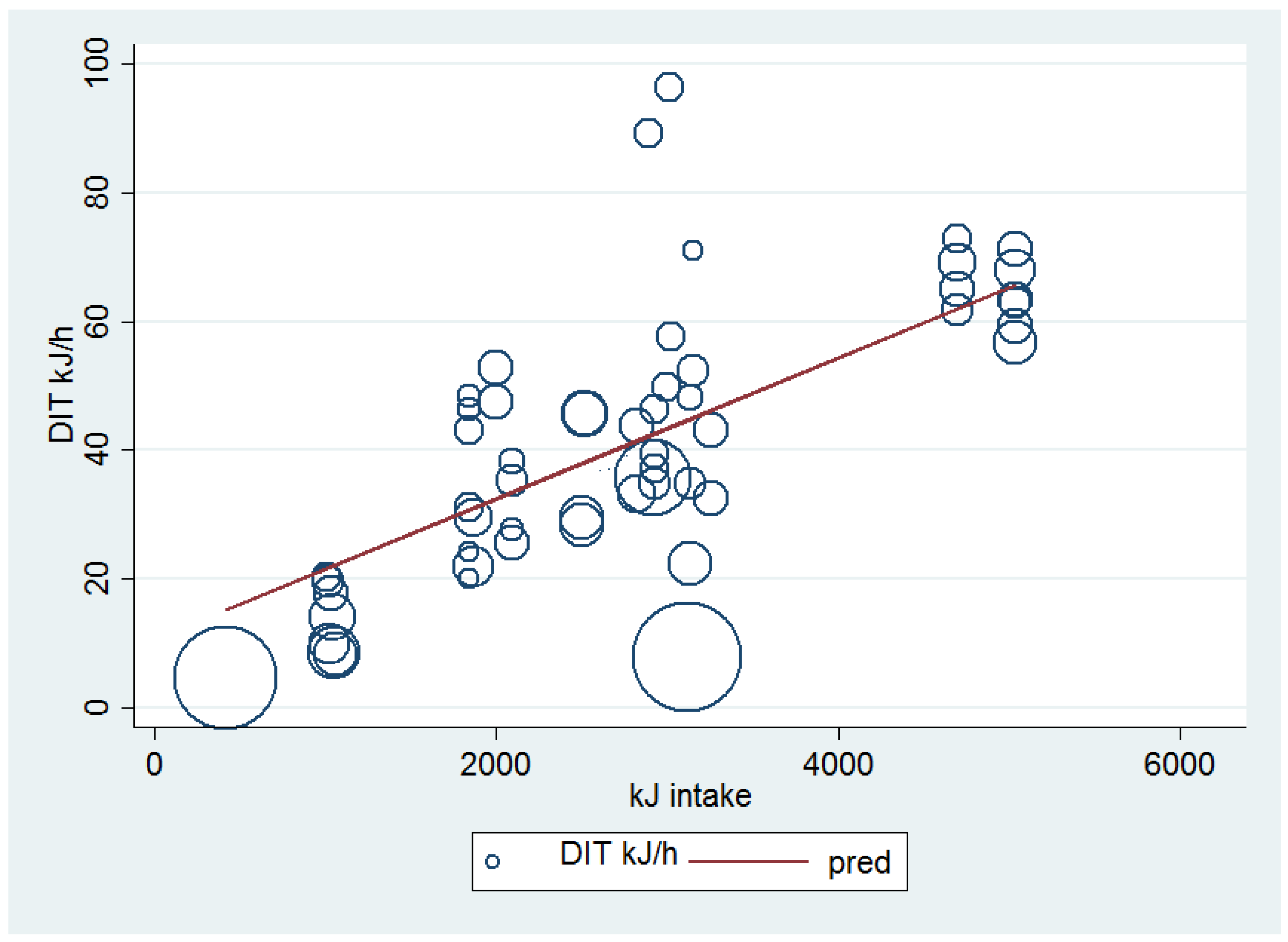
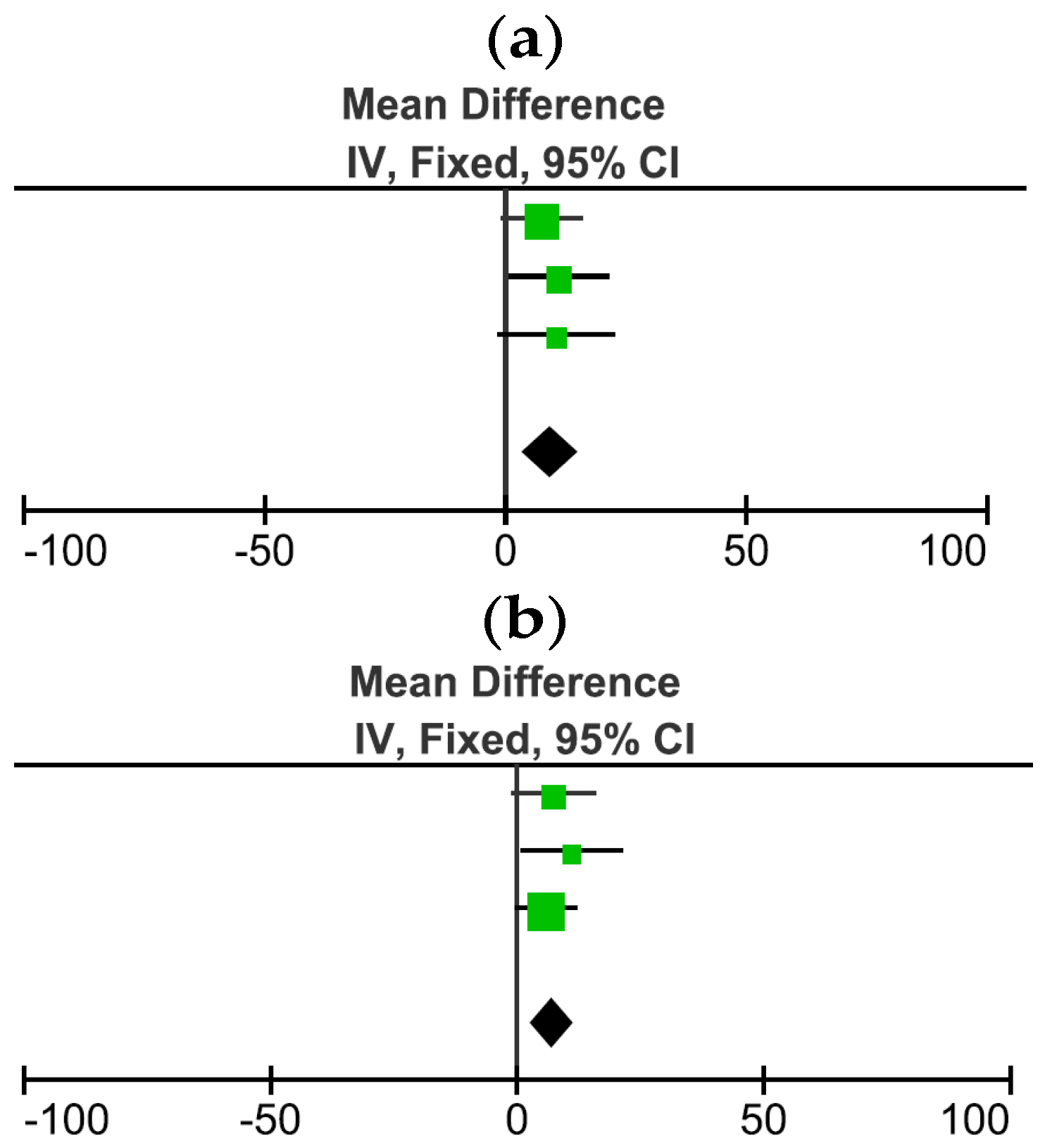
3.4. Comparison and Meta-Regression of the Effects of Higher and Lower Energy Intakes on DIT
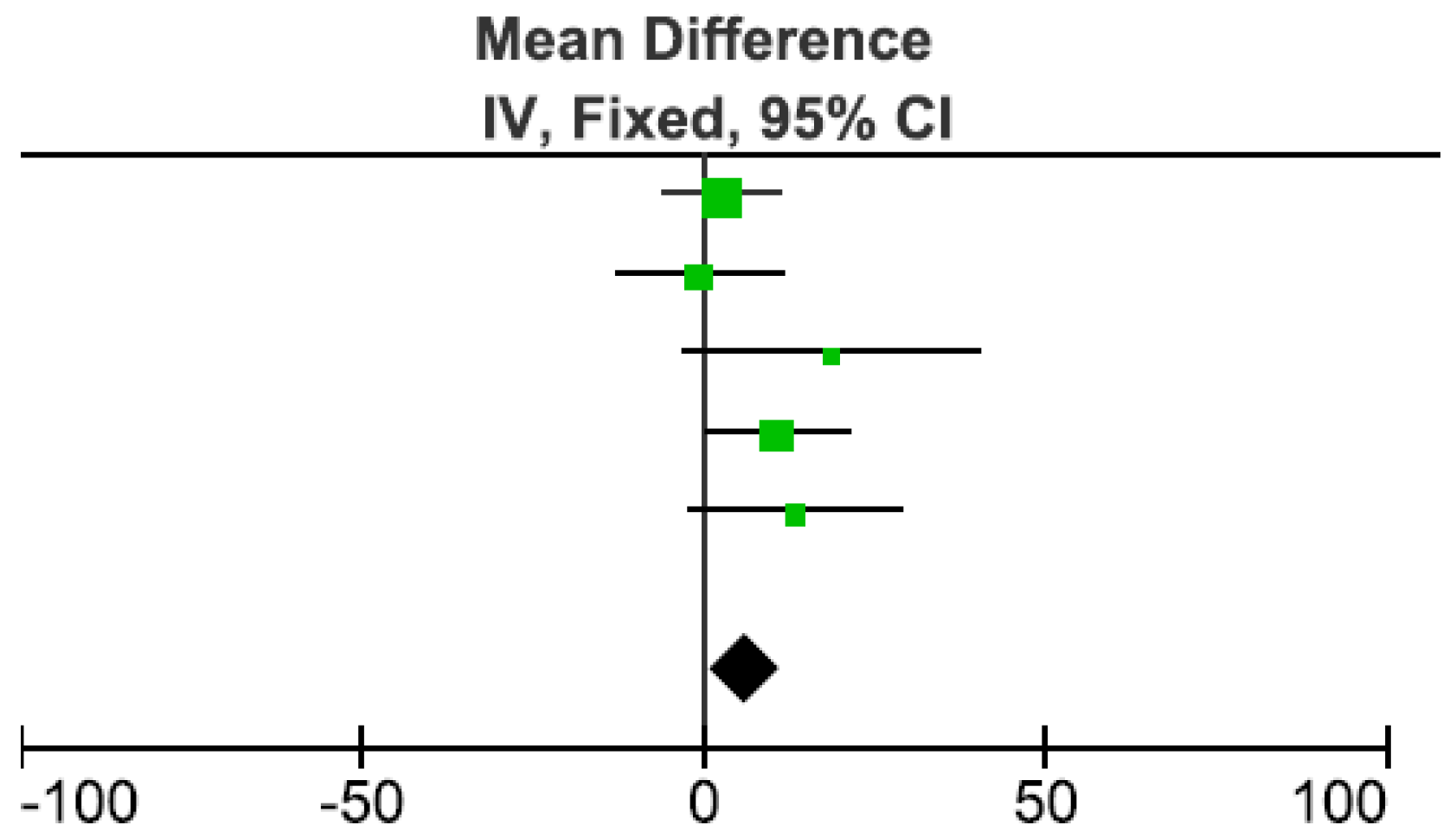
3.5. Influence of Macronutrient Composition on DIT
3.5.1. Long Chain Triglycerides vs. Medium Chain Triglycerides
3.5.2. Monounsaturated Fat vs. Polyunsaturated Fat
3.5.3. Structure of Fats
3.6. Processed vs. Unprocessed Food
3.7. One Bolus Event vs. Isocaloric Smaller Frequent Meals
3.8. Fast vs. Slow/Normal Meal Consumption
3.9. Palatable vs. Unpalatable
4. Discussion
4.1. Strengths of This SR
4.2. Limitations
4.3. Recommendations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AB | Above Baseline |
| ATP | Adenosine Triphosphate |
| BM | Body Mass |
| BMI | Body Mass Index |
| CHO | Carbohydrate |
| CI | Confidence Interval |
| ECM | Energy Content of the Meal |
| FFM | Fat Free Mass |
| FM | Fat Mass |
| DIT | Diet Induced Thermogenesis |
| LCT | Long Chain Triglycerides |
| M | Male |
| MCT | Medium Chain Triglycerides |
| MUFA | Mono Unsaturated Fatty Acids |
| N | Sample |
| NPI | Not Provided Information |
| NP | Not Provided |
| NS | Not Significant |
| PUFA | Poly Unsaturated Fatty Acids |
| RCT | Randomized Controlled Trials |
| REE | Resting Energy Expenditure |
| RMR | Resting Metabolic Rate |
| SD | Standard Deviation |
| SE | Standard Error |
| SFA | Saturated Fatty Acids |
| SR | Systematic Review |
| VO2 | Rate of Oxygen Consumption |
References
- Brown, A.W.; Bohan Brown, M.M.; Allison, D.B. Belief beyond the evidence: Using the proposed effect of breakfast on obesity to show 2 practices that distort scientific evidence. Am. J. Clin. Nutr. 2013. [Google Scholar] [CrossRef] [PubMed]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [CrossRef] [PubMed]
- Casazza, K.; Fontaine, K.R.; Astrup, A.; Birch, L.L.; Brown, A.W.; Bohan Brown, M.M.; Durant, N.; Dutton, G.; Foster, E.M.; Heymsfield, S.B.; et al. Myths, presumptions, and facts about obesity. N. Engl. J. Med. 2013, 368, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Dietitians Association of Australia (DAA). Breakfast. Available online: http://daa.asn.au/for-the-public/smart-eating-for-you/nutrition-a-z/breakfast/ (accessed on 19 July 2016).
- Betts, J.A.; Richardson, J.D.; Chowdhury, E.A.; Holman, G.D.; Tsintzas, K.; Thompson, D. The causal role of breakfast in energy balance and health: A randomized controlled trial in lean adults. Am. J. Clin. Nutr. 2014, 100, 539–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, F.; Ogata, H.; Omi, N.; Nagasaka, S.; Yamaguchi, S.; Hibi, M.; Tokuyama, K. Effect of breakfast skipping on diurnal variation of energy metabolism and blood glucose. Obes. Res. Clin. Pract. 2014, 8, e201–e298. [Google Scholar] [CrossRef] [PubMed]
- WHO. Overweight and Obesity. Available online: http://www.who.int/gho/ncd/risk_factors/overweight_text/en/ (accessed on 13 August 2015).
- Australian Institute of Health and Welfare (AIHW). Overweight and obesity. Available online: http://www.aihw.gov.au/overweight-and-obesity/ (accessed on 19 July 2016).
- Szajewska, H.; Ruszczynski, M. Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in Europe. Crit. Rev. Food Sci. Nutr. 2010, 50, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G. The benefits of breakfast cereal consumption: A systematic review of the evidence base. Adv. Nutr. Int. Rev. J. 2014, 5, 636S–673S. [Google Scholar] [CrossRef] [PubMed]
- Lean, M.E.J.; Malkova, D. Altered gut and adipose tissue hormones in overweight and obese individuals: Cause or consequence? Int. J. Obes. 2016, 40, 622–632. [Google Scholar] [CrossRef] [PubMed]
- Weststrate, J.A. Resting metabolic rate and diet-induced thermogenesis: A methodological reappraisal. Am. J. Clin. Nutr. 1993, 58, 592–601. [Google Scholar] [PubMed]
- Reed, G.W.; Hill, J.O. Measuring the thermic effect of food. Am. J. Clin. Nutr. 1996, 63, 164–169. [Google Scholar] [PubMed]
- Kasai, M.; Nosaka, N.; Maki, H.; Suzuki, Y.; Takeuchi, H.; Aoyama, T.; Ohra, A.; Harada, Y.; Okazaki, M.; Kondo, K. Comparison of diet-induced thermogenesis of foods containing medium-versus long-chain triacylglycerols. J. Nutr. Sci. Vitaminol. 2002, 48, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Raben, A.; Agerholm-Larsen, L.; Flint, A.; Holst, J.J.; Astrup, A. Meals with similar energy densities but rich in protein, fat, carbohydrate, or alcohol have different effects on energy expenditure and substrate metabolism but not on appetite and energy intake. Am. J. Clin. Nutr. 2003, 77, 91–100. [Google Scholar] [PubMed]
- Weststrate, J.A.; Dopheide, T.; Robroch, L.; Deurenberg, P.; Hautvast, J.G. Does variation in palatability affect the postprandial response in energy expenditure? Appetite 1990, 15, 209–219. [Google Scholar] [CrossRef]
- Clegg, M.; Golsorkhi, M.; Henry, C. Combined medium-chain triglyceride and chilli feeding increases diet-induced thermogenesis in normal-weight humans. Eur. J. Nutr. 2013, 52, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Piers, L.S.; Walker, K.Z.; Stoney, R.M.; Soares, M.J.; O’Dea, K. The influence of the type of dietary fat on postprandial fat oxidation rates: Monounsaturated (olive oil) vs. saturated fat (cream). Int. J. Obes. Relat. Metab. Disord. 2002, 26, 814–821. [Google Scholar] [PubMed]
- Sawaya, A.L.; Fuss, P.J.; Dallal, G.E.; Tsay, R.; McCrory, M.A.; Young, V.; Roberts, S.B. Meal palatability, substrate oxidation and blood glucose in young and older men. Physiol. Behav. 2001, 72, 5–12. [Google Scholar] [CrossRef]
- Bowden, V.L.; McMurray, R.G. Effects of training status on the metabolic responses to high carbohydrate and high fat meals. Int. J. Sport Nutr. Exerc. Metab. 2000, 10, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.; Reed, G.W.; Peters, J.C.; Abumrad, N.N.; Sun, M.; Hill, J.O. Short-term effects of dietary-fat ingestion on energy expenditure and nutrient balance. Am. J. Clin. Nutr. 1992, 55, 1071–1077. [Google Scholar] [PubMed]
- Segal, K.R.; Edano, A.; Blando, L.; Pi-Sunyer, F.X. Comparison of thermic effects of constant and relative caloric loads in lean and obese men. Am. J. Clin. Nutr. 1990, 51, 14–21. [Google Scholar] [PubMed]
- Hill, J.O.; Heymsfield, S.B.; McMannus, C., III; DiGirolamo, M. Meal size and thermic response to food in male subjects as a function of maximum aerobic capacity. Metabolism 1984, 33, 743–749. [Google Scholar] [CrossRef]
- Riggs, A.J.; White, B.D.; Gropper, S.S. Changes in energy expenditure associated with ingestion of high protein, high fat versus high protein, low fat meals among underweight, normal weight, and overweight females. Nutr. J. 2007, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Thyfault, J.P.; Richmond, S.R.; Carper, M.J.; Potteiger, J.A.; Hulver, M.W. Postprandial metabolism in resistance-trained versus sedentary males. Med. Sci. Sports Exerc. 2004, 36, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Barr, S.B.; Wright, J.C. Postprandial energy expenditure in whole-food and processed-food meals: Implications for daily energy expenditure. Food Nutr. Res. 2010, 54, 1. [Google Scholar] [CrossRef] [PubMed]
- Tai, M.M.; Castillo, P.; Pi-Sunyer, F.X. Meal size and frequency: Effect on the thermic effect of food. Am. J. Clin. Nutr. 1991, 54, 783–787. [Google Scholar] [PubMed]
- Hamada, Y.; Kashima, H.; Hayashi, N. The number of chews and meal duration affect diet-induced thermogenesis and splanchnic circulation. Obesity 2014, 22, E62–E69. [Google Scholar] [CrossRef] [PubMed]
- Toyama, K.; Zhao, X.; Kuranuki, S.; Oguri, Y.; Kashiwa Kato, E.; Yoshitake, Y.; Nakamura, T. The effect of fast eating on the thermic effect of food in young Japanese women. Int. J. Food Sci. Nutr. 2015, 66, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Nagai, N.; Sakane, N.; Moritani, T. Metabolic responses to high-fat or low-fat meals and association with sympathetic nervous system activity in healthy young men. J. Nutr. Sci. Vitaminol. 2005, 51, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Kinabo, J.L.; Durnin, J.V.G.A. Thermic effect of food in man: Effect of meal composition, and energy content. Br. J. Nutr. 1990, 64, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Kinabo, J.L.; Durnin, J.V. Effect of meal frequency on the thermic effect of food in women. Eur. J. Clin. Nutr. 1990, 44, 389–395. [Google Scholar] [PubMed]
- Blundell, J.E.; Cooling, J.; King, N.A. Differences in postprandial responses to fat and carbohydrate loads in habitual high and low fat consumers (phenotypes). Br. J. Nutr. 2002, 88, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Vaz, M.; Turner, A.; Kingwell, B.; Chin, J.; Koff, E.; Cox, H.; Jennings, G.; Esler, M. Postprandial sympatho-adrenal activity: Its relation to metabolic and cardiovascular events and to changes in meal frequency. Clin. Sci. 1995, 89, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Allirot, X.; Saulais, L.; Seyssel, K.; Graeppi-Dulac, J.; Roth, H.; Charrie, A.; Drai, J.; Goudable, J.; Blond, E.; Disse, E.; et al. An isocaloric increase of eating episodes in the morning contributes to decrease energy intake at lunch in lean men. Physiol. Behav. 2013, 110–111, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Normand, S.; Sothier, M.; Peyrat, J.; Louche-Pelissier, C.; Laville, M. Is advice for breakfast consumption justified? Results from a short-term dietary and metabolic experiment in young healthy men. Br. J. Nutr. 2000, 84, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Bendixen, H.; Flint, A.; Raben, A.; Hoy, C.E.; Mu, H.; Xu, E.; Bartels, E.M.; Astrup, A. Effect of 3 modified fats and a conventional fat on appetite, energy intake, energy expenditure, and substrate oxidation in healthy men. Am. J. Clin. Nutr. 2002, 75, 47–56. [Google Scholar] [PubMed]
- Petzke, K.J.; Klaus, S. Reduced postprandial energy expenditure and increased exogenous fat oxidation in young woman after ingestion of test meals with a low protein content. Nutr. Metab. 2008, 5. [Google Scholar] [CrossRef] [PubMed]
- Casas-Agustench, P.; Lopez-Uriarte, P.; Bullo, M.; Ros, E.; Gomez-Flores, A.; Salas-Salvado, J. Acute effects of three high-fat meals with different fat saturations on energy expenditure, substrate oxidation and satiety. Clin. Nutr. 2009, 28, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Prisma. Prisma Flow Diagram. Available online: http://www.prisma-statement.org/PRISMAStatement/FlowDiagram.aspx (accessed on 21 October 2016).
- Westerterp, K. Diet induced thermogenesis. Nutr. Metab. 2004, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tappy, L. Thermic effect of food and sympathetic nervous system activity in humans. Reprod. Nutr. Dev. 1996, 36, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Lejeune, M.P.; Westerterp, K.R.; Adam, T.C.; Luscombe-Marsh, N.D.; Westerterp-Plantenga, M.S. Ghrelin and glucagon-like peptide 1 concentrations, 24-h satiety, and energy and substrate metabolism during a high-protein diet and measured in a respiration chamber. Am. J. Clin. Nutr. 2006, 83, 89–94. [Google Scholar] [PubMed]
- Westerterp, K.R.; Wilson, S.A.; Rolland, V. Diet induced thermogenesis measured over 24 h in a respiration chamber: Effect of diet composition. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Westerterp-Plantenga, M.S. Protein intake and energy balance. Regul. Pept. 2008, 149, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Tessari, P.; Kiwanuka, E.; Zanetti, M.; Barazzoni, R. Postprandial body protein synthesis and amino acid catabolism measured with leucine and phenylalanine-tyrosine tracers. Am. J. Physiol. Endocrinol. Metab. 2003, 284, E1037–E1042. [Google Scholar] [CrossRef] [PubMed]
- Bach, A.C.; Babayan, V.K. Medium-chain triglycerides: An update. Am. J. Clin. Nutr. 1982, 36, 950–962. [Google Scholar] [PubMed]
- Odle, J. New insights into the utilization of medium-chain triglycerides by the neonate: Observations from a piglet model. J. Nutr. 1997, 127, 1061–1067. [Google Scholar] [PubMed]
- Seaton, T.B.; Welle, S.L.; Warenko, M.K.; Campbell, R.G. Thermic effect of medium-chain and long-chain triglycerides in man. Am. J. Clin. Nutr. 1986, 44, 630–634. [Google Scholar] [PubMed]
- Berry, M.N.; Clark, D.G.; Grivell, A.R.; Wallace, P.G. The contribution of hepatic metabolism to diet-induced thermogenesis. Metabolism 1985, 34, 141–147. [Google Scholar] [CrossRef]
- Dulloo, A.G.; Fathi, M.; Mensi, N.; Girardier, L. Twenty-four-hour energy expenditure and urinary catecholamines of humans consuming low-to-moderate amounts of medium-chain triglycerides: A dose-response study in a human respiratory chamber. Eur. J. Clin. Nutr. 1996, 50, 152–158. [Google Scholar] [PubMed]
- Ruddick-Collins, L.C.; King, N.A.; Byrne, N.M.; Wood, R.E. Methodological considerations for meal-induced thermogenesis: Measurement duration and reproducibility. Br. J. Nutr. 2013, 110, 1978–1986. [Google Scholar] [CrossRef] [PubMed]
- Piers, L.S.; Soares, M.J.; Makan, T.; Shetty, P.S. Thermic effect of a meal. 1. Methodology and variation in normal young adults. Br. J. Nutr. 1992, 67, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Schlundt, D.G.; Hill, J.O.; Sbrocco, T.; Pope-Cordle, J.; Sharp, T. The role of breakfast in the treatment of obesity: A randomized clinical trial. Am. J. Clin. Nutr. 1992, 55, 645–651. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference and Location | Sample (n) Males (m) % Age (Years) | BMI (kg/m2) FFM (% or kg) FM (% or kg) | RMR (kJ/h, Measured before Interventions a, b, c, etc.) | Protocol | Gap between Intervention Meals and Types of Meals Provided |
|---|---|---|---|---|---|
| Higher vs. lower energy intake | |||||
| Kinabo and Durnin [31]—Paper A †† UK | n = 16 m = 0 † % 22 (5.8) † years | BMI = 20.8 (0.2) † FFM = 42.9 (3.1) † kg FM = 240 (23.2) † g/kg body weight | (a) 222 † (69.7) † (b) 219 † (69.7) † (c) 221.4 † (69.7) † (d) 208.2 † (69.7) † | Arrival at 8:00 a.m.; fasting from 8:00 p.m. 30 min rest; RMR measured, meal consumed within 10 min. | Gap = each meal provided on different days. (a) high CHO, low Fat—lower energy (b) low CHO, high Fat—lower energy (c) high CHO, low Fat—higher energy (d) low CHO, high Fat—higher energy |
| Hill et al. [23] USA | n = 8 (4 low VO2max group average is 43 mL/kg/min—4 high VO2max group average is 62 mL/kg/min) m = 100 † % high VO2max 20 (3.5) † years low VO2max 26 (5.2) † years | High VO2max BMI = 21.9 † FFM = 62.9 (3.6) † kg FM = 13.8 (2.8) † % Low VO2max BMI = 23.7 † FFM = 66.8 (6.9) † kg FM = 16 (4.2) † % | High VO2max subjects 301.7 † (22.5) † Low VO2max subjects 294.6 † (40.5) † | 12 h fast; rest for 60–90 min; then RMR measured; meals consumed within 10 min. | Gap = NPI Liquid meal (a) lower energy intake (b) medium level energy intake (c) higher energy intake |
| Martin et al. [36] France | n = 10 m = 100 † % 28 (2) years | BMI = 22.2 (0.5) | 14 days of intervention meals: meal consumed at research centre daily between 7:00 and 8:00 a.m. On day 15: arrive at 7:00 a.m.; overnight fast; RMR measured; meal consumed within 30 min at 8:00 a.m. | Gap = 28 days (a) 14 days of intervention meals: low energy, moderate fat breakfast (b) 14 days of intervention meals: high energy, low fat breakfast | |
| Bennet et al. [21] USA | n = 4 (untrained) m = 100 † % 28 (8) years Excluded trained subjects | BMI = 23 † (3) † FM = 20.5 † (4.3) † % | Meal consumed at 8:30 a.m. | Gap ≥ 24 h (a) normal meal provided (25% of energy intake of the total day) (b) high fat meal: plus 50 g of fat compared to the normal fat meal | |
| Segal et al. [22] USA | n = 11 m = 100 † % 31 (6.3) † years Excluded obese subjects | BMI = 25.5 † FFM = 66.1 (4.1) † kg FM = 15.3 (2.2) † % | 343.9 † (31.6) † | 12 h fast; 9:00 a.m. arrival; 30 min rest; RMR measured for three five-minute measurements. | Gap = NPI (a) 35% of each man 24 h RMR meal (b) 3013 kJ meal |
| Meals varying in macronutrients composition | |||||
| Nagai et al. [30] Japan | n = 14 m = 100 † % 23.6 (1.8) † years | BMI = 21.3 (1.4) † FM = 18.4 (3.6) † % | 375.3 † (39.7) † 373.2 † (44.0) † | Fast from 10:00 p.m.; arrival at 7:30 a.m.; rest for 30 min; continuous RMR measurement. (NP length); meals consumed at 8:30 a.m. within 15 min. | Gap = NPI (a) standard meal—low fat meal (b) standard meal—high fat meal |
| Blundell, Cooling and King [33] UK | n = 24 m = 100 † % High fat consumers (n = 12) 20.7 (1.6) † years Low fat consumers (n = 12) 21.6 (2.3) † years | High fat consumers BMI = 21.2 (5.0) † FM = 11.1 (4.3) † % Low fat consumers BMI = 22.4 (2.0) † FM = 11.4 (4.3) † | High fat consumers 286.08 † (0.02) † Low fat consumers 259.58 † (0.03) † | Arrival at ~9:00 a.m. after 12 h fast; 30 min of steady RMR were measured; milkshake consumed within 5 min. | Gap = NPI (a) high fat milkshakes drink (b) high CHO milkshake drink |
| Bowden and McMurray [20] USA | n = 6 m = 0 † % 33.8 (10.7) years Excluded trained subjects | BMI = 21.7 (1.6) FFM = 43.9 (3.3) Kg FM = 21.4 (3.7) % | 208.2 † (12.6) † | Arrival at lab at 6:30 a.m.; 10 h fast; RMR obtained over two 5 min periods; meal consumed within 20 min | Gap = 2 days (a) high CHO meal (b) high fat meal |
| Thyfault et al. [25] USA | n = 12 Sedentary m = 100 † % 24.8 (4.6) † years Excluded trained subjects | FM = 21.5 (4.3) † % FFM = 58.3 (2.7) † kg | 7262 (394.7) kJ †—NP unit of time | Arrival at 5:00 a.m.; 12 h fast; 30 min supine rest; RMR measured for 30 min; meal consumed within 10 min. | Gap = 7 days (a) high carbohydrate liquid meal (b) moderate fat liquid meal |
| Raben et al. [15] Denmark | n = 19 m = 52.6 † % 23.3 (2.1) † years | BMI = 22.1 (1.7) † FM = 18.8 (4.7) † % | Arrival at 8:00 a.m.; 10 h fast; 30 min supine rest; RMR measured for 45 min; meals consumed within 15 min at 9:45 a.m. | Gap = ≥4 weeks and no more than 8 weeks standard meal (a) high protein meal (b) high fat meal (c) high CHO meal Excluded high alcohol meal | |
| Petzke and Klaus [38] Germany | n = 6 m = 0 † % 25.5 (2.6) years | BMI = 20.6 (2.5) | (a) 218 (12) (b) 230 (13) | 12 h fast; RMR measured for 30 min between 8 and 9 a.m.; meal ingested between 9 and 9:30 a.m. and within 10 min. | Gap = 2 days (a) low protein meal (b) adequate protein meal |
| Riggs et al. [24] USA | n = 21 m = 0 † % Overweight (n = 6) 22.8 (2.4) † years Normal weight (n = 12) 20.8 (2.6) † Underweight (n = 3) 20.7 (2.2) † years | Overweight BMI = 26.9 (1.7) † FFM = 48.4 (3.9) † kg FM = 31.4 (2.7) † % Normal weight BMI = 21.1 (1.7) † FFM = 44.6 (4.0) † kg FM = 23.0 (2.9) † % Underweight BMI = 18.1 (1.5) † FFM = 41.7 (4.0) † kg FM = 19.5 (2.4) † % | 12 h fast; 10 min rest; RMR measured between 7 and 8:00 a.m.; meal eaten within 15–20 min. | Gap = 1 week to 2.5 months (a) high protein, high fat bars (b) high protein, low fat bars | |
| Clegg et al. [17] UK | n = 7 m = 14.3 † % 25.7 (3.6) years | BMI = 21.9 † | Arrived after an overnight fast; rested for 30 min; RMR measured between 7:30 a.m. to 9:00 a.m. at 1 min intervals for 30 min; meal consumed within 15 min. | Gap = minimum of four days (a) meal with bell pepper and sunflower oil (18.4 g) (b) meal with bell pepper and MCT oil (20.0 g) Excluded two chilli meals | |
| Kasai et al.—study 1 [14] Japan | n = 8 m = 100 † % 26.8 (1.9) † years | BMI = 22.7 (2.1) † | (a) 294.6 † (32.3) † (b) 280.3 † (29.9) † (c) 286.3 † (23.5) † | Dinner at 9:00 p.m.; overnight fast; meal consumed at 11:00 a.m. | Gap = NP Liquid meal with (a) 10 g LCT (b) 5 g MCT; 5 g LCT (c) 10 g MCT |
| Kasai et al.—study 2 [14] Japan | n = 8 (n = 7 for the two mayonnaise arms as one drop out) m = 0 † % 28.1 (3.7) † years | BMI = 18.8 (1.1) † | (a) 211.1 † (14.9) † (b) 206.2 † (22.5) † (c) 209.4 † (34.9) † (d) 198.2 † (32.8) † | Dinner at 9:00 p.m.; overnight fast; meal consumed at 11:00 a.m. | Gap = 1 to 2 day interval within the same week for each experimental session (mayonnaise trials and margarine trials) Standard meal with (a) mayonnaise with 5 g LCT (b) mayonnaise with 5 g MCT (c) margarine with 5 g LCT (d) margarine with 5 g MCT |
| Casas-Agustench et al. [39] Spain | n = 29 m = 100 † % 22 (4) years | BMI = 24.1 (4.5) | (a) 318.5 (95% CI 298.2—338.8) (b) 318.9 (95% CI 298.5—339.3) (c) 323.2 (95% CI 302.3—344.1) | Arrived at 8:00 a.m. fast; 10 min rest; RMR measured for 30 min; meal provided at 9:00 a.m. and eaten within 30 min | Gap = 1–11 days (a) standard meal rich in PUFA (b) standard meal rich in MUFA (c) standard meal rich in SFA |
| Piers et al. [18] Australia | n = 14 m = 100 † % 38 (9) years | BMI = 27.8 (3.2) FFM = 62.7 (8.5) kg FM = 29.5 (4.8) % | (a) 311 (40) (b) 307 (36) | Arrival at 7:00–8:00 a.m.; 12–14 h of fast; 30 min rest; RMR measured for 35 min. | Gap = 7–14 days (a) meal with SFA (b) meal with MUFA |
| Bendixen et al. [37] Denmark | n = 11 m = 100 † % 25.1 (1.6) † years | BMI = 22.5 (1.9) † FM = 18 (3.2) † % FFM = 62.9 (6.3) † kg | (a) 290.4 † (28.5) † (b) 289.8 † (22.8) † (c) 292.2 † (26.6) † (d) 289.8 † (34.2) † | Fast ≥ 12 h; 30 min supine rest; RMR measured for 45 min; meal consumed by 15 min. | Gap = 14–28 days Standard meal with liquid test drink (a) conventional fat (rapeseed oil) (b) chemically structured fat (rapeseed oil and octanoic acid by esterification with sodium methoxide) (c) lipase structured fat (rapeseed oil and octanoic acid by esterification with lipoxime IM) (d) physically mixed fat (blending rapessed oil and trioctanoate) |
| Processed vs. unprocessed meals | |||||
| Barr and Wright [26] USA | n = 17 in analyses m = 29.4 † % 25.5 (12.4) † years | BMI = 22.0 (2.2) † | Fast for 12 h; 2 RMR measurements ~30 min apart before and just before consuming the meal; meals consumed between 9:15 and 11:15 a.m. and at approximately the same time for each measurement sessions. | Gap = on two consecutive days or not longer than a week apart. (a) whole-food meal as either 1½ sandwich or 2 sandwiches (b) pre-prepared processed foods as either 1½ sandwich or 2 sandwiches. | |
| Bolus vs. smaller frequent meals | |||||
| Kinabo and Durnin [32]-Paper B Scotland, UK | n = 18 m = 0 † % Group A (n = 8) 24 (5.3) † years Group B (n = 10) 20 (7.2) † years | Group A BMI = 21 (1.3) † FFM = 42.4 (2.9) † kg FM = 23 (2.6) † % Group B BMI = 21 (2.1) FFM = 43.6 (4.2) † kg FM = 23 (6) † % | Group A: (a) 226.8 † (27.0) † (b) 214.8 † (20.6) † Group B (c) 230.4 † (30.6) † (d) 221.4 † (14.4) † | Arrival at 8:00 a.m., at least 12 h fast; 30 min supine rest; RMR measured; meal consumed either as a large bolus meal within 20 min or as two smaller meals within 10 min every 180 min. | Gap = 1 week Group A: (a) high carb-low fat meal; one large meal (b) high carb-low fat meal; two smaller meals Group B: (c) low carb-high fat meal; one large meal (d) low carb-high fat meal; two smaller meals |
| Vaz et al. [34] Australia | n = 10 m = 100 † % | BMI = 22.9 (1.8) † FFM = 64 (5.7) † kg FM = 16.6 (6.0) † % | 12–14 h overnight fast; RMR measured after 30 min rest. | Gap = approximately 14 days (a) standard meal-single meal (b) standard meal- three smaller meals | |
| Allirot et al. [35] France | n = 20 m = 100 † % 27.1 (5.7) † years | BMI = 22.0 (1.3) † | Arrival at 7:00 a.m.; fast since 9:00 p.m.; RMR measured for 30 min; meals consumed either as a bolus event within 20 min or as smaller meals every hour within 10 min each. | Gap = at least 7 days (a) one 20 min long episode (b) 4 smaller meals in 10 min episodes | |
| Tai et al. [27] USA | n = 7 m = 0 † % 26.7 (2.9) years | BMI = 20.8 (2.1) FM = 17.1 (5.4) % | (a) 233.7 † (9.8) † (b) 236.22 † (14.1) † | RMR measured after 12–14 h fast and minimum of 30 min rest; meals consumed as one bolus event within 10 min or as smaller meals every 30 min. | Gap = meals provided on different days (a) liquid meal taken in one eating event of 10 min long (b) liquid meal in 6 equal smaller meals at 30 min interval over 150 min. |
| Fast vs. slow eating patterns | |||||
| Hamada et al. [28] Japan | n = 10 m = 100 † % 25 (1) years | BMI = 19.8 † FM = 13 (2) % | Fast since dinner (>10 h); 20 min semi-supine position rest; RMR measured for 20 min. | Gap = NPI standard meal (a) rapid eating (b) slow eating | |
| Toyama et al. [29] Japan | n = 9 m = 0% 22 (2.1) years | BMI (a) 21.3 (1.7) (b) 21.3 (1.8) FM (a) 24.1 (3.8) % (b) 24.0 (4.0) % | (a) 196.8 † (17.3) † (b) 191.6 † (17.6) † | Dinner by 9:00 p.m., fast until morning; arrival at 8:00 a.m., 30 min supine rest; RMR measured; meal consumed at 9:00 a.m. | Gap = at least 7 days Same meal provided (a) fast eating (5 min) (b) regular eating (15 min) |
| Palatable vs. unpalatable meals | |||||
| Sawaya et al. [19] USA | n = 19 m = 100 † % Old (n = 9) 69.4 (1.3) years Young (n = 10) 23.4 (1) years | Old BMI = 24.4 (0.9) FFM = 55 (2.2) FM = 26.2 (1.9) % Young BMI = 22.7 (0.5) FFM = 64.1 (1.9) kg FM = 12 (1.3) % | (a) young 319.8 † (32.4) † old 280.2 † (30.5) † (b) young 319.2 † (32.4) † old 268.8 † (23.8) † | Sleep at university by 10:00 p.m., awakened at 6:30 a.m.; 30 min rest; RMR measured for 30 min; meals consumed within 20 min. | Gap = 1 week interval (a) palatable meal (b) control meal |
| Weststrate et al. [16] Netherlands—study 1 | n = 12 m = 50 † % Men 22.7 (1.8) † years Women 21.2 (1.8) † years | Men FM = 12.0 (2.2) † % Women FM = 29.0 (2.5) † % | Overnight fast. | Gap = At least 2 days (a) palatable meal (b) unpalatable meal | |
| Reference and DIT Measurement | Energy Ingested (kJ) and % Energy from Macronutrients | DIT (kJ) | DIT % Energy Content of the Meal | DIT % above Baseline | Conclusions |
|---|---|---|---|---|---|
| Higher vs. lower energy intake | |||||
| Kinabo and Durnin [31] Paper A †† DIT = open circuit indirect calorimetry using Douglas bag for 5 h; DIT measured for 10 min, every 10 min for 3 collections then every 20 min for 5 collections | (a and b) 2520 kJ (c and d) 5040 kJ (a and c) 70% CHO, 11% protein, 19% fat (b and d) 24% CHO, 11% protein and 65% fat | (a) 45.6 † (9.3) † kJ/h (b) 45.6 † (10.8) † kJ/h (c) 71.2 † (15.5) † kJ/h (d) 68 † (12.4) † kJ/h NS (a and c vs. b and d for kJ/5 h) *** (a and b vs. c and d for kJ or kcal /5 h) NS (all four meals compared for kJ or kcal /5 h) | (a) 1.8 † (0.4) † %/h (b) 1.8 † (0.5) † %/h (c) 1.4 † (0.3) † %/h (d) 1.4 † (0.2) † %/h | (a) 21 (4.3) †% (b) 21 (5.8) † % (c) 33 (7.7) † % (d) 33 (6.2) † % | No significant difference between meals differing on macronutrient compositions. Significantly higher DIT for meals with higher energy intake compared to lower energy intake. |
| Hill et al. [23] DIT = indirect calorimetry for 3 h; DIT measured every 30 min | (a) 2092 kJ † (b) 4184 kJ † (c) 6276 kJ † 50% CHO, 16% protein, 34% fat | (a) high and low VO2 group: less than 10% (b) high VO2max 23% low VO2max 19% (c) high VO2max 41%, low VO2max 26% p value NP | An increase in meal size increased DIT. Unclear if effect was significant. | ||
| Martin et al. [36] DIT = ventilated hood indirect calorimetry for 4 h; DIT measured every hour | (a) 418 kJ, 62% CHO, 34.4% fat, 3.6% protein (b) 2920 kJ, 67% CHO, 24.6% fat, 8.4% protein | (a) 4.5 † (1.4) † kJ/h (b) 35.6 † (2.6) † kJ/h | (a) 1.1 (0.3) %/h (b) 1.2 (0.1) %/h p value NP | No difference on DIT between low energy, moderate fat meal, and high energy, low fat meal. | |
| Bennet et al. [21] DIT = ventilated hood indirect calorimetry for 6 h; continuously | NP kJ (a) 55% CHO, 30% fat, 15% protein (b) same meal as above plus 50 g of fat (addition of 1881 kJ compared to breakfast (a)) | (a) 1.3 † (0.3) † %/h (b) 1.2 † (0.40) † %/h NS (a vs. b for all subjects (trained and untrained) only included untrained for this SR) | No significant difference in DIT between high fat meal and normal fat meal for the overall subjects (trained vs. untrained). | ||
| Segal et al. [22] DIT = open circuit indirect calorimetry for 3 h; DIT measured for at least 6 min periods every 30 min | (a) 35% of each man 24 h RMR (2889 *‡ kJ) NP macronutrients (b) 3013 kJ †, 55% CHO, 24% protein, 21% fat | (a) 89.3 † (17.6) † kJ/h (b) 96.3 † (17.6) † kJ/h | (a) 3.2 † (0.8) † %/h (b) 3.3 † (0.4) † %/h NS (a vs. b %/3 h) | (a) 11.9% (b) 12.9% | N.A. |
| Meals varying in macronutrient composition | |||||
| Nagai et al. [30] DIT = open circuit indirect calorimetry for 3.5 h; DIT measured for 6 min every 30 min | 3255 (306.5) † kJ (a) 70% CHO, 10% protein, 20% fat (b) 20% CHO, 10% protein, 70% fat | (a) 43.1 † (13.7) † kJ/h (b) 32.6 † (14.1) † kJ/h * (a vs. b for kJ/3.5 h) | (a) 1.3 † (0.4) † %/h (b) 1.0 † (0.4) † %/h * (a vs. b for %/3.5 h ECM) | (a) 1.7 (0.7) † % (b) 1.3 (0.4) † % * (a vs. b for % AB) | DIT was significantly higher in low fat meal compared to high fat meal. |
| Blundell et al. [33] DIT = ventilated hood indirect calorimetry for 3 h continuously | 2092 kJ (a) 19.9% CHO, 78.8% fat, 1.3% protein (b) 90.4% CHO, 1.3% fat, 8.3% protein | (a) high fat consumers 27.5 † (28.9) † kJ/h; low fat consumers 25.6 † (14.5) † kJ/h (b) high fat consumers 38.2 † (26.0) † kJ/h; low fat consumers 35.2 † (15.6) † KJ/h * (a vs. b for kJ/day) | (a) high fat consumers 1.3 † (1.4) † %/h; low fat consumers 1.2 † (0.7) † %/h (b) high fat consumers 1.7 † (1.2) † %/h; low fat consumers 1.7 † (0.7) † %/h | (a) high fat consumers 10.2 † (10.8) † % low fat consumers 9.9 † (5.6) † % (b) high fat consumers 14.2 † (9.7) † % low fat consumers13.6 † (6.0) † % | The consumption of a high-carbohydrate meal was significantly associated with an increased DIT compared to a high fat meal |
| Bowden and McMurray [20] DIT = open circuit spirometry for 5 h; DIT measured for 10 min periods every 30 min | (a) 2068 kJ, 76% CHO, 5% protein, 23% fat (b) 2093 kJ (fixed amount), 21% CHO, 8% protein, 72% fat | (a) 54.6 † kJ/h (b) 27.8 † kJ/h | (a) 2.6 † %/h (b) 1.3 † %/h p value NP | (a) 26.2 † % (b) 13.4 † % | No significant difference on total energy expenditure between high CHO and high fat meal. |
| Thyfault et al. [25] DIT = indirect calorimetry with face mask for 4 h; DIT measured continuously with measurements averaged over 15 min periods for 1 h then for 30 min periods for the remaining hours | (a) 3021 (1194.0) † kJ, 79% CHO, 20% protein, 1% fat (b) 2996 (1167.4) † kJ, 37% CHO, 18% protein, 45% fat | (a) 57.8 † (19.1) † kJ/h or 1.0 (0.3) † kJ/FFM/h or 0.7 (0.9) † kJ/BM/h (b) 49.8 † (21.6) † kJ/h or 0.8 (0.3) † kJ/FFM/h or 0.6 (0.9) † kJ/BM/h p value NP | (a) 1.9 † (0.6) † %/h (b) 1.7 † (0.7) † %/h p value NP | N.A. | |
| Raben et al. [15] DIT = indirect calorimetry with an open-circuit ventilated hood system; continuously for 5 h with 5 min breaks every h if needed | 2500 kJ for f, 3000 kJ for m (a) 37.2% CHO, 31.8% protein, 31.1% fat (b) 23.9% CHO, 11.6% protein, 64.6% fat (c) 65.4% CHO, 12.2% protein, 23.7% fat | (a) 45.9 † kJ/h (b) 39.2 † kJ/h (c) 39.2 † kJ/h | (a) 1.7%/h (b) 1.4%/h (c) 1.4%/h ** (a vs. b vs. c vs. also meal with alcohol excluded for this SR for %/5 h) | Significant difference in DIT between the different meal types administered. Protein had a higher DIT compared to fat and CHO meals. | |
| Petzke and Klaus [38] DIT = indirect calorimetry ventilated-hood system for 6 h; 3 × 30 min measurements (first 5–10 min discarded) at 30, 150, and 270 min | (a) 3114 kJ, 35.4% CHO, 3.9% protein, 60.7% fat (b) 3131 kJ, 27.8% CHO, 11.4% protein, 60.8% fat | (a) 7.8 † (1.0) † kJ/h (b) 22.4 † (5.7) † kJ/h *** (a vs. b for kJ/6 h) | (a) 1.5 † (0.2) † %/h (b) 4.3 † (1.1) † %/h *** (a vs. b for %/6 h) | (a) 3.6 † (0.5) † % (b) 9.7 † (2.5) † % | DIT was significantly higher in adequate protein meal compared to low protein meal. |
| Riggs et al. [24] DIT = indirect calorimetry for 3.5 h; DIT measured every 30 min | 1841 kJ † (a) 23% CHO †††; 34% protein, 43% fat (b) 48% CHO †††; 28% protein, 24% fat | Overweight (a) 48.4 † (20.0) † kJ/h (b) 46.3 † (18.8) † kJ/h Normal weight (a) 43.1 † (19.2) † kJ/h (b) 31.0 † (19.2) † kJ/h Underweight (a) 20.0 † (16.4) † kJ/h (b) 24.2 † (15.6) † kJ/h ** (a vs. b for normal subjects for kcal/min/kg FFM) | Overweight (a) 2.6 † (0.2) † %/h (b) 2.5 † (1.0) † %/h Normal weight (a) 2.3 † (1.0) † %/h (b) 1.7 † (1.0) † %/h Underweight (a) 1.1 † (0.9) † %/h (b) 1.3 † (0.9) † %/h ** (a vs. b for normal subjects for %/3.5 h) | Significantly higher DIT for the high protein, high fat meal in normal weight subjects. | |
| Clegg et al. [17] DIT = ventilated hood indirect calorimetry for 6 h; measured for 15 min every 30 min | 1863 kJ 35.5% CHO, protein 19.9%, 44.6% fat | (a) 21.9 † (7.9) † kJ/h (b) 29.4 † (8.4) † kJ/h ** (a vs. b for kcal/6 h) | (a) 1.2 † (0.4) † %/h (b) 1.6 † (0.5) † %/h ** (a vs. b for %/6 h) | Pepper sunflower oil had a significantly lower DIT than pepper MCT oil intervention. | |
| Kasai et al. [14] study 1 DIT = indirect calorimetry Aeromonitor AE-300S; DIT measured for 6 h at 1 h intervals | (a) 1046 kJ † (b) 1029 kJ † (c) 1013 kJ † 43% CHO, 21% protein, 36% fat | (a) 8.4 † (4.6) † kJ/h or 0.1 † (0.07) † kJ/kg/h (b) 17.7 † (10.8) † kJ/h or 0.3 † (0.2) † kJ/kg/h (c) 19.5 † (14.1) † kJ/h or 0.3 † (0.2) † kJ/kg/h ** (a vs. b for cal/kg/6 h) ** (a vs. c for cal/kg/6 h) NS (b vs. c for cal/kg/6 h) | (a) 0.8 † (0.5) † %/h (b) 1.7 † (1.1) † %/h (c) 1.9 † (1.4) † %/h ** (a vs. b for %/5 h) ** (a vs. c for %/5 h) NS (b vs. c for kJ/5 h) | (a) 2.8 † (1.7) † % (b) 6.3 † (3.9) † % (c) 7.3 † (5.2) † % | Significant increase in DIT when a liquid meal containing MCT was consumed compared to a meal with LCT. |
| Kasai et al. [14] study 2 DIT = indirect calorimetry Aeromonitor AE-300S; DIT measured for 6 h at 1 h intervals | (a) 1059 kJ † (b) 1042 kJ † (c) 1020 kJ † (d) 1004 kJ †50% CHO, 10% protein, 40% fat | (a) 8.2 † (6.4) † kJ/h or 0.2 † (0.1) † kJ/kg/h (b) 14.0 † (5.7) † kJ/h or 0.3 † (0.1) † kJ/kg/h (c) 9.8 † (8.2) † kJ/h or 0.2 † (0.2) † kJ/kg/h d) 20.3 † (15.7) † kJ/h or 0.4 † (0.3) † kJ/kg/h * (a vs. b for cal/kg/6 h) * (c vs. d for cal/kg/6 h) | (a) 0.8 † (0.6) † %h (b) 1.3 † (0.5) † %h (c) 1.0 † (0.8) † %h (d) 2.0 † (1.6) † %h * (a vs. b for %/5 h) * (c vs. d for %/5 h) | (a) 3.9 † (3.0) † % (b) 6.8 †(2.7) † % (c) 4.7 † (3.9) † % (d) 10.5 † (7.9) † % | Significant increase in DIT in meals containing mayonnaise or margarine with MCT compared to LCT. |
| Casas-Agustench et al. [39] DIT = open circuit indirect calorimetry with a canopy system for 5 h continuously | Mean (95% CI) (a) 2655 (2510–2799) kJ, 36.4 (35.9–36.7)% CHO, 11.7 (11.4–11.9)% protein, 51.9 (95% CI 51.7–52.1)% fat (b) 2608 (2428–2788) kJ, 37 (95% CI 36.6–37.4)% CHO, 11.3 (95% CI 10.6–11.9)% protein, 51.7 (95% CI 51.3–52.0)% fat (c) 2599 (2421–2278) kJ, 37.1 (95% CI 36.4–37.7)% CHO, 11.2 (95% CI 10.8–11.6)% protein, 51.7 (95% CI 51.2–52.1)% fat | Mean (95% CI) (a) 37.2 † (29.5–44.8) † kJ/h (b) 36.8 † (30.5–43.0) † kJ/h (c) 30.0 † (24.2–35.8) † kJ/h * (a vs. b vs. c and a vs. c for kJ/5 h) | Mean (95% CI): (a) 1.4 † (1.1–1.7) † %/h (b) 1.4 † (1.2–1.7) † %/h (c) 1.2 † (0.9–1.4) † %/h | Mean (95% CI) (a) 12.3 (9.7–14.9)% (b) 11.8(9.7–13.9)% (c) 9.6 (7.7–11.4)% * (a vs. c and b vs. c for %AB) * (a vs. b vs. c for % AB) | DIT was significantly higher in PUFA and MUFA meals compared to SFA meal. |
| Piers et al. [18] DIT = open circuit ventilated hood canopy system for 5 h; DIT measured for 30 min periods each hour | 2500 † kJ 42% CHO, 15% of energy from protein, 43% fat | (a) 29.6 † (10) † kJ/h (b) 28.4 † (10) † kJ/h NS (a vs. b for kJ/5 h) | (a) 1.2 † (0.4) † %/h (b) 1.1 † (0.4) † %/h NS (a vs. b for %/5 h) | (a) 9.5 † (3.2) † % (b) 9.3 † (3.2) † % | No significant differences in DIT between SFA and MUFA meals. |
| Bendixen et al. [37] DIT = indirect calorimetry with open circuit, ventilated hood for 5 h continuously with 10 min breaks every hour | 4698 (550.2) † kJ, 34% CHO, 6% protein, 60% fat | (a) 61.8 † (15.2) † kJ/h (b) 72.8 † (19.0) † kJ/h (c) 69.2 † (11.4) † kJ/h (d) 65 † (13.9) † kJ/h * (a vs. b vs. c vs. d for kJ/5 h) ** (a vs. b for kJ/5 h) NS (All other pairwise comparison apart from a vs. b) | (a) 1.3 † (0.3) † %/h (b) 1.5 † (0.3) † %/h (c) 1.4 † (0.2) † %/h (d) 1.4 † (0.3) † %/h * (a vs. b vs. c vs. d for %/5 h) ** (a vs. b for %/5 h) NS (all other pairwise comparison apart from a vs. b) | (a) 21.3 † (5.2) † % (b) 25.1 † (6.6) † % (c) 23.7 † (3.9) † % (d) 22.4 † (4.8) † % | DIT was significantly higher in the three modified fat meals compared to the conventional fat meal. |
| Processed vs. unprocessed meals | |||||
| Barr and Wright [26] DIT = indirect calorimetry using spirometer and gas bags (a) 5.8 (0.11) h (b) 4.8 (0.23) h 2 min measurement by spirometer followed by 10 s exhalation for 5 or 6 breaths into a gas bag every hour | 2520 or 3360 kJ (a) 39% fat, 40% CHO, 20% protein (b) ½ sandwich: 33% fat, 49% CHO, 15% protein or 2 sandwiches: 33% fat, 50% CHO, 15% protein | (a) 99.4 † (40.7) † kJ/h (b) 63.9 † (35.6) † kJ/h *** (a vs. b kJ/5.8 and 4.8 h) | (a) 3.4 † (1.7) † %/h (b) 2.2 † (1.4) † %/h ** (a vs. b %/5.8 and %/4.8 h) | Whole food meal showed a significant higher DIT compared to processed meal. | |
| Bolus vs. smaller frequent meals | |||||
| Kinabo and Durnin [32]-Paper B DIT = open circuit indirect calorimetry using Douglas bag technique for 6 h; DIT measured for 10 min, every 10 min for the first 90 min and every 20 min for the last 90 min. | (a and c) 5040 kJ (b and d) 2520 × 2 kJ (a and b) 70% CHO, 11% protein, 19% fat (c and d) 24% CHO, 11% protein, 65% fat | Group A: (a) 62.8 † (13.2) † kJ/h (b) 63.5 † (11.7) † kJ/h Group B: (c) 59.3 † (11.5) † kJ/h (d) 56.7 † (8.0) † kJ/h NS (a vs. b and c vs. d for kJ/6 h) | Group A (a) 1.3 † (0.3) † %/h (b) 1.3 † (0.2) † %/h Group B (c) 1.2 † (0.25) † %/h (d) 1.1 † (0.2) † %/h | Group A (a) 28 (6.9) † % (b) 31 (5.0) † % Group B (c) 27 (7.8) † % (d) 28 (5.1) † % | No significant difference on DIT between meals consumed as bolus vs. two smaller frequent meals. |
| Vaz et al. [34] DIT = indirect calorimetry for 2 h; DIT measured every 30 min | (a) 3150 † (b) 1050 × 3 kJ † 53.3% CHO, 14.7% protein, 32% fat | (a) 71 † (31.5) † kJ/h (b) 52.3 † (15.3) † kJ/h NS (a vs. b for kJ/2 h) | (a) 2.3 † (1.0) † %/h (b) 1.7 † (0.49) † %/h | (a) 22.2%/h (b) NP | DIT was lower in the small frequent feeding regime compared to one bolus meal event – but not significantly different. |
| Allirot et al. [35] DIT = indirect calorimetry for 4 h; DIT measured for 30 min periods | (a) 2823.4 kJ † (b) total 2823.4 † divided in 705.8 † kJ meals 54.2 † % CHO, 6.3 † % Protein, 36.7 † % Fat | (a) 43.8 † (18.4) † kJ/h (b) 33.2 † (15.5) † kJ/h | (a) 1.6 † (0.7) † %/h (b) 1.2 † (0.6) † %/h * (a vs. b for %/4 h) | DIT was significantly higher when the meal consumed as one bolus event compared to four smaller isocaloric meals ingested over time in the morning. | |
| Tai et al. [27] DIT = indirect calorimetry for 5 h; DIT measured every 30 min | (a) one meal of 3138 kJ (b) 6 meals of 523 kJ 54.5% CHO, 14.0% protein, 31.5% fat | (a) 48.2 † (16.93) † kJ/h (b) 34.9 † (12.3) † kJ/h * (a vs. b for kJ/5 h) | (a) 1.5 † (0.5) † %/h (b) 1.1 † (0.4) † %/h | (a) 20.6 † (7.2) † % (b) 14.8 † (5.2) †% | DIT was significantly higher when the meal was consumed as a one bolus event compared to six smaller isocaloric meals ingested over time in the morning. |
| Fast vs. slow eating patterns | |||||
| Hamada et al. [28] DIT = gas analyzer AE-310S for 1.5 h continuously | 1255.2 † kJ, 42% CHO, 8% protein, 50% fat | (a) 19.5 † (142.2) † kJ/kg/h (b) 502.1 † (234.4) † kJ/kg/h * (a vs. b for kcal/kg/90 min) | Slowing eating was associated with a significant increase in DIT compared to rapid eating. | ||
| Toyama et al. [29] DIT = open-circuit indirect calorimetry for 3 h; first hour continuously, second and third hours measured for 15 min every 30 min intervals | 1464 kJ, 61.3% CHO, 16.4% protein, 22.3% fat | (a) 31.6 † (15) † kJ/kg/h (b) 41.9 † (14.6) † kJ/kg/h NS (a vs. b for kcal/kg/min) | (a) 6.8 (4.8)% (b) 8.5 (4.2)% | There was no significant difference in DIT between fast eating and regular eating. | |
| Palatable vs. unpalatable meals | |||||
| Sawaya et al. [19] DIT = ventilated hood indirect calorimetry, for 6 h; DIT measured for 10 min with 5 min breaks for the 6 h | 2930 kJ †, 65% CHO, 12% protein, 23% fat | (a) old 37.0 † (15.9) † kJ/h young 34.7 † (13.6) † kJ/h (b) old 46.4 † (18.4) † kJ/h young 39.5 † (17.0) † kJ/h | (a) old 1.3 † (0.5) † %/h young 1.2 † (0.5) † %/h (b) old 1.6 † (0.6) † %/h young 1.4 † (0.6) † %/h NS (a vs. b %/3 h) | (a) old 26.4 † (11.3) † % young 21.7 † (8.5) † % (b) old 34.6 † (13.7) † % young 24.8 † (10.6) † % | DIT did not significantly differ between palatable and unpalatable meals. |
| Weststrate et al. [16] study 1 DIT = ventilated hood indirect calorimetry for 3.5 h continuously | 2000 kJ †, NP % energy from macronutrient | (a) 47.3 † (14.2) † kJ/h (b) 52.9 † (13.3) † kJ/h NS (a vs. b for kJ/3.5 h) | (a) 2.4 † (0.7) † %/h (b) 2.6 † (0.7) † %/h NS (a vs. b for %/3.5 h) | There was not a significant difference in DIT between palatable and unpalatable meals. | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quatela, A.; Callister, R.; Patterson, A.; MacDonald-Wicks, L. The Energy Content and Composition of Meals Consumed after an Overnight Fast and Their Effects on Diet Induced Thermogenesis: A Systematic Review, Meta-Analyses and Meta-Regressions. Nutrients 2016, 8, 670. https://doi.org/10.3390/nu8110670
Quatela A, Callister R, Patterson A, MacDonald-Wicks L. The Energy Content and Composition of Meals Consumed after an Overnight Fast and Their Effects on Diet Induced Thermogenesis: A Systematic Review, Meta-Analyses and Meta-Regressions. Nutrients. 2016; 8(11):670. https://doi.org/10.3390/nu8110670
Chicago/Turabian StyleQuatela, Angelica, Robin Callister, Amanda Patterson, and Lesley MacDonald-Wicks. 2016. "The Energy Content and Composition of Meals Consumed after an Overnight Fast and Their Effects on Diet Induced Thermogenesis: A Systematic Review, Meta-Analyses and Meta-Regressions" Nutrients 8, no. 11: 670. https://doi.org/10.3390/nu8110670