3. Results
A total of 2118 female and male subjects from six different European countries with a mean age of 55 (range 35–74) years were studied for demographic characteristics, dietary habits, and plasma carotenoids, tocopherols, and retinol (
Table 1). Subjects in the higher age groups were shorter (
p < 0.001), while weight was similar throughout the age groups; thus, the mean BMI as well as the prevalence of overweight and obesity were higher in the higher age groups. Furthermore, subjects in the higher age groups were less likely to be current smokers.
The evaluation of frequencies of reported intake of fruit, vegetables, and use of vitamin supplements (assessed by chi-squared test,
Table 2) revealed the following: intake of fruit (≥1 serving/day) and vegetables (≥1 serving/day) were higher in women than in men (72% vs. 56%, and 69% vs. 51%, for fruit and vegetables, respectively, both
p < 0.001) as well as in non-smokers compared to smokers (68% vs. 47% and 62% vs. 50%, for fruit and vegetables, respectively, both
p < 0.001). The same is true for the frequencies of reported use of vitamin supplements (≥1 supplement/week) which were also higher in women than in men (22% vs. 17%,
p = 0.002) and in non-smokers compared to smokers (21% vs. 15%,
p = 0.019).
The daily consumption of fruit and juice were higher and the weekly meat consumption was lower with higher age. The frequencies of reported use of vitamin supplements (≥1 supplement/week) differed between countries (p < 0.001), being high in Germany (24%), Poland (23%), and Austria (23%) followed by Belgium (19%), Italy (15%), and Greece (14%). Also, frequencies of reported dietary intake differed between countries (p < 0.001): Fruit consumption was high in Italy and in Belgium where 78% and 66% of subjects, respectively, reported an intake of ≥1 serving of fruit/day; subjects from these countries also reported a high intake of vegetables (80% from Italy and 85% from Belgium with ≥1 serving of vegetables/day); French fries were frequently eaten in Belgium (40% of subjects reporting ≥1 serving/week) and Greece (26% of subjects with ≥1 serving/week), and meat consumption (≥1 serving/day) was high in Poland (30% of subjects) and Belgium (22% of subjects).
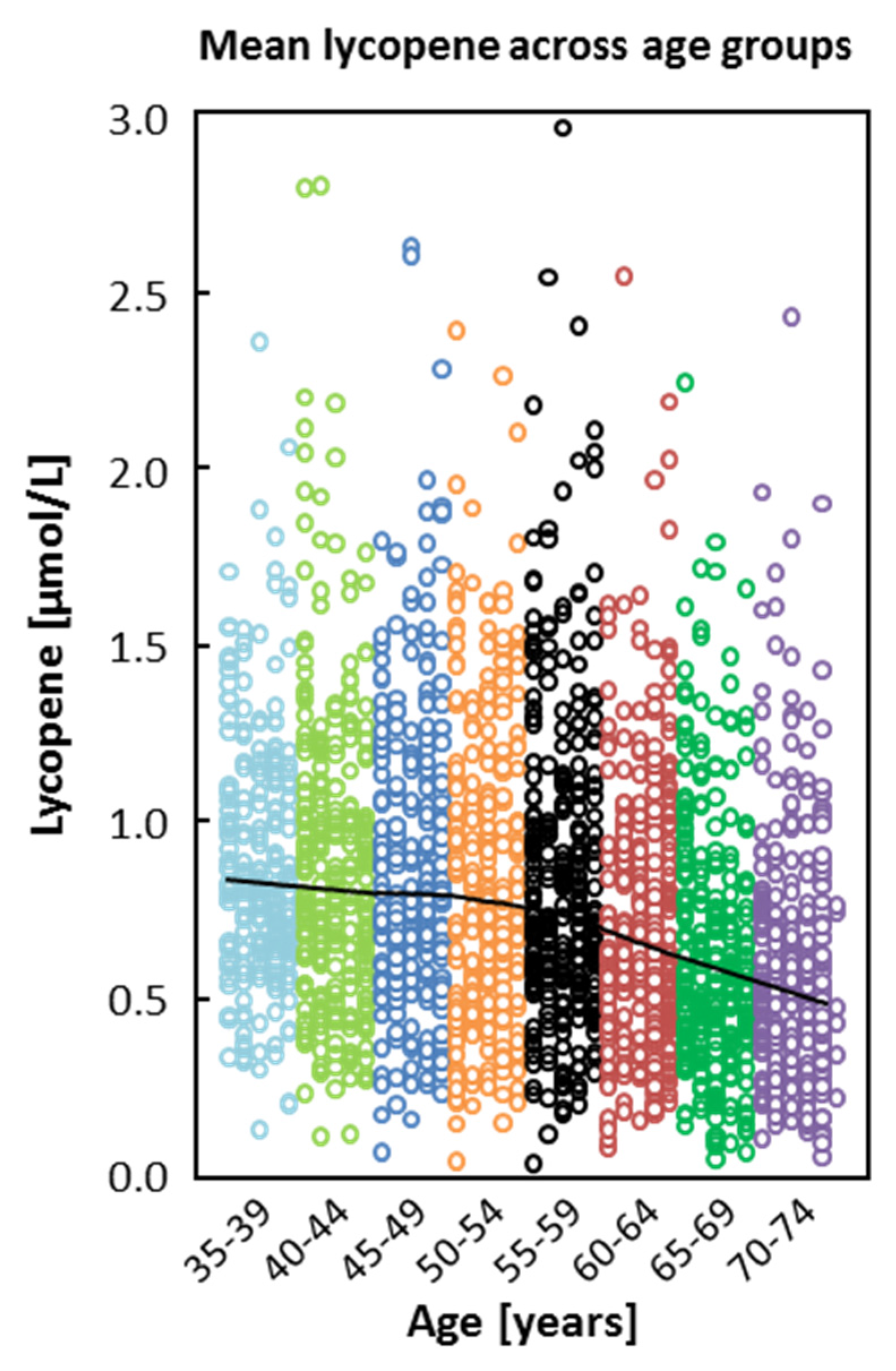
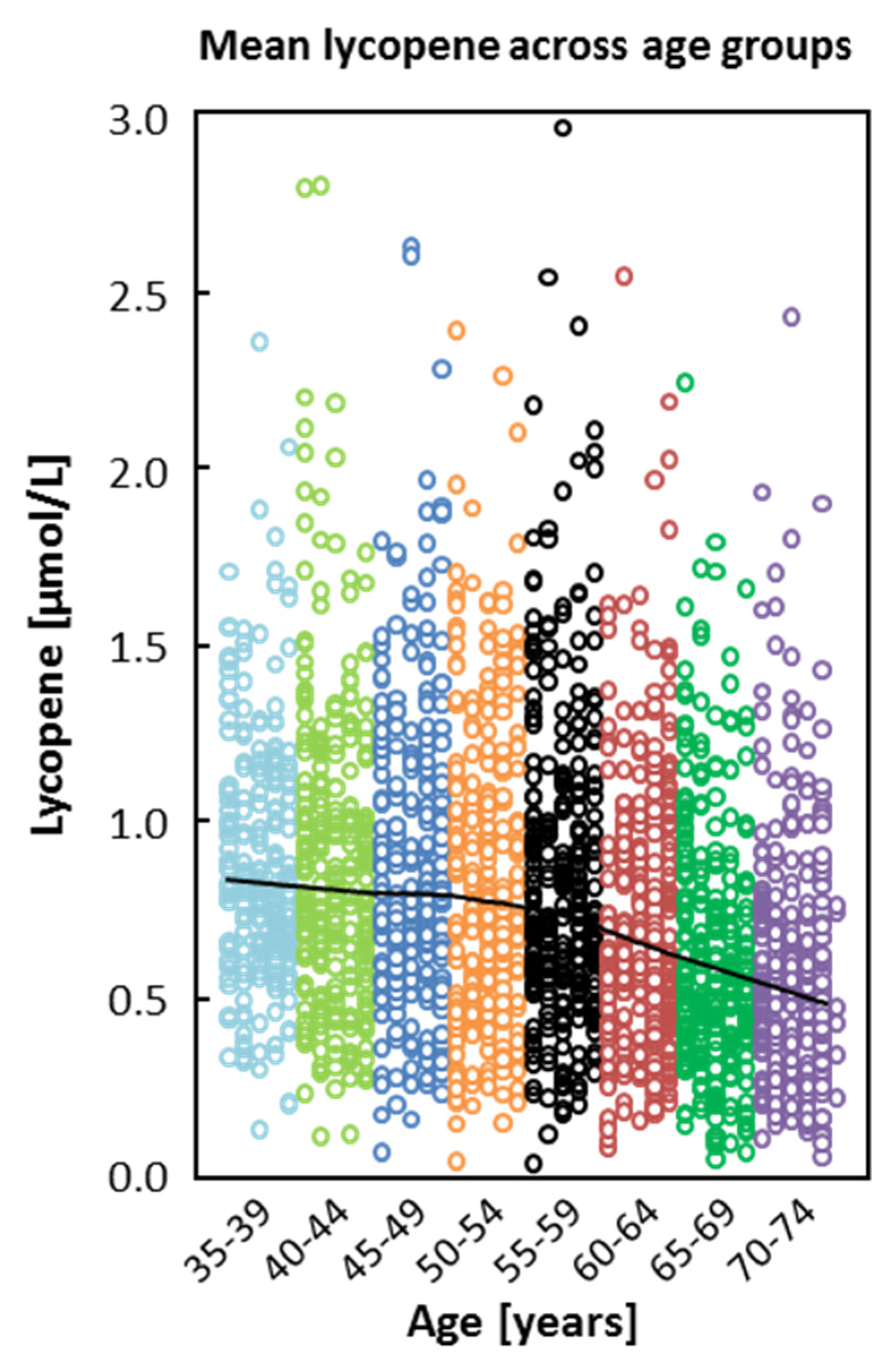
Lycopene showed the highest mean concentrations of plasma carotenoids, and except for β-carotene, all carotenoids, tocopherols, and retinol were statistically significantly associated with age (
Table 3). Lycopene and α-carotene were inversely correlated with age, whereas β-cryptoxanthin, lutein, zeaxanthin, α-/γ-tocopherol, and retinol were positively correlated with age (
Table 3).
These associations were confirmed in multivariable regression models (
Table 4), which revealed inverse associations of age with lycopene (
r = −0.248) and α-carotene (
r = −0.112), and positive associations with α-tocopherol (
r = 0.208), and β-cryptoxanthin (
r = 0.125) (all
p < 0.001). Cholesterol was positively associated with all carotenoids, tocopherols, and retinol (all
p < 0.001), but was not correlated with age when simultaneously assessed as a covariate with biomarkers in the forward regression model. The multiple regression model (forward approach) with cholesterol-adjusted compounds also confirmed lycopene (
r = −0.256), α-tocopherol (
r = 0.157), α-carotene (
r = −0.128), and β-cryptoxanthin (
r = 0.117) as those markers with a statistically significant association with age (
Table 4) in our study population.
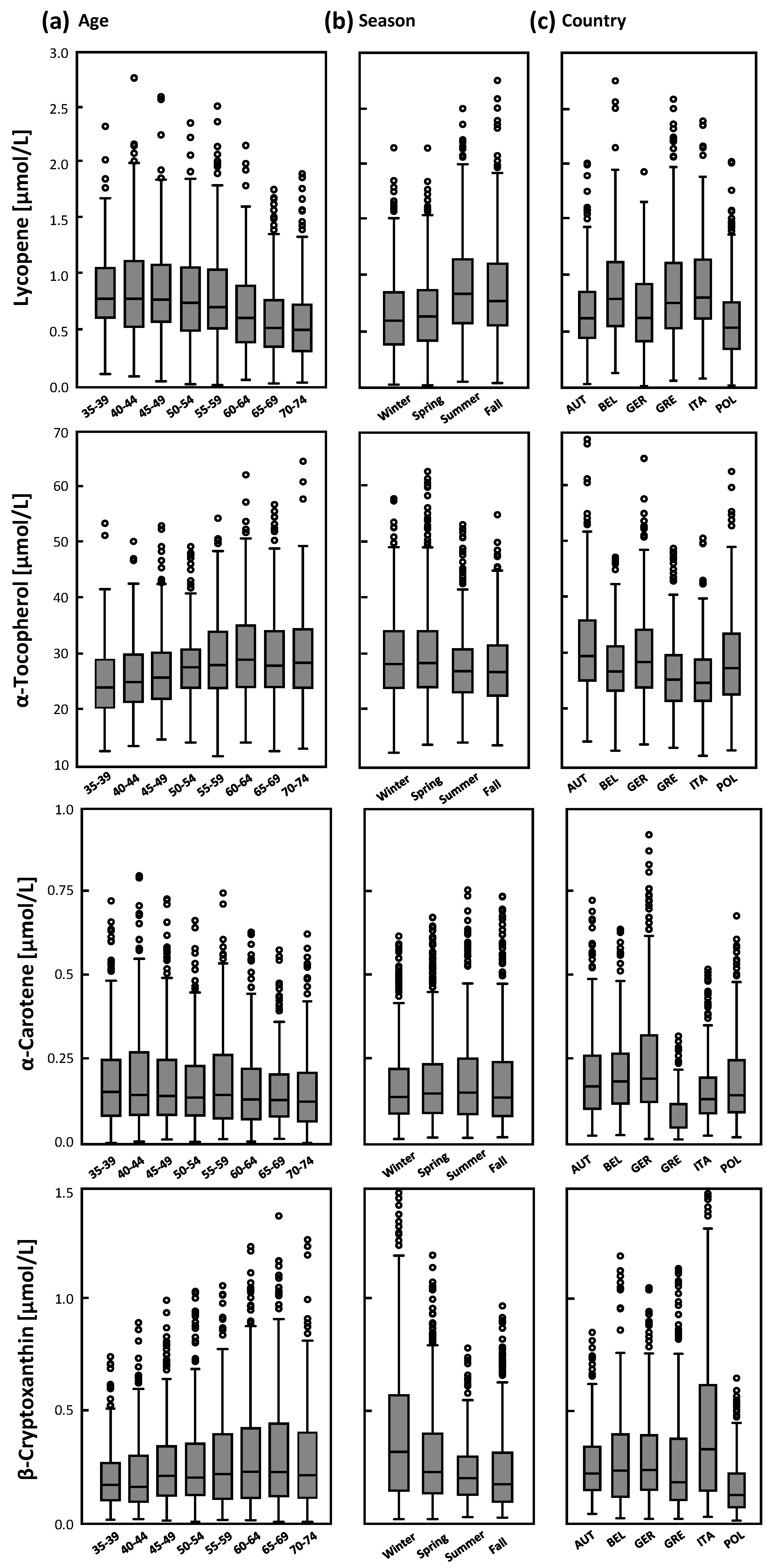
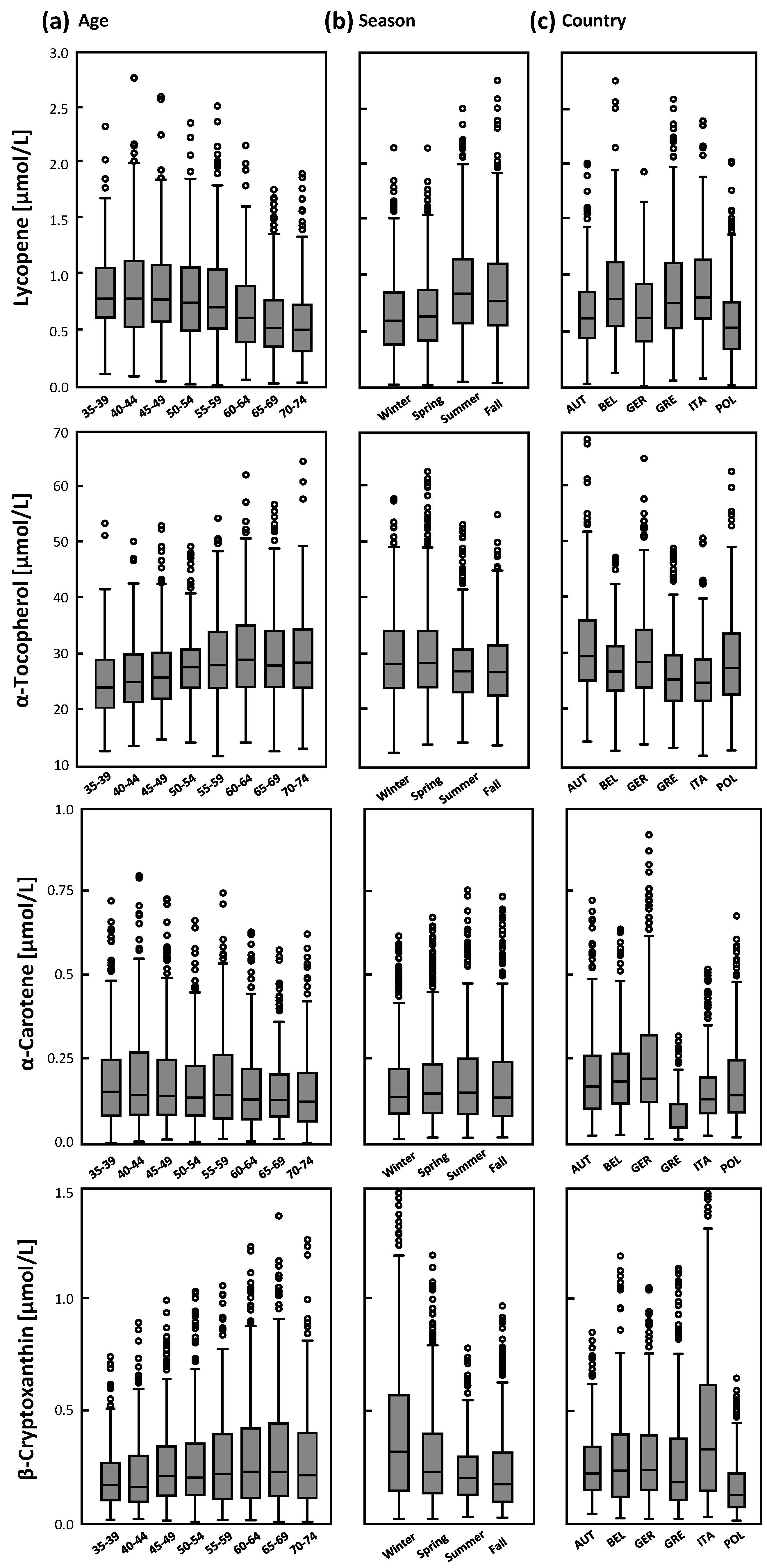
Lycopene, α-tocopherol, β-cryptoxanthin, and α-carotene were predicted by age group, country (study center), season, and cholesterol (
Table A1 and
Figure 1). In addition, gender, smoking status, BMI, and dietary habits were statistically significantly associated with these plasma biomarkers. The associations of age with lycopene and α-tocopherol are shown in
Figure 1 and
Figure 2. Plasma biomarkers were cross-sectionally associated with age groups, season, and country (
Table A1 and
Figure 2); higher mean lycopene concentrations were found in subjects from Belgium, Greece, and Italy than in subjects from the other countries, which is in agreement with the high fruit and vegetable consumption but also high intake of French fries in these countries. Regarding season, lycopene was higher in summer (and fall) and both mean α-tocopherol and β-cryptoxanthin were higher in winter (
Figure 2b).
Cholesterol was highly and positively associated with α-tocopherol (
ηp2 = 0.266;
Table A1).
Lower plasma lycopene was associated with overweight and/or obesity, use of vitamin supplements, daily fruit and high frequency in juice consumption, never consuming French fries and seldom but also daily meat servings. The frequent consumption of fruit or vegetables (≥ 2 servings/day) was highly predictive for higher β-cryptoxanthin and α-carotene (
Table A1).
The association of lower plasma lycopene with higher age (−0.046 µmol/L or 6.5%) remained after adjusting for co-factors and covariates (
Table 5). The age groups also had a high impact on lycopene (
ηp2 = 0.080,
Table 6) as did cholesterol; male gender was positively whereas BMI was inversely associated with lycopene in the multiple linear regression model. The association of higher α-tocopherol with age remained after adjusting for country and season, and remained if all covariates were assessed (0.486 vs. 0.667 µmol/L (1.7% vs. 2.4%)) (
Table 5); cholesterol explained most of variance in α-tocopherol (
ηp2 = 0.336), followed by age group, vitamin supplement use, and juice consumption (
Table 6). The inverse association of α-carotene with age remained statistically significant even after adjusting for all covariates (
Table 5); cholesterol, vegetable and fruit consumption, and female gender were positively while BMI, smoking, and age group were inversely associated with plasma α-carotene in the multiple regression model (
Table 6).
4. Discussion
The present study demonstrates that plasma carotenoids, tocopherol, and retinol are related to age in a healthy European age-stratified population. For lycopene, α-tocopherol, β-cryptoxanthin, and α-carotene these associations remained even after adjusting for cholesterol, BMI, dietary habits (intake of fruit, vegetables, juice, and meat), use of vitamin supplements, gender, smoking status, country, and season. The reported higher frequency of vitamin supplement use, and fruit and vegetable intake among females and non-smokers is consistent with statistically significantly higher plasma α-tocopherol, β-cryptoxanthin, and α-carotene. Higher fruit and vegetable intake with corresponding higher plasma carotenoids in females than in males was previously reported in younger and elderly populations [
25,
26,
27]. Because the intake of fruit is related to higher plasma β-cryptoxanthin, frequent intake of fruit in the higher age groups most likely contributed to higher β-cryptoxanthin with age. The main dietary sources of β-cryptoxanthin are orange fruits and their products, e.g., juice [
28]. However, the season and thus the availability of fruit and vegetables as well as differences in dietary habits between countries are important predictors of plasma carotenoids; season and country are also known to have a strong influence on plasma carotenoids [
11,
12,
15,
29].
Associations of individual plasma carotenoids and tocopherols with age have previously been described [
16,
17,
18,
30]. Our results confirm those of a small sub-cohort (
n = 272) of the U.S. Health Professional Follow-up and the Nurses’ Health Study, which revealed that plasma lycopene was inversely correlated with age in men and β-cryptoxanthin was positively associated with age in women (mean age: 54 years) [
16]. Age was positively associated with serum concentrations and dietary intake of all carotenoids except with lycopene in the Nutritional Factors in Eye Disease Study (mean age 65 ± 9 years) [
17]. Lycopene was inversely associated with age and the only carotenoid showing a statistically significant correlation with age after adjusting for gender, smoking status, BMI, supplement use, and serum cholesterol [
17], in agreement with our results. In our study not only lycopene but also α-carotene was negatively associated with age. For α-carotene our study is the first to show statistically significantly lower plasma α-carotene concentrations with higher age in an age-stratified group of men and women; however, the reason for the lower α-carotene concentrations cannot be explained by our data on dietary habits. Since plasma α-carotene is reduced in the higher age groups in both genders, the lower α-carotene concentration in men compared to women (
Table 6 and
Table A1) does not explain this finding. Two studies showing a statistically significant positive association of plasma α-carotene with age, carried out in the United States [
17] and in Venezuela [
18], do not show an altered dietary intake in the higher age groups and are therefore not able to explain the higher plasma α-carotene concentrations with a higher consumption of fruit/vegetables in these individuals.
The study in Venezuela, among 35–69-year-old women (
n = 718) and men (
n = 646), also showed higher plasma β-carotene and β-cryptoxanthin with higher age among women, but lower plasma lycopene with higher age in both men and women [
18]; the frequency of fruit and vegetable intake was statistically significantly associated with plasma lycopene. In the Framingham Heart Study, lycopene concentration, in contrast to all other carotenoids, was lower with age (as an independent factor besides BMI, cholesterol, smoking, and dietary intake of fruit, vegetables, juice, French fries, and meat) and use of vitamin supplements, and was lowest among subjects >85 years [
30]. Dietary carotene intake and plasma α-tocopherol, β-cryptoxanthin, and α-/β-carotene were lower in men (
n = 230; 67–96 years) than in women (
n = 408; 68–94 years) [
30]. In a sub-sample (
n = 2969) within the European multicenter study EPIC following an age-stratified sampling schema (five-year groups; 45–64 years) plasma lycopene was lower with age in both men and women, and higher in summer when tomatoes are available [
11]. All these previous studies and our results point to lower plasma lycopene concentrations with higher age.
The question arising is whether (a) changes in diet; (b) reduced bioavailability; or (c) different storage patterns in various organs during aging are responsible for the changes observed in older subjects in the present study.
Various factors influence the circulating concentrations and bioavailability of micronutrients, including lifestyle, metabolism, energy intake, food preparation, fat intake (plasma lipid concentration), and interactions between nutrients and drugs [
31,
32]. In the NHANES study with 3413 participants aged 17–90 years, race, supplement use, alcohol consumption, BMI, blood pressure, and consumption of non-tomato vegetables, fruit, and juices were not associated with serum lycopene, whereas age, gender, region, smoking, serum cholesterol and triacylglycerol, and dietary intake of fat, tomatoes, pizza, and pasta were statistically significant determinants of serum lycopene [
33]. In fact, multivariate-adjusted serum lycopene concentrations (adjusted for sex, geographical location, race/ethnicity, age, education, poverty income ratio, vitamin/mineral supplement use, alcohol consumption, serum cotinine, BMI, serum total cholesterol, serum triacylglycerol, and dietary intake of fat, tomatoes, non-tomato vegetables, fruit and juices, pizza, and pasta as categorical independent covariates) were 48.3% lower in people over 70 years than in those younger than 30 years (
p < 0.0001) [
33].
An age-related decrease in lycopene absorption resulting in reduced lycopene concentrations in older subjects has been previously observed [
33,
34]. Since lycopene is absorbed primarily from tomatoes and tomato products, it is plausible that specific groups (e.g., men, younger subjects, subjects from Italy or Belgium), who consume relatively more tomato-based products (e.g., ketchup and tomato sauce) have higher plasma lycopene than other groups. Other studies demonstrated that older persons were likely to consume less dietary fat and fewer processed tomato products, which were stated to cause heartburn [
33,
34]. In terms of bioavailability, only lycopene but not α-carotene, β-carotene, and lutein showed a statistically significantly lower response (−40%,
p < 0.04), as demonstrated in old compared to young subjects [
34], implying that the bioavailability of lycopene in the elderly is impaired. This effect on the carotenoid bioavailability appeared to be independent of the food matrix (tomato) because the standardized β-carotene response for a tomato-containing meal did not differ between the two groups [
34].
The bioavailability of lycopene could be, unlike other carotenoids, more dependent on age-related changes such as the physicochemical conditions of the gastrointestinal tract [
35,
36] in view of the fact that the absorption efficiency of lycopene is very low [
37]. The combination of physiological, behavioral, and lifestyle factors is most likely responsible for the different plasma carotenoid concentrations [
17].
Nevertheless, storage effects need to be considered, especially in obese persons, where a weak correlation between intake and concentrations of carotenoids in adipose tissues was observed [
38]. Carotenoids are lipophilic substances stored in the adipose tissue, which could explain their inverse association with BMI [
17,
39,
40]. Serum α-/β-carotene, β-cryptoxanthin, and lutein/zeaxanthin but not lycopene were inversely associated with BMI [
17]. This change in serum carotenoids (over seven years) was inversely associated with the change in BMI among young non-smokers (25 ± 3.6 years, 45% male, 56% white) from the CARDIA study [
39]. The authors also suggest that the oxidative stress associated with higher BMI may have caused lower carotenoid concentrations. Serum β-carotene was negatively associated with both general and central adiposity, whereas serum α-tocopherol was positively associated with central adiposity [
40].
The limitations of the study include the rather basic information on dietary habits. For instance, only the self-reported frequency (given in ‘per week’ or ‘per day’) of consumption for glasses of juice (not specified which kind), supplement use (not specified), meat consumption, French fries, fruit, and vegetables were collected. Another limitation is that the questionnaires did not ask for individual food items within the food groups (i.e., tomatoes or oranges). This information might have strengthened our suggestions of independent associations of micronutrients with age. We focused mainly on those food groups that are relevant regarding associations of plasma concentrations with age, i.e., plasma β-cryptoxanthin and fruit, or lycopene and vegetables. The cross-sectional design may reflect only occasional dietary intake; nevertheless, knowledge of the season partly corrects for the influence of a different availability of fruit and vegetables and therefore plasma carotenoid concentrations in the multivariable models. The assessment of dietary intake was not the main focus of the project but did give valuable information on dietary habits that correlate well with the parameters analyzed in plasma samples. The questionnaires were standardized, meaning that one questionnaire was uniformly used for all subjects recruited. It was drafted in English and translated into each national language. The results from our study confirm that persons with higher intakes of fruit or vegetables have higher levels of plasma β-cryptoxanthin and α-carotene. Whether this association persists into later life remains to be assessed in specific studies involving a higher number of older individuals.
The continuous age distribution from 35 to 74 years and the equal number of men and women included in the study are a feature distinguishing this study from others. Furthermore, the samples of this large European multicenter study were collected from fasting subjects. Potential confounding factors were assessed, and samples were distributed in a blinded manner to guarantee unbiased measurement and interpretation. The analyses of plasma micronutrients as well as cholesterol were carried out in a single laboratory each, with internal quality controls so that inter-laboratory variation can be excluded.
Our models in the present study suggest an independent inverse association of α-carotene and lycopene with age because these associations remained in multivariate models adjusted for multiple covariates including dietary habits (intake of fruit, vegetables, juice, and meat, and vitamin supplement use).
We conclude for the present study that age was inversely associated with lycopene and α-carotene but positively with α-tocopherol in both women and men from different European countries. These relations hold true after adjusting for well-known factors affecting plasma concentrations of carotenoids and tocopherols such as season, country, smoking status, gender, use of vitamin supplements, and intake of fruit, and vegetables. The lower plasma lycopene and α-carotene with age may be due to a combination of several effects including change of dietary habits, lifestyle, impaired bioavailability of nutrients, storage pattern, and/or increased demand of antioxidants with age.

 ,
, 

{kind=link}
{kind=link}