Development and Evaluation of a Home Enteral Nutrition Team

Abstract
:1. Introduction
2. Materials and Methods
2.1. Team Development
2.2. Team Aim and Objectives
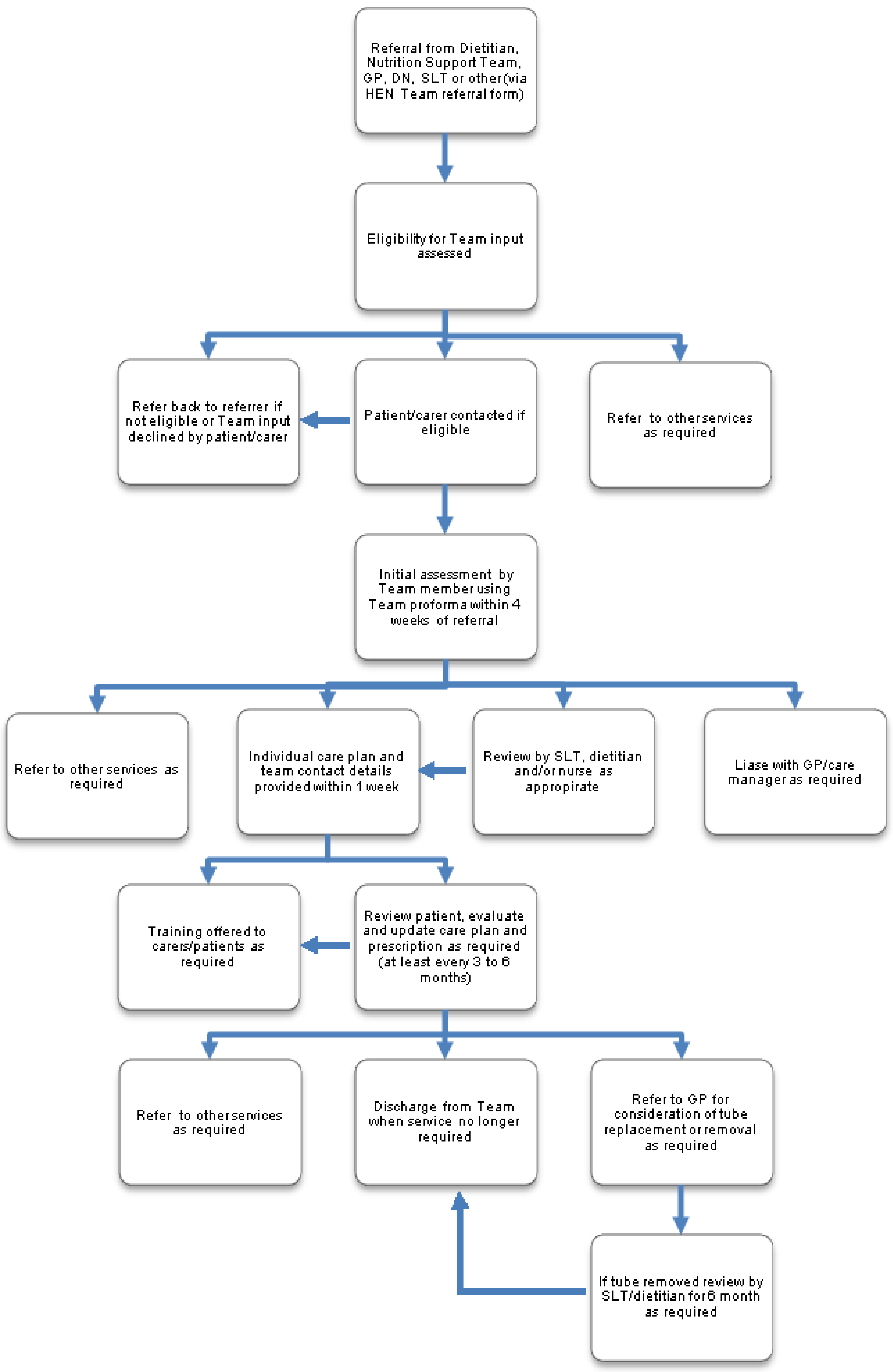
2.2.1. Objective: Development of a Care Pathway and Links with Other Services
2.2.2. Objective: Care Provision with Reference to NICE Guidelines [8,9]
- Review of use of feed ancillaries (giving sets, syringes, connectors, replacement parts), feed, thickener prescription and adjustment of plan of care if required on admission to the service and at least 6 monthly subsequently
- Review of stoma and tube and adjustment of plan of care if required
- Repair of tube as required
- Planned and emergency balloon-retained gastrostomy tube replacement at home where not clinically contraindicated
- Review of type of balloon-retained gastrostomy tubes and change to longer-lasting tubes requiring fewer balloon volume checks where possible
- Review of route and preparation of medication and suggestions for change if appropriate
2.2.3. Objective: Provision of Specialist Advice, Training and Education

2.2.4. Service Evaluation
2.2.5. Outcomes Included
- Number of patients whose risk of malnutrition decreased (measured using the Malnutrition Universal Screening Tool (MUST) [15])
- Number of patients, carers, healthcare staff and nursing home trained in gastrostomy tube care
- Number of patients who had tubes removed
- Estimates of cost of:
- ○
- enteral feed prescription
- ○
- thickening agents for dysphagia
- Frequency and length of hospital admission and hospital transport costs for ETF related problems for 28 patients in the caseload.
2.3. Statistical Analysis
2.4. Ethics and Governance
3. Results
3.1. Caseload Characteristics

{kind=link}
| Dietitian | Speech and Language Therapist | Nurse | TOTAL | |
|---|---|---|---|---|
| Number of contacts | 241 | 187 | 167 | 595 |
3.2. Must Score
3.3. Training
3.4. Number of Patients Who Had Tubes Removed
3.5. Estimated Cost Savings
| Component of provision | Calculation of estimated costs | Pre introduction estimated cost (2011) | Post introduction estimated cost (2012) | Estimated Cost differential |
|---|---|---|---|---|
| Enteral feed prescription per year | 2011: mean cost of feed £9.18 per patient per day 2012: mean cost of feed £7.41 per patient per day | £234,505 | £189,326 | £45,179 |
| Thickening agents for dysphagia | 2011: daily thickener costs per patient £0.53 2012: daily thickener costs per patient £0.48 | £13,542 | £12,264 | £1,278 |
3.6. Patient Satisfaction Survey
| Costs component | Calculation of estimated saving | Pre-introduction estimated cost (mean per year) | Post-introduction estimated cost (2012) | Estimated cost differential |
|---|---|---|---|---|
| Hospital admission (frequency and bed days) for balloon gastrostomy tube replacement and tube related problems | 2010/2011:
2012:
| £82,943 | £18,602 | £64,341 |
| Hospital transport for balloon gastrostomy tube replacement in hospital and tube related problems | 2010/2011: Transport based on 25 admissions and 10 day cases 2012: Transport based on 7 hospital admissions and 2 day cases | £976 | £502 | £474 |
4. Discussion
4.1. Limitations
4.2. Practice Recommendations
5. Conclusion
Acknowledgements
Author Contributions
Conflicts of interest
References
- Russell, C.A.; Rollins, H. The needs of patients requiring home enteral tube feeding. Prof. Nurs. 2002, 17, 500–502. [Google Scholar]
- British Association of Enteral and Parenteral Nutrition. Annual BANS Report; Smith, T., Ed.; The British Association for Parenteral and Enteral Nutrition: Redditch, UK, 2011; pp. 1–50. Available online: http://www.bapen.org.ukn (accessed on 18 February 2015).
- Kurien, M.; White, S.; Simpson, G.; Grant, J.; Sanders, D.S.; McAlindon, M.E. Managing patients with gastrostomy tubes in the community: Can a dedicated enteral feed dietetic service reduce hospital readmissions? Eur. J. Clin. Nutr. 2012, 66, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Bjuresäter, K.; Larsson, M.; Athlin, E. Struggling in an inescapable life situation: Being a close relative of a person dependent on home enteral tube feeding. J. Clin. Nurs. 2012, 21, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.; Philpin, S.; Warring, J.; Cheung, W.Y.; Williams, J. Percutaneous endoscopic gastrostomies: the burden of treatment from a patient perspective. J. Adv. Nurs. 2006, 56, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Blomberg, J.; Lagergren, P. Patients’ perspectives of living with a percutaneous endoscopic gastrostomy (PEG). BMC Gastroenterol. 2012, 12, 126. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence. Infection: Prevention and control of healthcare-associated infections in primary and community care; NICE: London, UK, 2012; pp. 1–47. [Google Scholar]
- National Institute for Health and Clinical Excellence. Quality standard for nutrition support in adults; NICE: Manchester, UK, 2012; pp. 1–33. [Google Scholar]
- National Institute for Health and Clinical Excellence. Nutritional Support in Adults: Oral Nutrition Support, Enteral Tube Feeding; NICE: London, UK, 2006; pp. 1–49. [Google Scholar]
- Green, S.; Dinenage, S.; Gower, M.; Van Wyk, J. Home enteral nutrition: Organisation of services. Nurs. Older People 2013, 25, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Majka, A.J.; Wang, Z.; Schmitz, K.R.; Niesen, C.R.; Larsen, R.A.; Kinsey, G.C.; Murad, A.L.; Prokop, L.J.; Murad, M.H. Care coordination to enhance management of long-term enteral tube feeding: A systematic review and meta-analysis. J. Parenter. Enter. Nutr. 2014, 38, 40–52. [Google Scholar] [CrossRef]
- Hall, B.T.; Englehart, M.S.; Blaseg, K.; Wessel, K.; Stawicki, S.P.; Evans, D.C. Implementation of a dietitian-led enteral nutrition support clinic results in quality improvement, reduced readmissions, and cost savings. Nutr. Clin. Prac. 2014, 29, 649–655. [Google Scholar] [CrossRef]
- Omorogieva, O.; Patel, I. Home enteral nutrition and team working. J. Community Nurs. 2012, 26, 15–18. [Google Scholar]
- Klek, S.; Szybinski, P.; Sierzega, M.; Szczepanek, K.; Sumlet, M.; Kupiec, M.; Koczur-Szozda, E.; Steinhoff-Nowak, M.; Figula, K.; Kowalczyk, T.; et al. Commercial enteral formulas and nutrition support teams improve the outcome of home enteral tube feeding. JPEN 2011, 35, 380–385. [Google Scholar] [CrossRef]
- British Association for Parenteral and Enteral Nutrition. Introducing “MUST”. Available online: http://www.bapen.org.uk/screening-for-malnutrition/must/introducing-must (accessed on 18 February 2015).
- Department of Health. Valuing People: A New Strategy for Learning Disability for the 21st Century. Department of Health: London, UK, 2001; pp. 1–142. [Google Scholar]
- McLaughlin, K.A. Home sweet home-can future enteral tube feeding for motor neurone disease begin in the community. CN 2014, 14, 35–37. [Google Scholar]
- Care Quality Commission. Essential Standards of Quality and Safety. Care Quality Commission: London, UK, 2010; pp. 1–278. [Google Scholar]
- Bermange, J.; Stewart, K. Measuring clinical outcomes in a community home enteral feeding team. CN 2013, 13, 50–52. [Google Scholar]
- Lämås, K.; Willman, A.; Lindholm, L.; Jacobsson, C. Economic evaluation of nursing practices: A review of literature. Int. Nurs. Rev. 2009, 56, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Blomberg, J.; Lagergren, J.; Martin, L.; Mattsson, F.; Lagergren, P. Complications after percutaneous endoscopic gastrostomy in a prospective study. Scan. J. Gastroenterol. 2012, 47, 737–742. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dinenage, S.; Gower, M.; Van Wyk, J.; Blamey, A.; Ashbolt, K.; Sutcliffe, M.; Green, S.M. Development and Evaluation of a Home Enteral Nutrition Team. Nutrients 2015, 7, 1607-1617. https://doi.org/10.3390/nu7031607
Dinenage S, Gower M, Van Wyk J, Blamey A, Ashbolt K, Sutcliffe M, Green SM. Development and Evaluation of a Home Enteral Nutrition Team. Nutrients. 2015; 7(3):1607-1617. https://doi.org/10.3390/nu7031607
Chicago/Turabian StyleDinenage, Sarah, Morwenna Gower, Joanna Van Wyk, Anne Blamey, Karen Ashbolt, Michelle Sutcliffe, and Sue M. Green. 2015. "Development and Evaluation of a Home Enteral Nutrition Team" Nutrients 7, no. 3: 1607-1617. https://doi.org/10.3390/nu7031607