A Multi-Center Assessment of Nutrient Levels and Foods Provided by Hospital Patient Menus

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Nutritional Analysis
2.3. Statistical Analysis
3. Results

{kind=link}
| Regular Menus | Carbohydrate-Controlled Menus | 3000 mg Menus | 2000 mg Menus | |||||
|---|---|---|---|---|---|---|---|---|
| Standard (n = 21) | Standard Range | Standard (n = 21) | Standard Range | Standard (n = 21) | Standard Range | Standard (n = 21) | Standard Range | |
| Calories (kcal) | 1673 ± 362 | 1296–3007 | 1808 ± 175 | 1516–2067 | 1600 ± 210 | 1281–2168 | 1687 ± 228 | 1342–2091 |
| Protein (g) | 63 ± 9 b | 49–86 | 77 ± 10 a | 61–96 | 66 ± 22 | 52–159 | 67 ± 14 | 51–102 |
| % Total Energy from Protein | 18 ± 5 | 12–31 | 22 ± 9 | 14–38 | 19 ± 5 | 13–29 | 18 ± 4 | 13–28 |
| <10% of kcal [5] | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Protein (g/kg) e | 0.9 ± 0.1 b | 0.7–1.2 | 1.1 ± 0.1 a | 0.9–1.4 | 1.0 ± 0.3 | 0.7–2.3 | 1.0 ± 0.2 | 0.7–1.5 |
| Fat (g) | 52 ± 13 | 30–83 | 61 ± 8 c,d | 48–76 | 48 ± 13b | 28–73 | 50 ± 14b | 33–74 |
| % Total Energy from Fat | 28 ± 3 | 21–34 | 30 ± 3 c,d | 25–35 | 26 ± 5b | 18–34 | 26 ± 4b | 20–32 |
| >35% of kcal [5] | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Carbohydrate (g) | 240 ± 60 | 193–483 | 242 ± 24 | 206–295 | 226 ± 23 | 191–278 | 246 ± 26 | 202–288 |
| % Total Energy from Carbohydrate | 57 ± 3 b | 52–64 | 54 ± 3 a,d | 47–58 | 57 ± 6 | 38–68 | 59 ± 5b | 50–68 |
| <45% of kcal [5] | 0 (0%) | 0 (%) | 1 (5%) | 0 (0%) | ||||
| Sodium (mg) | 2896 ± 606 b,c,d | 1746–4531 | 3406 ± 544 a,c,d | 2532–4425 | 2401 ± 389 a,b,d | 1755–3487 | 1504 ± 296 a,b,c | 1114–2149 |
| Fiber (g) | 17.6 ± 4.2 | 10.6–24.0 | 25.1 ± 4.9 | 18.0–33.3 | 17.0 ± 4.4 | 10.6–27.1 | 19.2 ± 6.6 | 10.0–34.1 |
| <30g | 14 (100) | 10 (71) | 14 (100%) | 13 (93%) | ||||
| Cholesterol (mg) | 282 ± 133 | 131–496 | 333 ± 136 | 136–498 | 295 ± 185 | 111–641 | 148 ± 80 | 58–359 |
| Vitamin C (mg) | 106 ± 75 | 11–248 | 114 ± 60 | 27–236 | 106 ± 74 | 7–214 | 107 ± 75 | 21–215 |
| <75 mg | 6 (43%) | 2 (14%) | 6 (43%) | 7 (50%) | ||||
| Iron (mg) | 11.9 ± 4.2 | 6.3–22.3 | 12.7 ± 2.9 | 8.2–17.2 | 11.7 ± 3.0 | 7.9–17.7 | 11.7 ± 2.9 | 7.6–16.2 |
| <6 mg | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | ||||
| Calcium (mg) | 682 ± 148 | 469–1002 | 1086 ±174 | 845–1375 | 658 ± 121 | 512–917 | 547 ± 145 | 367–920 |
| <1000 mg | 13 (93%) | 6 (43%) | 14 (100%) | 14 (100%) | ||||
3.1. Other Nutrients
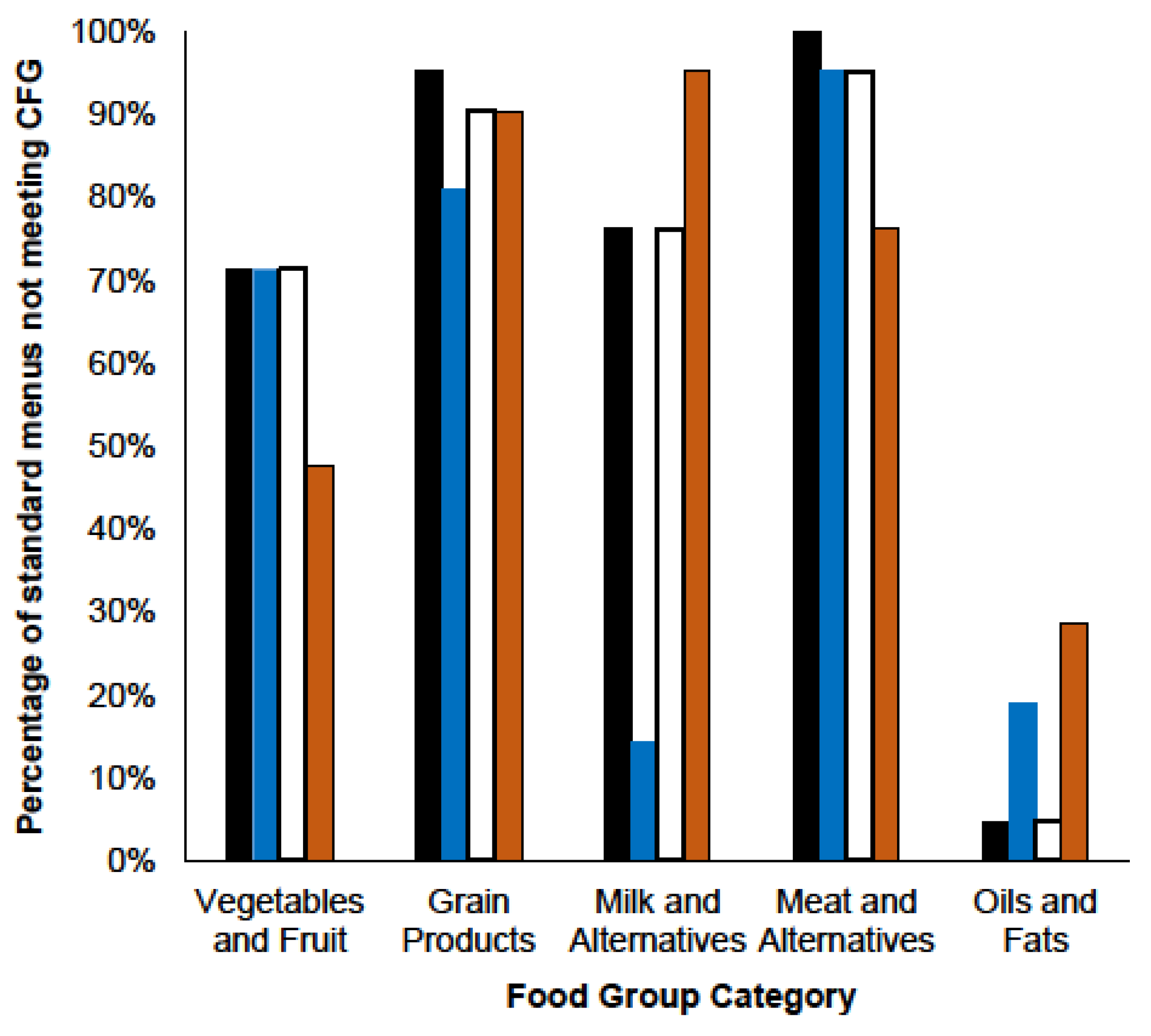
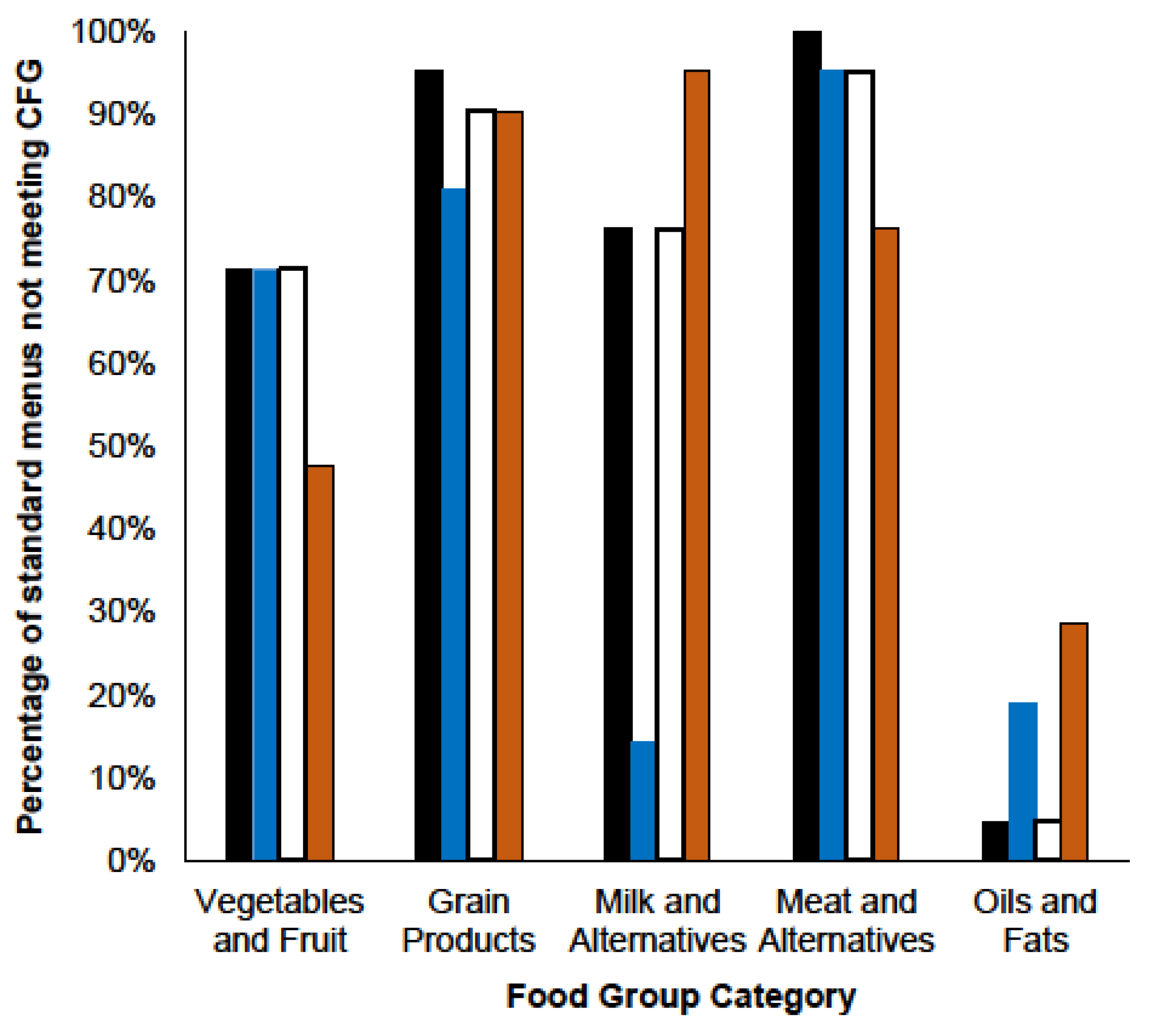
3.2. Food Guide Servings
| Regular Menus | Carbohydrate-Controlled Menus | 3000 mg Menus | 2000 mg Menus | |||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD (n = 21) | Range | Mean ± SD (n = 21) | Range | Mean ± SD (n = 21) | Range | Mean ± SD (n = 21) | Range | |
| Vegetables and Fruit | 5.9 ± 1.2 | 3.4–8.2 | 6.1 ± 1.4 | 4.6–9.7 | 5.7 ± 1.3 | 3.3–8.2 | 6.7 ± 1.6 | 3.9–8.7 |
| <7 servings | 15 (71%) | 15 (71%) | 15 (71%) | 10 (48%) | ||||
| Grain Products | 4.6 ± 1.2 | 2.3–6.7 | 5.6 ± 0.9 | 4.1–7.1 | 4.5 ± 1.4 | 2.3–7.0 | 4.6 ± 1.2 | 2.3–7.1 |
| <7 servings | 20 (95%) | 17 (81%) | 19 (90%) | 19 (90%) | ||||
| Milk and Alternatives | 2.1 ± 0.5 | 1.1–2.9 | 2.9 ± 0.5 | 2.0–3.8 | 2.0 ± 0.6 | 0.7–2.9 | 1.5 ± 0.7 | 0.6–2.6 |
| <3 servings | 16 (76%) | 3 (14%) | 16 (76%) | 20 (95%) | ||||
| Meat and Alternatives | 1.7 ± 0.5 | 0.4–2.9 | 1.7 ± 0.6 | 0.4–3.3 | 1.6 ± 0.6 | 0.4–2.7 | 1.9 ± 0.6 | 1.2–3.4 |
| <3 servings | 21 (100%) | 20 (95%) | 20 (95%) | 16 (76%) | ||||
| Oils and Fats | 0.4 ± 0.3 | 0.2–1.1 | 0.7 ± 0.3 | 0.3–1.5 | 0.4 ± 0.3 | 0.2–1.1 | 0.6 ± 0.5 | 0.2–1.7 |
| >45 mL | 1 (5%) | 4 (19%) | 1 (5%) | 6 (29%) | ||||
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Tappenden, K.A.; Quatrara, B.; Parkhurst, M.L.; Malone, A.M.; Fanjiang, G.; Ziegler, T.R. Critical role of nutrition in improving quality of care: An interdisciplinary call to action to address adult hospital malnutrition. JPEN J. Parenter. Enteral Nutr. 2013, 37, 482–497. [Google Scholar] [CrossRef] [PubMed]
- Allard, J.P.; Keller, H.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R.; Gramlich, L.; Payette, H.; Bernier, P.; Vesnaver, E.; Davidson, B.; et al. Malnutrition at hospital admission-contributors and effect on length of stay: A prospective cohort study from the Canadian malnutrition task force. JPEN J. Parenter. Enteral Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Iff, S.; Leuenberger, M.; Rösch, S.; Knecht, G.; Tanner, B.; Stanga, Z. Meeting the nutritional requirements of hospitalized patients: An interdisciplinary approach to hospital catering. Clin. Nutr. 2008, 27, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Food and Nutrition: Eating Well with Canada’s Food Guide. Available online: http://www.hc-sc.gc.ca/fn-an/food-guide-aliment/index-eng.php (accessed on 3 November 2015).
- Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Health Sciences Centre Winnipeg. Available online: http://www.hsc.mb.ca/patientsWhileInHosp.html (accessed on 10 October 2013).
- Mount Sinai Hospital. Patient Food Services. Available online: http://www.mountsinai.on.ca/patients/services/nutrition/patient-food-services (accessed on 10 October 2013).
- Restigouche Health Authority. Patients and visitors. Available online: http://www.santerestigouchehealth.com/page.aspx?page_id=80#Your Meals (accessed on 10 October 2013).
- Llywodraeth Cymru Welsh Government. All Wales Nutrition and Catering Standards for Food and Fluid Provision for Hospital Inpatients. Available online: http://wales.gov.uk/docs/dhss/publications/120305nutritioncateringstandardsen.pdf (accessed on 6 October 2013).
- NHS Quality Improvement Scotland (NHS QIS). National Overview-April 2010: Food, Fluid and Nutritional Care in Hospitals. Available online: http://www.healthcareimprovementscotland.org/default.aspx?page=11926 (accessed on 6 October 2013).
- The New York City Department of Health and Mental Hygiene. New York City Food Standards: Patient meals. Available online: http://www.nyc.gov/html/doh/downloads/pdf/cardio/patient-meals-standards.pdf (accessed on 24 October 2013).
- Department of Human Services (Victoria). Nutrition Standards for Menu Items in Victorian Hospitals and Residential Aged Care Facilities. Available online: http://www.health.vic.gov.au/archive/archive2011/patientfood/nutrition_standards.pdf (accessed on 6 October 2013).
- NSW Agency for Clinical Innovation. Nutritional Standards for Adult Inpatients in NSW Hospitals. Agency for Clinical Innovation. Available online: http://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0004/160555/ACI_Adult_Nutrition_web.pdf (accessed on 6 October 2013).
- Thibault, R.; Chikhi, M.; Clerc, A.; Darmon, P.; Chopard, P.; Genton, L.; Kossovsky, M.P.; Pichard, C. Assessment of food intake in hospitalised patients: A 10-year comparative study of a prospective hospital survey. Clin. Nutr. 2011, 30, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Arcand, J.; Steckham, K.; Tzianetas, R.; L'Abbe, M.R.; Newton, G.E. Evaluation of sodium levels in hospital patient menus. Arch. Intern. Med. 2012, 172, 1261–1262. [Google Scholar] [CrossRef] [PubMed]
- Barr, S.I.; Murphy, S.P.; Poos, M.I. Interpreting and using the dietary references intakes in dietary assessment of individuals and groups. J. Am. Diet. Assoc. 2002, 102, 780–788. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Nelms, M. Metabolic Stress and the Critically Ill. In Nutrient Therapy and Pathophysiology, 2nd ed.; Cengage Learning: Belmont, CA, USA, 2011. [Google Scholar]
- Katamay, S.W.; Esslinger, K.A.; Vigneault, M.; Johnston, J.L.; Junkins, B.A.; Robbins, L.G.; Sirois, I.V.; Jones-Mclean, E.M.; Kennedy, A.F.; Bush, M.A.; et al. Eating well with Canada's food guide (2007): Development of the food intake pattern. Nutr. Rev. 2007, 65, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Wright-Thompson, A.; Piche, L. Nutritional analysis of a long-term care menu before and after an increase in the raw food cost allowance. Can. J. Diet. Pract. Res. 2011, 72, 141–145. [Google Scholar] [CrossRef] [PubMed]
- The Scottish Government. Food in Hospitals: National Catering and Nutrition Specification for Food and Fluid Provision in Hospitals in Scotland. Available online: http://www.scotland.gov.uk/Resource/Doc/229423/0062185.pdf (accessed on 6 October 2013).
- Northwest Territories health and Social Services. Healthy foods in Facilities: Food and Beverage Guidelines for Health and Social Services. Available online: http://www.hss.gov.nt.ca/sites/default/files/healthy_foods_in_facilities.pdf (accessed on 7 October 2013).
- Ministry of Health—Government of British Columbia. Reducing the Sodium Intake of Canadians: A Provincial and Territorial Report on Progress and Recommendations for Future Action. Available online: http://www.health.gov.bc.ca/library/publications/year/2012/reducing-sodium-intake.pdf (accessed on 7 October 2013).
- Alberta Health Services. Trans Fat Policy. Available online: http://www.albertahealthservices.ca/Policies/ahs-pol-trans-fats.pdf (accessed on 9 October 2013).
- Healthy Families BC. Sodium Reduction in Health Care. Available online: http://www.healthyfamiliesbc.ca/home/sodium-reduction-healthcare (accessed on 9 October 2013).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trang, S.; Fraser, J.; Wilkinson, L.; Steckham, K.; Oliphant, H.; Fletcher, H.; Tzianetas, R.; Arcand, J. A Multi-Center Assessment of Nutrient Levels and Foods Provided by Hospital Patient Menus. Nutrients 2015, 7, 9256-9264. https://doi.org/10.3390/nu7115466
Trang S, Fraser J, Wilkinson L, Steckham K, Oliphant H, Fletcher H, Tzianetas R, Arcand J. A Multi-Center Assessment of Nutrient Levels and Foods Provided by Hospital Patient Menus. Nutrients. 2015; 7(11):9256-9264. https://doi.org/10.3390/nu7115466
Chicago/Turabian StyleTrang, Susan, Jackie Fraser, Lori Wilkinson, Katherine Steckham, Heather Oliphant, Heather Fletcher, Roula Tzianetas, and JoAnne Arcand. 2015. "A Multi-Center Assessment of Nutrient Levels and Foods Provided by Hospital Patient Menus" Nutrients 7, no. 11: 9256-9264. https://doi.org/10.3390/nu7115466