1. Introduction
Osteoporosis presents a growing health problem in many countries around the world [
1]. It is one of the most common complaints in people aged 50 and over and affects 30% of women and 8% of men in this age group [
2]. In Europe, USA and Japan, osteoporosis has been diagnosed in 75 million individuals [
1,
2]. In Europe, the annual costs of treatment of osteoporotic fractures amount to 25 billion Euros [
1]. Due to the aging of the society the incidence of osteoporosis will increase and thus it will generate a still further increase in treatment costs.
Women over the world are more exposed to osteoporosis and osteoporotic fractures then men [
1,
2,
3,
4]. In Europe and USA as well as Poland approximately 30% of postmenopausal women have osteoporosis of which 40% will sustain one or more fragility fracture in their remaining lifetime [
3,
4]. In Poland, osteoporosis affects 7% of women aged 45–64, 25% of women aged 65–74 and over 50% of women older than 75 years [
2]. In 2010, the number of cases of osteoporotic fractures in people aged 50 and over was 2.7 million, including 2.2 million females and 0.5 million males [
3]. It is predicted that four out of ten Polish women will be affected with at least one vertebral fracture before turning 80 years of age [
3]. Post-fracture complications result in the annual mortality of 20% of women and 30% of men with femoral neck fractures and a further 30% require constant medical care. It is thus justifiable for health science professionals to have an interest in the early diagnosis of osteoporosis, by understanding the risk factors and taking preventive measures.
Osteoporosis is a systemic metabolic bone disease which presents reduction in bone density together with abnormal structure [
5,
6]. Asymptomatic and pathological fractures are frequently the first clinical symptoms. Reduction in bone mineral density (BMD) with age is generally unavoidable. In the age range from 20 to 79, the proportion of individuals with regular bone mass and BMD values decreases in a mode near to linear, while the incidence of osteoporosis increases linearly [
7]. Until recently, diagnosis and treatment of osteoporosis was based on bone densitometry. Currently, both the diagnosis and therapy of osteoporosis focus on determining the individual risk for bone fracture [
3,
8]. However, this approach requires collecting information on the occurrence of dietary and non-dietary risk factors for bone fractures. Non-dietary factors increasing bone fracture risk include female sex, white race, advanced age, menstruation disorders, early menopause, previous fractures, hip fractures in parents, low BMI, low bone mass, administration of corticosteroids, rheumatoid arthritis, limited physical activity, poor self-evaluated health, smoking and alcohol abuse [
3,
5,
6]. Since some of these elements are non-modifiable risk factors (e.g., age, sex, inheritance), then more attention should be paid to the modifiable risk factors for bone fractures.
Dietary risk factors for bone fractures play a special role in the prevention of osteoporosis. Numerous studies indicate that adequate calcium intake improves bone mineral density [
9,
10,
11]. However, the role of dietary calcium and dairy products in preventing osteoporosis has not yet been fully explained. It is commonly thought that adequate intake of calcium during childhood and adolescence is most important [
12,
13]. It leads to high peak bone mass which serves as a sort of “deposit” for subsequent years of life [
14,
15]. The impact of calcium intake and consumption of dairy products on bone density in later stages of life is less understood [
10,
16]. It is thought that in adulthood, the role of dietary factors may be less and may mainly influence the rate of bone loss. It has been estimated that in post-menopausal women the involution rate of bone loss may change over a wide range of values from 1% to 5% or more per year [
7].
The predicted increase in the incidence of osteoporosis in women justifies a search for opportunities to prevent bone fractures. Undoubtedly, attention should be focused on exploring modifiable dietary risk factors. An in-depth understanding of these elements will provide opportunities for construction and implementation of prevention programs and improvement of public health. The objective of the studies was to analyze the consumption of dairy products and dietary calcium by women in the context of bone mineral density and to assess opportunities to prevent osteoporosis. We aimed to ascertain if there is a possibility to provide good bone status in the dietary manner, without nutritional intervention, but with the usual intake of dairy products and dietary calcium, typical of a Polish diet.
4. Discussion
The studies showed that women’s bone mineral density to a large extent depended on the combined impact of dietary and non-dietary risk factors. The factors included, as well as age and the presence of the menstrual cycle, consumption of dairy products during adulthood and daily consumption of dairy products during childhood and adolescence. The single dietary risk factors related to bone mineral density were the daily consumption of dairy products during childhood and adolescence. The single dietary risk factors had a weaker impact on bone mineral density than non-modifiable confounders.
A strong relationship between the risk of osteoporosis and age and the menstrual cycle was confirmed [
3,
29]. The women with regular bone mineral density were younger and more of them had regular menstrual cycles. The probability of regular bone mineral density was four times higher in the women under 50 years of age and almost eight times higher in the women with regular menstrual cycles. The women who menstruated were under the influence of oestrogens, which support regular bone mineralization [
6,
30,
31]. Non-menstruating women lack this protective effect of oestrogens and therefore menopause is an established risk factor for low bone density in women. The fastest loss of bone mass occurs in women in the first years after menopause due to rapid decrease in the level of oestrogens [
3,
16,
30,
31,
32]. Collagen fibres degenerate with age and this process reduces the hardness of bones. Furthermore, bone loss overwhelms bone tissue formation [
3,
16]. Hence, age and menstrual cycle are strong independent risk factors for bone mineral density and osteoporosis.
The independent impact of single dietary risk factors on bone mineral density in the adult women was revealed for two dietary risk factors. The daily consumption of dairy products during pre-school and school period 2.4 to 2.7 times increased the probability of bone mineral density in the upper tercile in adult women. The relation between bone mineral density and consumption of dietary calcium above 400 mg/day in adulthood was weak–we stated a significance odds ratio only after adjusting for age but not after adjusting for age, menstruation and BMI together. The impact of calcium intake on bone density in later stages of life is less understood [
10,
13,
16,
33]. It is thought that in adulthood, the role of dietary calcium may be less and it may mainly influence the rate of bone loss. It is possible that our result followed a too low value of dietary calcium cut-off (400 mg/day). However, we could not use a higher cut-off because of the generally low dietary calcium intake level observed in women in our sample as well as in the Polish population [
20,
34,
35]. The research should be continued with a greater number of women in the sample to explain the relation between dietary calcium and bone mineral density in adulthood and the point of good-fitted dietary calcium cut-off.
It is worth emphasizing that the impact of dietary factors on bone mineral density was connected to non-modifiable confounders. The relation was clear and is compatible with many papers [
9,
10,
13,
33]. The relationship between these risk factors was high since the explained variation of the system (inertia) was 58%. Our findings and the results by other authors indicate a multi-factorial aetiology of low bone mineral density and osteoporosis [
10,
14,
15,
16]. The number of risk factors for osteoporosis and bone fractures described in the literature exceeds 30 and this issue continues to be discussed and verified. It indicates a need for the simultaneous impact on many potential risk factors in the prevention of osteoporosis.
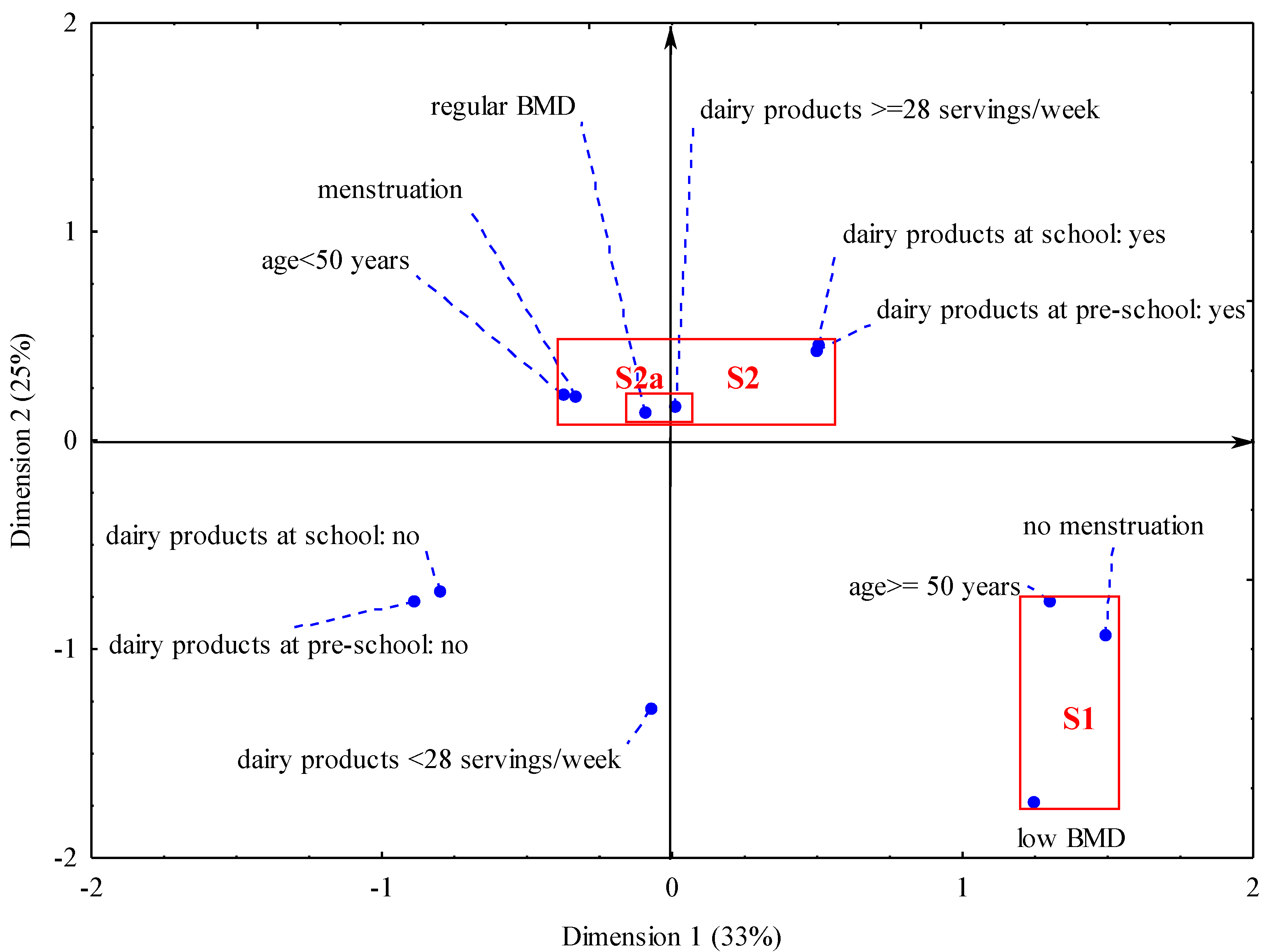
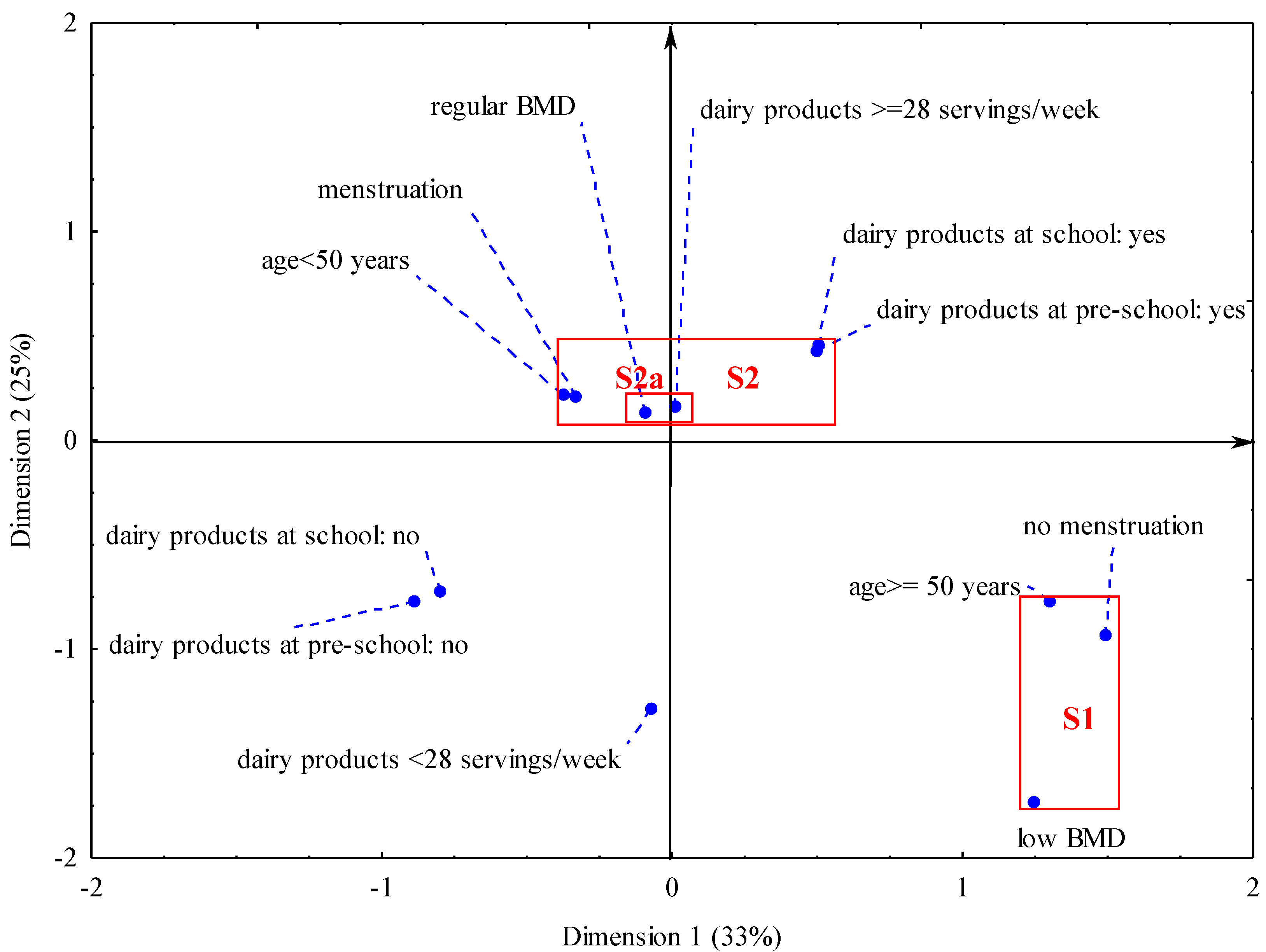
Interestingly, there is a relationship between the consumption of dairy products during adulthood and in the past and consequent benefits to bone health. The regular bone mineral density (S2 cluster) was revealed in younger and menstruating women who consumed more dairy products as adults and on every day in the past. The consumption of dairy products by the women during adulthood was relatively high since the established cut-off point was ≥28 servings/week. Such a consumption threshold was reached or exceeded by 89% of women with regular bone mineral density,
i.e., six percentage points more than in the women with low bone mineral density. The consumption of dairy products in the past related to a daily intake of these products, regardless of their amount, because the collection of quantitative data from the period that extends 20–50 years in the past is virtually impossible in retrospective studies [
24].
Our results indicate that the consumption of dairy products in childhood and adolescence had the largest and most positive impact on good bone health even if the level of intake in the past was unknown and the consumption of dairy products during adulthood was moderate. This conclusion is important for developing prevention programs and introducing preventive activities. It implies that childhood and adolescence are key periods for bone health. Firstly, this is the period of gaining peak bone mass [
14,
15]. Secondly, eating habits are established in this period. Numerous studies indicate that family and schoolmates during childhood and adolescence influence eating habits, consumption of food and human health in later stages of life [
36,
37,
38,
39]. Positive nutritional attitudes in parents and a good school environment facilitate and support eating behavior beneficial to health in children and adolescents. Prevention programs should thus aim at creating proper nutritional habits during childhood and adolescence and their reinforcement during adulthood.
Early formation of the habit of consuming dairy products daily may be critical to eating habits and bone health during adulthood [
36,
37]. Negative impact of low-calcium or non-dairy diets has been documented in Polish and foreign studies [
40,
41,
42]. For instance, in Polish girls with diagnosed allergy to cow’s milk and treated with a non-dairy diet, bone fractures were found to occur four times more often than in girls who consumed an adequate amount of dairy products [
41]. During childhood, nutrition depends on care-givers and is based on imitation. In later stages of life, food choices depend on a complex arrangement of many social, cultural, demographic, psychological and individual parameters such as age, sex, education, incomes, nutritional and health awareness, personal experiences, region and country-specific environment [
43,
44,
45]. Generally, young people have a lower health risk perception than adults and seniors [
46]. Therefore recalling diet-health awareness in order to improve the nutrition of young people can bring only small effects. This strengthens our earlier statement that in the young desirable eating habits should be formed by imitation and as a habitual behavior induced by the positive attitudes of parents and the good health impact of the school environment [
36,
37,
38,
39]. National health-nutrition policy should be focused on the early creation of good dietary habit in the first stage of life through the family and school environment.
The studies did not reveal any impact of non-dairy sources of calcium on bone mineral density. Our previous studies and some papers of other authors suggest a beneficial impact of taking calcium supplements and/or consumption of calcium-enriched food on bone health [
29,
47,
48]. This paper did not focus on analyzing the impact on non-dairy calcium sources on the bones. For instance, during our studies we did not collect information on the amount of calcium consumed with supplements and/or calcium-enriched food. Hence, within the framework of this study, interpreting the impact of non-dairy calcium sources on risks for osteoporosis and bone fractures is difficult.
We found a relatively low level of dietary calcium in the adult women. The average level of dietary calcium was about 500 mg/day. Our results are consistent with the studies of many Polish authors [
20,
34,
35]. In the WOBASZ studies it was found that adult Poles consumed on average 460 mg of calcium per day (less that 60% of DRI) [
20]. In the national survey of households, the consumption of calcium by women aged 26–60 was 520 mg/day [
31]. Higher consumption of calcium was recorded in Canadian women aged 50–70,
i.e., on average about 750 mg/day [
49]. Significantly higher calcium intake was reported in the prospective Swedish Mammography Cohort Clinical studies [
10]. Swedish women in the lowest dietary calcium quintile consumed on average 698 mg/day, whereas the women in the highest quintile averaged 1389 mg/day. On this basis, the intake of dietary calcium by Polish women was assessed as relatively low.
The strengths and weaknesses of our research are as follows:
This relatively low level of dietary calcium is a weakness in our studies. Our results do not definitively conclude the occurrence of a relationship between dietary calcium and bone mineral density in relation to the recommended calcium intake by adult women. In Poland, the recommended intake (EAR) of calcium is set at 800 mg/day for women aged 31–50 and 1000 mg/day for women over 50 years of age [
21]. It might indicate why our results cannot fully explain some of the opinions on the beneficial role of dietary calcium in reducing the risk of osteoporosis [
3,
9,
10,
13,
50].
The dietary and densitometry studies were conducted on a sub-sample of 170 women that was not selected randomly from the general population. The dietary studies were carried out with 712 women and the consumption of dairy products was assessed. The analysis did not reveal any difference in the consumption of dairy products between the women from the total sample and the women from the sub-sample tested with densitometry. This increases the strength of drawing conclusions and provides a basis for formulating more general statements. The lack of randomization in the sample selection makes it difficult to refer the results to the general population, but it establishes a relationship between the consumption of dairy products and dietary calcium and the risk for low mineral density and osteoporosis. In this context, our findings provide some interesting information.
The use of a validated questionnaire on the frequency of food consumption for assessing the intake of dietary calcium by women during adulthood constitutes the strength of our studies [
17]. The application of the consumption frequency method allows for an increase in the sample size in the dietary studies in comparison with food record or a 24-h interview [
24]. Moreover, it creates an opportunity to evaluate food consumption over a longer time period. The questionnaire on the frequency of food consumption related to the consumption of dairy products during the six months preceding the study. It enabled a good assessment of the habitual consumption of dairy products and dietary calcium in the adult women.

 ,
, 

{kind=link}