A Food Frequency Questionnaire for the Assessment of Calcium, Vitamin D and Vitamin K: A Pilot Validation Study

Abstract
:
1. Introduction
2. Experimental Section
2.1. Participant Recruitment
2.2. Nutrient Analysis
2.2.1. Food Frequency Questionnaire (FFQ)
2.2.2. 5-Day Diet Record (5DDR)
2.3. Statistical Analysis
3. Results and Discussion

{kind=link}
{kind=link}
{kind=link}
| Proportion, n (%) | |
|---|---|
| Ethnicity | |
| North-American Caucasian | 11 (73.3) |
| European | 2 (13.3) |
| South American | 1 (6.7) |
| Southeast Asian | 1 (6.7) |
| Ambulation status | |
| No aid | 11 (73.3) |
| Walking aid | 4 (26.7) |
| Living arrangements | |
| Living independently | 3 (20.0) |
| Living with family support | 9 (60.0) |
| Living independently with non-live in support | 3 (20.0) |
| Number of years since menopause | |
| 11–15 years | 3 (20.0) |
| 16–20 years | 2 (13.3) |
| >20 years | 10 (66.7) |
| Body mass index classification | |
| Normal weight (18.5–24.99 kg/ m2) | 0 |
| Overweight (25–29.99 kg/ m2) | 4 (26.7) |
| Obese (≥30 kg/ m2) | 11 (73.3) |
| Self-reported diagnosis of chronic disease | |
| Osteoporosis | 3 (20.0) |
| Osteoarthritis | 5 (33.3) |
| Type 2 diabetes | 12 (80.0) |
| Number of prescription medications | |
| None | 1 (6.7) |
| 1–5 medications | 4 (26.7) |
| 6–10 medications | 4 (26.7) |
| 11–15 medications | 1 (6.7) |
| 16–20 medications | 4 (26.7) |
| 161 item FFQ | 5DDR | p-value | Pearson r | |||||
|---|---|---|---|---|---|---|---|---|
| Diet sources | Supplement sources | Total | Diet sources | Supplement sources | Total | |||
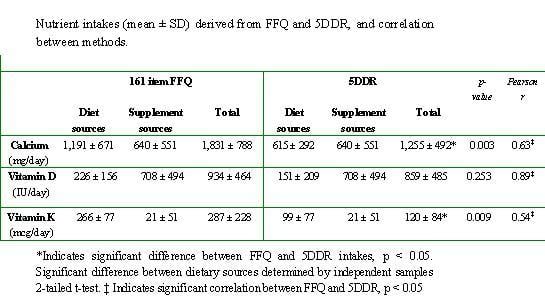
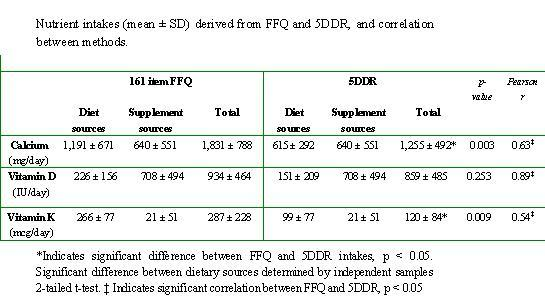
| Calcium (mg/day) | 1,191 ± 671 | 640 ± 551 | 1,831 ± 788 | 615 ± 292 | 640 ± 551 | 1,255 ± 492* | 0.003 | 0.63‡ |
| Vitamin D (IU/day) | 226 ± 156 | 708 ± 494 | 934 ± 464 | 151 ± 209 | 708 ± 494 | 859 ± 485 | 0.253 | 0.89‡ |
| Vitamin K (mcg/day) | 266 ± 77 | 21 ± 51 | 287 ± 228 | 99 ± 77 | 21 ± 51 | 120 ± 84* | 0.009 | 0.54‡ |
| % classified intosame quartile | % classified into same ± 1 quartile | % misclassified | |
| Calcium | 47 | 87 | 0 |
| Vitamin D | 73 | 100 | 0 |
| Vitamin K | 33 | 87 | 0 |
4. Discussion and Conclusions
Acknowledgements
References
- Papaioannou, A.; Joseph, L.; Ioannidis, G.; Berger, C.; Anastassiades, T.; Brown, J.P.; Hanley, D.A.; Hopman, W.; Josse, R.G.; Kirkland, S.; Murray, T.M.; Olszynski, W.P.; Pickard, L.; Prior, J.C.; Siminoski, K.; Adachi, J.D. Risk factors associated with incident clinical vertebral and nonvertebral fractures in postmenopausal women: the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos. Int. 2005, 16, 568–578. [Google Scholar]
- Kanis, J.A. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporos. Int. 1994, 4, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Adachi, J.D.; Loannidis, G.; Berger, C.; Joseph, L.; Papaioannou, A.; Pickard, L.; Papadimitropoulos, E.A.; Hopman, W.; Poliquin, S.; Prior, J.C.; Hanley, D.A.; Olszynski, W.P.; Anastassiades, T.; Brown, J.P.; Murray, T.; Jackson, S.A.; Tenenhouse, A. The influence of osteoporotic fractures on health-related quality of life in community-dwelling men and women across Canada. Osteoporos. Int. 2001, 12, 903–908. [Google Scholar]
- Cheung, A.M.; Tile, L.; Lee, Y.; Tomlinson, G.; Hawker, G.; Scher, J.; Hu, H.; Vieth, R.; Thompson, L.; Jamal, S.; Josse, R. Vitamin K supplementation in postmenopausal women with osteopenia (ECKO trial): a randomized controlled trial. PLoS Med. 2008, 5, e196. [Google Scholar]
- Cockayne, S.; Adamson, J.; Lanham-New, S.; Shearer, M.J.; Gilbody, S.; Torgerson, D.J. Vitamin K and the prevention of fractures: systematic review and meta-analysis of randomized controlled trials. Arch. Intern. Med. 2006, 166, 1256–1261. [Google Scholar]
- Cranney, A.; Weiler, H.A.; O'Donnell, S.; Puil, L. Summary of evidence-based review on vitamin D efficacy and safety in relation to bone health. Am. J. Clin. Nutr. 2008, 88, 513S–519S. [Google Scholar]
- Dawson-Hughes, B. Serum 25-hydroxyvitamin D and functional outcomes in the elderly. Am. J. Clin. Nutr. 2008, 88, 537S–540S. [Google Scholar]
- Jackson, R.D.; LaCroix, A.Z.; Gass, M.; Wallace, R.B.; Robbins, J.; Lewis, C.E.; Bassford, T.; Beresford, S.A.; Black, H.R.; Blanchette, P.; Bonds, D.E.; Brunner, R.L.; Brzyski, R.G.; Caan, B.; Cauley, J.A.; Chlebowski, R.T.; Cummings, S.R.; Granek, I.; Hays, J.; Heiss, G.; Hendrix, S.L.; Howard, B.V.; Hsia, J.; Hubbell, F.A.; Johnson, K.C.; Judd, H.; Kotchen, J.M.; Kuller, L.H.; Langer, R.D.; Lasser, N.L.; Limacher, M.C.; Ludlam, S.; Manson, J.E.; Margolis, K.L.; McGowan, J.; Ockene, J.K.; O'Sullivan, M.J.; Phillips, L.; Prentice, R.L.; Sarto, G.E.; Stefanick, M.L.; Van Horn, L.; Wactawski-Wende, J.; Whitlock, E.; Anderson, G.L.; Assaf, A.R.; Barad, D. Calcium plus vitamin D supplementation and the risk of fractures. N. Engl. J. Med. 2006, 354, 669–683. [Google Scholar]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Staehelin, H.B.; Orav, J.E.; Stuck, A.E.; Theiler, R.; Wong, J.B.; Egli, A.; Kiel, D.P.; Henschkowski, J. Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ 2009, 339, b3692. [Google Scholar]
- Bischoff-Ferrari, H.A.; Willett, W.C.; Wong, J.B.; Stuck, A.E.; Staehelin, H.B.; Orav, E.J.; Thoma, A.; Kiel, D.P.; Henschkowski, J. Prevention of nonvertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials. Arch. Intern. Med. 2009, 169, 551–561. [Google Scholar]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Baron, J.A.; Burckhardt, P.; Li, R.; Spiegelman, D.; Specker, B.; Orav, J.E.; Wong, J.B.; Staehelin, H.B.; O'Reilly, E.; Kiel, D.P.; Willett, W.C. Calcium intake and hip fracture risk in men and women: a meta-analysis of prospective cohort studies and randomized controlled trials. Am. J. Clin. Nutr. 2007, 86, 1780–1790. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionniares- a review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar]
- Weiler, H.A.; Leslie, W.D.; Krahn, J.; Steiman, P.W.; Metge, C.J. Canadian Aboriginal women have a higher prevalence of vitamin D deficiency than non-Aboriginal women despite similar dietary vitamin D intakes. J. Nutr. 2007, 137, 461–465. [Google Scholar]
- Langsetmo, L.; Poliquin, S.; Hanley, D.A.; Prior, J.C.; Barr, S.; Anastassiades, T.; Towheed, T.; Goltzman, D.; Kreiger, N. Dietary patterns in Canadian men and women ages 25 and older: relationship to demographics, body mass index, and bone mineral density. BMC Musculoskelet. Disord. 2010, 11, 20. [Google Scholar] [PubMed]
- Taylor, C.; Lamparello, B.; Kruczek, K.; Anderson, E.J.; Hubbard, J.; Misra, M. Validation of a food frequency questionnaire for determining calcium and vitamin D intake by adolescent girls with anorexia nervosa. J. Am. Diet. Assoc. 2009, 109, 479–485. [Google Scholar]
- Wu, H.; Gozdzik, A.; Barta, J.L.; Wagner, D.; Cole, D.E.; Vieth, R.; Parra, E.J.; Whiting, S.J. The development and evaluation of a food frequency questionnaire used in assessing vitamin D intake in a sample of healthy young Canadian adults of diverse ancestry. Nutr. Res. 2009, 29, 255–261. [Google Scholar]
- Kelemen, L.E.; Anand, S.S.; Vuksan, V.; Yi, Q.; Teo, K.K.; Devanesen, S.; Yusuf, S. Development and evaluation of cultural food frequency questionnaires for South Asians, Chinese, and Europeans in North America. J. Am. Diet. Assoc. 2003, 103, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.G.; Rohan, T.E.; Soskolne, C.L.; Kreiger, N. Calibration of the dietary questionnaire for the Canadian Study of Diet, Lifestyle and Health cohort. Public Health Nutr. 2003, 6, 79–86. [Google Scholar]
- USDA National Nutrient Database for Standard Reference. US Department of Agriculture, Agricultural Research Service. 2008, Release 22. Available online: http://www.ars.usda.gov/ (accessed on March 20, 2010).
- Health Canada, Canadian Nutrient File, 2007b version; Available online: http://www.healthcanada.ca/cnf.
- Calvo, M.S.; Whiting, S.J.; Barton, C.N. Vitamin D fortification in the United States and Canada: current status and data needs. Am. J. Clin. Nutr. 2004, 80, 1710S–1716S. [Google Scholar]
- Sacco, J.E.; Tarasuk, V. Health Canada's proposed discretionary fortification policy is misaligned with the nutritional needs of Canadians. J. Nutr. 2009, 139, 1980–1986. [Google Scholar]
- Booth, S.L.; Sokoll, L.J.; O'Brien, M.E.; Tucker, K.; Dawson-Hughes, B.; Sadowski, J.A. Assessment of dietary phylloquinone intake and vitamin K status in postmenopausal women. Eur. J. Clin. Nutr. 1995, 49, 832–841. [Google Scholar]
- Presse, N.; Shatenstein, B.; Kergoat, M.J.; Ferland, G. Validation of a semi-quantitative food frequency questionnaire measuring dietary vitamin K intake in elderly people. J. Am. Diet. Assoc. 2009, 109, 1251–1255. [Google Scholar]
- Institute of Medicine Food and Nutrition Board. Dietary Reference Intakes: Calcium, Magnesium, Phosphorus, Vitamin D and Fluoride; National Academy Press, Institute of Medicine, Food and Nutrition Board: Washington, DC, USA, 1997.
- Institute of Medicine Food and Nutrition Board. Dietary Reference Intakes: Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academy Press, Institute of Medicine, Food and Nutrition Board: Washington, DC, USA, 2001.
- Sebring, N.G.; Denkinger, B.I.; Menzie, C.M.; Yanoff, L.B.; Parikh, S.J.; Yanovski, J.A. Validation of three food frequency questionnaires to assess dietary calcium intake in adults. J. Am. Diet. Assoc. 2007, 107, 752–759. [Google Scholar]
- Angbratt, M.; Moller, M. Questionnaire about calcium intake: can we trust the answers? Osteoporos. Int. 1999, 9, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Chee, W.S.; Suriah, A.R.; Zaitun, Y.; Chan, S.P.; Yap, S.L.; Chan, Y.M. Dietary calcium intake in postmenopausal Malaysian women: comparison between the food frequency questionnaire and three-day food records. Asia Pac. J. Clin. Nutr. 2002, 11, 142–146. [Google Scholar]
- Hacker-Thompson, A.; Robertson, T.P.; Sellmeyer, D.E. Validation of two food frequency questionnaires for dietary calcium assessment. J. Am. Diet. Assoc. 2009, 109, 1237–1240. [Google Scholar]
- Khan, N.C.; Mai le, B.; Hien, V.T.; Lam, N.T.; Hoa, V.Q.; Phuong, T.M.; Nhung, B.T.; Nakamori, M.; Shimizu, Y.; Yamamoto, S. Development and validation of food frequency questionnaire to assess calcium intake in postmenopausal Vietnamese women. J. Nutr. Sci. Vitaminol. (Tokyo) 2008, 54, 124–129. [Google Scholar] [PubMed]
- Magkos, F.; Manios, Y.; Babaroutsi, E.; Sidossis, L.S. Development and validation of a food frequency questionnaire for assessing dietary calcium intake in the general population. Osteoporos. Int. 2006, 17, 304–312. [Google Scholar]
- Montomoli, M.; Gonnelli, S.; Giacchi, M.; Mattei, R.; Cuda, C.; Rossi, S.; Gennari, C. Validation of a food frequency questionnaire for nutritional calcium intake assessment in Italian women. Eur. J. Clin. Nutr. 2002, 56, 21–30. [Google Scholar]
- Osowski, J.M.; Beare, T.; Specker, B. Validation of a food frequency questionnaire for assessment of calcium and bone-related nutrient intake in rural populations. J. Am. Diet. Assoc. 2007, 107, 1349–1355. [Google Scholar]
- Pereira, G.A.; Genaro, P.S.; Santos, L.C.; Sarkis, K.S.; Pinheiro, M.M.; Szjenfeld, V.L.; Schuch, N.J.; Martini, L.A. Validation of a food frequency questionnaire for women with osteoporosis. J. Nutr. Health. Aging. 2009, 13, 403–407. [Google Scholar]
- Serra-Majem, L.; Frost Andersen, L.; Henrique-Sanchez, P.; Doreste-Alonso, J.; Sanchez-Villegas, A.; Ortiz-Andrelluchi, A.; Negri, E.; La Vecchia, C. Evaluating the quality of dietary intake validation studies. Br. J. Nutr. 2009, 102, S3–S9. [Google Scholar]
- McNeill, G.; Winter, J.; Jia, X. Diet and cognitive function in later life: a challenge for nutrition epidemiology. Eur. J. Clin. Nutr. 2009, 63, S33–S37. [Google Scholar]
- Rothenberg, E.M. Experience of dietary assessment and validation from three Swedish studies in the elderly. Eur. J. Clin. Nutr. 2009, 63, S64–S68. [Google Scholar]
- Block, G. Human dietary assessment: methods and issues. Prev. Med. 1989, 18, 653–660. [Google Scholar]
- Willett, W.C. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 1990. [Google Scholar]
- Potosky, A.L.; Block, G.; Hartman, A.M. The apparent validity of diet questionnaires is influenced by number of diet-record days used for comparison. J. Am. Diet. Assoc. 1990, 90, 810–813. [Google Scholar] [PubMed]
- Stram, D.O.; Longnecker, M.P.; Shames, L.; Kolonel, L.N.; Wilkens, L.R.; Pike, M.C.; Henderson, B.E. Cost-efficient design of a diet validation study. Am. J. Epidemiol. 1995, 142, 353–362. [Google Scholar]
- Cappuccio, F.P.; Elliott, P.; Allender, P.S.; Pryer, J.; Follman, D.A.; Cutler, J.A. Epidemiologic association between dietary calcium intake and blood pressure: a meta-analysis of published data. Am. J. Epidemiol. 1995, 142, 935–945. [Google Scholar]
- Suliburska, J.; Bogdanski, P.; Pupek-Musialik, D.; Krejpcio, Z. Dietary Intake and Serum and Hair Concentrations of Minerals and their Relationship with Serum Lipids and Glucose Levels in Hypertensive and Obese Patients with Insulin Resistance. Biol. Trace Elem. Res. 2010. Epub ahead of print.
- Scagliusi, F.B.; Ferriolli, E.; Pfrimer, K.; Laureano, C.; Cunha, C.S.; Gualano, B.; Lourenco, B.H.; Lancha, A.H., Jr. Characteristics of women who frequently under report their energy intake: a doubly labelled water study. Eur. J. Clin. Nutr. 2009, 63, 1192–1199. [Google Scholar] [Green Version]
- Tooze, J.A.; Vitolins, M.Z.; Smith, S.L.; Arcury, T.A.; Davis, C.C.; Bell, R.A.; DeVellis, R.F.; Quandt, S.A. High levels of low energy reporting on 24-hour recalls and three questionnaires in an elderly low-socioeconomic status population. J. Nutr. 2007, 137, 1286–1293. [Google Scholar]
- Vatanparast, H.; Dolega-Cieszkowski, J.H.; Whiting, S.J. Many adult Canadians are not meeting current calcium recommendations from food and supplement intake. Appl. Physiol. Nutr. Metab. 2009, 34, 191–196. [Google Scholar]
- Vatanparast, H.; Calvo, M.S.; Green, T.J.; Whiting, S.J. Despite mandatory fortification of staple foods, vitamin D intakes of Canadian children and adults are inadequate. J. Steroid Biochem. Mol. Biol. 2010, 121, 301–303. [Google Scholar]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pritchard, J.M.; Seechurn, T.; Atkinson, S.A. A Food Frequency Questionnaire for the Assessment of Calcium, Vitamin D and Vitamin K: A Pilot Validation Study. Nutrients 2010, 2, 805-819. https://doi.org/10.3390/nu2080805
Pritchard JM, Seechurn T, Atkinson SA. A Food Frequency Questionnaire for the Assessment of Calcium, Vitamin D and Vitamin K: A Pilot Validation Study. Nutrients. 2010; 2(8):805-819. https://doi.org/10.3390/nu2080805
Chicago/Turabian StylePritchard, Janet M., Tinasha Seechurn, and Stephanie A. Atkinson. 2010. "A Food Frequency Questionnaire for the Assessment of Calcium, Vitamin D and Vitamin K: A Pilot Validation Study" Nutrients 2, no. 8: 805-819. https://doi.org/10.3390/nu2080805