Canadian Adults with Moderate Intakes of Total Sugars have Greater Intakes of Fibre and Key Micronutrients: Results from the Canadian Community Health Survey 2015 Public Use Microdata File

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
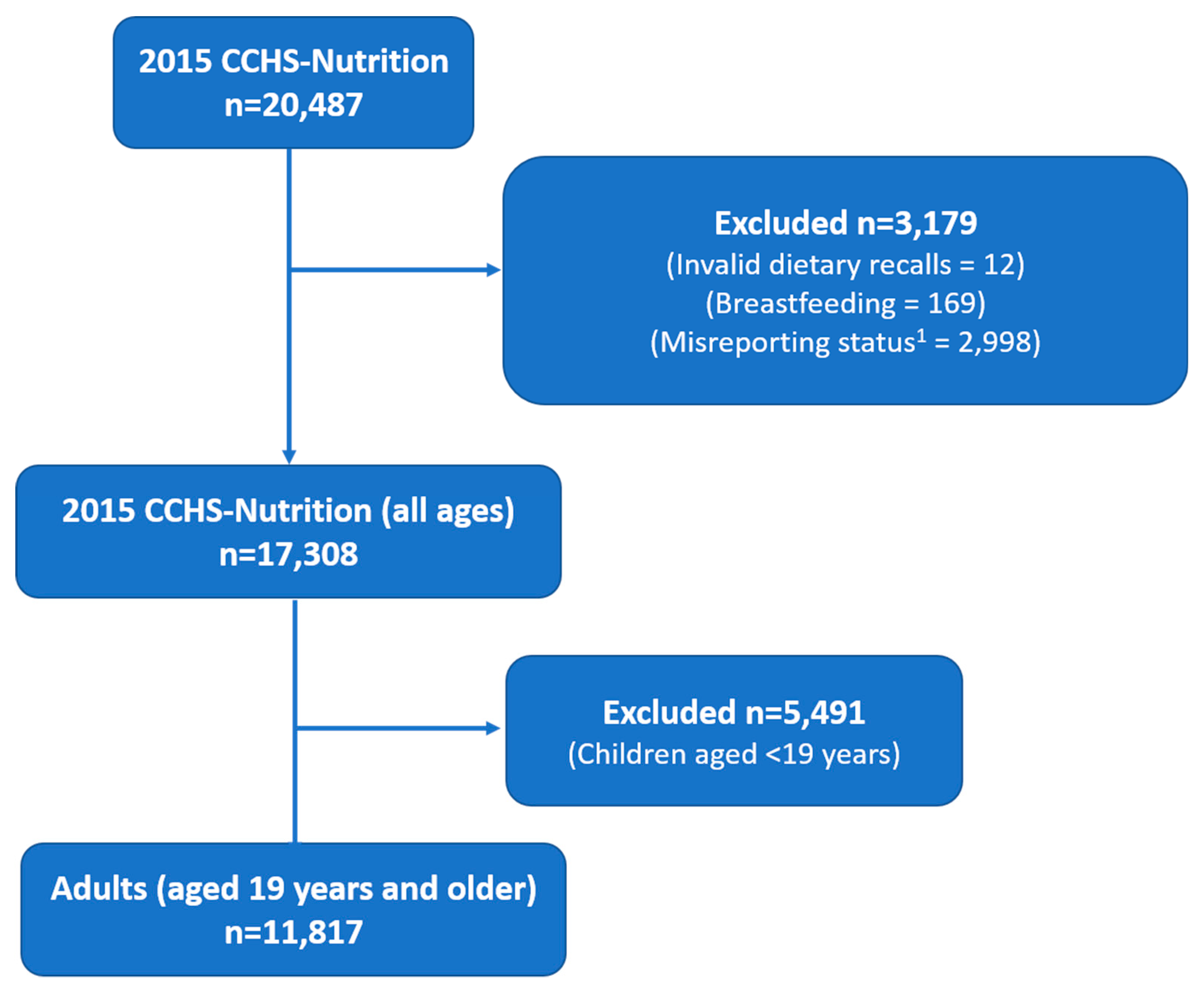
2.2. Participants and Data Collection
2.3. Estimation of Added and Free Sugars
2.4. Adjusting for Misreporting
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
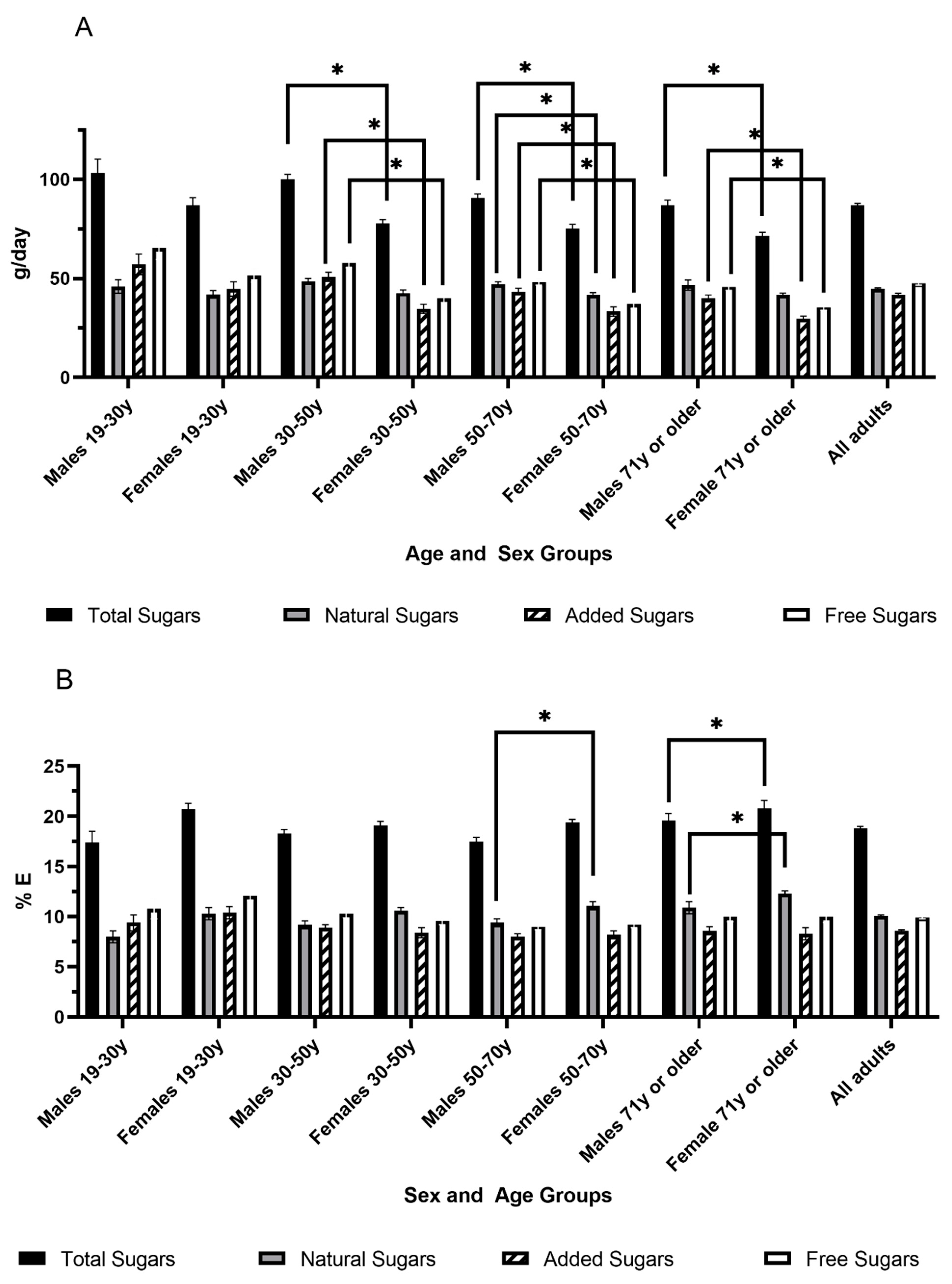
3.2. Consumption of Total, Free and Added Sugars by Age and Sex Groups
3.3. Consumption of Major Sugars-Containing Foods Categories
3.4. Consumption of Macronutrients and Micronutrients
4. Discussion
4.1. Canadian Consumption of Sugars
4.2. Food Categories
4.3. Macronutrient Intakes Across Different Total Sugars Intake Levels
4.4. Micronutrient Intakes Across Different Total Sugars Intake Levels
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sievenpiper, J.L. Sickeningly Sweet: Does Sugar Cause Chronic Disease? No. Can. J. Diabetes 2016, 40, 287–295. [Google Scholar] [CrossRef]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2012, 346, e7492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, T.A.S.; Sievenpiper, J.L. Controversies about Sugars: Results from Systematic Reviews and Meta-Analyses on Obesity, Cardiometabolic Disease and Diabetes. Eur. J. Nutr. 2016, 55, 25–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Corte, K.W.; Perrar, I.; Penczynski, K.J.; Schwingshackl, L.; Herder, C.; Buyken, A.E. Effect of Dietary Sugar Intake on Biomarkers of Subclinical Inflammation: A Systematic Review and Meta-Analysis of Intervention Studies. Nutrients 2018, 10, 606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015, 351, h3576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [Green Version]
- Jayalath, V.H.; De Souza, R.J.; Ha, V.; Mirrahimi, A.; Blanco-Mejia, S.; Di Buono, M.; Jenkins, A.L.; Leiter, L.A.; Wolever, T.M.; Beyene, J.; et al. Sugar-sweetened beverage consumption and incident hypertension: A systematic review and meta-analysis of prospective cohorts. Am. J. Clin. Nutr. 2015, 102, 914–921. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.K.; Willett, W.; Curhan, G. Fructose-rich beverages and risk of gout in women. JAMA 2010, 304, 2270–2278. [Google Scholar] [CrossRef] [Green Version]
- Xi, B.; Huang, Y.; Reilly, K.H.; Li, S.; Zheng, R.; Barrio-Lopez, M.T.; Martinez-Gonzalez, M.A.; Zhou, D. Sugar-sweetened beverages and risk of hypertension and CVD: A dose-response meta-analysis. Br. J. Nutr. 2015, 113, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Kim, S.A.; Ha, J.; Lim, K. Sugar-Sweetened Beverage Consumption in Relation to Obesity and Metabolic Syndrome among Korean Adults: A Cross-Sectional Study from the 2012–2016 Korean National Health and Nutrition Examination Survey (KNHANES). Nutrients 2018, 10, 1467. [Google Scholar] [CrossRef] [Green Version]
- Seo, E.H.; Kim, H.; Kwon, O. Association between Total Sugar Intake and Metabolic Syndrome in Middle-Aged Korean Men and Women. Nutrients 2019, 11, 2042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sievenpiper, J.L.; De Souza, R.J.; Mirrahimi, A.; Yu, M.E.; Carleton, A.J.; Beyene, J.; Chiavaroli, L.; Di Buono, M.; Jenkins, A.L.; Leiter, L.A.; et al. Effect of fructose on body weight in controlled feeding trials: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 156, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Sievenpiper, J.L.; Carleton, A.J.; Chatha, S.; Jiang, H.Y.; De Souza, R.J.; Beyene, J.; Kendall, C.W.; Jenkins, D.J. Heterogeneous effects of fructose on blood lipids in individuals with type 2 diabetes: Systematic review and meta-analysis of experimental trials in humans. Diabetes Care 2009, 32, 1930–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiavaroli, L.; De Souza, R.J.; Ha, V.; Cozma, A.I.; Mirrahimi, A.; Wang, D.D.; Yu, M.; Carleton, A.J.; Di Buono, M.; Jenkins, A.L.; et al. Effect of Fructose on Established Lipid Targets: A Systematic Review and Meta-Analysis of Controlled Feeding Trials. J. Am. Hear. Assoc. 2015, 4, e001700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, V.; Sievenpiper, J.L.; De Souza, R.J.; Chiavaroli, L.; Wang, D.D.; Cozma, A.I.; Mirrahimi, A.; Yu, M.E.; Carleton, A.J.; Dibuono, M.; et al. Effect of fructose on blood pressure: A systematic review and meta-analysis of controlled feeding trials. Hypertension 2012, 59, 787–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.D.; Sievenpiper, J.L.; De Souza, R.J.; Chiavaroli, L.; Ha, V.; Cozma, A.I.; Mirrahimi, A.; Yu, M.E.; Carleton, A.J.; Di Buono, M.; et al. The effects of fructose intake on serum uric acid vary among controlled dietary trials. J. Nutr. 2012, 142, 916–923. [Google Scholar] [CrossRef] [Green Version]
- Cozma, A.I.; Sievenpiper, J.L.; de Souza, R.J.; Chiavaroli, L.; Ha, V.; Wang, D.D.; Mirrahimi, A.; Yu, M.E.; Carleton, A.J.; Di Buono, M.; et al. Effect of fructose on glycemic control in diabetes: A systematic review and meta-analysis of controlled feeding trials. Diabetes Care 2012, 35, 1611–1620. [Google Scholar] [CrossRef] [Green Version]
- David Wang, D.; Sievenpiper, J.L.; de Souza, R.J.; Cozma, A.I.; Chiavaroli, L.; Ha, V.; Mirrahimi, A.; Carleton, A.J.; Di Buono, M.; Jenkins, A.L.; et al. Effect of fructose on postprandial triglycerides: A systematic review and meta-analysis of controlled feeding trials. Atherosclerosis 2014, 232, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Chiu, S.; Sievenpiper, J.L.; de Souza, R.J.; Cozma, A.I.; Mirrahimi, A.; Carleton, A.J.; Ha, V.; Di Buono, M.; Jenkins, A.L.; Leiter, L.A.; et al. Effect of fructose on markers of non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of controlled feeding trials. Eur. J. Clin. Nutr. 2014, 68, 416–423. [Google Scholar] [CrossRef]
- Hu, F.B. Resolved: There is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes. Rev. 2013, 14, 606–619. [Google Scholar] [CrossRef]
- Liu, Q.; Ayoub-Charette, S.; Khan, T.A.; Au-Yeung, F.; Blanco Mejia, S.; de Souza, R.J.; Wolever, T.M.S.; Leiter, L.A.; Kendall, C.W.C.; Sievenpiper, J.L. Important Food Sources of Fructose-Containing Sugars and Incident Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. J. Am. Hear. Assoc. 2019, 8, e010977. [Google Scholar] [CrossRef] [PubMed]
- Ayoub-Charette, S.; Liu, Q.; Khan, T.A.; Au-Yeung, F.; Blanco Mejia, S.; de Souza, R.J.; Wolever, T.M.; Leiter, L.A.; Kendall, C.; Sievenpiper, J.L. Important food sources of fructose-containing sugars and incident gout: A systematic review and meta-analysis of prospective cohort studies. BMJ Open 2019, 9, e024171. [Google Scholar] [CrossRef] [Green Version]
- Choo, V.L.; Viguiliouk, E.; Blanco Mejia, S.; Cozma, A.I.; Khan, T.A.; Ha, V.; Wolever, T.M.S.; Leiter, L.A.; Vuksan, V.; Kendall, C.W.C.; et al. Food sources of fructose-containing sugars and glycaemic control: Systematic review and meta-analysis of controlled intervention studies. BMJ 2018, 363, k4644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Sugars Intake for Adult and Children: Guideline; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th Edition; December 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 16 April 2020).
- Scientific Advisory Committee on Nutrition. SACN Carbohydrates and Health Report; The Stationery Office: London, UK, 2015. Available online: https://www.gov.uk/government/publications/sacn-carbohydrates-and-health-report (accessed on 16 April 2020).
- Tappy, L.; Morio, B.; Azzout-Marniche, D.; Champ, M.; Gerber, M.; Houdart, S.; Mas, E.; Rizkalla, S.; Slama, G.; Mariotti, F.; et al. French Recommendations for Sugar Intake in Adults: A Novel Approach Chosen by ANSES. Nutrients 2018, 10, 989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012. Available online: https://norden.diva-portal.org/smash/get/diva2:704251/FULLTEXT01.pdf (accessed on 16 April 2020).
- Erickson, J.; Sadeghirad, B.; Lytvyn, L.; Slavin, J.; Johnston, B.C. The Scientific Basis of Guideline Recommendations on Sugar Intake: A Systematic Review. Ann. Intern. Med. 2017, 166, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.R. Review of the scientific evidence used for establishing US policies on added sugars. Nutr. Rev. 2019, 77, 646–661. [Google Scholar] [CrossRef]
- Kearns, C.; Schillinger, D. Guidelines to Limit Added Sugar Intake. Ann. Intern. Med. 2017, 167, 220. [Google Scholar] [CrossRef]
- Wittekind, A.; Walton, J. Worldwide trends in dietary sugars intake. Nutr. Res. Rev. 2014, 27, 330–345. [Google Scholar] [CrossRef] [Green Version]
- Powell, E.S.; Smith-Taillie, L.P.; Popkin, B.M. Added Sugars Intake across the Distribution of US Children and Adult Consumers: 1977-2012. J. Acad. Nutr. Diet. 2016, 116, 1543–1550. [Google Scholar] [CrossRef] [Green Version]
- Moshtaghian, H.; Louie, J.C.Y.; Charlton, K.E.; Probst, Y.C.; Gopinath, B.; Mitchell, P.; Flood, V.M. Trends in added sugar intake and food sources in a cohort of older Australians: 15 years of follow-up from the Blue Mountains Eye Study. J. Hum. Nutr. Diet. 2017, 30, 339–348. [Google Scholar] [CrossRef]
- Bailey, R.L.; Jun, S.; Eldridge, A.L. The 2016 Feeding Infants and Toddlers Study (FITS): Dietary Intakes and Practices of Children in the United States from Birth to 48 Months. In Nurturing a Healthy Generation of Children: Research Gaps and Opportunities; Karger Publishers: Basel, Switzerland, 2019; Volume 91, pp. 99–109. [Google Scholar] [CrossRef]
- Lei, L.; Rangan, A.; Flood, V.M.; Louie, J.C. Dietary intake and food sources of added sugar in the Australian population. Br. J. Nutr. 2016, 115, 868–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Nutrition Foundation. Summary of Key Findings from the NDNS Report of Years 7 and 8 (combined). In British Nutrition Foundation News Reports; British Nutrition Foundation: London, UK, 2018. [Google Scholar]
- Sluik, D.; van Lee, L.; Engelen, A.I.; Feskens, E.J. Total, Free, and Added Sugar Consumption and Adherence to Guidelines: The Dutch National Food Consumption Survey 2007–2010. Nutrients 2016, 8, 70. [Google Scholar] [CrossRef]
- Langlois, K.; Garriguet, D.; Gonzalez, A.; Sinclair, S.; Colapinto, C.K. Change in total sugars consumption among Canadian children and adults. Health Rep. 2019, 30, 10–19. [Google Scholar]
- Canadian Foundation for Dietetic Research (CFDR). Canadian Foundation of Dietetic Research. Tracking Nutrition Trends (TNT) Report; Canadian Foundation for Dietetic Research (CFDR): Toronto, ON, Canada, 2018. [Google Scholar]
- Statistics Canada. 2015 Canadian Community Health Survey (CCHS)—Nutrition. User Guide; Statistics Canada: Ottawa, ON, Canada, 2017.
- United States Department of Agriculture. AMPM—USDA Automated Multiple-Pass Method; United States Department of Agriculture: Washington, DC, USA, 2019.
- Statistics Canada. Canadian Community Health Survey—Nutrition: Public Use Microdata File, 2015; Statistics Canada: Ottawa, ON, Canada, 2018.
- Health Canada. Reference Guide to Understanding and Using the Data—2015 Canadian Community Health Survey (Nutrition). Available online: https://www.canada.ca/content/dam/hc-sc/documents/services/food-nutrition/food-nutrition-surveillance/ReferenceGuide2015CCHS-Nutr_Eng_Final_06192017.pdf (accessed on 16 April 2020).
- Statistics Canada. Canadian Community Health Survey—Nutrition (CCHS). Detailed Information for 2015. Available online: https://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=5049 (accessed on 16 April 2020).
- Health Canada. Canadian Nutrient File—About Us; Health Canada: Montréal, QC, Canada, 2015.
- Garriguet, D. Accounting for misreporting when comparing energy intake across time in Canada. Health Rep. 2018, 29, 3–12. [Google Scholar]
- Louie, J.C.; Moshtaghian, H.; Boylan, S.; Flood, V.M.; Rangan, A.M.; Barclay, A.W.; Brand-Miller, J.C.; Gill, T.P. A systematic methodology to estimate added sugar content of foods. Eur. J. Clin. Nutr. 2015, 69, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients); National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Bilodeau, M.; Brenner, D. Theory of Multivariate Statistics; Springer: New York, NY, USA, 1999. [Google Scholar]
- National Cancer Institute. Usual Dietary Intakes: SAS Macros for Estimating Ratios of Two Dietary Components That Are Consumed Nearly Every Day. Available online: https://epi.grants.cancer.gov/diet/usualintakes/macros_double.html (accessed on 16 April 2020).
- Brisbois, T.D.; Marsden, S.L.; Anderson, G.H.; Sievenpiper, J.L. Estimated intakes and sources of total and added sugars in the Canadian diet. Nutrients 2014, 6, 1899–1912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Food Information Council. 2019 Food and Health Survey. Available online: https://foodinsight.org/wp-content/uploads/2019/05/IFIC-Foundation-2019-Food-and-Health-Report-FINAL.pdf (accessed on 16 April 2020).
- Bergeron, A.; Labonte, M.E.; Brassard, D.; Bedard, A.; Laramee, C.; Robitaille, J.; Desroches, S.; Provencher, V.; Couillard, C.; Vohl, M.C.; et al. Intakes of Total, Free, and Naturally Occurring Sugars in the French-Speaking Adult Population of the Province of Quebec, Canada: The PREDISE Study. Nutrients 2019, 11, 2317. [Google Scholar] [CrossRef] [Green Version]
- Charbonneau, H.D.B.; Légaré, J.; Denis, H. A Population History of North America; Cambridge University Press: New York, NY, USA, 2000. [Google Scholar]
- Beaudry, M.; Galibois, I.; Chaumette, P. Dietary Patterns of Adults in Québec and their Nutritional Adequacy. Can. J. Public Health 1997, 89, 347–351. [Google Scholar] [CrossRef]
- Bailey, R.L.; Fulgoni, V.L.; Cowan, A.; Gaine, P. Sources of Added Sugars in Young Children, Adolescents, and Adults with Low and High Intakes of Added Sugars. Nutrients 2018, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- Kibblewhite, R.; Nettleton, A.; McLean, R.; Haszard, J.; Fleming, E.; Kruimer, D.; Te Morenga, L. Estimating Free and Added Sugar Intakes in New Zealand. Nutrients 2017, 9, 1292. [Google Scholar] [CrossRef] [Green Version]
- Chatelan, A.; Gaillard, P.; Kruseman, M.; Keller, A. Total, Added, and Free Sugar Consumption and Adherence to Guidelines in Switzerland: Results from the First National Nutrition Survey menuCH. Nutrients 2019, 11, 1117. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, E.; Rodriguez, P.; Valero, T.; Avila, J.M.; Aranceta-Bartrina, J.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Dietary Intake of Individual (Free and Intrinsic) Sugars and Food Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 275. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, A.; Murakami, K.; Asakura, K.; Uechi, K.; Sugimoto, M.; Wang, H.C.; Masayasu, S.; Sasaki, S. Estimation of Starch and Sugar Intake in a Japanese Population Based on a Newly Developed Food Composition Database. Nutrients 2018, 10, 1474. [Google Scholar] [CrossRef] [Green Version]
- Seidelmann, S.B.; Folsom, A.R.; Rimm, E.B.; Willett, W.C.; Solomon, S.D. Dietary carbohydrate intake and mortality: Reflections and reactions—Authors’ reply. Lancet Public Health 2018, 3, e521. [Google Scholar] [CrossRef]
- Sadler, M.J.; McNulty, H.; Gibson, S. Sugar-fat seesaw: A systematic review of the evidence. Crit. Rev. Food Sci. Nutr. 2015, 55, 338–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Canada. Fibre. Available online: https://www.canada.ca/en/health-canada/services/nutrients/fibre.html (accessed on 16 April 2020).
- Slavin, J. Fiber and prebiotics: Mechanisms and health benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [Green Version]
- Gianfredi, V.; Salvatori, T.; Villarini, M.; Moretti, M.; Nucci, D.; Realdon, S. Is dietary fibre truly protective against colon cancer? A systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2018, 69, 904–915. [Google Scholar] [CrossRef] [PubMed]
- Threapleton, D.E.; Greenwood, D.C.; Evans, C.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Cade, J.E.; Gale, C.P.; Burley, V.J. Dietary fibre intake and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ 2013, 347, f6879. [Google Scholar] [CrossRef] [Green Version]
- InterAct, C. Dietary fibre and incidence of type 2 diabetes in eight European countries: The EPIC-InterAct Study and a meta-analysis of prospective studies. Diabetologia 2015, 58, 1394–1408. [Google Scholar] [CrossRef] [Green Version]
- Priebe, M.G.; van Binsbergen, J.J.; de Vos, R.; Vonk, R.J. Whole grain foods for the prevention of type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2008, 1, 1–33. [Google Scholar] [CrossRef] [Green Version]
- Aeberli, I.; Gerber, P.A.; Hochuli, M.; Kohler, S.; Haile, S.R.; Gouni-Berthold, I.; Berthold, H.K.; Spinas, G.A.; Berneis, K. Low to moderate sugar-sweetened beverage consumption impairs glucose and lipid metabolism and promotes inflammation in healthy young men: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 479–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, M.; Hammersley, R.; Duffy, M.; Ballantyne, C. Effects on obese women of the sugar sucrose added to the diet over 28 d: A quasi-randomised, single-blind, controlled trial. Br. J. Nutr. 2014, 111, 563–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, M.; Hammersley, R.; Hill, A.J.; Skidmore, P. Long-term dietary compensation for added sugar: Effects of supplementary sucrose drinks over a 4-week period. Br. J. Nutr. 2007, 97, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njike, V.Y.; Faridi, Z.; Shuval, K.; Dutta, S.; Kay, C.D.; West, S.G.; Kris-Etherton, P.M.; Katz, D.L. Effects of sugar-sweetened and sugar-free cocoa on endothelial function in overweight adults. Int. J. Cardiol. 2011, 149, 83–88. [Google Scholar] [CrossRef]
- Health Canada. Vitamin D and Calcium: Updated Dietary Reference Intakes. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/vitamins-minerals/vitamin-calcium-updated-dietary-reference-intakes-nutrition.html (accessed on 16 April 2020).
- Tanase, C.M.; Koski, K.G.; Laffey, P.J.; Cooper, M.J.; Cockell, K.A. Canadians Continue to Consume Too Much Sodium and Not Enough Potassium. Can. J. Public Health 2011, 102, 164–168. [Google Scholar] [CrossRef]
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Liu, S.; Looker, A.C.; Wallace, T.C.; Wang, D.D. Calcium plus vitamin D supplementation and risk of fractures: An updated meta-analysis from the National Osteoporosis Foundation. Osteoporos Int. 2016, 27, 367–376. [Google Scholar] [CrossRef] [Green Version]
- Hofmeyr, G.J.; Lawrie, T.A.; Atallah, A.N.; Duley, L.; Torloni, M.R. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2014, 6. [Google Scholar] [CrossRef]
- Bonovas, S.; Fiorino, G.; Lytras, T.; Malesci, A.; Danese, S. Calcium supplementation for the prevention of colorectal adenomas: A systematic review and meta-analysis of randomized controlled trials. World J. Gastroenterol 2016, 22, 4594–4603. [Google Scholar] [CrossRef]
- Bolland, M.J.; Avenell, A.; Baron, J.A.; Grey, A.; MacLennan, G.S.; Gamble, G.D.; Reid, I.R. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: Meta-analysis. BMJ 2010, 341, c3691. [Google Scholar] [CrossRef] [Green Version]
- Asemi, Z.; Saneei, P.; Sabihi, S.S.; Feizi, A.; Esmaillzadeh, A. Total, dietary, and supplemental calcium intake and mortality from all-causes, cardiovascular disease, and cancer: A meta-analysis of observational studies. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 623–634. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Avenell, A. Effects of vitamin D supplementation on musculoskeletal health: A systematic review, meta-analysis, and trial sequential analysis. Lancet Diabetes Endocrinol. 2018, 6, 847–858. [Google Scholar] [CrossRef] [Green Version]
- Mirhosseini, N.; Rainsbury, J.; Kimball, S.M. Vitamin D Supplementation, Serum 25(OH)D Concentrations and Cardiovascular Disease Risk Factors: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2018, 5, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.J.; Iyer, G.; Liu, Y.; Kalyani, R.R.; Bamba, N.; Ligon, C.B.; Varma, S.; Mathioudakis, N. The effect of vitamin D supplementation on glucose metabolism in type 2 diabetes mellitus: A systematic review and meta-analysis of intervention studies. J. Diabetes Complicat. 2017, 31, 1115–1126. [Google Scholar] [CrossRef] [PubMed]
- Franco, A.S.; Freitas, T.Q.; Bernardo, W.M.; Pereira, R.M.R. Vitamin D supplementation and disease activity in patients with immune-mediated rheumatic diseases: A systematic review and meta-analysis. Medicine 2017, 96, e7024. [Google Scholar] [CrossRef] [PubMed]
- Vatanparast, H.; Islam, N.; Patil, R.P.; Shafiee, M.; Whiting, S.J. Calcium Intake from Food and Supplemental Sources Decreased in the Canadian Population from 2004 to 2015. J. Nutr. 2019, 150, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Vatanparast, H.; Dolega-Cieszkowski, J.H.; Whiting, S.J. Many adult Canadians are not meeting current calcium recommendations from food and supplement intake. Appl. Physiol. Nutr. Metab. 2009, 34, 191–196. [Google Scholar] [CrossRef]
- Jayedi, A.; Ghomashi, F.; Zargar, M.S.; Shab-Bidar, S. Dietary sodium, sodium-to-potassium ratio, and risk of stroke: A systematic review and nonlinear dose-response meta-analysis. Clin. Nutr. 2019, 38, 1092–1100. [Google Scholar] [CrossRef]
- Gibson, S.A. Dietary sugars intake and micronutrient adequacy: A systematic review of the evidence. Nutr. Res. Rev. 2007, 20, 121–131. [Google Scholar] [CrossRef] [Green Version]
- Fulgoni, V.L., III; Gaine, P.C.; Scott, M.O.; Ricciuto, L.; DiFrancesco, L. Association of Added Sugars Intake with Micronutrient Adequacy in US Children and Adolescents: NHANES 2009–2014. Curr. Dev. Nutr. 2019, 3. [Google Scholar] [CrossRef]
- Wong, T.H.T.; Mok, A.; Ahmad, R.; Rangan, A.; Louie, J.C.Y. Intake of free sugar and micronutrient dilution in Australian children and adolescents. Eur. J. Nutr. 2019, 58, 2485–2495. [Google Scholar] [CrossRef]
- Eldridge, A.L.; Catellier, D.J.; Hampton, J.C.; Dwyer, J.T.; Bailey, R.L. Trends in Mean Nutrient Intakes of US Infants, Toddlers, and Young Children from 3 Feeding Infants and Toddlers Studies (FITS). J. Nutr. 2019, 149, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Canada, S. Research Data Centre. Available online: https://www.statcan.gc.ca/eng/microdata/data-centres (accessed on 16 April 2020).
- Bingham, S.A.; Gill, C.; Welch, A.; Day, K.; Cassidy, A.; Khaw, K.T.; Sneyd, M.J.; Key, T.J.; Roe, L.; Day, N.E. Comparison of dietary assessment methods in nutritional epidemiology: Weighed records v. 24 h recalls, food-frequency questionnaires and estimated-diet records. Br. J. Nutr. 1994, 72, 619–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Q1 | Q3 | Q5 | Model 1 | Model 2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N = 2364 | N = 2363 | N = 2364 | ||||||||||||
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |||||||||
| Food Category | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | p-Value ** | p-Value ** |
| Pasta, rice, cereal grains and flour | 112.3 | 83.6, 141.0 | 100.4 ¥ | 75.5, 125.2 | 83.9 | 71.7, 96.2 | 74.3 ¥ | 64.0, 84.7 | 53.6 | 41.5, 65.8 | 49.4 | 39.3, 59.4 | <0.0001 | <0.0001 |
| White breads | 21.0 | 17.7, 24.3 | 20.6 | 15.6, 25.6 | 31.2 | 22.5, 39.9 | 32.1 | 26.6, 37.7 | 22.9 | 19.6, 26.3 | 24.3 | 21.4, 27.3 | 0.1833 | 0.067 |
| Wholemeal breads | 21.6 | 18.0, 25.2 | 23.5 | 20.6, 26.4 | 21.7 | 15.9, 27.6 | 22.9 | 18.1, 27.7 | 16.6 | 12.8, 20.5 | 18.2 | 14.6, 21.8 | 0.0519 | 0.114 |
| Other breads | 43.9 | 36.6, 51.1 | 40.4 ¥ | 34.5, 46.2 | 35.4 | 25.8, 45.1 | 32.6 | 24.5, 40.8 | 26.7 | 21.6, 31.9 | 26.8 | 22.9, 30.8 | <0.0001 | 0.001 |
| Wholegrain and high fibre breakfast cereals | 15.0 | 8.0, 22.0 | 16.0 | 8.7, 23.3 | 19.7 | 13.6, 25.9 | 19.7 | 13.6, 25.8 | 18.6 | 15.2, 21.9 | 19.9 | 16.4, 23.3 | 0.6212 | 0.787 |
| Other breakfast cereals | 1.1 | 0.1, 2.1 | 1.1 ¥ | 0.2, 2.1 | 1.9 | 0.7, 3.1 | 2.0 | 0.7, 3.3 | 2.8 | 1.6, 4.0 | 3.0 | 1.8, 4.2 | 0.0068 | 0.004 |
| Cookies, biscuits and granola bars | 7.0 | 4.7, 9.3 | 7.1 ¥ | 5.3, 8.8 | 10.1 | 8.2, 12.0 | 10.2 | 7.8, 12.5 | 11.2 | 9.3, 13.2 | 11.7 | 9.9, 13.6 | <0.0001 | <0.0001 |
| Cakes, pies, danishes and other pastries | 13.3 | 9.7, 16.9 | 14.4 ¥,£ | 8.7, 20.0 | 30.4 | 25.2, 35.7 | 30.9 | 26.0, 35.8 | 35.7 | 28.6, 42.8 | 38.3 | 31.1, 45.4 | <0.0001 | <0.0001 |
| Frozen dairy products | 2.3 | 1.1, 3.5 | 1.8 ¥,£ | 0.6, 3.1 | 16.1 | 8.0, 24.2 | 15.8 | 9.3, 22.4 | 22.6 | 17.7, 27.5 | 23.2 | 17.9, 28.6 | <0.0001 | <0.0001 |
| Milks | 58.7 | 49.6, 67.9 | 56.4 ¥,£ | 47.0, 65.9 | 170.7 | 154.2, 187.2 | 169.7 | 154.0, 185.3 | 190.5 | 161.4, 219.5 | 198.4 | 170.5, 226.3 | <0.0001 | <0.0001 |
| Yogurts (natural and with fruits) | 11.4 | 7.0, 15.7 | 12.7 ¥ | 9.0, 16.4 | 26.8 | 18.9, 34.7 | 26.3 | 17.0, 35.6 | 33.3 | 26.9, 39.6 | 33.4 | 27.5, 39.4 | <0.0001 | <0.0001 |
| Fruit | 59.7 | 51.9, 67.5 | 56.1 ¥,£ | 48.3, 63.9 | 160.4 | 145.0, 175.8 | 152.7 ¥ | 139.6, 165.8 | 223.6 | 202.4, 244.7 | 224.2 | 203.8, 244.6 | <0.0001 | <0.0001 |
| Sugars, syrups, preserves | 4.4 | 3.6, 5.1 | 3.8 ¥,£ | 2.6, 4.9 | 10.7 | 9.2, 12.2 | 10.5 ¥ | 9.2, 11.7 | 20.4 | 16.8, 24.1 | 20.7 | 17.2, 24.2 | <0.0001 | <0.0001 |
| Confectionary | 2.5 | 1.7, 3.3 | 2.5 ¥,£ | 1.3, 3.6 | 9.1 | 6.0, 12.2 | 8.9 ¥ | 6.1, 11.7 | 24.2 | 17.5, 30.9 | 24.7 | 18.0, 31.3 | <0.0001 | <0.0001 |
| Fruit juice | 23.4 | 15.6, 31.3 | 17.4 | 10.1, 24.7 | 58.9 | 51.1, 66.8 | 54.8 ¥ | 47.3, 62.3 | 112.6 | 96.6, 128.5 | 112.2 | 96.8, 127.6 | <0.0001 | <0.0001 |
| Alcoholic beverages | 326.8 | 244.2, 409.5 | 311.0 ¥,£ | 233.6, 388.4 | 116.2 | 79.5, 152.9 | 114.5 ¥ | 96.1, 132.9 | 52.5 | 34.9, 70.1 | 59.5 | 42.9, 76.1 | <0.0001 | <0.0001 |
| Tea, coffee | 1511.1 | 1441.0, 1581.2 | 1482.4 ¥ | 1414.5, 1550.2 | 1555.6 | 1460.9, 1650.4 | 1523.1 ¥ | 1451.0, 1595.2 | 1308.7 | 1240.5, 1377.0 | 1305.1 | 1243.4, 1366.8 | <0.0001 | <0.0001 |
| Soft drinks, regular | 24.5 | 15.6, 33.4 | 12.1 ¥,£ | 0.7, 25.0 | 60.6 | 48.5, 72.6 | 58.5 ¥ | 41.4, 75.7 | 190.4 | 139.3, 241.5 | 191.9 | 144.4, 239.4 | <0.0001 | <0.0001 |
| Soft drinks, diet | 55.4 | 38.2, 72.6 | 55.7 | 40.9, 70.6 | 40.6 | 18.1, 63.0 | 43.5 | 23.4, 63.6 | 21.8 | 11.1, 32.5 | 26.3 | 15.3, 37.3 | 0.0109 | 0.014 |
| Fruit drinks | 11.1 | 4.1, 18.2 | 9.8 ¥ | 3.5, 16.1 | 18.2 | 10.0, 26.3 | 17.9 ¥ | 9.6, 26.1 | 53.5 | 39.9, 67.0 | 54.4 | 40.0, 68.8 | <0.0001 | <0.0001 |
| Other beverages | 3.4 | 0.8, 6.0 | 0.2 | 5.5, 5.8 | 9.5 | 0.1, 19.0 | 8.9 | 0.2, 18.0 | 27.1 | 3.5, 57.6 | 27.0 | 0.2, 53.7 | 0.0065 | 0.014 |
| Soups | 39.3 | 32.3, 46.3 | 41.5 | 34.2, 48.7 | 39.6 | 26.5, 52.7 | 41.3 | 27.7, 54.9 | 41.7 | 30.8, 52.6 | 43.1 | 33.4, 52.8 | 0.0571 | 0.088 |
| Q1 | Q3 | Q5 | Model 1 | Model 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N = 2364 | N = 2363 | N = 2364 | ||||||||||||
| Model 1 | Model 3 | Model 1 | Model 3 | Model 1 | Model 3 | |||||||||
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | p-value ** | p-value ** | |
| Energy (kcal) | 1953.8 | 1903.8, 2003.8 | 1854.6 | 1819.1,1890.1 | 1919.2 | 1819.9, 2018.5 | 1893.7 ¥ | 1828.8,1958.5 | 1805.5 | 1763.9, 1847.2 | 1823.1 | 1789.6, 1856.6 | <0.0001 | 0.012 |
| Carbohydrates (%) | 38.9 | 37.2, 40.5 | 38.9 ¥,£ | 37.4, 40.4 | 47.7 | 46.0, 49.4 | 47.6 ¥ | 46.3, 49.0 | 58.4 | 57.6, 59.3 | 58.3 | 57.5, 59.2 | <0.0001 | <0.0001 |
| Total Fibre (g/1000 kcal) | 8.6 | 8.2, 8.9 | 8.9 ¥,£ | 8.5, 9.2 | 10.1 | 9.4, 10.9 | 10.1 | 9.6, 10.6 | 10.3 | 9.9, 10.8 | 10.3 | 9.9, 10.7 | <0.0001 | <0.0001 |
| Total Sugars (%) | 7.9 | 7.7, 8.1 | 7.8 ¥,£ | 7.7, 8.0 | 18.3 | 18.3, 18.4 | 18.4 ¥ | 18.2, 18.5 | 33.0 | 32.4, 33.7 | 33.0 | 32.5, 33.6 | <0.0001 | <0.0001 |
| Natural Sugars (%) | 4.8 | 4.6, 5.0 | 5.0 ¥,£ | 4.8, 5.2 | 10.2 | 9.7, 10.7 | 10.1 ¥ | 9.8, 10.5 | 15.6 | 15.0, 16.3 | 15.7 | 15.0, 16.3 | <0.0001 | <0.0001 |
| Added Sugars (%) | 3.0 | 2.8, 3.1 | 2.8 ¥,£ | 2.6, 3.0 | 8.1 | 7.6, 8.6 | 8.2 ¥ | 7.8, 8.5 | 17.3 | 16.5, 18.1 | 17.3 | 16.5, 18.0 | <0.0001 | <0.0001 |
| Free Sugars (%) | 3.2 | 3.1, 3.4 | 3.0 ¥,£ | 2.8, 3.2 | 9.2 | 8.7, 9.7 | 9.2 ¥ | 8.8, 9.6 | 20.1 | 19.2, 20.9 | 20.0 | 19.2, 20.8 | <0.0001 | <0.0001 |
| Fat (%) | 36.1 | 35.1, 37.2 | 36.2 ¥,£ | 35.3, 37.1 | 32.2 | 31.1, 33.2 | 32.3 ¥ | 31.5, 33.1 | 26.4 | 25.7, 27.1 | 26.4 | 25.8, 27.0 | <0.0001 | <0.0001 |
| Saturated Fat (%) | 11.3 | 10.8, 11.7 | 11.4 ¥,£ | 11.0, 11.7 | 10.4 | 9.9, 11.0 | 10.5 ¥ | 10.1, 10.9 | 9.0 | 8.8, 9.3 | 9.1 | 8.8, 9.4 | <0.0001 | <0.0001 |
| Monounsaturated Fat (%) | 13.8 | 13.4, 14.3 | 13.8 ¥,£ | 13.4, 14.2 | 12.0 | 11.5, 12.5 | 12.0 ¥ | 11.6, 12.4 | 9.4 | 9.0, 9.8 | 9.4 | 9.0, 9.8 | <0.0001 | <0.0001 |
| Polyunsaturated Fat (%) | 7.8 | 7.4, 8.1 | 7.9 ¥,£ | 7.5, 8.2 | 6.8 | 6.6, 7.0 | 6.9 ¥ | 6.7, 7.1 | 5.5 | 5.2, 5.7 | 5.4 | 5.2, 5.7 | <0.0001 | <0.0001 |
| Linoleic acid (%) | 6.6 | 6.3, 7.0 | 6.7 ¥,£ | 6.4, 7.0 | 5.7 | 5.6, 5.9 | 5.8 ¥ | 5.6, 5.9 | 4.6 | 4.4, 4.9 | 4.6 | 4.4, 4.9 | <0.0001 | <0.0001 |
| Alpha, linolenic Acid (%) | 0.8 | 0.8, 0.8 | 0.8 ¥ | 0.8, 0.9 | 0.8 | 0.7, 0.8 | 0.8 ¥ | 0.7, 0.8 | 0.6 | 0.6, 0.7 | 0.6 | 0.6, 0.7 | <0.0001 | <0.0001 |
| Protein (%) | 18.8 | 17.9, 19.7 | 18.7 ¥ | 18.0, 19.5 | 17.5 | 17.1, 17.9 | 17.4 ¥ | 16.9, 17.9 | 13.9 | 13.3, 14.5 | 14.0 | 13.5, 14.4 | <0.0001 | <0.0001 |
| Cholesterol (mg/1000 kcal) | 178.1 | 162.6, 193.6 | 175.9 ¥ | 164.0, 187.8 | 153.2 | 139.5, 167.0 | 151.5 ¥ | 137.0, 165.9 | 109.9 | 101.2, 118.7 | 109.9 | 101.7, 118.1 | <0.0001 | <0.0001 |
| Alcohol (%) | 6.2 | 4.8, 7.6 | 6.2 ¥,£ | 4.8, 7.5 | 2.6 | 2.0, 3.3 | 2.7 ¥ | 2.2, 3.2 | 1.3 | 0.7, 1.8 | 1.3 | 0.8, 1.8 | <0.0001 | <0.0001 |
| Micronutrients: Per 1000 kcal | ||||||||||||||
| Vitamin A (ug RAE) | 338.9 | 298.5, 379.4 | 349.9 £ | 311.0, 388.7 | 370.6 | 349.8, 391.5 | 371.0 | 346.6, 395.5 | 378.7 | 340.8, 416.7 | 376.8 | 340.6, 413.1 | <0.0001 | <0.0001 |
| Thiamin (mg) | 0.9 | 0.8, 0.9 | 0.9 | 0.8, 0.9 | 0.9 | 0.8, 0.9 | 0.9 | 0.8, 1.0 | 0.8 | 0.8, 0.9 | 0.8 | 0.8, 0.9 | 0.003 | 0.006 |
| Riboflavin (mg) | 1.0 £ | 1.0, 1.0 | 1.0 | 1.0, 1.1 | 1.1 | 1.1, 1.1 | 1.1 | 1.1, 1.1 | 1.1 | 1.0, 1.1 | 1.1 | 1.0, 1.1 | <0.0001 | <0.0001 |
| Niacin (mg) | 23.7 | 22.6, 24.8 | 23.7 ¥,£ | 22.6, 24.7 | 21.7 | 20.9, 22.5 | 21.7 ¥ | 21.0, 22.4 | 18.0 | 17.4, 18.5 | 18.0 | 17.5, 18.5 | <0.0001 | <0.0001 |
| Vitamin B,6 (mg) | 0.9 | 0.9, 1.0 | 0.9 | 0.9, 1.0 | 1.0 | 0.9, 1.0 | 0.9 | 0.9, 1.0 | 0.9 | 0.9, 0.9 | 0.9 | 0.9, 0.9 | 0.070 | 0.019 |
| Folate (ug DFE) | 247.8 ¥ | 238.8,256.8 | 246.9 | 238.0, 255.8 | 242.8 | 228.1, 257.5 | 240.0 ¥ | 226.7, 253.4 | 221.9 | 210.8, 233.1 | 219.0 | 207.2, 230.9 | <0.0001 | <0.0001 |
| Vitamin B,12 (mg) | 2.3 | 2.1,2.5 | 2.3 | 2.0, 2.6 | 2.4 | 2.1, 2.6 | 2.4 ¥ | 2.1, 2.6 | 1.9 | 1.7, 2.0 | 1.9 | 1.7, 2.0 | 0.013 | 0.011 |
| Vitamin C (mg) | 35.9 ¥,£ | 32.3,39.5 | 36.4 | 33.0, 39.9 | 56.2 | 50.2, 62.2 | 55.0 | 50.2, 59.9 | 85.1 | 74.0, 96.2 | 84.5 | 73.9, 95.2 | <0.0001 | <0.0001 |
| Vitamin D (ug) | 2.3 ¥,£ | 1.9,2.8 | 2.5 | 2.1, 2.8 | 2.7 | 2.5, 2.9 | 2.8 | 2.6, 2.9 | 2.6 | 2.4, 2.8 | 2.6 | 2.5, 2.8 | <0.0001 | <0.0001 |
| Calcium (mg) | 370.8 ¥,£ | 347.9,393.8 | 380.1 | 360.0, 400.3 | 439.8 | 421.8, 457.9 | 442.6 | 423.9, 461.3 | 458.2 | 441.6, 474.9 | 459.2 | 442.3, 476.2 | <0.0001 | <0.0001 |
| Iron (mg) | 6.7 ¥ | 6.5,6.9 | 6.8 | 6.6, 7.0 | 6.9 | 6.7, 7.2 | 6.9 ¥ | 6.7, 7.2 | 6.3 | 6.1, 6.5 | 6.3 | 6.1, 6.5 | <0.0001 | <0.0001 |
| Magnesium (mg) | 167.3 | 161.2,173.4 | 170.0 | 165.2, 174.9 | 177.7 | 170.7, 184.6 | 176.8 | 170.4, 183.2 | 169.7 | 163.9, 175.1 | 169.9 | 164.6, 175.1 | <0.0001 | 0.007 |
| Phosphorus (mg) | 696.2 ¥ | 671.7,720.6 | 706.4 | 682.0, 370.8 | 704.8 | 688.8, 720.8 | 707.4¥ | 692.9, 722.0 | 652.0 | 635.5, 668.5 | 655.2 | 639.2, 671.1 | <0.0001 | <0.0001 |
| Potassium (mg) | 1378.1 ¥,£ | 1336.1,1420.0 | 1409.6 | 1365.0,1454.2 | 1536.7 | 1495.6,1577.8 | 1541.3 | 1506.0, 1576.6 | 1611.8 | 1560.3, 1663.3 | 1619.2 | 1570.0, 1668.4 | <0.0001 | <0.0001 |
| Zinc (mg) | 6.0 ¥ | 5.8, 6.2 | 6.0 | 5.8, 6.2 | 5.7 | 5.5, 5.9 | 5.7 ¥ | 5.6, 5.9 | 4.8 | 4.6, 5.0 | 4.8 | 4.7, 5.0 | <0.0001 | <0.0001 |
| Sodium (mg) | 1621.9 ¥,£ | 1567.9,1675.8 | 1629.0 | 1580.6,1677.5 | 1512.0 | 1473.5,1550.6 | 1523.2 ¥ | 1486.1, 1560.4 | 1255.1 | 1215.3, 1294.3 | 1257.4 | 1216.8, 1298.0 | <0.0001 | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Chiavaroli, L.; Roke, K.; DiAngelo, C.; Marsden, S.; Sievenpiper, J. Canadian Adults with Moderate Intakes of Total Sugars have Greater Intakes of Fibre and Key Micronutrients: Results from the Canadian Community Health Survey 2015 Public Use Microdata File. Nutrients 2020, 12, 1124. https://doi.org/10.3390/nu12041124
Wang Y, Chiavaroli L, Roke K, DiAngelo C, Marsden S, Sievenpiper J. Canadian Adults with Moderate Intakes of Total Sugars have Greater Intakes of Fibre and Key Micronutrients: Results from the Canadian Community Health Survey 2015 Public Use Microdata File. Nutrients. 2020; 12(4):1124. https://doi.org/10.3390/nu12041124
Chicago/Turabian StyleWang, Ye (Flora), Laura Chiavaroli, Kaitlin Roke, Chiara DiAngelo, Sandra Marsden, and John Sievenpiper. 2020. "Canadian Adults with Moderate Intakes of Total Sugars have Greater Intakes of Fibre and Key Micronutrients: Results from the Canadian Community Health Survey 2015 Public Use Microdata File" Nutrients 12, no. 4: 1124. https://doi.org/10.3390/nu12041124