Adaptation and Validation of Alternative Healthy Eating Index in Hemodialysis Patients (AHEI-HD) and Its Association with all-Cause Mortality: A Multi-Center Follow-Up Study

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
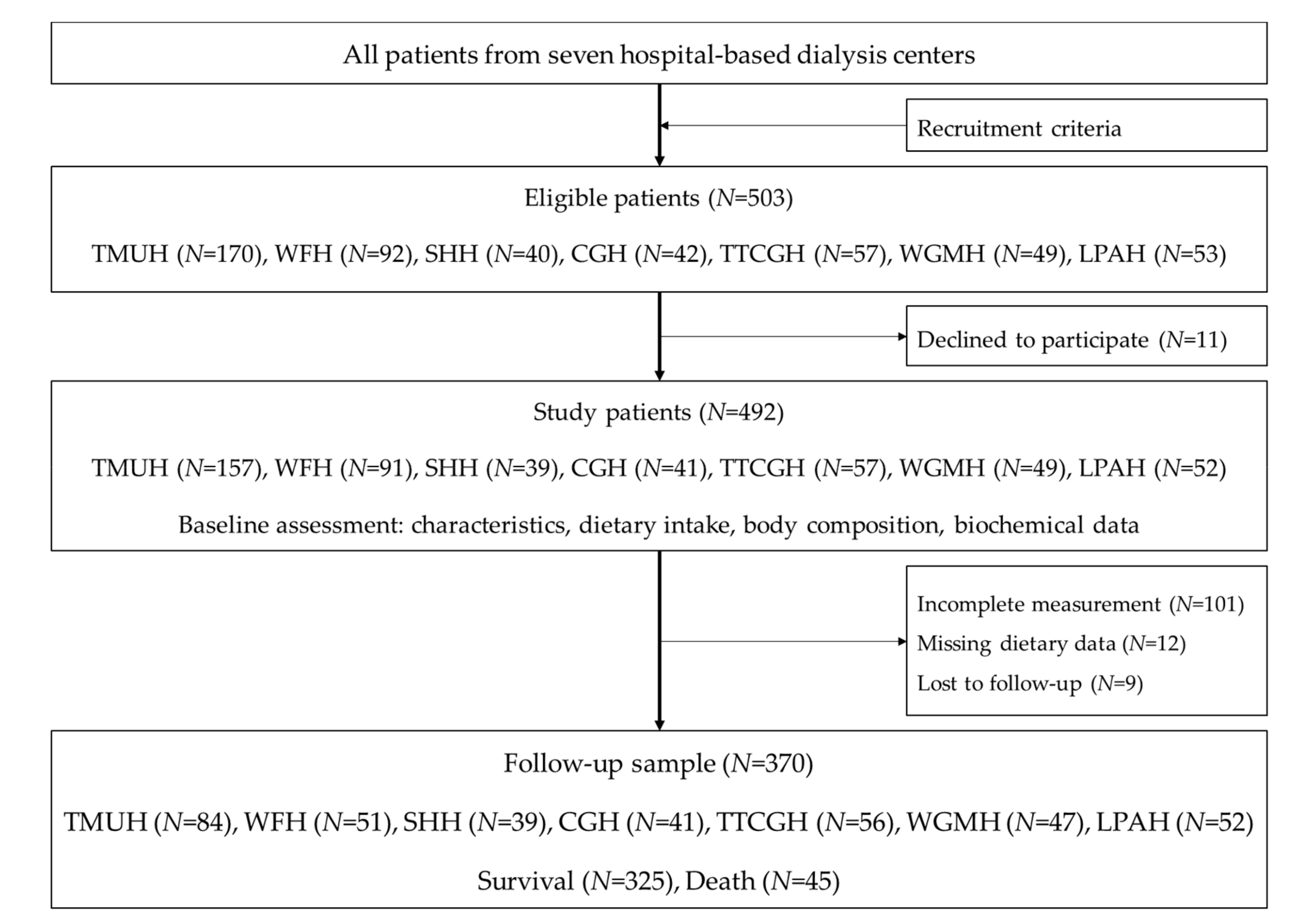
2.1. Study Design and Settings
2.2. Study Patients
2.3. Assessments and Measurements
2.4. Patients’ Characteristics
2.5. Body Composition
2.6. Biochemical Parameters
2.7. The Alternative Healthy Eating Index (AHEI) in Hemodialysis Patients
2.8. Statistical Analysis
2.9. Ethical Approvals
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United States Renal Data System. International Comparisons. The 2016 Annual Data Report: Epidemiology of Kidney Disease in the United States: Volume 2—End-Stage Renal Disease (ESRD) in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, USRDS Coordinating Center: Bethesda, MD, USA, 2016. [Google Scholar]
- United States Renal Data System. 2016 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, USRDS Coordinating Center: Bethesda, MD, USA, 2016. [Google Scholar]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Lacson, E., Jr.; Ikizler, T.A.; Lazarus, J.M.; Teng, M.; Hakim, R.M. Potential Impact of Nutritional Intervention on End-Stage Renal Disease Hospitalization, Death, and Treatment Costs. J. Ren. Nutr. 2007, 17, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, N.; Geelen, A.; Streppel, M.T.; de Groot, L.C.P.G.M.; Orfanos, P.; van den Hooven, E.H.; Pikhart, H.; Boffetta, P.; Trichopoulou, A.; Bobak, M.; et al. Adherence to a Healthy Diet According to the World Health Organization Guidelines and All-Cause Mortality in Elderly Adults From Europe and the United States. Am. J. Epidemiol. 2014, 180, 978–988. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; The Office of Disease Prevention and Health Promotion: Washington, DC, USA, 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines (accessed on 31 December 2015).
- Ministry of Health and Welfare. Daily Food Guide 2018; Health Promotion Administration, Ministry of Health and Welfare: Taipei, Taiwan, 2018. Available online: https://www.hpa.gov.tw/Pages/EBook.aspx?nodeid=1208 (accessed on 31 December 2015).
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Willett, W.C. Evaluating adherence to recommended diets in adults: The Alternate Healthy Eating Index. Public Health Nutr. 2006, 9, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Varraso, R.; Chiuve, S.E.; Fung, T.T.; Barr, R.G.; Hu, F.B.; Willett, W.C.; Camargo, C.A. Alternate Healthy Eating Index 2010 and risk of chronic obstructive pulmonary disease among US women and men: Prospective study. BMJ 2015, 350, 286. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Boushey, C.J.; Wilkens, L.R.; Haiman, C.A.; Le Marchand, L. High-Quality Diets Associate With Reduced Risk of Colorectal Cancer: Analyses of Diet Quality Indexes in the Multiethnic Cohort. Gastroenterology 2017, 153, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Onvani, S.; Haghighatdoost, F.; Surkan, P.J.; Larijani, B.; Azadbakht, L. Adherence to the Healthy Eating Index and Alternative Healthy Eating Index dietary patterns and mortality from all causes, cardiovascular disease and cancer: A meta-analysis of observational studies. J. Hum. Nutr. Diet. 2017, 30, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Kivimaki, M.; Akbaraly, T. Alternate Healthy Eating Index 2010, Dietary Inflammatory Index and risk of mortality: Results from the Whitehall II cohort study and meta-analysis of previous Dietary Inflammatory Index and mortality studies. Br. J. Nutr. 2017, 118, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Akbaraly, T.N.; Ferrie, J.E.; Berr, C.; Brunner, E.J.; Head, J.; Marmot, M.G.; Singh-Manoux, A.; Ritchie, K.; Shipley, M.J.; Kivimaki, M. Alternative Healthy Eating Index and mortality over 18 y of follow-up: Results from the Whitehall II cohort. Am. J. Clin. Nutr. 2011, 94, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Krebs-Smith, S.M.; Miller, P.E.; Liese, A.D.; Kahle, L.L.; Park, Y.; Subar, A.F. Higher diet quality is associated with decreased risk of all-cause, cardiovascular disease, and cancer mortality among older adults. J. Nutr. 2014, 144, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: An Updated Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2018, 118, 74–100. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Moio, M.R.; Fois, A.; Sofronie, A.; Gendrot, L.; Cabiddu, G.; D’Alessandro, C.; Cupisti, A. The Diet and Haemodialysis Dyad: Three Eras, Four Open Questions and Four Paradoxes. A Narrative Review, Towards a Personalized, Patient-Centered Approach. Nutrients 2017, 9, 372. [Google Scholar] [CrossRef] [PubMed]
- Duong, T.V.; Wong, T.C.; Su, C.T.; Chen, H.H.; Chen, T.W.; Chen, T.H.; Hsu, Y.H.; Peng, S.J.; Kuo, K.L.; Liu, H.C.; et al. Associations of dietary macronutrients and micronutrients with the traditional and nontraditional risk factors for cardiovascular disease among hemodialysis patients: A clinical cross-sectional study. Medicine 2018, 97, 11306. [Google Scholar] [CrossRef] [PubMed]
- Liou, Y.M.; Jwo, C.J.C.; Yao, K.G.; Chiang, L.C.; Huang, L.H. Selection of Appropriate Chinese Terms to Represent Intensity and Types of Physical Activity Terms for Use in the Taiwan Version of IPAQ. J. Nurs. Res. 2008, 16, 252–263. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, T.P.; Potischman, N.; Douglass, D.; Dixit-Joshi, S.; Kirkpatrick, S.I.; Subar, A.F.; McNutt, S.; Coleman, L.A.; Alexander, G.L.; Kushi, L.H.; et al. The Effect of Editing Open-Ended Text Responses on Nutrient and Food Group Estimates from the Automated Self-Administered 24-Hour Dietary Recall (ASA24). Procedia Food Sci. 2015, 4, 160–172. [Google Scholar] [CrossRef] [Green Version]
- Duong, T.V.; Wong, T.C.; Chen, H.H.; Chen, T.W.; Chen, T.H.; Hsu, Y.H.; Peng, S.J.; Kuo, K.L.; Liu, H.C.; Lin, E.T.; et al. Inadequate dietary energy intake associates with higher prevalence of metabolic syndrome in different groups of hemodialysis patients: A clinical observational study in multiple dialysis centers. BMC Nephrol. 2018, 19, 236. [Google Scholar] [CrossRef]
- Chiu, Y.F.; Chen, Y.C.; Wu, P.Y.; Shih, C.K.; Chen, H.H.; Chen, H.H.; Chen, T.H.; Yang, S.H. Association Between the Hemodialysis Eating Index and Risk Factors of Cardiovascular Disease in Hemodialysis Patients. J. Ren. Nutr. 2014, 24, 163–171. [Google Scholar] [CrossRef]
- Wong, T.C.; Su, H.Y.; Chen, Y.T.; Wu, P.Y.; Chen, H.H.; Chen, T.H.; Hsu, Y.H.; Yang, S.H. Ratio of C-Reactive Protein to Albumin Predicts Muscle Mass in Adult Patients Undergoing Hemodialysis. PLoS ONE 2016, 11, e0165403. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Food and Drug Administration. Food Nutrition Database; Ministry of Health and Welfare: Taipei, Taiwan, 2018. Available online: https://consumer.fda.gov.tw/Food/TFND.aspx?nodeID=178 (accessed on 31 December 2018).
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M.; Reeve, B.B. Evaluation of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1854–1864. [Google Scholar] [CrossRef]
- Wu, P.Y.; Huang, C.L.; Lei, W.S.; Yang, S.H. Alternative health eating index and the Dietary Guidelines from American Diabetes Association both may reduce the risk of cardiovascular disease in type 2 diabetes patients. J. Hum. Nutr. Diet. 2016, 29, 363–373. [Google Scholar] [CrossRef] [PubMed]
- K/DOQI Workgroup. K/DOQI Clinical Practice Guidelines for Nutrition in Chronic Renal Failure. Am. J. Kidney Dis. 2000, 35, S1–S140. [Google Scholar]
- Biruete, A.; Jeong, J.H.; Barnes, J.L.; Wilund, K.R. Modified Nutritional Recommendations to Improve Dietary Patterns and Outcomes in Hemodialysis Patients. J. Ren. Nutr. 2017, 27, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.P.; Willett, W.C.; Hu, F.B. Sugar-Sweetened Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Li, Y.; Pan, A.; De Koning, L.; Schernhammer, E.; Willett, W.C.; Hu, F.B. Long-Term Consumption of Sugar-Sweetened and Artificially Sweetened Beverages and Risk of Mortality in US Adults. Circulation 2019, 139, 2113–2125. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; Ghissassi, F.E.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Orsini, N. Red Meat and Processed Meat Consumption and All-Cause Mortality: A Meta-Analysis. Am. J. Epidemiol. 2014, 179, 282–289. [Google Scholar] [CrossRef]
- Wang, X.; Lin, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G.; Pan, A.; Hu, F.B. Red and processed meat consumption and mortality: Dose–response meta-analysis of prospective cohort studies. Public Health Nutr. 2015, 19, 893–905. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, A.H.; Appel, L.J.; Brands, M.; Carnethon, M.; Daniels, S.; Franch, H.A.; Franklin, B.; Kris-Etherton, P.; Harris, W.S.; Howard, B.; et al. Diet and Lifestyle Recommendations Revision 2006: A Scientific Statement From the American Heart Association Nutrition Committee. Circulation 2006, 114, 82. [Google Scholar] [CrossRef] [PubMed]
- Khor, B.H.; Narayanan, S.S.; Sahathevan, S.; Gafor, A.H.A.; Daud, Z.A.M.; Khosla, P.; Sabatino, A.; Fiaccadori, E.; Chinna, K.; Karupaiah, T. Efficacy of Nutritional Interventions on Inflammatory Markers in Haemodialysis Patients: A Systematic Review and Limited Meta-Analysis. Nutrients 2018, 10, 397. [Google Scholar] [CrossRef] [PubMed]
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.M.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- Maraj, M.; Kuśnierz-Cabala, B.; Dumnicka, P.; Gala-Błądzińska, A.; Gawlik, K.; Pawlica-Gosiewska, D.; Ząbek-Adamska, A.; Mazur-Laskowska, M.; Ceranowicz, P.; Kuźniewski, M. Malnutrition, Inflammation, Atherosclerosis Syndrome (MIA) and Diet Recommendations among End-Stage Renal Disease Patients Treated with Maintenance Hemodialysis. Nutrients 2018, 10, 69. [Google Scholar] [CrossRef]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Maldonado, G.; Greenland, S. Simulation Study of Confounder-Selection Strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef] [Green Version]
- Lopes, A.A.; Bragg-Gresham, J.L.; Elder, S.J.; Ginsberg, N.; Goodkin, D.A.; Pifer, T.; Lameire, N.; Marshall, M.R.; Asano, Y.; Akizawa, T.; et al. Independent and Joint Associations of Nutritional Status Indicators With Mortality Risk Among Chronic Hemodialysis Patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). J. Ren. Nutr. 2010, 20, 224–234. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (N = 370) | Survival (N = 325) | Death (N = 45) | p-value 1 |
|---|---|---|---|---|
| Age, years | 60.7 ± 11.9 | 60.0 ± 11.8 | 66.0 ± 12.0 | 0.002 |
| Gender, male | 208 (56.2) | 179 (55.1) | 29 (64.4) | 0.235 |
| Hemodialysis vintage, year | 5.7 ± 4.9 | 5.9 ± 5.1 | 4.4 ± 2.9 | 0.060 |
| CCI | 4.7 ± 1.6 | 4.6 ± 1.5 | 5.5 ± 1.6 | <0.001 |
| PA, MET-min/wk | 4964.9 ± 1871.9 | 5082.6 ± 1872.4 | 4114.2 ± 1651.4 | 0.001 |
| BMI, kg/m2 | 23.6 ± 3.9 | 23.6 ± 3.9 | 23.0 ± 3.5 | 0.348 |
| Body composition | ||||
| FFM, kg | 44.1 ± 11.1 | 44.0 ± 11.1 | 45.1 ± 9.1 | 0.507 |
| BFM, kg | 17.9 ± 8.3 | 18.1 ± 8.5 | 16.4 ± 7.4 | 0.212 |
| Laboratory parameters | ||||
| hs-CRP, mg/dL | 0.25 (0.11–0.60) | 0.24 (0.10–0.52) | 0.52 (0.16–1.00) | 0.003 |
| Hgb, g/dL | 10.7 ± 1.1 | 10.8 ± 1.1 | 10.5 ± 1.3 | 0.174 |
| FBG (mg/dL) | 132.3 ± 58.4 | 131.9 ± 59.0 | 135.5 ± 54.9 | 0.697 |
| Insulin, µU/mL | 17.1 (8.8–31.7) | 17.9 (9.0–32.3) | 14.4 (7.2–28.0) | 0.165 |
| TG (mg/dL) | 159.6 ± 111.9 | 162.8 ± 115.2 | 136.3 ± 81.5 | 0.137 |
| HDL-C (mg/dL) | 39.9 ± 22.0 | 39.3 ± 21.8 | 43.9 ± 23.1 | 0.204 |
| LDL-C, mg/dL | 100.3 ± 31.7 | 101.1 ± 32.1 | 94.8 ± 28.2 | 0.212 |
| TC, mg/dL | 165.6 ± 35.2 | 166.2 ± 35.0 | 160.9 ± 36.4 | 0.347 |
| Ca, mg/dL | 9.3 (8.9 – 9.7) | 9.3 (8.7–9.7) | 9.3 (9.0–9.7) | 0.463 |
| PO4, mg/dL | 5.2 ± 1.2 | 5.2 ± 1.2 | 5.0 ± 1.3 | 0.381 |
| iPTH, pg/mL | 254.0 (95.9–450.8) | 266.5 (103.9–451.3) | 139.4 (53.0–407.0) | 0.063 |
| Hcy, µmol/L | 20.7 ± 6.7 | 20.6 ± 6.6 | 21.2 ± 7.6 | 0.616 |
| Albumin, g/dL | 4.0 ± 0.4 | 4.0 ± 0.4 | 3.9 ± 0.4 | 0.229 |
| Pre-BUN, mg/dL | 72.8 ± 19.7 | 72.8 ± 20.2 | 73.4 ± 16.0 | 0.829 |
| Creatinine, mg/dL | 11.1 ± 2.2 | 11.2 ± 2.2 | 10.2 ± 1.5 | 0.005 |
| K, mEq/L | 4.8 (4.3–5.2) | 4.8 (4.3–5.2) | 4.8 (4.3–5.2) | 0.876 |
| Uric acid, mg/dL | 7.3 ± 1.3 | 7.3 ± 1.3 | 6.8 ± 1.2 | 0.009 |
| eKt/V | 1.6 ± 0.3 | 1.6 ± 0.3 | 1.5 ± 0.2 | 0.038 |
| Component | Criteria | Actual Eating Index Distribution 1 | ||||
|---|---|---|---|---|---|---|
| Minimum Score of 0 | Maximum Score of 10 | Total (N = 370) | Survival (N = 325) | Death (N = 45) | p-value | |
| Whole fruits, serving/d 2 | 0 | ≥2–4 | 1.7 (0.3–2.9) | 1.8 (0.5–3.1) | 0.7 (0.0–2.2) | 0.007 |
| Total vegetables, serving/d 2 | 0 | ≥3–5 | 3.3 (2.0–5.0) | 3.3 (2.1–5.0) | 3.1 (1.8–5.0) | 0.590 |
| Whole grains, serving/d 3 | Highest decile | Lowest decile | 361 (97.6) | 318 (97.8) | 43 (95.6) | 0.350 |
| Sugar-sweetened beverages and fruit juice, serving/d 4 | >0 | 0 | 175 (47.3) | 150 (46.2) | 25 (55.6) | 0.236 |
| Nuts and legumes, serving/d 3,5 | Highest decile | Lowest decile | 269 (72.7) | 236 (72.6) | 33 (73.3) | 0.919 |
| Fresh red meat, serving/d 3 | ≥1.5 | <1.5 | 154 (41.6) | 139 (42.8) | 15 (33.3) | 0.229 |
| Processed meat, serving/d 6 | >0 | 0 | 160 (43.2) | 134 (41.2) | 26 (57.8) | 0.036 |
| Fish (EPA + DHA), serving/week | 0 | ≥1 | 209 (56.5) | 197 (60.6) | 12 (26.7) | <0.001 |
| UFAs rich foods, serving/d 2,4,7 | 0 | ≥4–8 | 3.5 (1.0–6.7) | 3.5 (0.9–6.5) | 3.4 (1.8–9.0) | 0.247 |
| Alcohol, drinks/d 8 | >0 | 0 | 358 (96.8) | 313 (96.3) | 45 (100.0) | 0.190 |
| Sodium, mg/d 5 | Highest decile | Lowest decile | 217 (58.6) | 193 (59.4) | 24 (46.7) | 0.440 |
| Total AHEI-2010 score | 0 | 110 | 64.7 ± 13.4 | 65.0 ± 13.3 | 62.5 ± 13.7 | 0.235 |
| Total Grains, serving/d 2 | 0 | ≥8–18 | 5.3 ± 1.9 | 5.4 ± 1.9 | 5.0 ± 1.8 | 0.185 |
| Total protein foods, serving/d 2 | 0 | ≥4.5–10 | 6.0 ± 2.3 | 6.0 ± 2.3 | 5.8 ± 2.5 | 0.636 |
| HBV proteins, % total protein 3 | 0 | ≥50 | 360 (97.3) | 318 (97.8) | 42 (93.3) | 0.080 |
| Dairy products, serving/d 3 | Highest decile | Lowest decile | 268 (72.4) | 237 (72.9) | 31(68.9) | 0.570 |
| SFAs rich foods, serving/d 4,7 | >0 | 0 | 195 (52.7) | 158 (48.6) | 37 (82.2) | <0.001 |
| Total AHEI-HD score | 0 | 160 | 98.7 ± 15.6 | 98.7 ± 15.6 | 98.7 ± 15.3 | 0.992 |
| Whole Fruits | Total Vegetables | Whole Grains | SSB and Fruit Juice | Nuts and Legumes | Fresh Red Meat | Processed Meat | Fish (EPA + DHA) | UFAs Rich Oils | Alcohol | Sodium | Total Grains | Total Protein Foods | HBV Proteins | Dairy Products | SFAs Rich Oils | AHEI-2010 | AHEI-HD | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total vegetables | 0.11 | |||||||||||||||||
| Whole grains | −0.01 | −0.01 | ||||||||||||||||
| SSB and fruit juice | −0.06 | 0.14 | 0.08 | |||||||||||||||
| Nuts and legumes | −0.07 | 0.01 | 0.08 | 0.28 | ||||||||||||||
| Fresh red meat | −0.08 | −0.09 | −0.01 | 0.05 | 0.01 | |||||||||||||
| Processed meat | 0.06 | 0.16 | −0.04 | 0.06 | 0.08 | 0.08 | ||||||||||||
| Fish (EPA + DHA) | 0.12 | 0.08 | 0.01 | −0.09 | −0.07 | 0.01 | −0.09 | |||||||||||
| UFAs rich oils | 0.06 | 0.23 | 0.01 | 0.09 | −0.03 | −0.07 | 0.07 | 0.07 | ||||||||||
| Alcohol | −0.06 | −0.04 | −0.03 | 0.05 | 0.09 | 0.12 | 0.04 | 0.00 | 0.06 | |||||||||
| Sodium | −0.01 | −0.13 | 0.01 | 0.03 | −0.01 | 0.11 | 0.10 | 0.10 | −0.11 | 0.08 | ||||||||
| Total Grains | 0.00 | 0.13 | 0.01 | −0.07 | −0.03 | −0.19 | −0.11 | 0.01 | 0.07 | 0.00 | −0.27 | |||||||
| Total protein foods | 0.06 | 0.21 | 0.03 | −0.15 | −0.05 | −0.46 | −0.19 | 0.23 | 0.19 | −0.08 | −0.29 | 0.27 | ||||||
| HBV proteins | 0.09 | 0.10 | −0.03 | −0.08 | −0.07 | −0.20 | 0.04 | 0.06 | 0.11 | −0.03 | 0.01 | 0.09 | 0.05 | |||||
| Dairy products | −0.03 | −0.03 | 0.05 | 0.14 | 0.04 | 0.05 | 0.06 | 0.07 | −0.02 | 0.05 | 0.01 | −0.05 | −0.06 | −0.06 | ||||
| SFAs rich oils | −0.07 | −0.07 | −0.01 | 0.10 | 0.08 | 0.05 | 0.12 | −0.14 | 0.37 | 0.10 | −0.07 | −0.13 | −0.12 | −0.06 | 0.07 | |||
| AHEI-2010 | 0.14 | 0.33 | 0.12 | 0.52 | 0.42 | 0.41 | 0.47 | 0.33 | 0.32 | 0.23 | 0.20 | −0.12 | −0.17 | −0.04 | 0.14 | 0.14 | ||
| AHEI-HD | 0.11 | 0.30 | 0.13 | 0.48 | 0.38 | 0.28 | 0.41 | 0.30 | 0.44 | 0.22 | 0.07 | −0.01 | −0.03 | −0.02 | 0.37 | 0.42 | 0.89 | |
| Total energy intake | 0.05 | 0.20 | 0.02 | −0.13 | −0.13 | −0.33 | −0.12 | 0.06 | 0.27 | −0.15 | −0.41 | 0.60 | 0.55 | 0.08 | −0.07 | −0.07 | −0.19 | −0.05 |
| AHEI-2010 | AHEI-HD | ||
|---|---|---|---|
| N | Mean ± SD | Mean ± SD | |
| Gender | |||
| Women | 162 | 66.4 ± 13.3 | 99.3 ± 14.7 |
| Men | 208 | 63.4 ± 13.3 | 98.2 ± 16.3 |
| p value | 0.031 | 0.492 | |
| Age | |||
| < 65 years | 239 | 63.3 ± 13.4 | 97.0 ± 15.9 |
| ≥ 65 years | 131 | 67.3 ± 13.0 | 101.8 ± 14.5 |
| p value | 0.006 | 0.004 | |
| DM history | |||
| Non-DM | 223 | 63.0 ± 12.6 | 96.7 ± 14.6 |
| DM | 147 | 67.3 ± 14.1 | 101.8 ± 16.5 |
| p value | 0.003 | 0.002 |
| Death | Model 1 | Model 2 | |||
|---|---|---|---|---|---|
| (N = 45) | HR (95% CI) | p | HR (95% CI) | p | |
| Categorical model | |||||
| Total AHEI-2010 score | |||||
| Tertile 1 (27.4–57.5) | 16 | Reference | Reference | ||
| Tertile 2 (57.5–71.1) | 18 | 0.97 (0.49–1.90) | 0.926 | 0.64 (0.31–1.34) | 0.237 |
| Tertile 3 (71.1–95.9) | 11 | 0.67 (0.31–1.45) | 0.308 | 0.40 (0.18–0.90) | 0.028 |
| Total AHEI-HD score | |||||
| Tertile 1 (64.1–91.6) | 15 | Reference | Reference | ||
| Tertile 2 (91.6–106.6) | 16 | 0.83 (0.41–1.70) | 0.616 | 0.57 (0.26–1.25) | 0.161 |
| Tertile 3 (106.6–135.0) | 14 | 0.71 (0.34–1.48) | 0.363 | 0.37 (0.17–0.82) | 0.014 |
| Continuous model | |||||
| Per each tertile increment in AHEI-2010 score | 45 | 0.83 (0.57–1.20) | 0.318 | 0.63 (0.42–0.95) | 0.027 |
| Per each tertile increment in AHEI-HD score | 45 | 0.84 (0.58–1.22) | 0.363 | 0.61 (0.41–0.91) | 0.016 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Duong, T.; Tseng, I.-H.; Wong, T.-C.; Chen, H.-H.; Chen, T.-H.; Hsu, Y.-H.; Peng, S.-J.; Kuo, K.-L.; Liu, H.-C.; Lin, E.-T.; et al. Adaptation and Validation of Alternative Healthy Eating Index in Hemodialysis Patients (AHEI-HD) and Its Association with all-Cause Mortality: A Multi-Center Follow-Up Study. Nutrients 2019, 11, 1407. https://doi.org/10.3390/nu11061407
Van Duong T, Tseng I-H, Wong T-C, Chen H-H, Chen T-H, Hsu Y-H, Peng S-J, Kuo K-L, Liu H-C, Lin E-T, et al. Adaptation and Validation of Alternative Healthy Eating Index in Hemodialysis Patients (AHEI-HD) and Its Association with all-Cause Mortality: A Multi-Center Follow-Up Study. Nutrients. 2019; 11(6):1407. https://doi.org/10.3390/nu11061407
Chicago/Turabian StyleVan Duong, Tuyen, I-Hsin Tseng, Te-Chih Wong, Hsi-Hsien Chen, Tso-Hsiao Chen, Yung-Ho Hsu, Sheng-Jeng Peng, Ko-Lin Kuo, Hsiang-Chung Liu, En-Tzu Lin, and et al. 2019. "Adaptation and Validation of Alternative Healthy Eating Index in Hemodialysis Patients (AHEI-HD) and Its Association with all-Cause Mortality: A Multi-Center Follow-Up Study" Nutrients 11, no. 6: 1407. https://doi.org/10.3390/nu11061407