Mechanisms Involved in the Relationship between Low Calcium Intake and High Blood Pressure
by

Cecilia Villa-Etchegoyen
1,*, 
Mercedes Lombarte
2,
Natalia Matamoros
3,
José M. Belizán
4 and
Gabriela Cormick
4,5 1
Laboratory of Cardiovascular Surveillance of Drugs, Department of Toxicology and Pharmacology, School of Medicine, Universidad de Buenos Aires, Ciudad Autonoma de Buenos Aires, Buenos Aires 1121, Argentina
2
Bone Biology Laboratory, School of Medicine, Rosario National University, Rosario, Santa Fe 3100, Argentina
3
Instituto de Desarrollo e Investigaciones Pediátricas “Prof. Dr. Fernando E. Viteri” Hospital de Niños “Sor María Ludovica de La Plata (IDIP), Ministerio de Salud/Comisión de Investigacines Científicas de la Provincia de Buenos Aires, La Plata, Buenos Aires 1900, Argentina
4
Department of Mother and Child Health Research, Institute for Clinical Effectiveness and Health Policy (IECS-CONICET), Ciudad Autonoma de Buenos Aires, Buenos Aires 1414, Argentina
5
Departamento de Salud, Universidad Nacional de La Matanza, Florencio Varela, San Justo 1903, Argentina
*
Author to whom correspondence should be addressed.
Nutrients 2019, 11(5), 1112; https://doi.org/10.3390/nu11051112
Submission received: 11 April 2019
/
Revised: 1 May 2019
/
Accepted: 16 May 2019
/
Published: 18 May 2019
(This article belongs to the Special Issue Nutrients Intake and Hypertension)
Abstract
:There is increasing epidemiologic and animal evidence that a low calcium diet increases blood pressure. The aim of this review is to compile the information on the link between low calcium intake and blood pressure. Calcium intake may regulate blood pressure by modifying intracellular calcium in vascular smooth muscle cells and by varying vascular volume through the renin–angiotensin–aldosterone system. Low calcium intake produces a rise of parathyroid gland activity. The parathyroid hormone increases intracellular calcium in vascular smooth muscles resulting in vasoconstriction. Parathyroidectomized animals did not show an increase in blood pressure when fed a low calcium diet as did sham-operated animals. Low calcium intake also increases the synthesis of calcitriol in a direct manner or mediated by parathyroid hormone (PTH). Calcitriol increases intracellular calcium in vascular smooth muscle cells. Both low calcium intake and PTH may stimulate renin release and consequently angiotensin II and aldosterone synthesis. We are willing with this review to promote discussions and contributions to achieve a better understanding of these mechanisms, and if required, the design of future studies.
1. Introduction
The relationship between calcium intake and blood pressure has been widely studied since the 1980s [1,2,3]. Dietary calcium has been shown to have an effect on blood pressure in animal studies. Normotensive rats fed a free-calcium diet significantly increased their systolic blood pressure (SBP) between 15 to 35 mmHg in comparison with rats fed with normal calcium diet [4,5,6]. On the other hand, normotensive and hypertensive rats supplemented with calcium had significant lower values of SBP [7,8,9,10]. Systematic reviews of calcium supplementation randomized controlled trials in hypertensive and normotensive populations have shown a consistent decrease of blood pressure, with a mean difference in systolic blood pressure (SBP) of 2.5 mmHg (95% confidence interval (CI) = 0.6–4.5) in hypertensive subjects and of 1.4 mmHg (95% (CI) = 0.72–2.15) in normotensive subjects [11,12]. In humans, even such a small reduction in blood pressure was estimated to be associated with about 10% lower stroke mortality and about 7% lower mortality from ischemic heart disease [13].
The effect of calcium supplementation on SBP was higher in people aged less than 35 years (−2.11 mmHg) and with doses of calcium equal to or over 1500 mg/day (−2.79 mmHg). The higher impact on BP reduction observed in these cases seem to be diluted in the overall revision due to these studies only representing approximately 20% of the participants [11]. Also, the vast majority of the included trials were performed in high-income countries that usually have a higher basal dietary calcium intake.
Most importantly this effect on blood pressure has been studied during pregnancy for the prevention of preeclampsia [14]. A systematic review of randomized controlled trials of calcium supplementation on the prevention of preeclampsia shows a large effect (13 trials, 15,730 women: RR = 0.45, 95% CI = 0.31–0.65) [15]. This evidence was used to update WHO guidelines for the prevention of preeclampsia, which include the recommendation to supplement pregnant women from areas with low calcium intake with 1.5 to 2 g of calcium per day during the second half of pregnancy [16,17]. Moreover, the follow up of children whose mothers were supplemented during pregnancy show noticeable effects on preventing high blood pressure and dental caries in the progeny [18,19]. Recently, the preconceptional and early pregnancy effect of a low calcium supplementation dose was studied in a multi-country randomized placebo controlled trial showing the beneficial effect of calcium before conception and throughout pregnancy [20]. All these effects of calcium intake have also been replicated in animal models so as to gain insight on the mechanisms that link calcium intake and blood pressure regulation [1,2,4,5,6].
The aim of this literature review is to contribute to finding the mechanisms that could explain the relationship between calcium intake and blood pressure.
2. Calcium and Blood Pressure Regulation
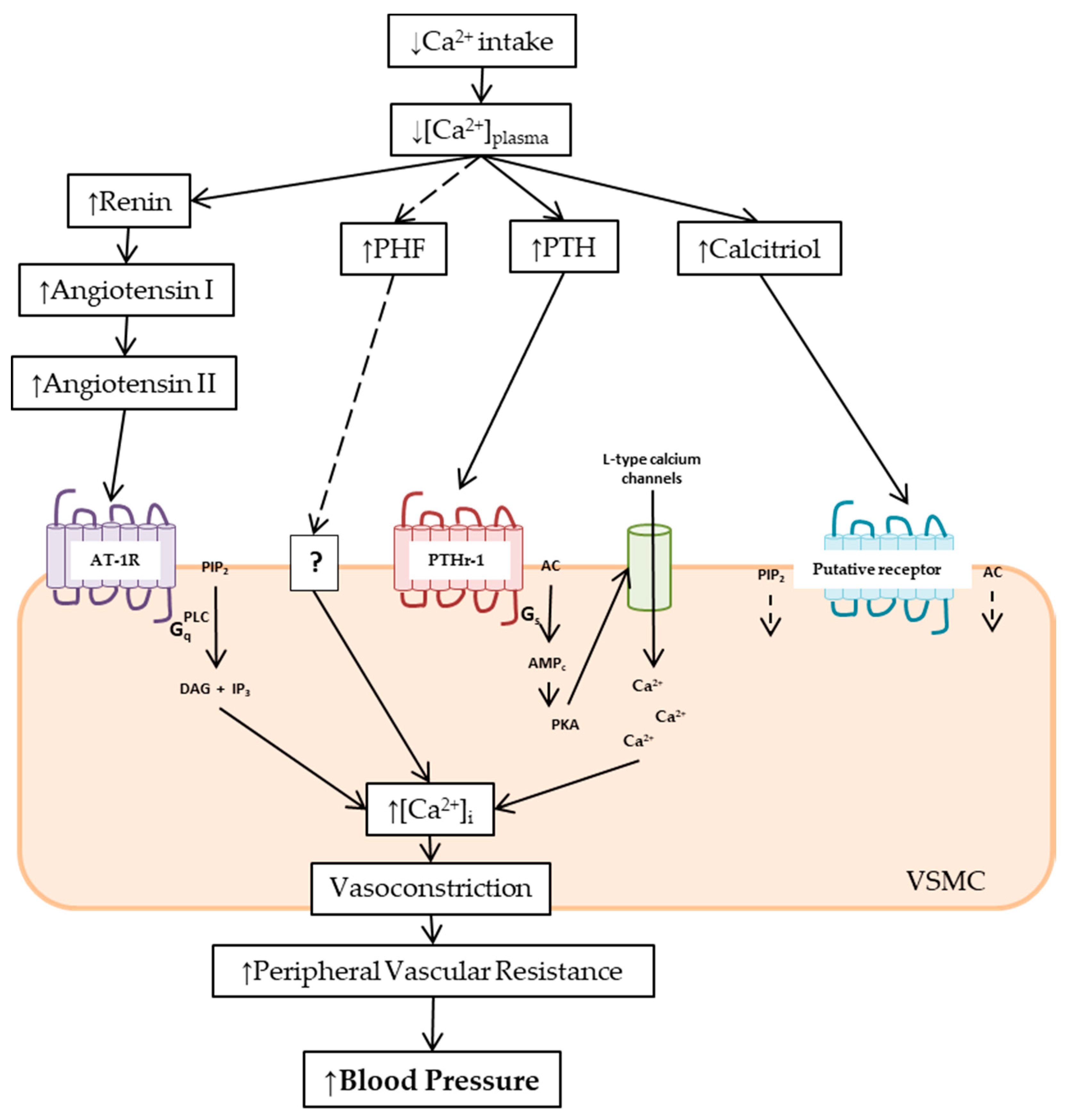
Calcium intake may regulate blood pressure by increasing intracellular calcium in vascular smooth muscle cells leading to vasoconstriction, and by increasing vascular volume through the renin–angiotensin–aldosterone system (RAAS). We found three major mechanisms explaining the relationship between a low calcium intake and the increase in blood pressure: (a) parathyroid function, (b) vitamin D, and (c) the renin–angiotensin–aldosterone system (RAAS). These three mechanisms are described below (Figure 1).
2.1. Calcium Intake and Parathyroid Function on Blood Pressure Regulation
Calcium intake has a role in blood pressure regulation and the parathyroid glands play a role in calcium homeostasis, thus the link between calcium intake, parathyroid function, and blood pressure seems to be intuitively valid. However, few studies have evaluated the pathways linking calcium intake, parathyroid function, and blood pressure altogether. The following section accounts for the physiological bases of this relationship, focusing on the effects of the parathyroid hormone (PTH) and the not completely purified and characterized parathyroid hypertensive factor (PHF).
2.1.1. Mechanisms Mediated by Parathyroid Hormone (PTH)
Several studies have reported that calcium intake is inversely associated with blood pressure, both in humans [3,11,12,21,22,23] and in animals [2,5,6]. The inverse relationship between calcium intake and plasma PTH levels has also been widely studied at different ages and physiological stages in both humans and animals, in acute and long term studies [24,25,26,27]. Similarly, the direct relationship between plasma PTH and blood pressure both in healthy subjects and animals is also well documented [25,28,29,30,31,32,33]. The relationship between the reported parathyroid hormone serum levels and blood pressure measurements in normotensive and hypertensive subjects is shown in Table 1. Studies showing a correlation between blood pressure values and quartiles and quintiles of parathyroid hormone levels in human studies are shown in Table 2. Some studies in humans have shown low calcium intake, increased PTH levels, and increased blood pressure in the same subjects, although no description of mechanisms involved in this relationship were mentioned [34,35,36] (Table 3).
Several studies have shown that PTH levels can independently predict cardiovascular disease and mortality [35,37,38,39]. The prospective and multicenter Osteoporotic Fractures in Men (MrOS) study, including 1490 men older than 65 years and followed up for 7.3 years, shows that concentrations of PTH were associated with an increased risk of cardiovascular mortality (adjusted hazard ratio SD = 1.21, 95% CI = 1.00–1.45) and from all causes (adjusted HR per SD = 1.15, 95% CI = 1.03–1.29) [37]. The Multi-Ethnic Study of Atherosclerosis (MESA) cohort study in which 3002 men and women, aged 59 ± 9.7 years, without cardiovascular antecedents were followed up for 9.0 years found that higher PTH serum concentrations were associated with a greater risk of hypertension, even after adjusting for potential confounders (HR = 1.27, 95% CI = 1.01–1.59) [39]. The population-based, cross-sectional Tromsø study including 3570 men and women aged 25–79 years found a positive relationship between serum PTH and SBP with the highest quartile of serum PTH found to be an independent predictor of coronary heart disease in both sexes (OR = 1.70, 95% CI = 1.08–2.70 for males, OR = 1.73, 95% CI = 1.04–2.88 for females, p < 0.05).
PTH is an 84-amino-acid polypeptide (≈9.5 kilodalton (kDa)) secreted by the chief cells of the parathyroid gland. PTH acts on the cell membrane of its target tissues through a G-protein-coupled receptor, the parathyroid hormone receptor type 1 (PTHr-1). Expression of PTH receptors has been reported in many tissues, including vascular smooth muscle and endothelial cells [40]. The PTHr-1 couples to several signaling pathways, namely: the Gαs/adenylate cyclase (AC)/cAMP/protein kinase A (PKA), the Gαq/phospholipase C (PLC)β/inositol trisphosphate (IP3)/intracellular Ca/protein kinase C (PKC), the Gα12/13 phospholipase D/RhoA pathway, and the mitogen-activated protein kinase (extracellular signal regulated kinase [ERK1/2]) signaling cascade [41,42].
Several mechanisms have been proposed to explain the effect of PTH on blood pressure: (a) an increase in cytosolic free calcium concentration ([Ca2+]i) through the PTH receptor (PTHr-1) in vascular smooth muscle, (b) increase calcitriol concentration, and (c) a cross-talk with the renin–angiotensin–aldosterone system (RAAS). The last two will be described in its corresponding sections.
High [Ca2+]i increases vascular reactivity, and therefore peripheral vascular resistance and responsiveness to the sympathetic and the RAAS, which all elevate blood pressure. Calcium channel blockers, such as nifedipine and verapamil, are valuable antihypertensive drugs as they inhibit Ca2+ entry to the cell and reduce [Ca2+]i. In the same way, calcium supplementation in subjects with low calcium intake has been described to decrease [Ca2+]i [43,44], hence diminishing blood pressure. It has been shown that PTH increases calcium entry into a variety of mammalian tissues and cell lines, such as cardiomyocytes [45], enterocytes [46], kidney [47], liver [48], peripheral nerves [49], osteosarcoma cells [50], and osteoblastlike cells [51]. Significantly higher [Ca2+]i was also found in human platelets and lymphocytes of hypertensive patients [29,52]. The activation of PTHr-1/Gq/PLC/IP3, PTHr-1/Gα12-13/phospholipase D/RhoA cascades, and of calcium channels are the signaling pathways by which PTH increases [Ca2+]i and blood pressure [47].
A controversial effect is the vasodilator effect of acute PTH infusion, both in vivo and in vitro. In vascular smooth muscle cells, PTHr-1 couples primarily to Gαs, which increases cAMP and decreases [Ca2+]i [53]. Nonetheless, the sustained activation of this cascade shows desensitization to PTH in a time- and concentration-dependent fashion [54,55,56]. The chronic infusion of PTH has been associated with arterial hypertension [57]. Long-standing high levels of PTH, such as in hyperparathyroidism, are frequently related to hypertension, whereas parathyroidectomy is associated with a decrease in [Ca2+]i and blood pressure [58]. A rise of [Ca2+]i through PTHr-1/Gαs/AC/cAMP via opening calcium channels in a cell line derived from fetal rat aorta was also described [59]. Therefore, the desensitization of the cAMP pathway to PTH, as well as the stimulation of other blood pressure mediators considered below, like the RAAS and calcitriol, may explain the long-term pressor effects of PTH.
2.1.2. Parathyroid Hypertensive Factor (PHF)
In the early 1990s, Lewanczuk et al. described that the infusion of plasma from hypertensive rats and from hypertensive subjects on normotensive rats increased the mean arterial pressure of those rats [60,61]. They attributed this effect to the presence of a novel hypertensive factor in the plasma of the hypertensive donors. The same group also reported the parathyroid origin of this factor by transplanting parathyroid glands from hypertensive rats into parathyroidectomized normotensive rats. An increase in blood pressure was shown in the rats after transplantation [60,62,63]. Due to this, the non-isolated substance was called parathyroid hypertensive factor (PHF) [60].
In spontaneously hypertensive rat strains, low calcium intake increases blood pressure that the authors explained was due to an increase of PFH [64]. These authors also proposed that PHF regulates blood pressure by modifying the concentration of [Ca2+]i in vascular smooth muscle [60,65,66]. In isolated vascular smooth muscle cells from rat tail arteries, Shan et al. found that the infusion of semi-purified plasma from hypertensive rats enhanced the opening of the L-type calcium channel, an effect antagonized by the dihydropyridine calcium channel blocker nifedipine [67].
Although the effect of plasma from hypertensive rats has been well-documented, the purification and characterization of PHF is uncomplete. Benishin et al. showed the correlation of a UV spectrum of dialyzed plasma from hypertensive rats with a small (≈3 kDa), trypsin-inactivated and boiled-resistant peptide [68]. Years later, the same group proposed that the PHF structure has both peptide and lysophospholid motifs, critical for its biological activity [69]. Schlüter et al. also isolated a peptide-like vasopressor of low molecular weight (0.6–2.5 kDa) from parathyroid tissue of patients with tertiary hyperparathyroidism. The eluent was shown to be polar, hydrophilic, and protease-sensitive, but not heat-resistant. Schlüter’s group also suggested that further purifications were needed as several substances were shown on the mass spectrometry [70].
Although the existence of PHF may explain the blood pressure changes induced by alterations in a calcium diet, there is still much to know about this mediator. First, the published results have been poorly replicated outside the group that described PHF [71]. On the other hand, after 30 years of being described, the definitive chemical structure of this mediator is still unknown and there have not been reports of new attempts to purify it. Nonetheless, the function of the parathyroid gland seems to play a key role in blood pressure regulation, as was reported both in humans and in normotensive and hypertensive animals.
In summary, the bulk of information of this section orients towards an increase of the parathyroid gland activity by low calcium intake leading to an increase of [Ca2+]i in vascular smooth muscle cells and consequently a rise in blood pressure (Figure 1). In addition to the direct effect of PTH (or PHF) in smooth muscle, we will later discuss the effects of PTH mediated by calcitriol and RAAS. A demonstration of the effect of parathyroid activity in the regulation of blood pressure related to calcium intake is shown in a study of parathyroidectomized rats in comparison with sham operation rats. After 10 weeks on a calcium-free diet, the sham operation rats showed an increase in SBP of 3.44 (SE = 1.95) mmHg, while the parathyroidectomized rats showed a decrease in SBP of −9.67 (SE = 2.05) mmHg. A highly statistical significant difference of 13.11 mmHg was found between the two groups [2].
2.2. Calcium Intake and Vitamin D in Blood Pressure Regulation
Most systematic reviews of randomized controlled trials do not show an effect of vitamin D supplementation on blood pressure. A systematic review of 46 trials (4541 participants) found no effect of vitamin D supplementation on SBP (effect size = 0.0 [95% CI = −0.8 to 0.8] mmHg; p = 0.97; I2 = 21%) or diastolic blood pressure (DBP) (effect size = −0.1 [95% CI = −0.6 to 0.5] mmHg; p = 0.84; I2 = 20%) nor in subgroup analysis via basal vitamin D or blood pressure levels [72]. A systematic review in hypertensive subjects did not find evidence of vitamin D supplementation on blood pressure [73]. However, one systematic review found that in vitamin D deficient populations, supplementation has a small effect on peripheral DBP but not in central DBP nor in peripheral nor central SBP, though this evidence is weak as it mainly comes from one small trial on vitamin D deficient and hypertensive subjects [74,75]. However, in these systematic reviews some population groups, such as those with vitamin D deficiency, might be underrepresented. One randomized, double-blind, placebo-controlled clinical trial of oral calcitriol in African-Americans with low baseline calcitriol level reported a significant decrease in SBP but not DBP after a three-month follow up [76].
Vitamin D is a steroid hormone that can be synthesized in the skin under the influence of sunlight (cholecalciferol or vitamin D3) or be obtained from foods such as fish and vegetables (ergocalciferol or vitamin D2). Later, a two-step hydroxylation is required to procure its biological active form (1,25-OHVitD, calcitriol). Low calcium intake increases calcitriol concentration, both in human and in animals [77,78,79]. PTH stimulates the renal α-1 hydroxylase enzyme to produce the final activation. However, PTH is probably not the sole regulator of calcitriol synthesis as an increase in the efficiency of calcium absorption has been described with low calcium intake diets even after parathyroidectomy [79]. The renal α-1 hydroxylase activity seems to be directly modulated by calcium, as the addition of calcium ions in vitro produced an inhibitory effect of the enzyme activity [80]. In addition, α-1 hydroxylase activity was found in tissues other than kidney such as endothelial cells. Vitamin D receptor (VDR) expression was described in endothelial cells. These findings could orient towards an auto/paracrine action of calcitriol in endothelial cells [81].
The effects of calcitriol are mediated by both genomic and nongenomic mechanisms. Genomic responses are mediated by intracellular vitamin D receptor (VDR) functioning as transcription factors to modulate gene expression, whilst the short-term effects seem to be mediated by putative receptors [82].
Among the rapid nongenomic effects, it has been shown that calcitriol increases [Ca2+]i by increasing calcium uptake in many types of cells, including rat vascular smooth muscle cells and aorta-derived cell lines [83,84,85]. The intraperitoneal administration of calcitriol on spontaneously hypertensive and normotensive rats enhanced the contractile response of isolated mesenteric resistance arteries, showing that the effect is not related to the hypertensive condition [86]. Furthermore, Shan et al. reported a significant increase in the calcium channel current of rat artery-derived smooth muscle cells after calcitriol infusion [87]. In skeletal muscle, calcitriol effects have been extensively studied showing that calcitriol: (a) stimulates L-type voltage-operated calcium channels by cAMP pathway, (b) activates AC/cAMP/PKA and PLC/IP3/PKC signaling cascades, and (c) boosts the calcium messenger system [88], all of which are responsible for the increase of [Ca2+]i (Figure 1).
Calcitriol regulates RAAS via genomic mechanisms [89]. An inverse association between serum calcitriol levels and plasma renin activity, in both human and animals, has been described [90]. Studies in VDR knockout mice show that calcitriol negatively regulates the RAAS and blood pressure by a genomic calcium- and PTH-independent mechanism [91,92,93].
The mechanism by which calcitriol regulates blood pressure seems not to be the same with low calcium intake as it is with vitamin D deficiency. Whereas restrictive calcium diets may dominate the nongenomic short-term effects by increasing [Ca2+]i, vitamin D deficiency may preponderate the VDR mediated actions on the RAAS.
In summary, the mechanism by which calcitriol regulates blood pressure in low calcium diets may be mediated by the nongenomic short-term effects increasing [Ca2+]i and consequently rising blood pressure.
2.3. Calcium Intake and Renin–Angiotensin–Aldosterone System
The renin–angiotensin–aldosterone system (RAAS) plays a key role in the physiologic regulation of blood pressure. As shown below, several interactions between calcium intake, calcium homeostatic hormones and the RAAS have been described.
2.3.1. Renin
Renin enzymatic activity consists in the hydrolysis of angiotensinogen to angiotensin I. The acute incubation or infusion of high concentrations of calcium has an inhibitory effect on renin secretion, both in isolated cells and animals [94,95,96,97]. Dietary calcium supplementation has shown to decrease but not to abolish the renin release [98]. It has been reported that acute activation of the calcium sensing receptor in juxtaglomerular cells by high extracellular calcium concentration decreases renin release and plasma renin activity, both in vivo and in vitro. Renin secretion is dependent on cAMP formation. Increased extracellular calcium concentration decreases renin release by diminishing AC and enhancing phosphodiesterase activities [95,99]. cAMP concentration could also be raised by PTH as PTHr-1 along the nephron, including the juxtaglomerular apparatus [100]. The stimulation of PTHr-1 increases cAMP and enhances renin release [101] (Figure 1).
2.3.2. Angiotensin II
Angiotensin II is the primary active product of the RAAS and a potent vasoconstrictor whose actions are mediated by the type I angiotensin II receptor (AT-1R). Low calcium diets have been shown to increase angiotensin II [6,102]. In animals fed low calcium diets, the binding of angiotensin II withAT-1R decreases in smooth muscle cells and increases in the adrenal cortex. These findings suggest that with low calcium intake, angiotensin II may raise blood pressure via increasing aldosterone synthesis or secretion [5].
It has also been described that the infusion of angiotensin II produced a significant dose-dependent increase in PTH serum levels [101]. Moreover, AT-1R has been isolated in the parathyroid glands, and although the intracellular pathway is still unknown, AT-1R inhibition lowered PTH levels [103]. These observations may explain the blood pressure elevation by angiotensin II in a low calcium diet (Figure 1).
2.3.3. Aldosterone
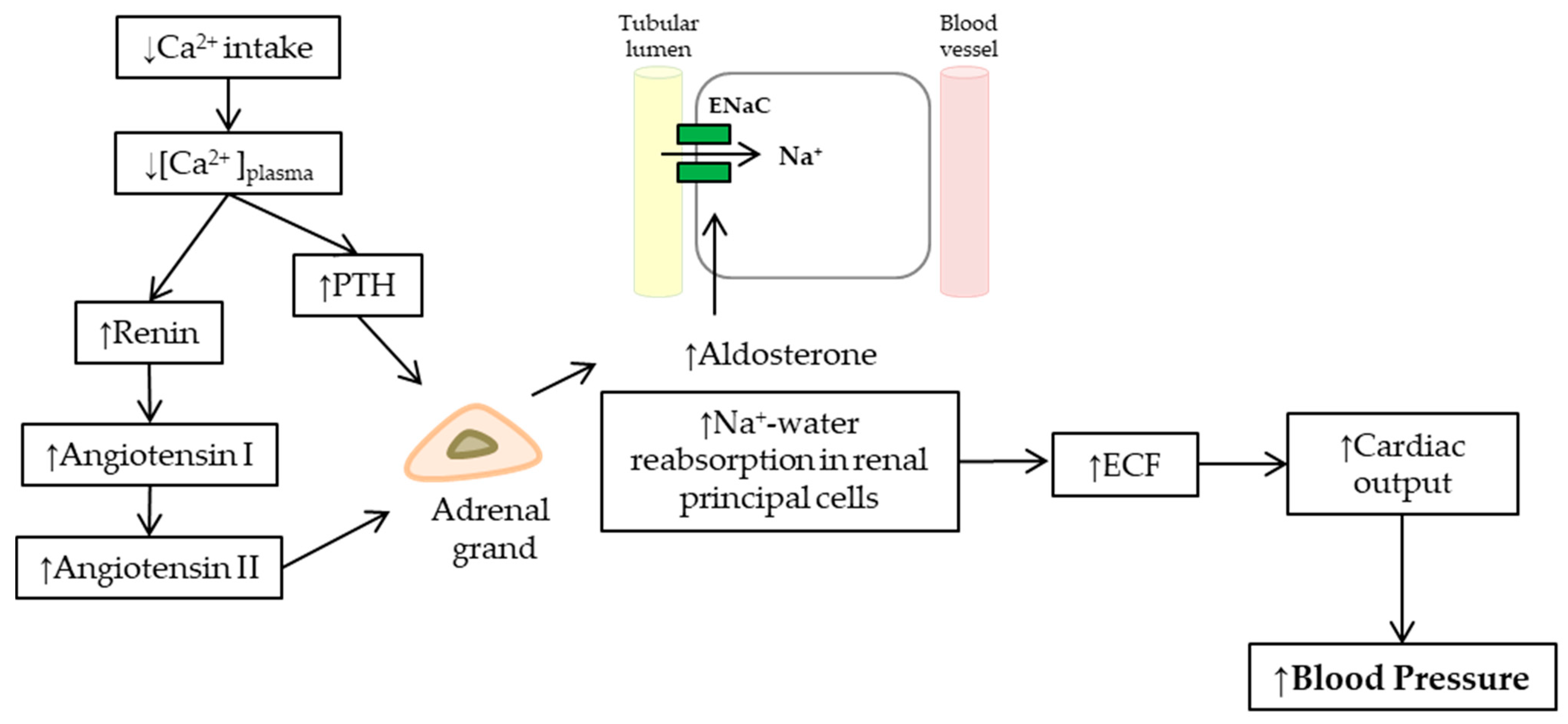
Aldosterone, a steroid hormone, is synthesized by the zona glomerulosa of the adrenal cortex (CZG) in the adrenal gland. Its primary effect is the regulation of blood pressure through the reabsorption of sodium and excretion of potassium in the distal tubules and the collecting ducts of the nephron [104], increasing apical membrane permeability for sodium, thus causing sodium and water reabsorption. This rise of extracellular fluid volume increased cardiac output, and hence blood pressure (Figure 2).
Aldosterone synthesis is stimulated by angiotensin II and high extracellular potassium levels via the calcium messenger system that boosts the steroidogenic cascade within the mitochondria. The acute steroidogenic regulatory protein (StAR) is a key molecule that transports cholesterol through the inner mitochondrial membrane, a fundamental step for the synthesis of steroid hormones, such as aldosterone. StAR is activated by increases in [Ca2+]i. Angiotensin II, via AT-1R activating the PLC/IP3 cascades, and high extracellular potassium levels via depolarizing the plasma membrane of the cell activating calcium voltage-dependent channels, increase [Ca2+]i and thus aldosterone synthesis [105].
A bidirectional stimulating relationship between PTH and aldosterone is reported. Patients with primary aldosteronism have high levels of PTH that return to physiological concentration after the adenoma removal or pharmacological treatment with aldosterone antagonists [106]. Similarly, hypertension associated with secondary aldosteronism due to hyperparathyroidism resolves after parathyroidectomy [107,108]. Studies in humans have also shown a rise in blood pressure and aldosterone after two weeks of an infusion of PTH [57], and this effect is antagonized by PTH-receptor blocking agents [109]. PTHr-1 has been found in the CZG of animals and humans [110], and mineralocorticoid receptors, for aldosterone, have been identified in the parathyroid gland [111].
It has been shown that PTHr-1 stimulates basal steroid secretion (aldosterone, cortisol) from adrenal cells through both AC/PKA- and PLC/PKC-dependent signaling mechanisms [109]. Adrenal cells incubated with PTH increase cAMP and IP3 production, with this effect being partially suppressed by inhibitors of both cascade. The activation of PKA, by increasing the concentration of cAMP, activates StAR. PTH can also indirectly favor steroidogenesis by increasing [Ca2+]i [109].
In summary, it has been shown that both low calcium intake and PTH stimulate renin release, and consequently, angiotensin II and aldosterone synthesis.
3. Conclusions
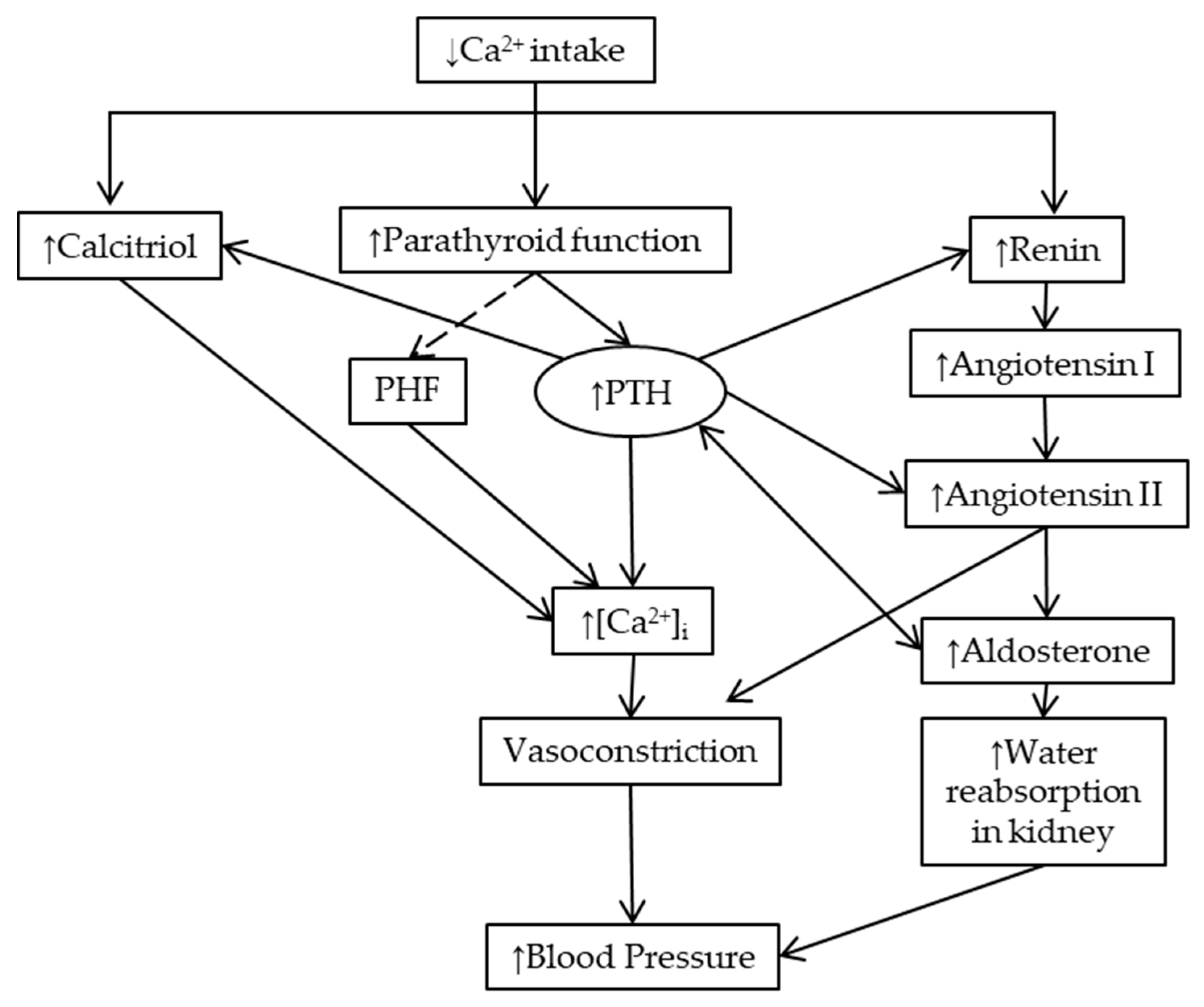
In this manuscript, we reviewed the literature exploring the mechanisms involved in the relationship between calcium intake and blood pressure. It has been shown that, particularly in individuals with low calcium intake, an increase in calcium intake reduces blood pressure. We consider that in view of hypertension being a major factor involved in the global burden of disease, the study of interventions that could prevent the development of hypertension should be prioritized [112]. The link between calcium intake and blood pressure involves a connection between calciotropic hormones and blood pressure regulators. As was hypothesized many years ago, parathyroid activity increases the cytosolic concentration of calcium and increases vascular reactivity and blood pressure [113]. The effect of calcium intake on blood pressure is not shown in parathyroidectomized animal studies. Low calcium intake also increases the synthesis of calcitriol in a direct manner or is mediated by PTH. Calcitriol increases intracellular calcium in vascular smooth muscle cells. Low calcium intake stimulates renin release, and consequently, angiotensin II synthesis. PTH stimulates renin release, angiotensin II and aldosterone synthesis (Figure 3). We are willing with this review to promote discussions and contributions to achieve a better understanding of these mechanisms, and if required, the design of future studies.
Author Contributions
Conceptualization, project administration and funding acquisition J.M.B. and G.C.; investigation and writing—original draft preparation C.V.-E.; writing—review & editing, M.L., N.M., J.M.B. and G.C.
Funding
This research was funded by Bill & Melinda Gates Foundation grant number OPP1190821.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| [Ca2+]i | cytosolic free calcium/intracellular calcium concentration |
| ACAT-1R | adenylate cyclasetype I angiotensin II receptor |
| cAMP | 3′,5′-cyclic adenosine monophosphate |
| CZG | zona glomerulosa of the adrenal cortex of the adrenal gland |
| DBP | diastolic blood pressure |
| IP3 | inositol trisphosphate |
| PHF | parathyroid hypertensive factor |
| PKA | protein kinase A |
| PKC | protein kinase C |
| PLC | phospholipase C |
| PRA | plasma renin activity |
| PTH | parathyroid hormone |
| PTHr-1 | PTH receptor |
| RAAS | the renin–angiotensin-aldosterone system |
| StAR | acute steroidogenic regulatory protein |
| SBP | systolic blood pressure |
| VDR | Vitamin D intracellular receptor |
References
- Belizan, J.M.; Villar, J. The relationship between calcium intake and edema-, proteinuria-, and hypertension-gestosis: An hypothesis. Am. J. Clin. Nutr. 1980, 33, 2202–2210. [Google Scholar] [CrossRef]
- Belizán, J.M.; Villar, J.; Self, S.; Pineda, O.; González, I.; Sainz, E. The mediating role of the parathyroid gland in the effect of low calcium intake on blood pressure in the rat. Arch. Latinoam. Nutr. 1984, 34, 666–675. [Google Scholar] [PubMed]
- Belizan, J.M.; Villar, J.; Pineda, O.; Gonzalez, A.E.; Sainz, E.; Garrera, G.; Sibrian, R. Reduction of blood pressure with calcium supplementation in young adults. J. Am. Med. Assoc. 1983, 249, 1161–1165. [Google Scholar] [CrossRef]
- Belizan, J.M.; Pineda, O.; Sainz, E.; Menendez, L.A.; Villar, J. Rise of blood pressure in calcium-deprived pregnant rats. Am. J. Obstet. Gynecol. 1981, 141, 163–169. [Google Scholar] [CrossRef]
- Baksi, S.N.; Abhold, R.H.; Speth, R.C. Low-calcium diet increases blood pressure and alters peripheral but not central angiotensin II binding sites in rats. J. Hypertens. 1989, 7, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Yuasa, S.; Shoji, T.; Miki, S.; Fujioka, H.; Uchida, K.; Sumikura, T.; Takamitsu, Y.; Yura, T.; Matsuo, H. Effect of Low Dietary Calcium Intake on Blood Pressure and Pressure Natriuresis Response in Rats: A Possible Role of the Renin-Angiotensin System. Blood Press. 1996, 5, 121–127. [Google Scholar]
- McCarron, D. Blood pressure and calcium balance in the Wistar-Kyoto rat. Life Sci. 1982, 30, 683–689. [Google Scholar] [CrossRef]
- Furspan, P.B.; Rinaldi, G.J.; Hoffman, K.; Bohr, D.F. Dietary calcium and cell membrane abnormality in genetic hypertension. Hypertension 1989, 13, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Hatton, D.C.; Scrogin, K.E.; Levine, D.; Feller, D.; Mccarron, D.A. Dietary calcium modulates blood pressure through alpha 1-adrenergic receptors. Am. J. Physiol. 1993, 264, 234–238. [Google Scholar] [CrossRef]
- Arvola, P.; Ruskoaho, H.; Pörsti, I. Effects of high calcium diet on arterial smooth muscle function and electrolyte balance in mineralocorticoid-salt hypertensive rats. Br. J. Pharmacol. 1993, 108, 948–958. [Google Scholar] [CrossRef] [Green Version]
- Cormick, G.; Ciapponi, A.; Cafferata, M.L.; Belizán, J.M. Calcium supplementation for prevention of primary hypertension. Cochrane Database Syst. Rev. 2015, 30, CD010037. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Nicolson, D.J.; Cook, J.V.; Campbell, F.; Beyer, F.R.; Ford, G.A.; Mason, J. Calcium supplementation for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2006, 19, CD004639. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; He, J.; Appel, L.J.; Cutler, J.A.; Havas, S.; Kotchen, T.A.; Roccella, E.J.; Stout, R.; Vallbona, C.; Winston, M.C.; et al. Primary prevention of hypertension: Clinical and public health advisory from The National High Blood Pressure Education Program. JAMA J. Am. Med. Assoc. 2002, 288, 1882–1888. [Google Scholar] [CrossRef]
- Belizán, J.M.; Villar, J.; Gonzalez, L.; Campodonico, L.; Bergel, E. Calcium supplementation to prevent hypertensive disorders of pregnancy. N. Engl. J. Med. 1991, 325, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyr, G.J.; Lawrie, T.A.; Atallah, A.N.; Duley, L.; Torloni, M.R. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2014, 24, CD001059. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Betrán, A.P.; Singata-Madliki, M.; Cormick, G.; Munjanja, S.P.; Fawcus, S.; Mose, S.; Hall, D.; Ciganda, A.; Seuc, A.H.; et al. Prepregnancy and early pregnancy calcium supplementation among women at high risk of pre-eclampsia: A multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2019, 393, 330–339. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Guideline: Calcium Supplementation in Pregnant Women; WHO: Geneva, Switzerland, 2013; pp. 1–35. [Google Scholar]
- Belizan, J.M.; Villar, J.; Bergel, E.; del Pino, A.; Di Fulvio, S.; Galliano, S.V.; Kattan, C. Long-term effect of calcium supplementation during pregnancy on the blood pressure of offspring: Follow up of a randomised controlled trial. BMJ 1997, 315, 281–285. [Google Scholar] [CrossRef]
- Bergel, E.; Gibbons, L.; Rasines, M.G.; Luetich, A.; Belizán, J.M. Maternal calcium supplementation during pregnancy and dental caries of children at 12 years of age: Follow-up of a randomized controlled trial. Acta Obstet. Gynecol. Scand. 2010, 89, 1396–1402. [Google Scholar] [CrossRef]
- Hofmeyr, G. Protocol 11PRT/4028: Long term calcium supplementation in women at high risk of pre-eclampsia: A randomised, placebo-controlled trial. Lancet 2011. Available online: https://www.thelancet.com/protocol-reviews/11PRT-4028 (accessed on 17 May 2019).
- McCarron, D.A.; Morris, C.D.; Henry, H.J.; Stanton, J.L. Blood pressure and nutrient intake in the United States. Nutr. Today 1984, 19, 14–23. [Google Scholar] [CrossRef]
- Skowrońska-Jóźwiak, E.; Jaworski, M.; Lorenc, R.; Karbownik-Lewińska, M.; Lewiński, A. Low dairy calcium intake is associated with overweight and elevated blood pressure in Polish adults, notably in premenopausal women. Public Health Nutr. 2016, 20, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Schmelz, E.; Marrugat, J. Relationship between diet and blood pressure in a representative Mediterranean population. Eur. J. Nutr. 2002, 41, 161–167. [Google Scholar] [CrossRef]
- Grubenmann, W.; Binswanger, U.; Hunziker, W.; Fischer, J.A. Effects of calcium intake and renal function on plasma immunoreactive parathyroid hormone levels in rats. Horm. Metab. Res. 1978, 10, 438–443. [Google Scholar] [CrossRef]
- Chan, R.; Woo, J.; Chan, D.; Mellström, D.; Leung, P.; Ohlsson, C.; Kwok, T. Serum 25-hydroxyvitamin D and parathyroid hormone levels in relation to blood pressure in a cross-sectional study in older Chinese men. J. Hum. Hypertens. 2011, 26, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Schoenmakers, I.; Jarjou, L.M.A.; Goldberg, G.R.; Tsoi, K.; Harnpanich, D.; Prentice, A. Acute response to oral calcium loading in pregnant and lactating women with a low calcium intake: A pilot study. Osteoporos. Int. 2013, 24, 2301–2308. [Google Scholar] [CrossRef]
- Sadideen, H.; Swaminathan, R. Effect of acute oral calcium load on serum PTH and bone resorption in young healthy subjects: An overnight study. Eur. J. Clin. Nutr. 2004, 58, 1661–1665. [Google Scholar] [CrossRef]
- Young, E.W.; McCarron, D.A.; Morris, C.D. Calcium regulating hormones in essential hypertension. Importance of gender. Am. J. Hypertens. 1990, 3, 161S–166S. [Google Scholar] [CrossRef]
- Brickman, A.S.; Nyby, M.D.; Von Hungen, K.; Eggena, P.; Tuck, M.L. Calcitropic hormones, platelet calcium, and blood pressure in essential hypertension. Hypertension 1990, 16, 515–522. [Google Scholar] [CrossRef]
- Morfis, L.; Smerdely, P.; Howes, L.G. Relationship between serum parathyroid hormone levels in the elderly and 24 h ambulatory blood pressures. J. Hypertens. 1997, 15, 1271–1276. [Google Scholar] [CrossRef]
- Snijder, M.B.; Lips, P.; Seidell, J.C.; Visser, M.; Deeg, D.J.H.; Dekker, J.M.; Van Dam, R.M. Vitamin D status and parathyroid hormone levels in relation to blood pressure: A population-based study in older men and women. J. Intern. Med. 2007, 261, 558–565. [Google Scholar] [CrossRef]
- Park, J.S.; Choi, S.B.; Rhee, Y.; Chung, J.W.; Choi, E.Y.; Kim, D.W. Parathyroid Hormone, Calcium, and Sodium Bridging Between Osteoporosis and Hypertension in Postmenopausal Korean Women. Calcif. Tissue Int. 2015, 96, 417–429. [Google Scholar] [CrossRef]
- Yao, L.; Folsom, A.R.; Pankow, J.S.; Selvin, E.; Michos, E.D.; Alonso, A.; Tang, W.; Lutsey, P.L. Parathyroid hormone and the risk of incident hypertension: The Atherosclerosis Risk in Communities study. J. Hypertens. 2016, 34, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Takagi, Y.; Fukase, M.; Takata, S.; Fujimi, T.; Fujita, T. Calcium Treatment of Essential Hypertension in Elderly Patients Evaluated by 24 H Monitoring. Am. J. Hypertens. 1991, 4, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Kamycheva, E.; Sundsfjord, J.; Jorde, R. Serum parathyroid hormone levels predict coronary heart disease: The Tromsø Study. Eur. J. Prev. Cardiol. 2004, 11, 69–74. [Google Scholar] [CrossRef]
- Jorde, R.; Sundsfjord, J.; Haug, E.; Bønaa, K.H. Relation between low calcium intake, parathyroid. hormone, and blood pressure. Blood Press. 2000, 35, 1154–1159. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Parimi, N.; Barrett-Connor, E.; Laughlin, G.A.; Ensrud, K.E.; Hoffman, A.R.; Shikany, J.M.; Cauley, J.A.; Lane, N.E.; Bauer, D.C.; et al. Serum 25-hydroxyvitamin D, parathyroid hormone, and mortality in older men. J. Clin. Endocrinol. Metab. 2010, 95, 4625–4634. [Google Scholar] [CrossRef]
- Grandi, N.C.; Breitling, L.P.; Hahmann, H.; Wüsten, B.; März, W.; Rothenbacher, D.; Brenner, H. Serum parathyroid hormone and risk of adverse outcomes in patients with stable coronary heart disease. Heart 2011, 97, 1215–1221. [Google Scholar] [CrossRef]
- Van Ballegooijen, A.J.; Kestenbaum, B.; Sachs, M.C.; de Boer, I.H.; Siscovick, D.S.; Hoofnagle, A.N.; Ix, J.H.; Visser, M.; Brouwer, I.A. Association of 25-Hydroxyvitamin D and Parathyroid Hormone with Incident Hypertension. J. Am. Coll. Cardiol. 2014, 63, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Morimoto, S.; Yang, J.; Niinoabu, T.; Fukuo, K.; Ogihara, T. Expression of parathyroid hormone/parathyroid hormone-related protein receptor in vascular endothelial cells. J. Cardiovasc. Pharmacol. 1998, 31, S142–S144. [Google Scholar] [CrossRef]
- Vilardaga, J.P.; Romero, G.; Friedman, P.A.; Gardella, T.J. Molecular basis of parathyroid hormone receptor signaling and trafficking: A family B GPCR paradigm. Cell. Mol. Life Sci. 2011, 68, 1–13. [Google Scholar] [CrossRef]
- Gardella, T.J.; Vilardaga, J.P. International Union of Basic and Clinical Pharmacology. XCIII. The Parathyroid Hormone Receptors—Family B G Protein-Coupled Receptors. Pharmacol. Rev. 2015, 67, 310–337. [Google Scholar] [CrossRef]
- Hilpert, K.F.; West, S.G.; Bagshaw, D.M.; Fishell, V.; Barnhart, L.; Lefevre, M.; Most, M.M.; Zemel, M.B.; Chow, M.; Hinderliter, A.L.; et al. Effects of Dairy Products on Intracellular Calcium and Blood Pressure in Adults with Essential Hypertension. J. Am. Coll. Nutr. 2009, 28, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; de la Sierra, A.; Coca, A.; Poch, E.; Giner, V.; Urbano-Márquez, A. Oral Calcium Supplementation Reduces Intraplatelet Free Calcium Concentration and Insulin Resistance in Essential Hypertensive Patients. Hypertension 1997, 29, 531–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogin, E.; Massry, S.G.; Harary, I. Effect of parathyroid hormone on rat heart cells. J. Clin. Investig. 1981, 67, 1215–1227. [Google Scholar] [CrossRef] [PubMed]
- Picotto, G. Rapid effects of calciotropic hormones on female rat enterocytes: Combined actions of 1,25(OH)2-vitamin D3, PTH and 17β-estradiol on intracellular CA2+ regulation. Horm. Metab. Res. 2001, 33, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Smogorzewski, M.; Koss, M.; Massry, S.G. Pathways involved in PTH-induced rise in cytosolic Ca2+ concentration of rat renal proximal tubule. Am. J. Physiol. Physiol. 1995, 268, F330–F337. [Google Scholar] [CrossRef] [PubMed]
- Chausmer, A.B.; Sherman, B.S.; Wallach, S. The eflfect of parathyroid hormone on hepatic cell transport of calcium. Endocrinology 1972, 90, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.A.; Chui, L.A.; Massry, S.G. Effect of parathyroid hormone and uremia on peripheral nerve calcium and motor nerve conduction velocity. J. Clin. Investig. 1978, 62, 88–93. [Google Scholar] [CrossRef]
- Yamaguchi, D.T.; Hahn, T.J.; Iida-Klein, A.; Kleeman, C.R.; Muallem, S. Parathyroid hormone-activated calcium channels in an osteoblast-like clonal osteosarcoma cell line. cAMP-dependent and cAMP-independent calcium channels. J. Biol. Chem. 1987, 262, 7711–7718. [Google Scholar] [PubMed]
- Reid, I.R.; Civitelli, R.; Halstead, L.R.; Avioli, L.V.; Hruska, K.A. Parathyroid hormone acutely elevates intracellular calcium in osteoblastlike cells. Am. J. Physiol. Metab. 1987, 253, E45–E51. [Google Scholar] [CrossRef]
- Fardella, C.; Rodriguez-Portales, J.A. Intracellular calcium and blood pressure: Comparison between primary hyperparathyroidism and essential hypertension. J. Endocrinol. Investig. 1995, 18, 827–832. [Google Scholar] [CrossRef]
- Song, G.J.; Fiaschi-Taesch, N.; Bisello, A. Endogenous Parathyroid Hormone-Related Protein Regulates the Expression of PTH Type 1 Receptor and Proliferation of Vascular Smooth Muscle Cells. Mol. Endocrinol. 2009, 23, 1681–1690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, A.S.; Linas, S.L. Parathyroid hormone/adenylate cyclase coupling in vascular smooth muscle cells. Hypertension 1994, 23, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, C.; Schoefer, P.; Stoclet, J.C.; Gairard, A. Effect of parathyroid hormone and antagonist on aortic cAMP levels. Can. J. Physiol. Pharmacol. 1987, 65, 2349–2353. [Google Scholar] [CrossRef]
- Nickols, G.A.; Metz, M.A.; Cline, W.H. Endothelium-independent linkage of parathyroid hormone receptors of rat vascular tissue with increased adenosine 3′,5′-monophosphate and relaxation of vascular smooth muscle. Endocrinology 1986, 119, 349–356. [Google Scholar] [CrossRef]
- Hulter, H.N.; Melby, J.C.; Peterson, J.C.; Cooke, C.R. Chronic continuous PTH infusion results in hypertension in normal subjects. J. Clin. Hypertens. 1986, 2, 360–370. [Google Scholar]
- Oshima, T.; Schleiffer, R.; Young, E.W.; McCarron, D.A.; Bukoski, R.D. Parathyroidectomy lowers blood pressure independently of changes in platelet free calcium. J. Hypertens. 1991, 9, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, H. Parathyroid hormone causes a transient rise in intracellular ionized calcium in vascular smooth muscle cells. Biochem. Biophys. Res. Commun. 1990, 166, 709–714. [Google Scholar] [CrossRef]
- Lewanczuk, R.Z.; Wang, J.; Zhang, Z.R.; Pang, P.K.T. Effects of Spontaneously Hypertensive Rat Plasma on Blood Pressure and Tail Artery Calcium Uptake in Normotensive Rats. Am. J. Hypertens. 1989, 2, 26–31. [Google Scholar]
- Lewanczuk, R.Z.; Resnick, L.M.; Blumenfeld, J.D.; Laragh, J.H.; Pang, P.K. A new circulating hypertensive factor in the plasma of essential hypertensive subjects. J. Hypertens. 1990, 8, 105–108. [Google Scholar] [CrossRef]
- Pernot, F.; Burkhard, C.; Gairard, A. Parathyroid cross-transplantation and development of high blood pressure in rats. J. Cardiovasc. Pharmacol. 1994, 23, S18–S22. [Google Scholar] [CrossRef]
- Neuser, D.; Schulte-Brinkmann, R.; Kazda, S. Development of hypertension in WKY rats after transplantation of parathyroid glands from SHR/SP. J. Cardiovasc. Pharmacol. 1990, 16, 971–974. [Google Scholar] [CrossRef] [PubMed]
- Pang, P.K.Y.; Benishin, C.G.; Lewanczuk, R.Z. Combined effect of dietary calcium and calcium antagonists on blood pressure reduction in spontaneously hypertensive rats. J. Cardiovasc. Pharmacol. 1992, 19, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Lewanczuk, R.Z. In vivo potentiation of vasopressors by spontaneously hypertensive rat plasma correlation with blood pressure and calcium uptake. Clin. Exp. Hypertens. A 1989, 11, 1471–1485. [Google Scholar] [CrossRef] [PubMed]
- Lewanczuk, R.Z.; Pang, P.K.T. Vascular and calcemic effects of plasma of spontaneously hypertensive rats. Am. J. Hypertens. 1990, 3, 189S–194S. [Google Scholar] [CrossRef]
- Shan, J.; Benishin, C.G.; Lewanczuk, R.Z.; Pang, P.K. Mechanism of the vascular action of parathyroid hypertensive factor. J. Cardiovasc. Pharmacol. 1994, 23, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Pang, P.K.T.; Benishin, C.G.; Lewanczuk, R.Z. Parathyroid hypertensive factor, a circulating factor in animal and human hypertension. Am. J. Hypertens. 1991, 4, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Benishin, C.G.; Lewanczuk, R.Z.; Shan, J.; Pang, P.K. Purification and structural characterization of parathyroid hypertensive factor.pdf. J. Cardiovasc. Pharmacol. 1994, 23, S9–S13. [Google Scholar] [CrossRef]
- Schlüter, H.; Quante, C.; Buchholz, B.; Dietl, K.H.; Spieker, C.; Karas, M.; Zidek, W. A vasopressor factor partially purified from human parathyroid glands. Biochem. Biophys. Res. Commun. 1992, 188, 323–329. [Google Scholar] [CrossRef]
- Mangos, G.J.; Brown, M.A.; Whitworth, J.A. Difficulties in detecting parathyroid hypertensive factor in the rat. Clin. Exp. Pharmacol. Physiol. 1998, 25, 936–938. [Google Scholar] [CrossRef]
- Beveridge, L.A.; Struthers, A.D.; Khan, F.; Jorde, R.; Scragg, R.; Macdonald, H.M.; Alvarez, J.A.; Boxer, R.S.; Dalbeni, A.; Gepner, A.D.; et al. Effect of vitamin D supplementation on blood pressure a systematic review and meta-analysis incorporating individual patient data. JAMA Intern. Med. 2015, 175, 745–754. [Google Scholar] [CrossRef]
- Lennon, S.L.; DellaValle, D.M.; Rodder, S.G.; Prest, M.; Sinley, R.C.; Hoy, M.K.; Papoutsakis, C. 2015 Evidence Analysis Library Evidence-Based Nutrition Practice Guideline for the Management of Hypertension in Adults. J. Acad. Nutr. Diet. 2017, 117, 1445–1458. [Google Scholar] [CrossRef]
- Mozaffari-Khosravi, H.; Loloei, S.; Mirjalili, M.R.; Barzegar, K. The effect of vitamin D supplementation on blood pressure in patients with elevated blood pressure and vitamin D deficiency: A randomized, double-blind, placebo-controlled trial. Blood Press. Monit. 2015, 20, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Huang, K. Effect of vitamin D supplementation on blood pressure parameters in patients with vitamin D deficiency: A systematic review and meta-analysis. J. Am. Soc. Hypertens. 2018, 12, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.P.; Scott, J.B.; Ng, K.; Drake, B.F.; Suarez, E.G.; Hayden, D.L.; Bennett, G.G.; Chandler, P.D.; Hollis, B.W.; Emmons, K.M.; et al. Effect of vitamin D supplementation on blood pressure in blacks. Hypertension 2013, 61, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Areco, V.; Rivoira, M.A.; Rodriguez, V.; Marchionatti, A.M.; Carpentieri, A.; De Talamoni, N.T. Dietary and pharmacological compounds altering intestinal calcium absorption in humans and animals. Nutr. Res. Rev. 2015, 28, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Centeno, V.; Díaz De Barboza, G.; Marchionatti, A.; Rodríguez, V.; Tolosa De Talamoni, N. Molecular mechanisms triggered by low-calcium diets. Nutr. Res. Rev. 2009, 22, 163–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favus, M.J.; Walling, M.W.; Kimberg, D.V. Effects of dietary calcium restriction and chronic thyroparathyroidectomy on the metabolism of [3H]25 hydroxyvitamin D3 and the active transport of calcium by rat intestine. J. Clin. Investig. 1974, 53, 1139–1148. [Google Scholar] [CrossRef]
- Colston, K.W.; Evans, I.M.A.; Galante, L.; MacIntyre, I.; Moss, D.W. Regulation of vitamin D metabolism: Factors influencing the rate of formation of 1,25-dihydroxycholecalciferol by kidney homogenates (Short Communication). Biochem. J. 2015, 134, 817–820. [Google Scholar] [CrossRef]
- Zehnder, D.; Bland, R.; Chana, R.S.; Wheeler, D.C.; Howie, A.J.; Williams, M.C.; Stewart, P.M.; Hewison, M. Synthesis of 1,25-dihydroxyvitamin D(3) by human endothelial cells is regulated by inflammatory cytokines: A novel autocrine determinant of vascular cell adhesion. J. Am. Soc. Nephrol. 2002, 13, 621–629. [Google Scholar]
- Norman, A.W.; Okamura, W.H.; Bishop, J.E.; Henry, H.L. Update on biological actions of 1α,25(OH)2-vitamin D3 (rapid effects) and 24R,25(OH)2-vitamin D3. Mol. Cell. Endocrinol. 2002, 197, 1–13. [Google Scholar] [CrossRef]
- Bukoski, R.D.; Xue, H.; McCarron, D.A. Effect of 1,25(OH)2 vitamin D3 and ionized Ca2+ on 45Ca uptake by primary cultures of aortic myocytes of spontaneously hypertensive and Wistar Kyoto normotensive rats. Biochem. Biophys. Res. Commun. 1987, 146, 1330–1335. [Google Scholar] [CrossRef]
- Inoue, T.; Kawashima, H. 1,25-Dihydroxyvitamin D3 stimulates 45Ca2+-uptake by cultured vascular smooth muscle cells derived from rat aorta. Biochem. Biophys. Res. Commun. 1988, 152, 1388–1394. [Google Scholar] [CrossRef]
- Xue, H.; Mccarron, D.A.; Bukoski, R.D. 1,25 (OH)2 vitamin D3-induced 45CA uptake in vascular myocytes cultured from spontaneously hypertensive and normotensive rats. Life Sci. 1991, 49, 651–659. [Google Scholar] [CrossRef]
- Bukoski, R.D.; Wang, D.; Wagman, D.W. Injection of 1,25-(OH)2 vitamin D3 enhances resistance artery contractile properties. Hypertension 1990, 16, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Shan, J.; Resnick, L.M.; Lewanczuk, R.Z.; Karpinski, E.; Li, B.; Pang, P.Κ.T. 1,25-dihydroxyvitamin D as a cardiovascular hormone. Effects on calcium current and cytosolic free calcium in vascular smooth muscle cells. Am. J. Hypertens 1993, 6, 983–988. [Google Scholar] [CrossRef]
- Boland, R.; Buitrago, C.; de Boland, A.R. Modulation of tyrosine phosphorylation signalling pathways by 1α,25(OH)2-vitamin D3. Trends Endocrinol. Metab. 2005, 16, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C. Vitamin D regulation of the renin-angiotensin system. J. Cell. Biochem. 2003, 88, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Resnick, L.M.; Müller, F.B.; Laragh, J.H. Calcium-regulating hormones in essential hypertension: Relation to plasma renin activity and sodium metabolism. Ann. Intern. Med. 1986, 105, 649–654. [Google Scholar] [CrossRef]
- Li, Y.C.; Kong, J.; Wei, M.; Chen, Z.F.; Liu, S.Q.; Cao, L.P. 1,25-Dihydroxyvitamin D 3 is a negative endocrine regulator of the renin-angiotensin system. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Lu, F.; Cao, K.; Xu, D.; Goltzman, D.; Miao, D. Calcium-independent and 1,25(OH)2D3-dependent regulation of the renin-angiotensin system in 1α-hydroxylase knockout mice. Kidney Int. 2008, 74, 170–179. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; Qiao, G.; Zhang, Z.; Liu, S.Q.; Li, Y.C. Targeted vitamin D receptor expression in juxtaglomerular cells suppresses renin expression independent of parathyroid hormone and calcium. Kidney Int. 2008, 74, 1577–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grünberger, C.; Kurtz, A.; Klar, J.; Obermayer, B.; Schweda, F. The Calcium Paradoxon of Renin Release. Circ. Res. 2006, 99, 1197–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Capisano, M.C.; Ortiz, P.A.; Garvin, J.L.; Harding, P.; Beierwaltes, W.H. Expression and function of the calcium-sensing receptor in juxtaglomerular cells. Hypertension 2007, 50, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Watkins, B.E.; Davis, J.O.; Lohmeier, T.E.; Freeman, R.H. Intrarenal site of action of calcium on renin secretion in dogs. Circ. Res. 1976, 36, 847–853. [Google Scholar] [CrossRef]
- Helwig, J.J.; Musso, M.J.; Judes, C.; Nickols, G.A. Parathyroid hormone and calcium: Interactions in the control of renin secretion in the isolated, nonfiltering rat kidney. Endocrinology 1991, 129, 1233–1242. [Google Scholar] [CrossRef]
- Kotchen, T.A.; Maull, K.I.; Luke, R. Effect of acute and chronic calcium administration on plasma renin. J. Clin. Investig. 1974, 54, 1279–1286. [Google Scholar] [CrossRef]
- Atchison, D.K.; Harding, P.; Beierwaltes, W.H. Hypercalcemia reduces plasma renin via parathyroid hormone, renal interstitial calcium, and the calcium-sensing receptor. Hypertension 2011, 58, 604–610. [Google Scholar] [CrossRef]
- Riccardi, D.; Lee, W.S.; Lee, K.; Segre, G.V.; Brown, E.M.; Hebert, S.C. Localization of the extracellular Ca(2+)-sensing receptor and PTH/PTHrP receptor in rat kidney. Am. J. Physiol. Physiol. 1996, 271, F951–F956. [Google Scholar] [CrossRef]
- Grant, F.D.; Mandel, S.J.; Brown, E.M.; Williams, G.H.; Seely, E.W. Interrelationships between the renin-angiotensin-aldosterone and calcium homeostatic systems. J. Clin. Endocrinol. Metab. 1992, 75, 988–992. [Google Scholar]
- Doris, P.A. Plasma angiotensin II: Interdependence on sodium and calcium homeostasis. Peptides 1988, 9, 243–248. [Google Scholar] [CrossRef]
- Brown, J.M.; Williams, J.S.; Luther, J.M.; Garg, R.; Garza, A.E.; Pojoga, L.H.; Ruan, D.T.; Williams, G.H.; Adler, G.K.; Vaidya, A. Human interventions to characterize novel relationships between the renin-angiotensin-aldosterone system and parathyroid hormone. Hypertension 2014, 63, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Müller, J. Aldosterone: The minority hormone of. Steroids 1995, 60, 2–9. [Google Scholar] [CrossRef]
- Rojas, J.; Olivar, L.C.; Chavez Castillo, M.; Martinez, M.S.; Wilches-Duran, S.; Graterol, M.; Contreras-Velasquez, J.; Cerda, M.; Riaño, M.; Bermudez, V. Hormona paratiroidea, aldosterona e hipertensión arterial ¿una amenaza infravalorada? Rev. Latinoam. Hipertens. 2017, 12, 1–18. [Google Scholar]
- Catena, C.; Colussi, G.L.; Brosolo, G.; Bertin, N.; Novello, M.; Palomba, A.; Sechi, L.A. Salt, Aldosterone, and Parathyroid Hormone: What Is the Relevance for Organ Damage? Int. J. Endocrinol. 2017, 2017, 4397028. [Google Scholar] [CrossRef] [PubMed]
- Sabbadin, C.; Cavedon, E.; Zanon, P.; Iacobone, M.; Armanini, D. Resolution of hypertension and secondary aldosteronismafter surgical treatment of primary hyperparathyroidism. J. Endocrinol. Investig. 2013, 36, 665–666. [Google Scholar]
- Barkan, A.; Marilus, R.; Winkelsberg, G.; Yeshurun, D.; Blum, I. Primary hyperparathyroidism: Possible cause of primary hyperaldosteronism in a 60-year-old woman. J. Clin. Endocrinol. Metab. 1980, 51, 144–147. [Google Scholar] [CrossRef]
- Mazzocchi, G.; Aragona, F.; Malendowicz, L.K.; Nussdorfer, G.G. PTH and PTH-related peptide enhance steroid secretion from human adrenocortical cells. Am. J. Physiol. Metab. 2001, 280, E209–E213. [Google Scholar] [CrossRef] [PubMed]
- Isales, C.M.; Barrett, P.Q.; Brines, M.; Bollag, W. Parathyroid Hormone Modulates Angiotensin II-Induced. Endocrinology 1991, 129, 489–495. [Google Scholar] [CrossRef]
- Maniero, C.; Fassina, A.; Guzzardo, V.; Lenzini, L.; Amadori, G.; Pelizzo, M.R.; Gomez-Sanchez, C.; Rossi, G.P. Primary hyperparathyroidism with concurrent primary aldosteronism. Hypertension 2011, 58, 341–346. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Belizán, J.M.; Villar, J.; Repke, J. The relationship between calcium intake and pregnancy-induced hypertension: Up-to-date evidence. Am. J. Obstet. Gynecol. 1988, 158, 898–902. [Google Scholar] [CrossRef]
Figure 1.
Scheme of the mechanisms involved in the rise of blood pressure in low calcium intake by an increase in peripheral vascular resistance. Low calcium intake decreases plasmatic calcium concentration ([Ca2+]plasma), stimulating the release of parathyroid hormone (PTH) and parathyroid hypertensive factor (PHF), the synthesis of calcitriol, and the activation of the renin–angiotensin–aldosterone system (RAAS). In vascular smooth muscle cells (VSMC), angiotensin II via the angiotensin II type I receptor (AT1R)/Gq/phospholipase C (PLC)/inositol trisphosphate (IP3) pathway, PTH via PTHr-1/Gs/3′,5′-cyclic adenosine monophosphate (cAMP)/protein kinase A (PKA), and calcitriol via adenylate cyclase (AC)/cAMP/PKA and PLC/IP3 signaling pathways increased the intracellular calcium concentration ([Ca2+]i). The rise of [Ca2+]i leads to vasoconstriction, and hence increases in peripheral vascular resistance and blood pressure. The PHF mechanism of action remains unknown. See text for further details.
Figure 1.
Scheme of the mechanisms involved in the rise of blood pressure in low calcium intake by an increase in peripheral vascular resistance. Low calcium intake decreases plasmatic calcium concentration ([Ca2+]plasma), stimulating the release of parathyroid hormone (PTH) and parathyroid hypertensive factor (PHF), the synthesis of calcitriol, and the activation of the renin–angiotensin–aldosterone system (RAAS). In vascular smooth muscle cells (VSMC), angiotensin II via the angiotensin II type I receptor (AT1R)/Gq/phospholipase C (PLC)/inositol trisphosphate (IP3) pathway, PTH via PTHr-1/Gs/3′,5′-cyclic adenosine monophosphate (cAMP)/protein kinase A (PKA), and calcitriol via adenylate cyclase (AC)/cAMP/PKA and PLC/IP3 signaling pathways increased the intracellular calcium concentration ([Ca2+]i). The rise of [Ca2+]i leads to vasoconstriction, and hence increases in peripheral vascular resistance and blood pressure. The PHF mechanism of action remains unknown. See text for further details.

Figure 2.
Scheme of the mechanisms involved in the rise of blood pressure in low calcium intake via an increase in cardiac output. Low calcium intake decreased the plasmatic calcium concentration ([Ca2+]plasma), stimulating PTH and the renin–angiotensin–aldosterone system (RAAS). Both angiotensin II and PTH were increased aldosterone secretion due to the adrenal gland. Aldosterone upregulates epithelial sodium channels (ENaC) in the principal cells of the collecting duct in the kidney, increasing apical membrane permeability for Na+, thus Na+ and water reabsorption. The rise of extracellular fluid volume (ECF) increased cardiac output and hence blood pressure.
Figure 2.
Scheme of the mechanisms involved in the rise of blood pressure in low calcium intake via an increase in cardiac output. Low calcium intake decreased the plasmatic calcium concentration ([Ca2+]plasma), stimulating PTH and the renin–angiotensin–aldosterone system (RAAS). Both angiotensin II and PTH were increased aldosterone secretion due to the adrenal gland. Aldosterone upregulates epithelial sodium channels (ENaC) in the principal cells of the collecting duct in the kidney, increasing apical membrane permeability for Na+, thus Na+ and water reabsorption. The rise of extracellular fluid volume (ECF) increased cardiac output and hence blood pressure.

Figure 3.
Scheme of the mechanisms involved in the rise of blood pressure due to low calcium intake, namely the link between calciotropic hormones and blood pressure regulators. Low calcium intake: (a) increases calcitriol serum levels, (b) stimulates parathyroid function, and (c) increases renin secretion. Calcitriol may increase cytosolic free calcium concentration ([Ca2+]i) via non-genomic short-term mechanisms. The parathyroid gland secretes parathyroid hormone (PTH) and possibly (dash arrow) the parathyroid hypertensive factor (PHF). Both mediators increase [Ca2+]i, leading to the contraction of the vascular smooth muscle cells (vasoconstriction). Renin release is stimulated both by low extracellular calcium and PTH, activating the renin–angiotensin–aldosterone system (RAAS). In addition, PTH increases angiotensin II and aldosterone synthesis, which also leads to vasoconstriction and increases renal water reabsorption, increasing blood pressure. Aldosterone also increases PTH serum levels (double-headed arrow). See text for further details.
Figure 3.
Scheme of the mechanisms involved in the rise of blood pressure due to low calcium intake, namely the link between calciotropic hormones and blood pressure regulators. Low calcium intake: (a) increases calcitriol serum levels, (b) stimulates parathyroid function, and (c) increases renin secretion. Calcitriol may increase cytosolic free calcium concentration ([Ca2+]i) via non-genomic short-term mechanisms. The parathyroid gland secretes parathyroid hormone (PTH) and possibly (dash arrow) the parathyroid hypertensive factor (PHF). Both mediators increase [Ca2+]i, leading to the contraction of the vascular smooth muscle cells (vasoconstriction). Renin release is stimulated both by low extracellular calcium and PTH, activating the renin–angiotensin–aldosterone system (RAAS). In addition, PTH increases angiotensin II and aldosterone synthesis, which also leads to vasoconstriction and increases renal water reabsorption, increasing blood pressure. Aldosterone also increases PTH serum levels (double-headed arrow). See text for further details.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Parathyroid hormone (PTH) serum levels and blood pressure (BP) values in normotensive and hypertensive subjects.
Table 1.
Parathyroid hormone (PTH) serum levels and blood pressure (BP) values in normotensive and hypertensive subjects.
| Reference (First Author) | Method | Country and Participants | PTH (pmol/L) | BP (SBP − DBP mmHg) |
|---|---|---|---|---|
| Young 1990 [28] | Cross-sectional | USA, 115 subjects, ≈45 years | NT = 4.5 ± 2.2 | NT = 120(±11) − 80(±8) |
| HT = 5.0 ± 2.4 | HT = 138(±8) − 95(±5) | |||
| Brickman 1990 [29] | Cross-sectional | USA, 38 men, ≈56 years | NT = 20.8 ± 1.1 | NT = 123(±2.8) − 78(±1.3) |
| HT = 28.4 + 3.5 | HT = 150(±3.9) − 97(±0.9) | |||
| Morfis 1997 [30] | Cross-sectional | Australia, 123 subjects, 63–88 years | NT = 2.7 ± 1.1 | NT = 125(±12) − 71(±7) |
| HT = 2.9 ± 1.3 | HT =135(±14) − 73(±10) | |||
| Park 2015 [32] | Cross-sectional | Korea, 1664 postmenopausal women, >50 years | NT = 63.7 ± 23.4 | NT = 117.5(±12.4) − 73.3(±8.1) |
| HT = 68.3 ± 23.6 | HT = 149.4(±11.4) − 86.0(±10.1) |
NT = normotensive people; HT = hypertensive people, SBP = systolic blood pressure; DBP = diastolic blood pressure. Values are expressed as mean (±standard deviation).
Table 2.
Blood pressure (BP) values by quartiles or quintiles of parathyroid hormone (PTH) levels in human studies.
Table 2.
Blood pressure (BP) values by quartiles or quintiles of parathyroid hormone (PTH) levels in human studies.
| Reference (First Author) | Method | Country and Participants | PTH (pmol/L) | BP (SBP − DBP mmHg) |
|---|---|---|---|---|
| Snijder 2007 [31] | Cross-sectional | The Netherlands, 1205 subjects, participants, 55–85 years | Q1: <2.45 | 150.1(±26.1) − 82.5(±13.0) |
| Q2: 2.45–3.13 | 151.7(±24.8) − 82.6(±13.4) | |||
| Q3: 3.14–4.25 | 154.7(±24.6) – 84.3(±13.6) | |||
| Q4: >4.25 | 156.2(±27.6) − 83.9(±13.0) | |||
| Chan 2011 [25] | Cross-sectional | China, 939 men, >65 years | Q1: <3.1 | 135.8(±1.7) − 76.5(±0.8) |
| Q2: 3.2–4.1 | 139.9(±1.6) − 76.5(±0.8) | |||
| Q3: 4.2–5.5 | 141.4(±1.7) − 76.5(±0.8) | |||
| Q4: >5.5 | 143.6(±1.8) − 79.9(±0.8) | |||
| Yao 2016 [33] | Cohort study | USA, 7504 subjects, 45–64 years | Q1: 3.2–28.8 | 112(±13) − 68.0(±8.2) |
| Q2: 28.9–34.9 | 113(±12) − 68.4(±8.3) | |||
| Q3: 35.0–41.5 | 114(±12) − 69.4(±8.5) | |||
| Q4: 41.6–50.1 | 115(±12) − 69.9(±8.1) | |||
| Q5: 50.2–162.6 | 115(±12) − 70.5(±8.2) |
SBP = systolic blood pressure; DBP = diastolic blood pressure. Values are expressed as mean (±standard deviation) or mean [±standard error of the mean].
Table 3.
Parathyroid hormone (PTH) and blood pressure (BP) and dietary calcium intake in human studies.
Table 3.
Parathyroid hormone (PTH) and blood pressure (BP) and dietary calcium intake in human studies.
| Reference (First Author) | Method | Country and Participants | Ca Intake (mg/day) | PTH (pmol/L) | BP (SBP − DBP mmHg) | |
|---|---|---|---|---|---|---|
| Takagi 1991 [34] | Clinical trial | Japan, 9 HT, 65–86 years, CaSup (1 g) vs. diet Ca 500 mg, 8 weeks | 1 g/day (CaSup) | 27 | −13.6 mmHg to −5.0 mmHg | |
| 500 mg/day (diet) | 33 | −1.5 mmHg to +1.0 mmHg | ||||
| Jorde 2000 [36] | Cohort study | Norway, 1113 subjects, 30–79 years | 592.1(±459.6) | 4.5(±1.2) | 143.4(±19.9) − 84.3(±10.4) | |
| 400.3(±227.3) | 9.1(±2.4) | 153.9(±27.1) − 89.7(±14.1) | ||||
| Kamycheva 2004 [35] | Cross-sectional | Norway, 3570 subjects, >24 years | ♂ | 499(±259) | Q1 <1.9 | 136.9(±17.7) |
| 476(±257) | Q2 1.9–2.6 | 140.1(±19.6) | ||||
| 443(±233) | Q3 2.61–3.5 | 142.0(±20.3) | ||||
| 430(±243) | Q4 >3.5 | 145.2(±20.3) | ||||
| ♀ | 478(±277) | Q1 <1.8 | 133.2(±18.5) | |||
| 428(±227) | Q2 1.8–2.4 | 135.5(±21.5) | ||||
| 431(±226) | Q3 2.41–3.3 | 141.9(±22.4) | ||||
| 408(±217) | Q4 >3.3 | 146.5(±23.2) | ||||
NT = normotensive people; HT = hypertensive people, CaSup= calcium supplementation; SBP = systolic blood pressure; DBP = diastolic blood pressure. Values are expressed as mean (±standard deviation).
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Villa-Etchegoyen, C.; Lombarte, M.; Matamoros, N.; Belizán, J.M.; Cormick, G. Mechanisms Involved in the Relationship between Low Calcium Intake and High Blood Pressure. Nutrients 2019, 11, 1112. https://doi.org/10.3390/nu11051112
AMA Style
Villa-Etchegoyen C, Lombarte M, Matamoros N, Belizán JM, Cormick G. Mechanisms Involved in the Relationship between Low Calcium Intake and High Blood Pressure. Nutrients. 2019; 11(5):1112. https://doi.org/10.3390/nu11051112
Chicago/Turabian StyleVilla-Etchegoyen, Cecilia, Mercedes Lombarte, Natalia Matamoros, José M. Belizán, and Gabriela Cormick. 2019. "Mechanisms Involved in the Relationship between Low Calcium Intake and High Blood Pressure" Nutrients 11, no. 5: 1112. https://doi.org/10.3390/nu11051112
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.