Comparisons of Estimated Intakes and Plasma Concentrations of Selected Fatty Acids in Pregnancy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
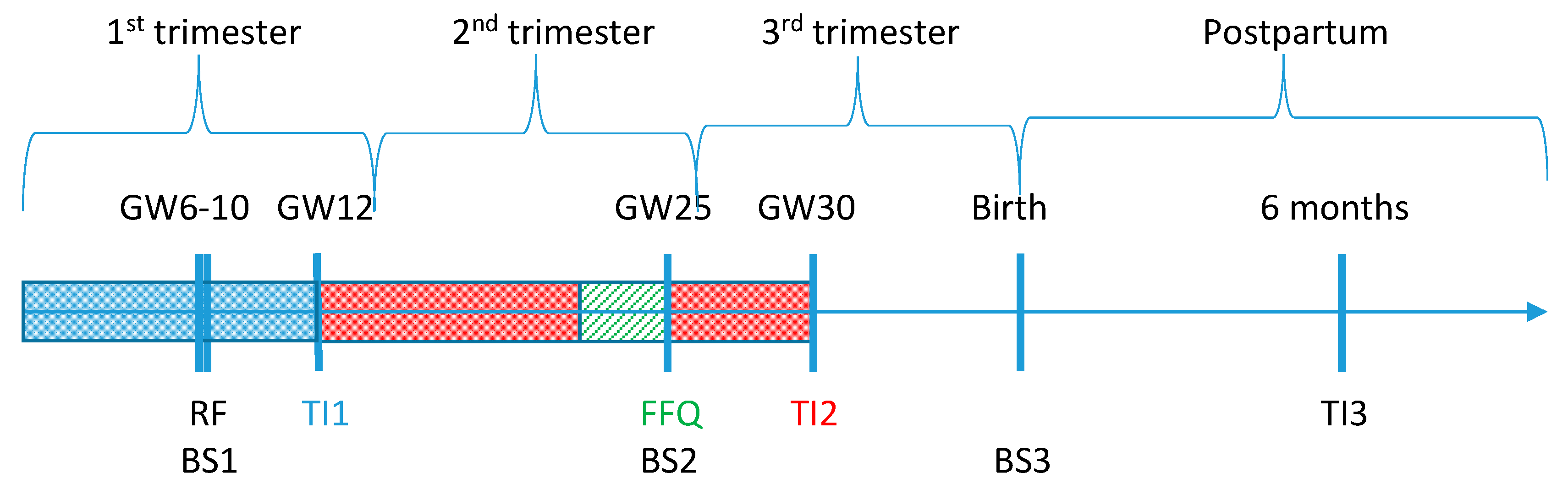
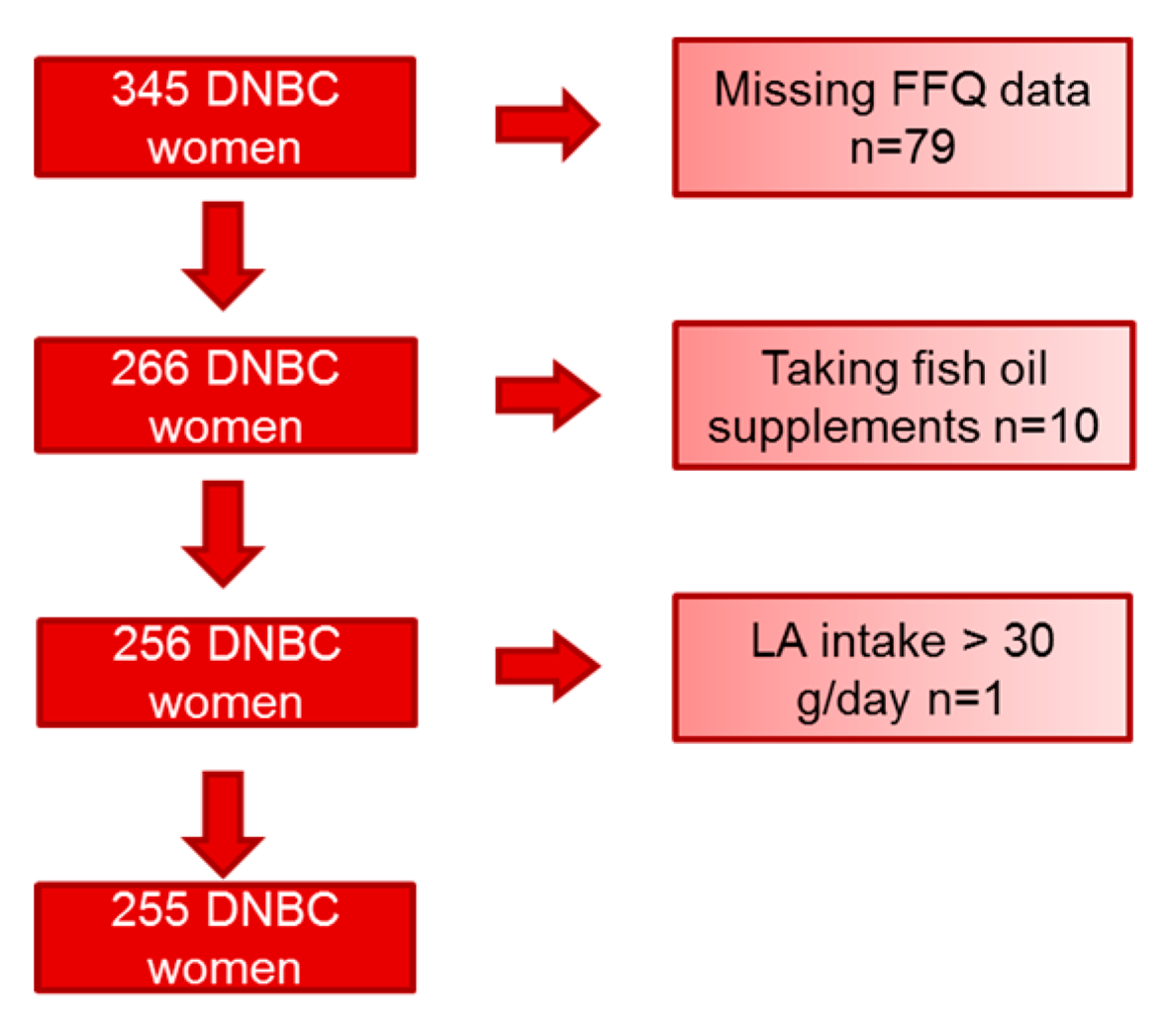
2.1. The Cohort Database
2.2. Dietary Fatty Acid Intake
2.3. Plasma Fatty Acid Concentration
2.4. Statistical Analyses
2.5. Secondary Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Swanson, D.; Block, R.; Mousa, S.A. Omega-3 fatty acids EPA and DHA: Health benefits throughout life. Adv. Nutr. 2012, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bisgaard, H.; Stokholm, J.; Chawes, B.L.; Vissing, N.H.; Bjarnadóttir, E.; Schoos, A.M.; Wolsk, H.M.; Pedersen, T.M.; Vinding, R.K.; Thorsteinsdóttir, S.; et al. Fish Oil-Derived Fatty Acids in Pregnancy and Wheeze and Asthma in Offspring. N. Engl. J. Med. 2016, 375, 2530–2539. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am. J. Clin. Nutr. 2006, 83, 1505S–1519S. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.; Strøm, M.; Maslova, E.; Dahl, R.; Hoffmann, H.J.; Rytter, D.; Bech, B.H.; Henriksen, T.B.; Granström, C.; Halldorsson, T.I.; et al. Fish oil supplementation during pregnancy and allergic respiratory disease in the adult offspring. J. Allergy Clin. Immunol. 2017, 139, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Imhoff-Kunsch, B.; Briggs, V.; Goldenberg, T.; Ramakrishnan, U. Effect of n-3 long-chain polyunsaturated fatty acid intake during pregnancy on maternal, infant, and child health outcomes: A systematic review. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. 1), 91–107. [Google Scholar] [CrossRef] [PubMed]
- Riediger, N.D.; Othman, R.A.; Suh, M.; Moghadasian, M.H. A systemic review of the roles of n-3 fatty acids in health and disease. J. Am. Diet. Assoc. 2009, 109, 668–679. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Hodson, L.; Skeaff, C.M.; Fielding, B.A. Fatty acid composition of adipose tissue and blood in humans and its use as a biomarker of dietary intake. Prog. Lipid Res. 2008, 47, 348–380. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Nissensohn, M.; Øverby, N.C.; Fekete, K. Dietary methods and biomarkers of omega 3 fatty acids: A systematic review. Br. J. Nutr. 2012, 107 (Suppl. 2), S64–S76. [Google Scholar] [CrossRef] [PubMed]
- Baylin, A.; Kim, M.K.; Donovan-Palmer, A.; Siles, X.; Dougherty, L.; Tocco, P.; Campos, H. Fasting whole blood as a biomarker of essential fatty acid intake in epidemiologic studies: Comparison with adipose tissue and plasma. Am. J. Epidemiol. 2005, 162, 373–381. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.A.; Hughes, M.C.; Marks, G.C. Validation of a FFQ to estimate the intake of PUFA using plasma phospholipid fatty acids and weighed foods records. Br. J. Nutr. 2007, 97, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Ma, J.; Campos, H.; Hankinson, S.E.; Hu, F.B. Comparison between plasma and erythrocyte fatty acid content as biomarkers of fatty acid intake in US women. Am. J. Clin. Nutr. 2007, 86, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.M.; Simpson, J.A.; Gibson, R.A.; Sinclair, A.J.; Makrides, M.; O’Dea, K.; English, D.R.; Giles, G.G. Plasma phospholipid fatty acid composition as a biomarker of habitual dietary fat intake in an ethnically diverse cohort. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Jwa, S.C.; Ogawa, K.; Morisaki, N.; Fujiwara, T. Validity of a food frequency questionnaire to estimate long-chain polyunsaturated fatty acid intake among Japanese women in early and late pregnancy. J. Epidemiol. 2017, 27, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Warensjö Lemming, E.; Nälsén, C.; Becker, W.; Ridefelt, P.; Mattisson, I.; Lindroos, A.K. Relative validation of the dietary intake of fatty acids among adults in the Swedish National Dietary Survey using plasma phospholipid fatty acid composition. J. Nutr. Sci. 2015, 4, e25. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, T.B.; Osler, M.; Olsen, S.F. Validity of protein, retinol, folic acid and n-3 fatty acid intakes estimated from the food-frequency questionnaire used in the Danish National Birth Cohort. Public Health Nutr. 2006, 9, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Melbye, M.; Olsen, S.F.; Sørensen, T.I.; Aaby, P.; Andersen, A.M.; Taxbøl, D.; Hansen, K.D.; Juhl, M.; Schow, T.B.; et al. The Danish National Birth Cohort--its background, structure and aim. Scand. J. Public Health. 2001, 29, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.F.; Mikkelsen, T.B.; Knudsen, V.K.; Orozova-Bekkevold, I.; Halldórsson, T.I.; Strøm, M.; Osterdal, M.L. Data collected on maternal dietary exposures in the Danish National Birth Cohort. Paediatr. Perinat. Epidemiol. 2007, 21, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Fødevaredata, 2nd ed.; Danmarks Tekniske Universitet: Copenhagen, Denmark, 2016.
- Zock, P.L.; Gerritsen, J.; Katan, M.B. Partial conservation of the sn-2 position of dietary triglycerides in fasting plasma lipids in humans. Eur. J. Clin. Invest. 1996, 26, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Zock, P.L.; Mensink, R.P.; Harryvan, J.; de Vries, J.H.; Katan, M.B. Fatty acids in serum cholesteryl esters as quantitative biomarkers of dietary intake in humans. Am. J. Epidemiol. 1997, 145, 1114–1122. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.F.; Halldorsson, T.I.; Thorne-Lyman, A.L.; Strøm, M.; Gørtz, S.; Granstrøm, C.; Nielsen, P.H.; Wohlfahrt, J.; Lykke, J.A.; Langhoff-Roos, J.; et al. Plasma Concentrations of Long Chain N-3 Fatty Acids in Early and Mid-Pregnancy and Risk of Early Preterm Birth. EBioMedicine 2018, 35, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Fagt, S.; Biltoft-Jensen, A.; Matthiessen, J.; Groth, M.V.; Christensen, T.; Trolle, E. Danskernes Kostvaner 1995–2006 Status og Udvikling Med Fokus på Frugt og Grønt Samt Sukker; Danmarks Tekniske Universitet: Copenhagen, Denmark, 2008. [Google Scholar]
- Sullivan, B.L.; Williams, P.G.; Meyer, B.J. Biomarker validation of a long-chain omega-3 polyunsaturated fatty acid food frequency questionnaire. Lipids 2006, 41, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.F.; Solvoll, K.; Drevon, C.A. Very-long-chain n-3 fatty acids as biomarkers for intake of fish and n-3 fatty acid concentrates. Am. J. Clin. Nutr. 1996, 64, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Giltay, E.J.; Gooren, L.J.; Toorians, A.W.; Katan, M.B.; Zock, P.L. Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. Am. J. Clin. Nutr. 2004, 80, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Pusukuru, R.; Shenoi, A.S.; Kyada, P.K.; Ghodke, B.; Mehta, V.; Bhuta, K.; Bhatia, A. Evaluation of Lipid Profile in Second and Third Trimester of Pregnancy. J. Clin. Diagn Res. 2016, 10, QC12–QC16. [Google Scholar] [CrossRef] [PubMed]
- Crozier, S.; Robinson, S.; Borland, S.; Godfrey, K.; Cooper, C.; Inskip, H.; Grp, S.S.; Grp, S.S. Do women change their health behaviours in pregnancy? Findings from the Southampton Women’s Survey. Paediatr. Perinat. Epidemiol. 2009, 23, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Sasaki, S.; Kawabata, T.; Hasegawa, K.; Tsugane, S.; JPHC. Validity of a self-administered food frequency questionnaire used in the 5-year follow-up survey of the JPHC Study Cohort I to assess fatty acid intake: Comparison with dietary records and serum phospholipid level. J. Epidemiol. 2003, 13, S64–S81. [Google Scholar] [CrossRef] [PubMed]
- Marckmann, P.; Lassen, A.; Haraldsdóttir, J.; Sandström, B. Biomarkers of habitual fish intake in adipose tissue. Am. J. Clin. Nutr. 1995, 62, 956–959. [Google Scholar] [CrossRef] [PubMed]
- Tjønneland, A.; Overvad, K.; Thorling, E.; Ewertz, M. Adipose tissue fatty acids as biomarkers of dietary exposure in Danish men and women. Am. J. Clin. Nutr. 1993, 57, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Vidgren, H.M.; Agren, J.J.; Schwab, U.; Rissanen, T.; Hänninen, O.; Uusitupa, M.I. Incorporation of n-3 fatty acids into plasma lipid fractions, and erythrocyte membranes and platelets during dietary supplementation with fish, fish oil, and docosahexaenoic acid-rich oil among healthy young men. Lipids 1997, 32, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Stampfer, M.J.; Munoz, A.; McManus, K.; Canessa, M.; Kass, E.H. Effect of linoleic and oleic acids on blood pressure, blood viscosity, and erythrocyte cation transport. J. Am. Coll. Nutr. 1987, 6, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Farukhi, Z.; Mora, S. Re-assessing the role of non-fasting lipids; a change in perspective. Ann. Transl. Med. 2016, 4, 431. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age, years | 29.5 (4.4) |
| BMI, kg/m2 | 23.2 (4.2) |
| Parity, n (%) | |
| 0 children | 118, 51% |
| 1 child | 84, 36% |
| ≥2 children | 30, 13% |
| Smoking, n (%) | |
| Non-smoker | 177, 70% |
| Occasional smoker | 26, 10% |
| Daily smoker <15 cigarettes/day | 43, 17% |
| Daily smoker ≥15 cigarettes/day | 8, 3% |
| Education, n (%) 201 | |
| 10th grade or less | 53, 26% |
| High school similar or more | 140, 70% |
| Dietary intake | |
| Total energy intake, kJ/day | 10,210 (2550) |
| Carbohydrate, % energy | 51.8 (5.9) |
| Fat, % energy | 32.6 (6.3) |
| Protein, % energy | 15.2 (2.5) |
| Alcohol, % energy | 0.4 (0.5) |
| EPA, g/day | 0.10 (0.12) * |
| DHA, g/day | 0.26 (0.25) * |
| EPA + DHA, g/day | 0.37 (0.35) * |
| ALA, g/day | 2.06 (1.17) * |
| LA, g/day | 9.81 (4.36) * |
| AA, g/day | 0.08 (0.06) * |
| Plasma biomarker (%TPFA) | |
| EPA | 0.45 (0.21) |
| DHA | 1.53 (0.55) |
| EPA + DHA | 1.99 (0.73) |
| ALA | 0.58 (0.15) |
| LA | 19.86 (3.12) |
| AA | 3.08 (1.02) |
| Regression Coefficients (95% CI) from Linear Regressions | Correlation Coefficients | ||
| Non-Adjusted | Adjusted for Age, Parity, BMI, Smoking, and Total Energy Intake | ||
| EPA | 0.05 (0.02; 0.08) % per 100 mg/day ** | 0.05 (0.02; 0.08) % per 100 mg/day * | 0.24 *** |
| DHA | 0.05 (0.01; 0.08) % per 100 mg/day * | 0.05 (0.01; 0.08) % per 100 mg/day * | 0.18 * |
| EPA + DHA | 0.05 (0.02; 0.08) % per 100 mg/day * | 0.05 (0.02; 0.08) % per 100 mg/day * | 0.21 ** |
| ALA | 0.03 (0.01; 0.05) % per 1 g/day | 0.07 (0.03; 0.10) % per 1 g /day ** | 0.15 a |
| LA | 0.10 (−0.01; 0.22) % per 1 g/day | 0.17 (−0.04; 0.38) % per 1 g/day | 0.08 |
| AA | 0.01 (−0.02; 0.03) % per 10 mg/day | 0.02 (−0.01; 0.04) % per 10 mg/day | 0.05 a |
| Regression Coefficients (95% CI) from Linear Regressions | Correlation Coefficient | |||
| Non-Adjusted | Adjusted for Age, Parity, BMI, Smoking and Total Energy Intake | |||
| EPA | ≥2.06 g/day ALA | 0.05 (0.01; 0.09) % per 100 mg/day | 0.05 (0.01; 0.09) % per 100 mg/day | 0.18 |
| <2.06 g/day ALA | 0.06 (0.02; 0.11) % per 100 mg/day * | 0.05 (0.01; 0.10) % per 100 mg/day * | 0.33 ** | |
| DHA | ≥2.06 g/day ALA | 0.03 (−0.02; 0.07) % per 100 mg/day | 0.02 (−0.02; 0.07) % per 100 mg/day | 0.09 |
| <2.06 g/day ALA | 0.09 (0.04; 0.15) % per 100 mg/day * | 0.09 (0.03; 0.14) % per 100 mg/day * | 0.27 * | |
| EPA + DHA | ≥2.06 g/day ALA | 0.03 (−0.01; 0.07) % per 100 mg/day | 0.03 (−0.01; 0.07) % per 100 mg/day | 0.12 |
| <2.06 g/day ALA | 0.08 (0.03; 0.14) % per 100 mg/day * | 0.08 (0.03; 0.13) % per 100 mg/day * | 0.29 ** | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
B. Madsen, M.T.; A. Bjerregaard, A.; Furtado, J.D.; Halldorsson, T.I.; Ström, M.; Granström, C.; Giovannucci, E.; Olsen, S.F. Comparisons of Estimated Intakes and Plasma Concentrations of Selected Fatty Acids in Pregnancy. Nutrients 2019, 11, 568. https://doi.org/10.3390/nu11030568
B. Madsen MT, A. Bjerregaard A, Furtado JD, Halldorsson TI, Ström M, Granström C, Giovannucci E, Olsen SF. Comparisons of Estimated Intakes and Plasma Concentrations of Selected Fatty Acids in Pregnancy. Nutrients. 2019; 11(3):568. https://doi.org/10.3390/nu11030568
Chicago/Turabian StyleB. Madsen, Marie T., Anne A. Bjerregaard, Jeremy D. Furtado, Thorhallur I. Halldorsson, Marin Ström, Charlotta Granström, Edward Giovannucci, and Sjurdur F. Olsen. 2019. "Comparisons of Estimated Intakes and Plasma Concentrations of Selected Fatty Acids in Pregnancy" Nutrients 11, no. 3: 568. https://doi.org/10.3390/nu11030568