Paediatric Home Artificial Nutrition in Italy: Report from 2016 Survey on Behalf of Artificial Nutrition Network of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP)

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
- patient initials
- current age
- age at HAN beginning
- gender
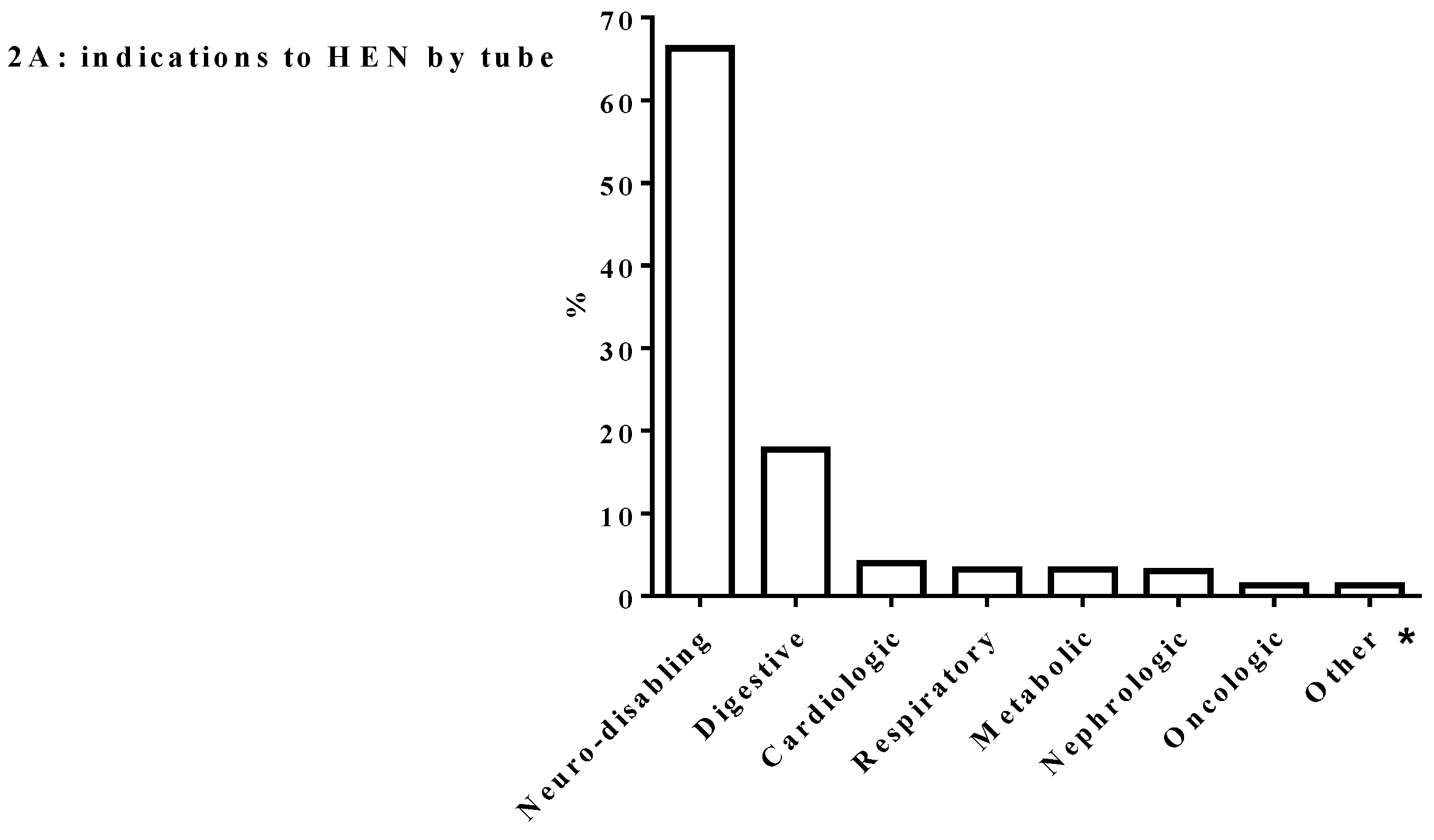
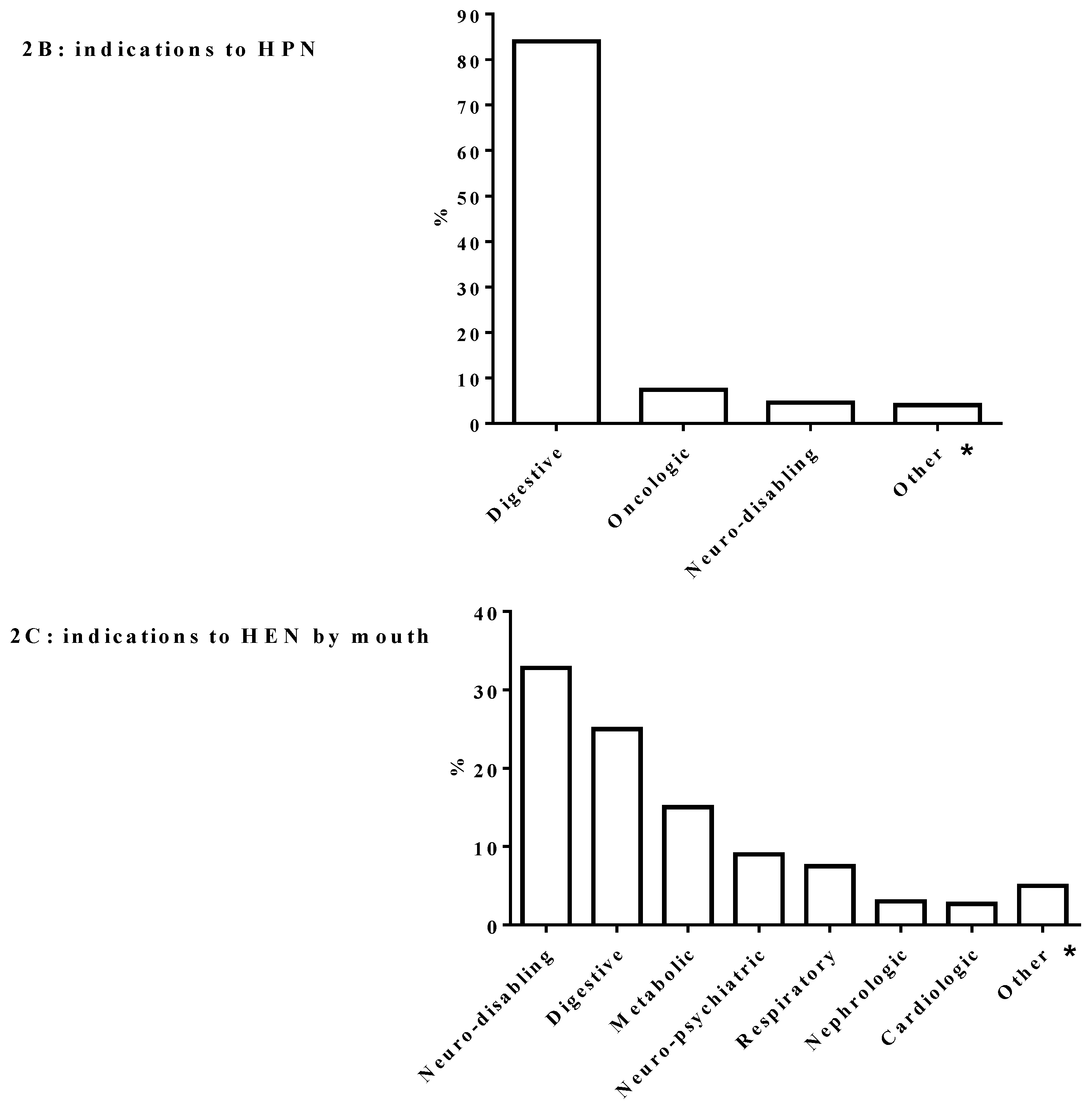
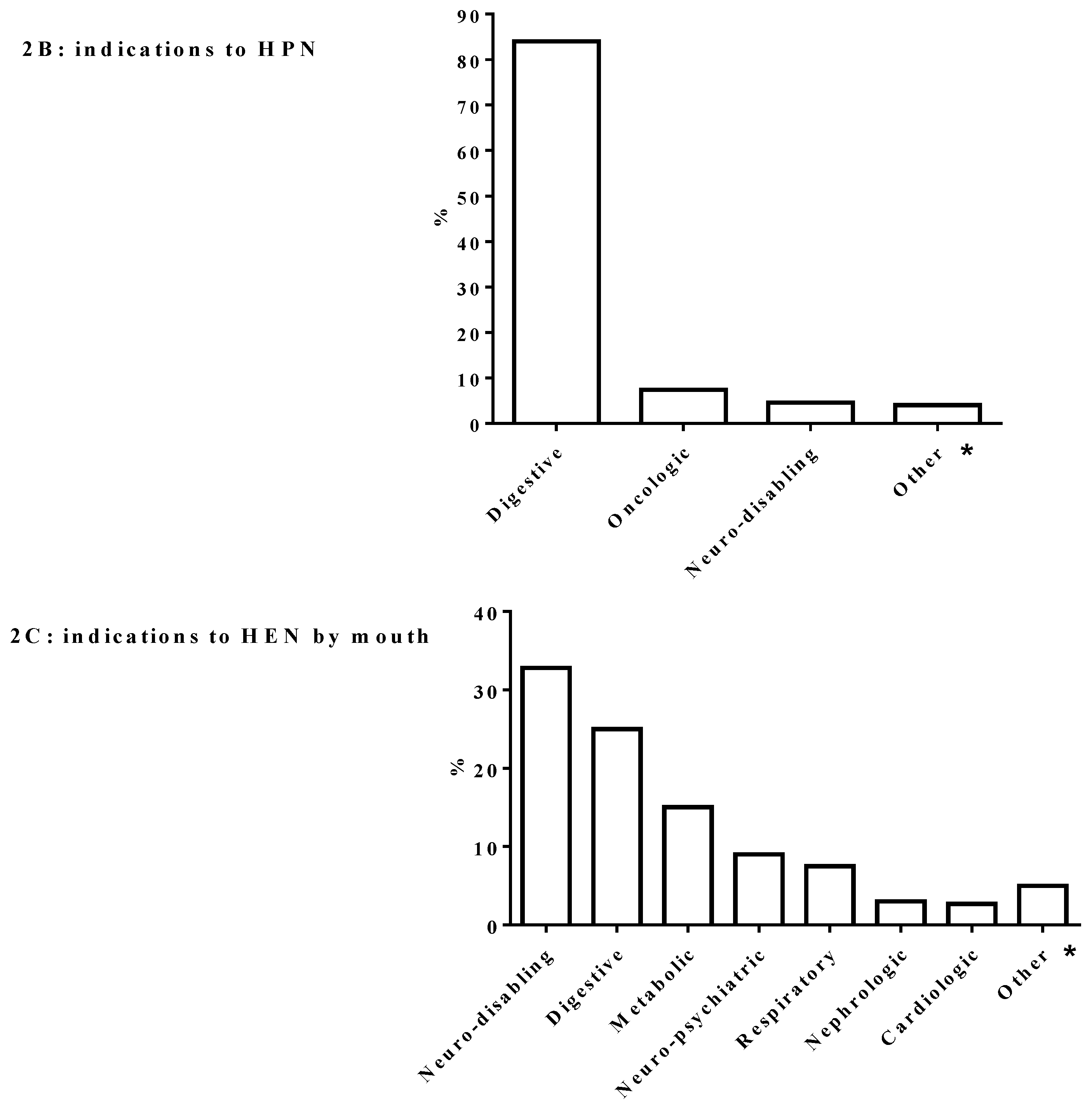
- primary diagnosis requiring HAN
- number of HEN by tube and HPN programs started in 2016
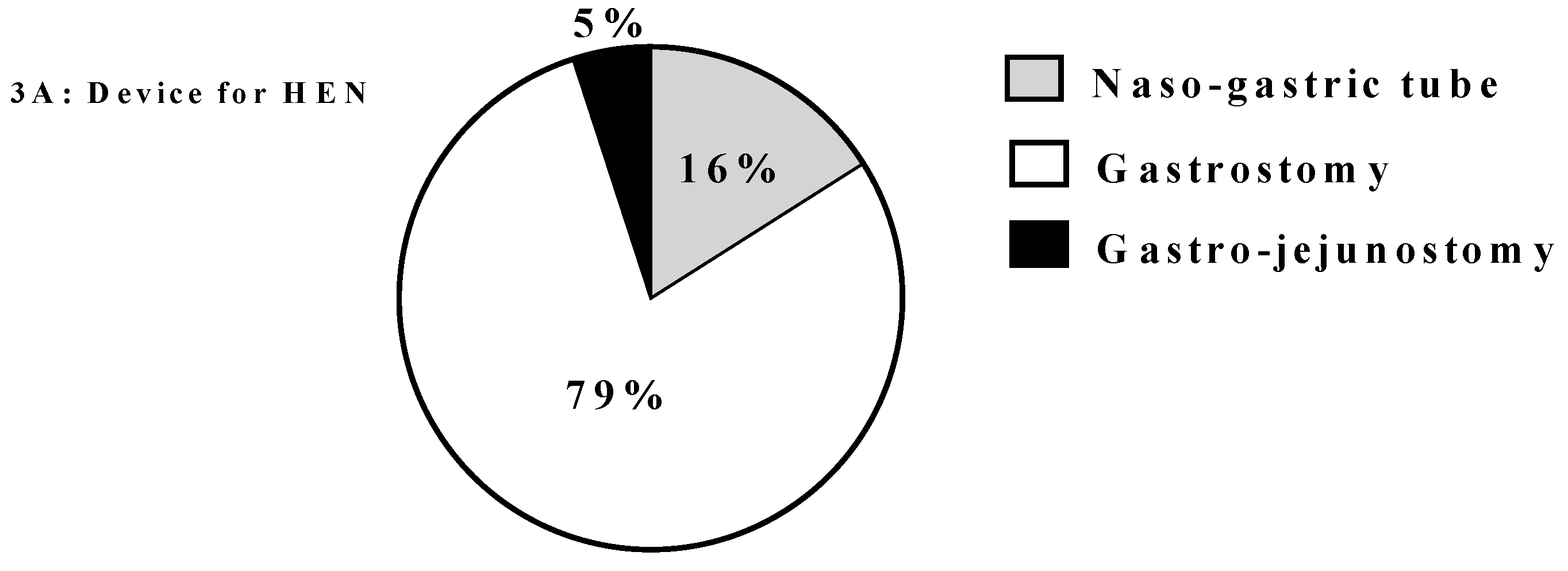
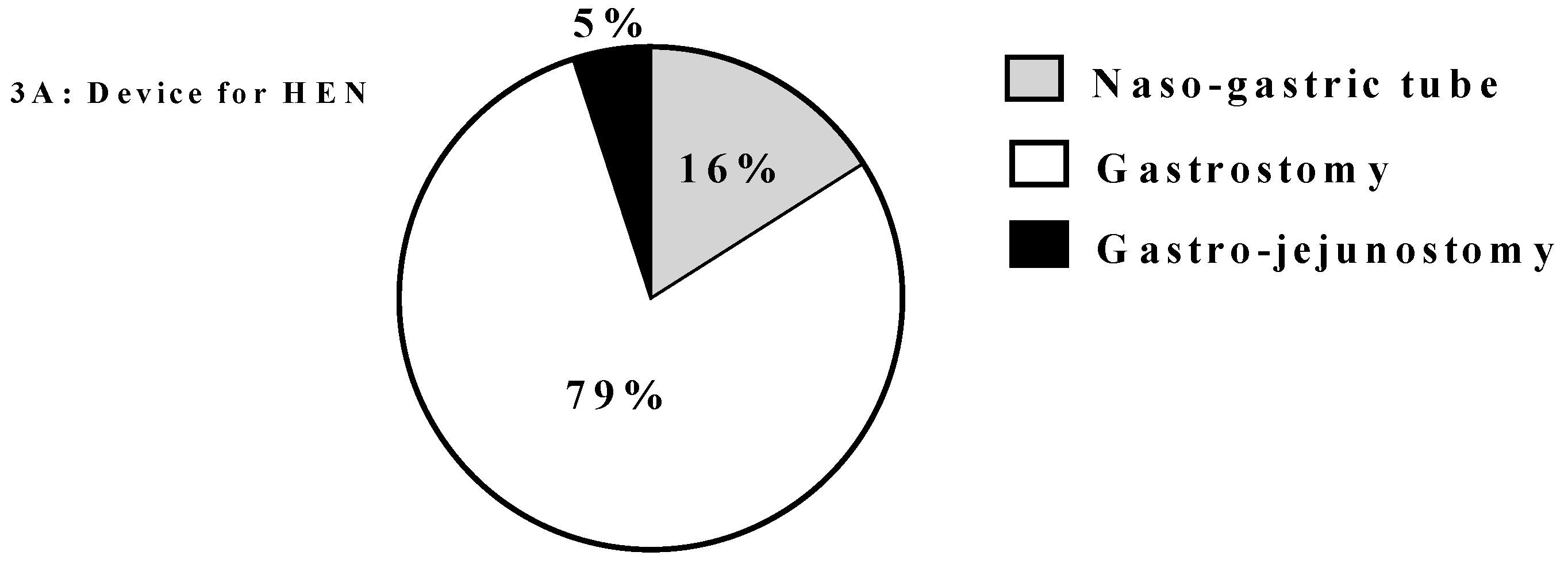
- device for HEN delivery
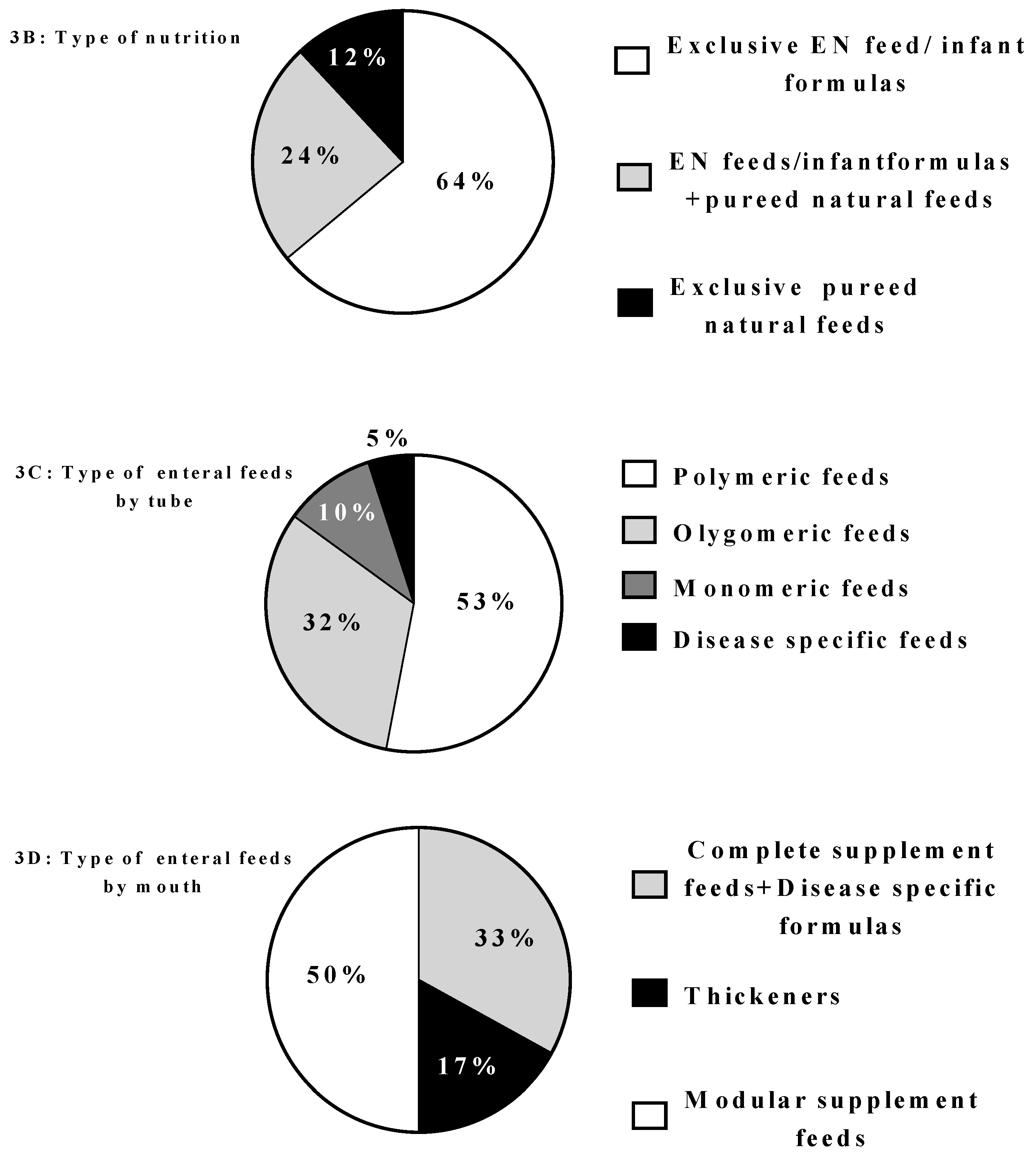
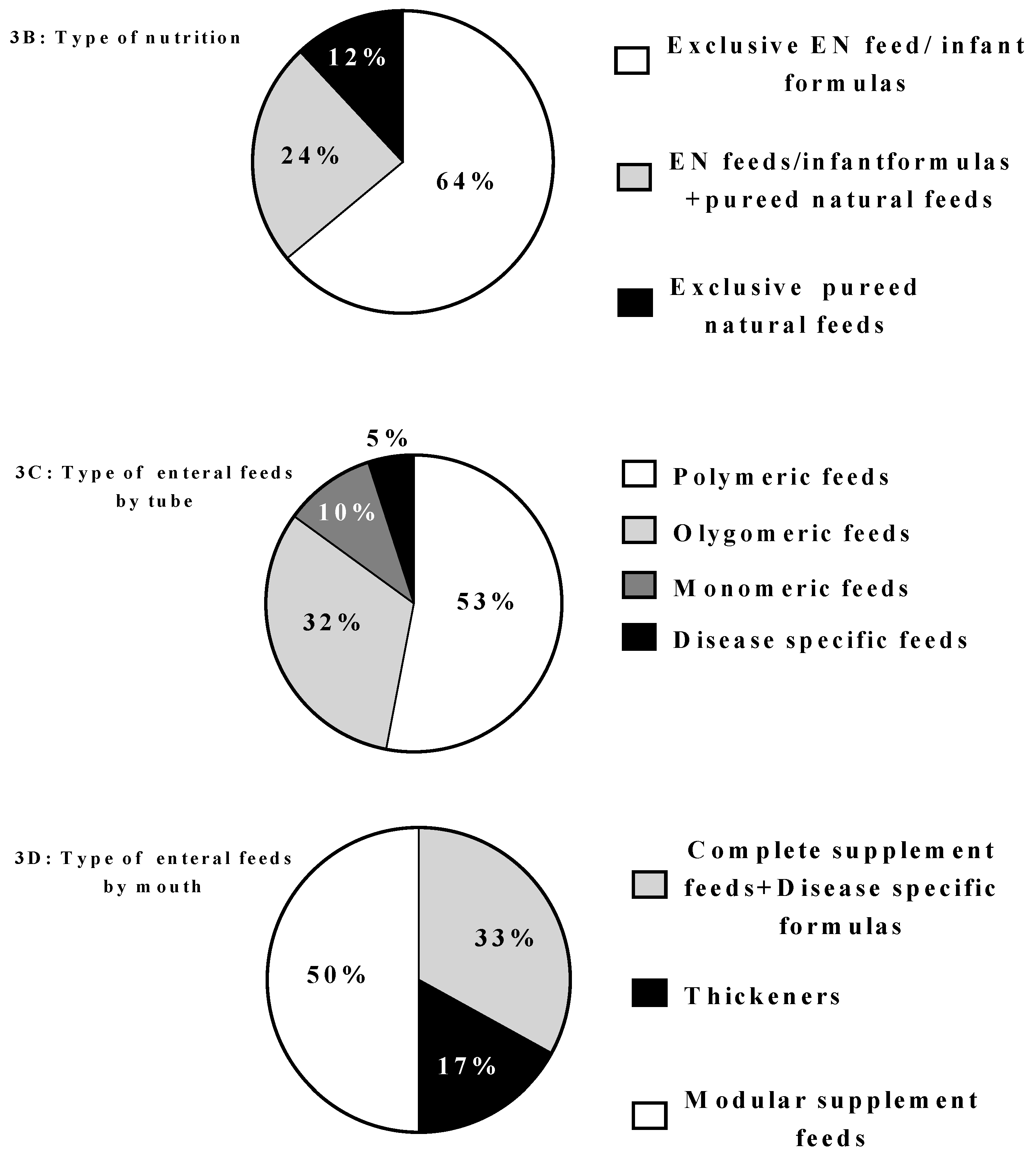
- type of enteral feeds (by tube and mouth)
- type of parenteral bag (customized or standard)
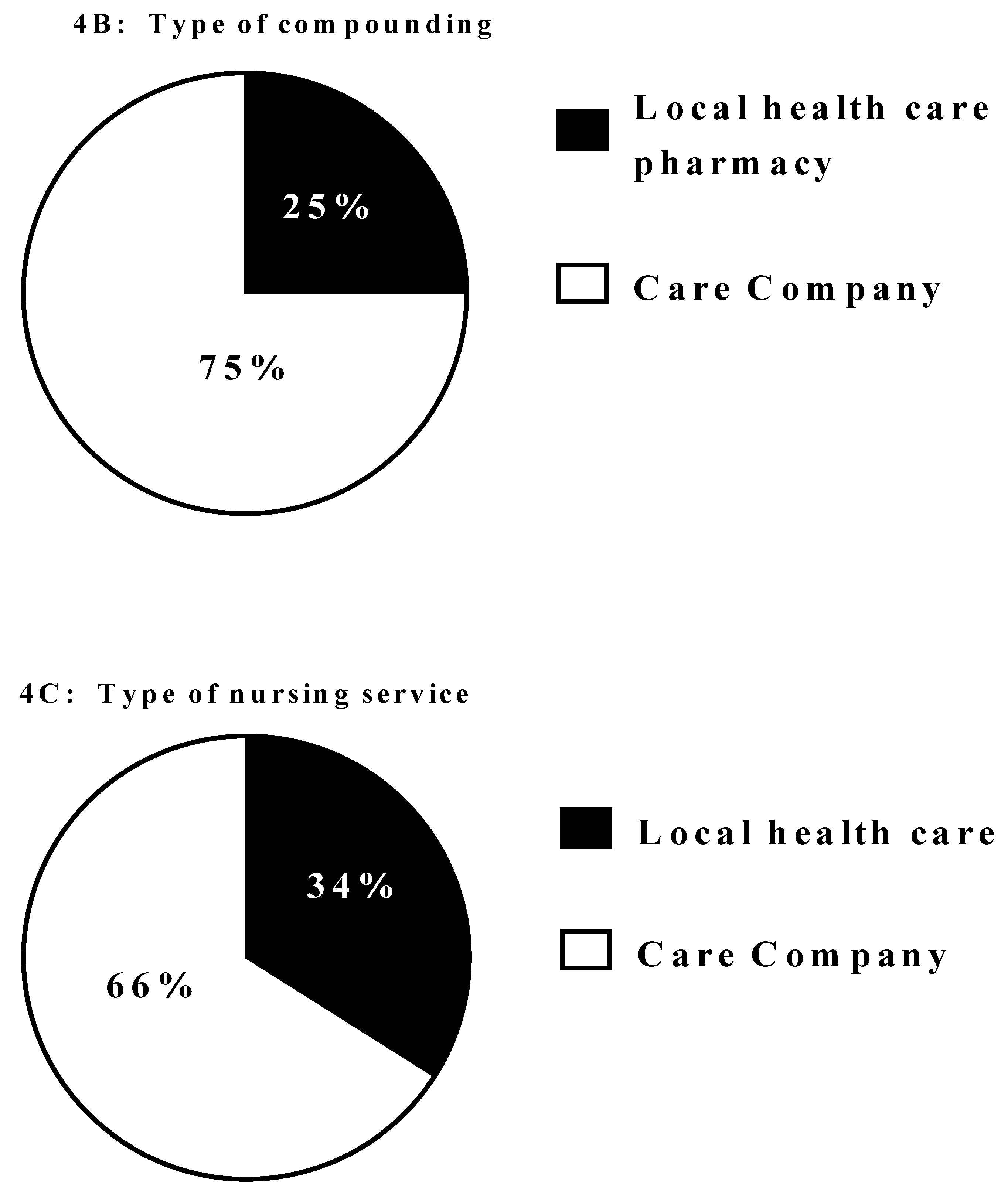
- producer of parenteral bags (care company or local health service pharmacy)
- nursing service for HPN care (care company or local health service)
3. Results
4. Discussion
4.1. Home Enteral Nutrition (HEN)
4.2. Oral Enteral Nutrition (OEN)
4.3. Home Parenteral Nutrition (HPN)
5. Strength and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- ESPGHAN Committee on Nutrition. Practical Approach to Paediatric Enteral Nutrition: A Comment by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 110–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gossum, J.; Colomb, V.; Hebuteme, X. Home parenteral nutrition (HPN) in children: A multicentre survey in Europe in 1997. Clin. Nutr. 1998, 17, 42–43. [Google Scholar] [CrossRef]
- Commission Directive 1999/21/EC of 25 March 1999 on Dietary Foods for Special Medical Purposes. Available online: http://www.idace.org/legislation/fsmps/ Dir%2099-21%20FSMPs.pdf (accessed on 1 July 2018).
- Pironi, L.; Arends, J.; Bozzetti, F. ESPEN guidelines on chronic intestinal failure in adults. Clin. Nutr. 2016, 37, 247–307. [Google Scholar] [CrossRef] [PubMed]
- Santarpia, L.; Pagano, M.C.; Pasanisi, F.; Contaldo, F. Home artificial nutrition: An update seven years after the regional regulation. Clin. Nutr. 2014, 33, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Pironi, L.; Candusso, M.; Biondo, A.; Bosco, A.; Castaldi, P.; Contaldo, F.; Finocchiaro, E.; Giannoni, A.; Mazzuoli, S.; Orlandoni, P.; et al. Italian Society for Parenteral and Enteral Nutrition Executive Committee. Prevalence of home artificial nutrition in Italy in 2005: A survey by the Italian Society for Parenteral and Enteral Nutrition (SINPE). Clin. Nutr. 2007, 26, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Diamanti, A.; Di Ciommo, V.M.; Tentolini, A.; Lezo, A.; Spagnuolo, M.I.; Campanozzi, A.; Panetta, F.; Basso, M.S.; Elia, D.; Gambarara, M.; on behalf of the Italian Society of the Pediatric Gastroenterology Hepatology and Nutrition (SIGENP). Home enteral nutrition in children: A 14-year multicenter survey. Eur. J. Clin. Nutr. 2013, 67, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Italian Institute for National Statitistics (ISTAT) Home Page. Available online: http://www.istat.it/en/ (accessed on 30 December 2016).
- Pedrón-Giner, C.; Navas-López, V.M.; Martínez-Zazo, A.B.; Martínez-Costa, C.; Sánchez-Valverde, F.; Blasco-Alonso, J.; Moreno-Villares, J.M.; Redecillas-Ferreiro, S.; Canals-Badía, M.J.; Rosell-Camps, A.; et al. Analysis of the Spanish national registry for pediatric home enteral nutrition (NEPAD): Implementation rates and observed trends during the past 8 years. Eur. J. Clin. Nutr. 2013, 67, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Winkler, M.F.; Di Maria-Ghalili, R.A.; Guenter, P.; Resnick, H.E.; Robinson, L.; Lyman, B.; Ireton-Jones, C.; Banchik, L.H.; Steiger, E. Characteristics of a Cohort of Home Parenteral Nutrition Patients at the Time of Enrollment in the Sustain Registry. JPEN J. Parenter. Enter. Nutr. 2016, 40, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Annual BANS Report, 2011. Artificial Nutrition Support in the UK 2000–2010: A Report by the British Artificial Nutrition Survey (BANS), a Committee of BAPEN (The British Association for Parenteral and Enteral Nutrition). Available online: https://www.bapen.org.uk/pdfs/bans_reports/bans_report_11.pdf (accessed on 8 September 2018).
- Diamanti, A.; Capriati, T.; Gandullia, P.; Di Leo, G.; Lezo, A.; Lacitignola, L.; Spagnuolo, M.I.; Gatti, S.; D’Antiga, L.; Verlato, G.; et al. Pediatric Chronic Intestinal Failure in Italy: Report from the 2016 Survey on Behalf of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP). Nutrients 2017, 9, 1217. [Google Scholar] [CrossRef] [PubMed]
- Protheroe, S. Young people, artificial nutrition and transitional care. Transition in young people on home parenteral nutrition. Proc. Nutr. Soc. 2009, 68, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Prevalenza della NAD in Italia nel 2012: Indagine epidemiologica SINPE. Available online: http://www.sifoweb.it/images/pdf/attivita/attivita-scientifica/aree_scientifiche/nutrizione_clinica/SINPE_SurveyNAD2012.pdf (accessed on 1 July 2018).
- Daveluy, W.; Guimber, D.; Uhlen, S.; Lescut, D.; Michaud, L.; Turck, D.; Gottrand, F. Dramatic changes in home-based enteral nutrition practices in children during an 11-year period. J. Pediatr. Gastroenterol. Nutr. 2006, 43, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Beath, S.V.; Gowen, H.; Puntis, J.W.L. Trends in pediatric home parenteral nutrition and implications for service development. Clin. Nutr. 2011, 30, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Kyrana, E.; Beath, S.V.; Gabe, S.; Small, M.; Hill, S.; on Behalf of the Members BAPEN. Current practices and experience of transition of young people on longterm home parenteral nutrition (PN) to adult services e a perspectivefrom specialist centres. Clin. Nutr. ESPEN 2016, 14, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Jürgens, H.; Frühwald, M.C. Important Aspects of Nutrition in Children with Cancer. Adv. Nutr. 2011, 2, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forchielli, M.L.; Azzi, N.; Cadranel, S.; Paolucci, G. Total parenteral nutrition in bone marrow transplant: What is the appropriate energy level? Oncology 2003, 64, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Skolin, I.; Hernell, O.; Larsson, M.V.; Wahlgren, C.; Wahlin, Y.B. Percutaneous endoscopic gastrostomy in children with malignant disease. J. Pediatr. Oncol. Nurs. 2002, 19, 154–163. [Google Scholar] [CrossRef]
- Lakdawalla, D.N.; Mascarenhas, M.; Jena, A.B.; Vanderpuye-Orgle, J.; LaVallee, C.; Linthicum, M.T.; Snider, J.T. Impact of oral nutrition supplements on hospital outcomes in pediatric patients. JPEN J. Parenter. Enter. Nutr. 2014, 38, 42S–49S. [Google Scholar] [CrossRef] [PubMed]
- Wahid, A.M.; Powell, C.V.; Davies, I.H.; Evans, J.A.; Jenkins, H.R. Intestinal failure in children and young people with neurodisabling conditions. Arch. Dis. Child. 2017, 102, 475–476. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Administrative Region | Centre | City | Type of HAN |
|---|---|---|---|
| Lombardia | “Papa Giovanni XXIII” Hospital | Bergamo | HEN, HPN |
| “Sant’Anna” Hospital | Como | HEN | |
| “San Paolo” Hospital | Milano | HEN | |
| “F. Del Ponte” Hospital | Varese | HEN | |
| “Cà Granda” Hospital | Milano | HEN, HPN | |
| Piemonte | “Regina Margherita” Hospital | Torino | HEN, HPN |
| Campania | University Hospital “Federico II” | Napoli | HEN, HPN |
| “Santobono-Pausillipon” Hospital | Napoli | HEN, HPN | |
| Puglia | University Hospital | Bari | HPN |
| Emilia-Romagna | “Sant’Orsola” Hospital | Bologna | HEN, HPN |
| Local health care service | Rimini-Riccione | HEN, HPN | |
| “Bufalini” Hospital | Cesena | HEN | |
| “Morgagni-Pierantoni” Hospital | Forlì | HEN, HPN | |
| “Arcispedale Santa Maria” Hospital | Reggio Emilia | HEN, HPN | |
| “S. Maria delle Croci”Hospital | Ravenna | HEN, HPN | |
| Sicilia | University General Hospital | Messina | HEN |
| Marche | “Salesi”Children’s Hospital | Ancona | HEN, HPN |
| Liguria | “Giannina Gaslini”Children’s Hospital | Genova | HEN, HPN |
| Lazio | “Bambino Gesù”Children’s Hospital | Roma | HEN, HPN |
| Trentino-Alto Adige | “Santa Maria del Carmine” Hospital | Rovereto | HEN |
| Friuli Venezia Giulia | “Burlo Garofolo”Children’s Hospital | Trieste | HEN, HPN |
| Toscana | “Meyer”Children’s Hospital | Firenze | HEN, HPN |
| HEN by Tube | HPN | HEN by Mouth | |
|---|---|---|---|
| Number of programs | 2277 | 176 | 950 |
| (% of overall HAN) | (70) | (5) | (25) |
| M/F (%) | 43/57 | 45/55 | 51/49 |
| Age at HAN beginning (years) | 2.3 | 0.8 | 5.0 |
| (median ± IQ range) | (0.3–9.7) | (0.1–1.8) | (1.6–12) |
| Current age (years) | 7.2 | 4.8 | 9.7 |
| (median ± IQ range) | (1.1–15.0) | (1.7–11.7) | (5.3–14.3) |
| Length of the program | 6 years | 3 years | 1.3 years |
| (median ± IQ range) | (0.1–18.7) | (1.5–6.3) | (0.3–6.8) |
| Prevalence | 204.7 | 15.8 | 85.5 |
| (pts/million of inhabitants < 19 years) | |||
| Incidence | 35.9 | 1.6 | / |
| (pts/million of inhabitants < 19 years) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lezo, A.; Capriati, T.; Spagnuolo, M.I.; Lacitignola, L.; Goreva, I.; Di Leo, G.; Cecchi, N.; Gandullia, P.; Amarri, S.; Forchielli, M.L.; et al. Paediatric Home Artificial Nutrition in Italy: Report from 2016 Survey on Behalf of Artificial Nutrition Network of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP). Nutrients 2018, 10, 1311. https://doi.org/10.3390/nu10091311
Lezo A, Capriati T, Spagnuolo MI, Lacitignola L, Goreva I, Di Leo G, Cecchi N, Gandullia P, Amarri S, Forchielli ML, et al. Paediatric Home Artificial Nutrition in Italy: Report from 2016 Survey on Behalf of Artificial Nutrition Network of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP). Nutrients. 2018; 10(9):1311. https://doi.org/10.3390/nu10091311
Chicago/Turabian StyleLezo, Antonella, Teresa Capriati, Maria Immacolata Spagnuolo, Laura Lacitignola, Irina Goreva, Grazia Di Leo, Nicola Cecchi, Paolo Gandullia, Sergio Amarri, Maria Luisa Forchielli, and et al. 2018. "Paediatric Home Artificial Nutrition in Italy: Report from 2016 Survey on Behalf of Artificial Nutrition Network of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP)" Nutrients 10, no. 9: 1311. https://doi.org/10.3390/nu10091311