Cobalamin and Folate Status among Breastfed Infants in Bhaktapur, Nepal


Abstract
:1. Introduction
2. Methods
2.1. Study Site and Population
2.2. Methods and Study Design
2.3. Ethics
2.4. Blood Sampling and Biochemical Analyses
2.5. Definitions
2.6. Statistical Analyses
3. Results
3.1. General Characteristics and Breast and Complementary Feeding Practices
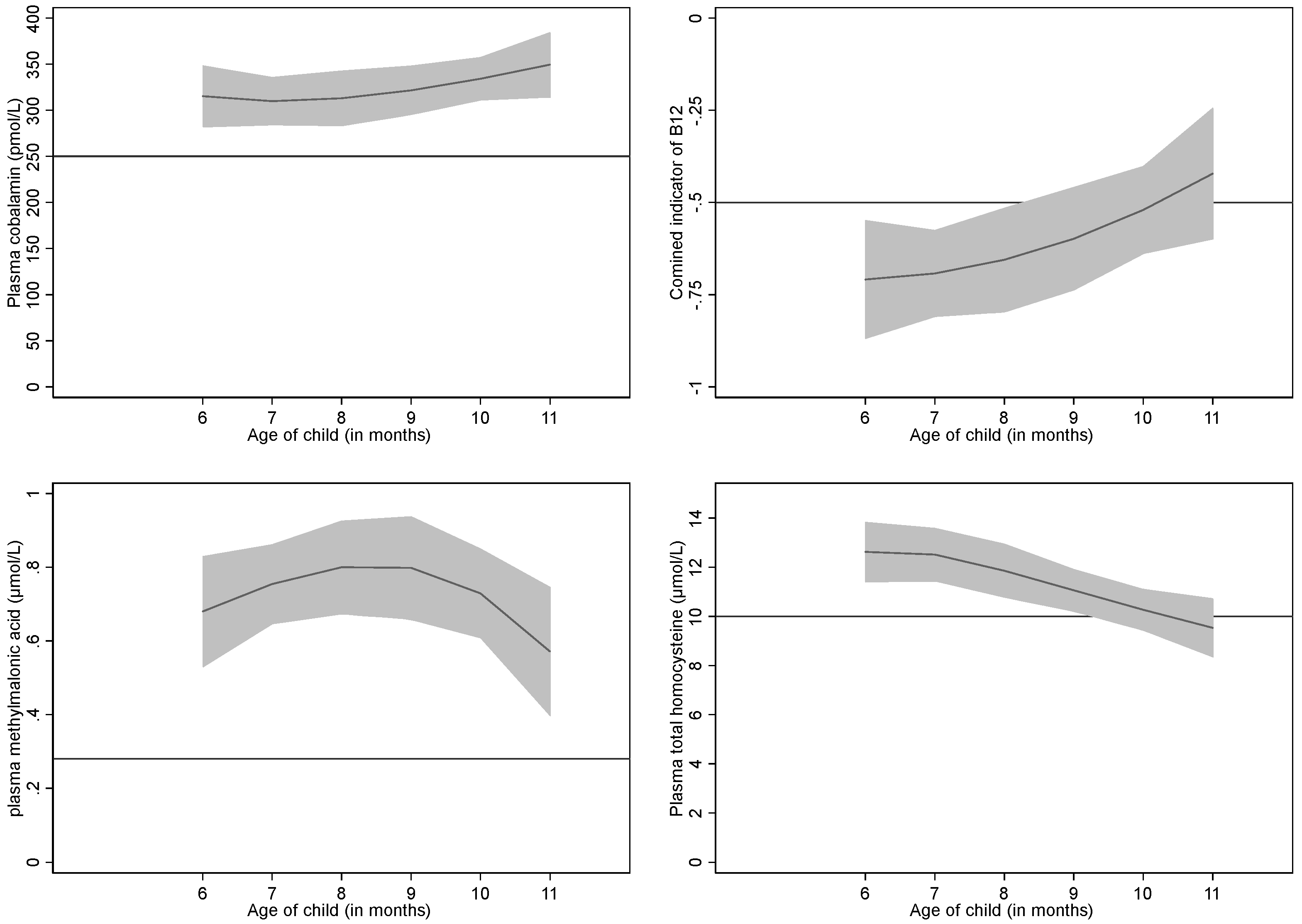
3.2. Plasma Cobalamin, Folate, MMA, tHcy and 3cB12
3.3. Determinants for Cobalamin Status Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
List of Abbreviations
References
- Black, M.M. Effects of vitamin B12 and folate deficiency on brain development in children. Food Nutr. Bull. 2008, 29, S126–S131. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.; Mander, A.; Ames, D.; Carne, R.; Sanders, K.; Watters, D. Cognitive impairment and vitamin B12: A review. Int. Psychogeriatr. 2012, 24, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Obeid, R.; Murphy, M.; Sole-Navais, P.; Yajnik, C. Cobalamin Status from Pregnancy to Early Childhood: Lessons from Global Experience. Adv. Nutr. 2017, 8, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. Causes of vitamin B12 and folate deficiency. Food Nutr. Bull. 2008, 29, S20–S34; discussion S35–S37. [Google Scholar] [CrossRef] [PubMed]
- Samuel, T.M.; Duggan, C.; Thomas, T.; Bosch, R.; Rajendran, R.; Virtanen, S.M.; Srinivasan, K.; Kurpad, A.V. Vitamin B(12) intake and status in early pregnancy among urban South Indian women. Ann. Nutr. Metab. 2013, 62, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Taneja, S.; Bhandari, N.; Strand, T.A.; Sommerfelt, H.; Refsum, H.; Ueland, P.M.; Schneede, J.; Bahl, R.; Bhan, M.K. Cobalamin and folate status in infants and young children in a low-to-middle income community in India. Am. J. Clin. Nutr. 2007, 86, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Chandyo, R.K.; Ulak, M.; Sommerfelt, H.; Schneede, J.; Ueland, P.M.; Strand, T.A. Nutritional Intake and Status of Cobalamin and Folate among Non-Pregnant Women of Reproductive Age in Bhaktapur, Nepal. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Ulak, M.; Chandyo, R.K.; Adhikari, R.K.; Sharma, P.R.; Sommerfelt, H.; Refsum, H.; Strand, T.A. Cobalamin and folate status in 6 to 35 months old children presenting with acute diarrhea in Bhaktapur, Nepal. PLoS ONE 2014, 9, e90079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strand, T.A.; Taneja, S.; Ueland, P.M.; Refsum, H.; Bahl, R.; Schneede, J.; Sommerfelt, H.; Bhandari, N. Cobalamin and folate status predicts mental development scores in North Indian children 12—18 mo of age. Am. J. Clin. Nutr. 2013, 97, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Strand, T.A.; Taneja, S.; Kumar, T.; Manger, M.S.; Refsum, H.; Yajnik, C.S.; Bhandari, N. Vitamin B-12, folic acid, and growth in 6- to 30-month-old children: A randomized controlled trial. Pediatrics 2015, 135, e918–e926. [Google Scholar] [CrossRef] [PubMed]
- Kvestad, I.; Hysing, M.; Shrestha, M.; Ulak, M.; Thorne-Lyman, A.L.; Henjum, S.; Ueland, P.M.; Midttun, O.; Fawzi, W.; Chandyo, R.K.; et al. Vitamin B-12 status in infancy is positively associated with development and cognitive functioning 5 y later in Nepalese children. Am. J. Clin. Nutr. 2017, 105, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Roth, C.; Magnus, P.; Schjolberg, S.; Stoltenberg, C.; Suren, P.; McKeague, I.W.; Davey Smith, G.; Reichborn-Kjennerud, T.; Susser, E. Folic acid supplements in pregnancy and severe language delay in children. JAMA 2011, 306, 1566–1573. [Google Scholar] [CrossRef] [PubMed]
- Suren, P.; Roth, C.; Bresnahan, M.; Haugen, M.; Hornig, M.; Hirtz, D.; Lie, K.K.; Lipkin, W.I.; Magnus, P.; Reichborn-Kjennerud, T.; et al. Association between maternal use of folic acid supplements and risk of autism spectrum disorders in children. JAMA 2013, 309, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Bjorke Monsen, A.L.; Ueland, P.M. Homocysteine and methylmalonic acid in diagnosis and risk assessment from infancy to adolescence. Am. J. Clin. Nutr. 2003, 78, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Refsum, H.; Yajnik, C.S.; Gadkari, M.; Schneede, J.; Vollset, S.E.; Orning, L.; Guttormsen, A.B.; Joglekar, A.; Sayyad, M.G.; Ulvik, A.; et al. Hyperhomocysteinemia and elevated methylmalonic acid indicate a high prevalence of cobalamin deficiency in Asian Indians. Am. J. Clin. Nutr. 2001, 74, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Hannibal, L.; Lysne, V.; Bjorke-Monsen, A.L.; Behringer, S.; Grunert, S.C.; Spiekerkoetter, U.; Jacobsen, D.W.; Blom, H.J. Biomarkers and Algorithms for the Diagnosis of Vitamin B12 Deficiency. Front. Mol. Biosci. 2016, 3, 27. [Google Scholar] [CrossRef] [PubMed]
- Green, R.; Allen, L.H.; Bjorke-Monsen, A.L.; Brito, A.; Gueant, J.L.; Miller, J.W.; Molloy, A.M.; Nexo, E.; Stabler, S.; Toh, B.H.; et al. Vitamin B12 deficiency. Nat. Rev. Dis. Primers 2017, 3, 17040. [Google Scholar] [CrossRef] [PubMed]
- Fedosov, S.N.; Brito, A.; Miller, J.W.; Green, R.; Allen, L.H. Combined indicator of vitamin B12 status: Modification for missing biomarkers and folate status and recommendations for revised cut-points. Clin. Chem. Lab. Med. 2015, 53, 1215–1225. [Google Scholar] [CrossRef] [PubMed]
- WHO/FAO (World Health Organization/Food and Agriculture Organization). Vitamin and Mineral Requirements in Human Nutrition: Report of a Joint FAO/WHO Expert Consultation, Bangkok, Thailand, 21–30 September 1998; WHO/FAO: Geneva, Switzerland, 2004. [Google Scholar]
- NAP; Institute of Medicine. Vitamin B12. In Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academy Press: Washington, DC, USA, 2000; pp. 306–356. [Google Scholar]
- Greibe, E.; Lildballe, D.L.; Streym, S.; Vestergaard, P.; Rejnmark, L.; Mosekilde, L.; Nexo, E. Cobalamin and haptocorrin in human milk and cobalamin-related variables in mother and child: A 9-mo longitudinal study. Am. J. Clin. Nutr. 2013, 98, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. B vitamins in breast milk: Relative importance of maternal status and intake, and effects on infant status and function. Adv. Nutr. 2012, 3, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Koc, A.; Kocyigit, A.; Soran, M.; Demir, N.; Sevinc, E.; Erel, O.; Mil, Z. High frequency of maternal vitamin B12 deficiency as an important cause of infantile vitamin B12 deficiency in Sanliurfa province of Turkey. Eur. J. Nutr. 2006, 45, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Roumeliotis, N.; Dix, D.; Lipson, A. Vitamin B(12) deficiency in infants secondary to maternal causes. Can. Med. Assoc. J. 2012, 184, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, J.L.; Kurpad, A.V.; Thomas, T.; Srinivasan, K.; Duggan, C. Vitamin B12 status in pregnant women and their infants in South India. Eur. J. Clin. Nutr. 2017, 71, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Hay, G.; Trygg, K.; Whitelaw, A.; Johnston, C.; Refsum, H. Folate and cobalamin status in relation to diet in healthy 2-y-old children. Am. J. Clin. Nutr. 2011, 93, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.A. If high folic acid aggravates vitamin B12 deficiency what should be done about it? Nutr. Rev. 2007, 65, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.; Selhub, J. Interaction between excess folate and low vitamin B12 status. Mol. Asp. Med. 2017, 53, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.A.; Fernhoff, P.M.; Scanlon, K.S. Vitamin B12 deficiency in children and adolescents. J. Pediatr. 2001, 138, 10–17. [Google Scholar] [CrossRef] [PubMed]
- New ERA; Ministry of Health, Nepal; ICF. Nepal Demographic and Health Survey 2016: Key Indicators; Ministry of Health: Kathmandu, Nepal, 2017.
- Ng’eno, B.N.; Perrine, C.G.; Whitehead, R.D.; Subedi, G.R.; Mebrahtu, S.; Dahal, P.; Jefferds, M.E. High Prevalence of Vitamin B12 Deficiency and No Folate Deficiency in Young Children in Nepal. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- WHO. Indicators for Assesing Infant and Young Child Feeding Practices. In Proceedings of the Consensus Meeting, Washington, DC, USA, 6–8 November 2007. [Google Scholar]
- Cusick, S.E.; Georgieff, M.K. The Role of Nutrition in Brain Development: The Golden Opportunity of the “First 1000 Days”. J. Pediatr. 2016, 175, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Yajnik, C.S.; Deshmukh, U.S. Maternal nutrition, intrauterine programming and consequential risks in the offspring. Rev. Endocr. Metab. Disord. 2008, 9, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Abeshu, M.A.; Lelisa, A.; Geleta, B. Complementary Feeding: Review of Recommendations, Feeding Practices, and Adequacy of Homemade Complementary Food Preparations in Developing Countries—Lessons from Ethiopia. Front. Nutr. 2016, 3, 41. [Google Scholar] [CrossRef] [PubMed]
- Strand, T.A.; Ulak, M.; Chandyo, R.K.; Kvestad, I.; Hysing, M.; Shrestha, M.; Basnet, S.; Ranjitkar, S.; Shrestha, L.; Shrestha, P.S. The effect of vitamin B12 supplementation in Nepalese infants on growth and development: Study protocol for a randomized controlled trial. Trials 2017, 18, 187. [Google Scholar] [CrossRef] [PubMed]
- Windelberg, A.; Arseth, O.; Kvalheim, G.; Ueland, P.M. Automated assay for the determination of methylmalonic acid, total homocysteine, and related amino acids in human serum or plasma by means of methylchloroformate derivatization and gas chromatography-mass spectrometry. Clin. Chem. 2005, 51, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Molloy, A.M.; Scott, J.M. Microbiological assay for serum, plasma, and red cell folate using cryopreserved, microtiter plate method. Methods Enzymol. 1997, 281, 43–53. [Google Scholar] [PubMed]
- Kelleher, B.P.; Walshe, K.G.; Scott, J.M.; O’Broin, S.D. Microbiological assay for vitamin B12 with use of a colistin-sulfate-resistant organism. Clin. Chem. 1987, 33, 52–54. [Google Scholar] [PubMed]
- WHO. Serum and Red Blood Cell Folate Concentrations for Assessing Folate Status in Population. Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- WHO. World Health Organization. Anthro 2005, Beta Version, 17 February 2006: Software for Assessing Growth and Development of the World’s Children; WHO: Geneva, Switzerland, 2006; Available online: http://www.who.int/childgrowth/software/en/ (accessed on 2 February 2016).
- Labbok, M.; Krasovec, K. Toward consistency in breastfeeding definitions. Stud. Fam. Plan. 1990, 21, 226–230. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; John Wiley & Sons Inc.: New York, NY, USA, 2000. [Google Scholar]
- Bjorke-Monsen, A.L.; Torsvik, I.; Saetran, H.; Markestad, T.; Ueland, P.M. Common metabolic profile in infants indicating impaired cobalamin status responds to cobalamin supplementation. Pediatrics 2008, 122, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Torsvik, I.; Ueland, P.M.; Markestad, T.; Bjorke-Monsen, A.L. Cobalamin supplementation improves motor development and regurgitations in infants: Results from a randomized intervention study. Am. J. Clin. Nutr. 2013, 98, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Stabler, S.P. Vitamin B12 deficiency. N. Engl. J. Med. 2013, 368, 2041–2042. [Google Scholar] [CrossRef] [PubMed]
- Ulak, M.; Chandyo, R.K.; Thorne-Lyman, A.L.; Henjum, S.; Ueland, P.M.; Midttun, O.; Shrestha, P.S.; Fawzi, W.W.; Graybill, L.; Strand, T.A. Vitamin Status among Breastfed Infants in Bhaktapur, Nepal. Nutrients 2016, 8, 149. [Google Scholar] [CrossRef] [PubMed]
- Na, M.; Aguayo, V.M.; Arimond, M.; Dahal, P.; Lamichhane, B.; Pokharel, R.; Chitekwe, S.; Stewart, C.P. Trends and predictors of appropriate complementary feeding practices in Nepal: An analysis of national household survey data collected between 2001 and 2014. Matern. Child Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Ulak, M.; Chandyo, R.K.; Mellander, L.; Shrestha, P.S.; Strand, T.A. Infant feeding practices in Bhaktapur, Nepal: A cross-sectional, health facility based survey. Int. Breastfeed. J. 2012, 7, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koury, M.J.; Ponka, P. New insights into erythropoiesis: The roles of folate, vitamin B12, and iron. Annu. Rev. Nutr. 2004, 24, 105–131. [Google Scholar] [CrossRef] [PubMed]
- Bondevik, G.T.; Schneede, J.; Refsum, H.; Lie, R.T.; Ulstein, M.; Kvale, G. Homocysteine and methylmalonic acid levels in pregnant Nepali women. Should cobalamin supplementation be considered? Eur. J. Clin. Nutr. 2001, 55, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Torsvik, I.K.; Ueland, P.M.; Markestad, T.; Midttun, O.; Bjorke Monsen, A.L. Motor development related to duration of exclusive breastfeeding, B vitamin status and B12 supplementation in infants with a birth weight between 2000–3000 g, results from a randomized intervention trial. BMC Pediatr. 2015, 15, 218. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, J.L.; Layden, A.J.; Stover, P.J. Vitamin B-12 and Perinatal Health. Adv. Nutr. 2015, 6, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Moschonis, G.; Dekkers, R.; Mavrogianni, C.; Grammatikaki, E.; van den Heuvel, E. Vitamin B2, vitamin B12 and total homocysteine status in children and their associations with dietary intake of B-vitamins from different food groups: The Healthy Growth Study. Eur. J. Nutr. 2017, 56, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.Y.; Chan, E.W.; Chui, C.S.; Sutcliffe, A.G.; Wong, I.C. The phenomenon of micronutrient deficiency among children in China: A systematic review of the literature. Public Health Nutr. 2014, 17, 2605–2618. [Google Scholar] [CrossRef] [PubMed]
- Senarath, U.; Dibley, M.J. Complementary feeding practices in South Asia: Analyses of recent national survey data by the South Asia Infant Feeding Research Network. Matern. Child Nutr. 2012, 8 (Suppl. 1), 5–10. [Google Scholar] [CrossRef] [PubMed]
- Khanal, V.; Sauer, K.; Zhao, Y. Determinants of complementary feeding practices among Nepalese children aged 6–23 months: findings from Demographic and Health Survey 2011. BMC Pediatr. 2013, 13, 131. [Google Scholar] [CrossRef] [PubMed]
- Morseth, M.S.; Torheim, L.E.; Gebremariam, M.K.; Chandyo, R.K.; Ulak, M.; Shrestha, S.K.; Shrestha, B.; Henjum, S. Tracking of infant and young child feeding practices among 9- to 24-month-old children in Nepal: The MAL-ED Birth Cohort Study. Public Health Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Mittal, M.; Bansal, V.; Jain, R.; Dabla, P.K. Perturbing Status of Vitamin B12 in Indian Infants and Their Mothers. Food Nutr. Bull. 2017, 38, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Hay, G.; Clausen, T.; Whitelaw, A.; Trygg, K.; Johnston, C.; Henriksen, T.; Refsum, H. Maternal folate and cobalamin status predicts vitamin status in newborns and 6-month-old infants. J. Nutr. 2010, 140, 557–564. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | N (%) | Mean | SD |
|---|---|---|---|
| Age, months | 8.3 | 1.9 | |
| First born child | 151 (48) | ||
| Male child | 167 (53) | ||
| Home delivery | 15 (5) | ||
| Birth weight, gm 1 | 2813 | 482 | |
| Low birth weight (<2500 gm) | 52 (17) | ||
| Demographic features | |||
| Illiterate or up to grade 5 education of mother | 128 (41) | ||
| Illiterate or up to grade 5 education of father | 118 (37) | ||
| Not working mother or engaging only in agricultural work | 197 (62) | ||
| Mother’s age | 27.4 | 4.7 | |
| Family staying in own house | 161 (51) | ||
| Family staying in joint family | 159 (50) | ||
| Family having own land | 145 (46) | ||
| Breastfeeding status | |||
| Exclusive breastfeeding for 3 months or more 2 | 137 (43) | ||
| Exclusive breastfeeding for 6 months | 33 (10) | ||
| Nutritional status | |||
| Underweight (weight for age <−2 z-score) | 62 (19) | ||
| Stunting (length for age <−2 z-score) | 106 (33) | ||
| Wasting (weight for length <−2 z-score) | 13 (6) | ||
| Maternal undernutrition 3 | 34 (6) |
| Mean/Centile | Cobalamin (pmol/L) | Folate (nmol/L) | tHcy (µmol/L) | MMA (µmol/L) | 3cB12 | Hb (g/dL) |
|---|---|---|---|---|---|---|
| Mean (SD) | 304 (152) | 65 (23) | 12.1 (6.5) | 0.74 (0.86) | −0.70 (0.84) | 10.7 (0.9) |
| 5% | 124 | 33 | 5.6 | 0.15 | −2.2 | 9.4 |
| 25% | 201 | 48 | 7.8 | 0.27 | −1.2 | 10 |
| 50% | 272 | 62 | 10.3 | 0.48 | −0.64 | 10.6 |
| 75% | 364 | 77 | 14.2 | 0.83 | −0.13 | 11.4 |
| 95% | 601 | 112 | 24.8 | 2.43 | 0.62 | 12.3 |
| Definition | Cut off | Prevalence (95% CI) |
|---|---|---|
| Anemia | <11 gm/dL | 61% (55–66) |
| Altitude adjusted anemia | <11.3 gm/dL | 70% (65–75) |
| Cobalamin deficiency | <148 pmol/L | 11% (7–14) |
| Marginal cobalamin deficiency | 148–221 pmol/L | 24% (19–29) |
| Combined indicator of B12 (3cB12) 1 | <−0.5 | 58% (53–64) |
| Folate deficiency | <10 nmol/L | 0 |
| High total homocysteine 2 High methylmalonic acid2 | >10 µmol/L >0.28 µmol/L | 53% (47–58) 75% (70–79) |
| Independent Variables | Dependent Variables | |||
|---|---|---|---|---|
| 3cB12 | tHcy | MMA | Cobalamin | |
| Age of child (month) | 0.06(0.01, 0.11) | 0.93 (0.89, 0.96) | 0.99 (0.93, 1.06) | 1.05 (1.01, 1.10) |
| Family not staying in own house | −0.19 (−0.39, 0.01) | 1.17 (1.01, 1.36) | 1.43 (1.10, 1.85) | |
| Age of Mother (year) | 0.02(0.02, 0.04) | 0.98 (0.97, 0.99) | ||
| Father completed education ≤5 year | 0.22(0.03,0.41) | 0.85 (0.74, 0.98) | ||
| Excl. breastfeeding ≥ 3 months | 1.16 (1.01, 1.35) | |||
| Underweight (weight for age <−2 z-score) | 1.29 (1.07, 1.56) | |||
| Stunting (length for age <−2 z-score) | 1.47 (1.12, 1.93) | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandyo, R.K.; Ulak, M.; Kvestad, I.; Hysing, M.; Shrestha, M.; Ranjitkar, S.; Ulvik, A.; Ueland, P.M.; Shrestha, L.; Strand, T.A. Cobalamin and Folate Status among Breastfed Infants in Bhaktapur, Nepal. Nutrients 2018, 10, 639. https://doi.org/10.3390/nu10050639
Chandyo RK, Ulak M, Kvestad I, Hysing M, Shrestha M, Ranjitkar S, Ulvik A, Ueland PM, Shrestha L, Strand TA. Cobalamin and Folate Status among Breastfed Infants in Bhaktapur, Nepal. Nutrients. 2018; 10(5):639. https://doi.org/10.3390/nu10050639
Chicago/Turabian StyleChandyo, Ram K., Manjeswori Ulak, Ingrid Kvestad, Mari Hysing, Merina Shrestha, Suman Ranjitkar, Arve Ulvik, Per Magne Ueland, Laxman Shrestha, and Tor A. Strand. 2018. "Cobalamin and Folate Status among Breastfed Infants in Bhaktapur, Nepal" Nutrients 10, no. 5: 639. https://doi.org/10.3390/nu10050639