1. Introduction
Inadequate dietary zinc intake is widespread in the world’s population, especially in developing countries, where staple diets are predominantly plant-based, and consumption of animal source foods, such as red meat, poultry, and fish, is often modest because of economic, cultural, and religious constraints [
1]. At present, China, as the largest developing country, is experiencing critical changes in its nutrition and health along with its rapid economic development. The dietary structure and the population’s consumption of food, energy, and nutrients are changing significantly [
2]. Studies have showed that the intake of dietary zinc in Chinese households has decreased over the past decade [
3,
4,
5,
6,
7,
8], but few studies have examined Chinese dietary zinc intake in the last five years. Using the most recent data from 2015, we analyzed the dietary zinc intake of Chinese adults, assessed the prevalence of zinc deficiency, determined the main food sources of zinc, and examined the impact of the socioeconomic status on dietary zinc intake.
Zinc is a trace element essential to many metabolic processes and is important for growth and development, immunity, neurological functions, and reproduction [
9,
10,
11,
12]. It is present in many enzymes, such as alkaline phosphatase, copper/zinc superoxide dismutase, nitric oxide synthase, neutral endopeptidase, and angiotensin-I-converting enzyme [
13,
14]. In addition, studies have documented that zinc acts as an antioxidant, has membrane-stabilizing properties, blocks apoptotic cell death, and is essential for endothelial integrity [
15,
16]. Therefore, zinc plays a substantial role in the prevention of metabolic syndrome [
17], including atherogenic dyslipidemia, hyperglycemia, insulinemia, and elevated blood pressure, through the inhibition of proinflammatory cytokine expression, which suppresses reactive oxygen species (ROS) production, protecting against oxidative stress damage. In addition to ROS neutralization, zinc participates in glucose and lipid metabolism. Numerous studies have showed that zinc supplements improve blood pressure, glucose, and lipid levels. However, the results of previous studies on the association between zinc status and metabolic indicators are controversial [
18], as they used serum zinc concentrations derived from patient populations and experiments. Despite the clinical significance of zinc deficiency, there is no established method or biomarker to reliably evaluate the zinc status [
19], although serum zinc is widely used in most studies. To the best of our knowledge, few studies have addressed the relationship between dietary zinc intake and metabolic syndrome indicators in epidemiological studies. Accordingly, in addition to describing dietary zinc intake levels in Chinese adults, we examined the relationship between dietary zinc intake and metabolic indicators, including blood pressure, fasting glucose, and triglycerides (TG) in that population.
4. Discussion
This study found that, in 2015, the average dietary zinc intake of Chinese adults in 15 provinces was 10.2 mg/day, which is lower than the results from the China National Nutrition and Health Survey that measured 11.3 mg/day in 2002 and 10.7 mg/day in 2010–2012 [
24]. This study found that the average dietary zinc density was 5.2 mg/day per 1000 kcal, higher than the results from the China National Nutrition and Health Survey in 2002 (5.1–5.2 mg/day per 1000 kcal in urban residents and 4.7–4.8 mg/day per 1000 kcal in rural residents) [
25]. The comparison of the above results suggests that, over time, up to 2015, Chinese dietary zinc intake was on a declining trend and Chinese dietary zinc density was on the rise. Our study found that 31.0% of Chinese adults consumed the dietary zinc at a level <EAR, which was slightly lower than the 35.6% from the China National Nutrition and Health Survey in 2010–2012 [
8]. Our results indicate that the dietary zinc intake of nearly half of the male population was <EAR. In contrast, the dietary zinc intake of women was better, with 85.2% of women reaching the EAR, and 67.0% reaching the RNI.
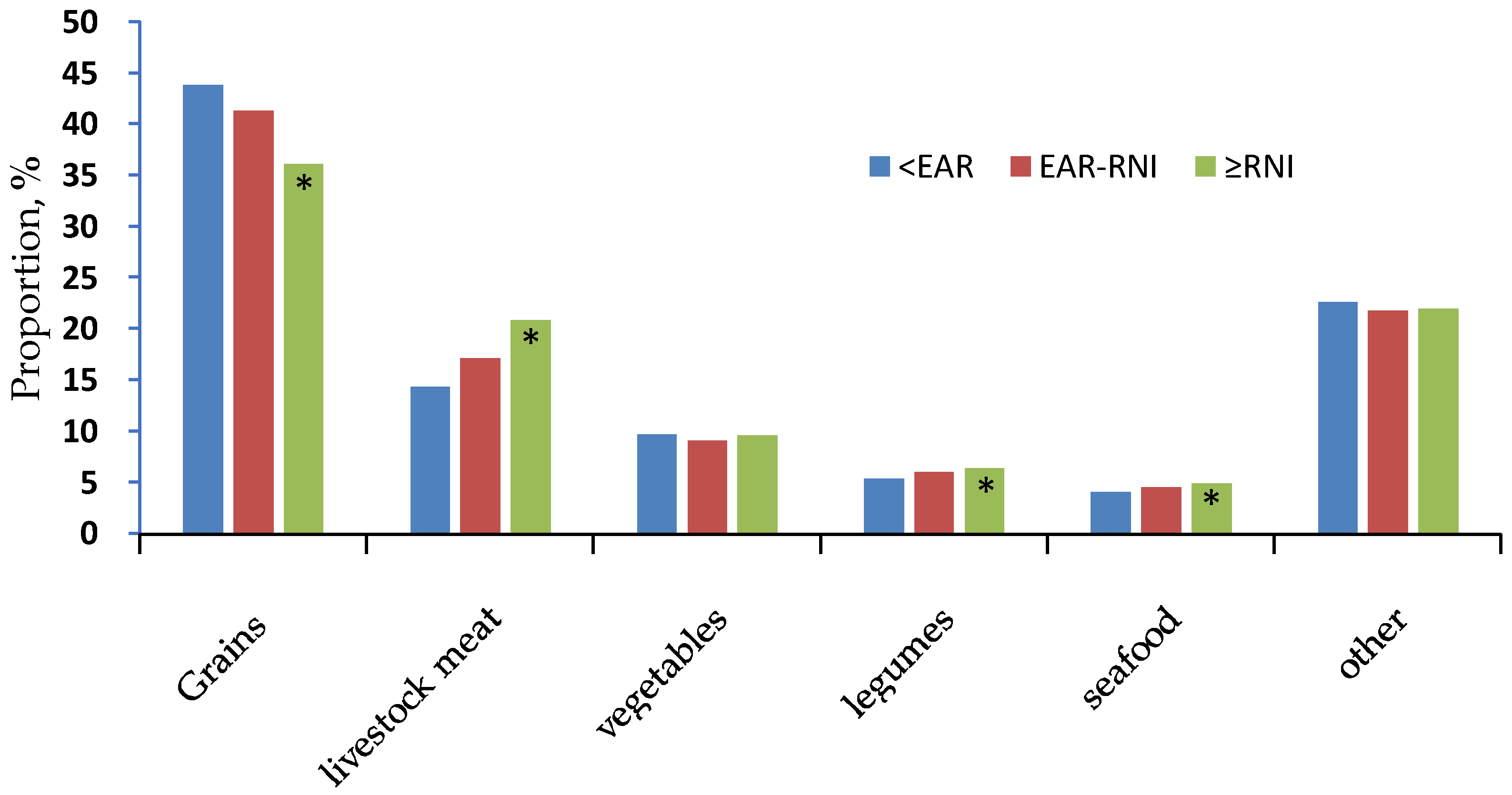
In the past decade or so, China’s food structure has changed greatly. Consumption of grains, vegetables, and other plants has decreased, and consumption of animal source foods, such as livestock and poultry, has significantly increased [
26]. In 2002, 51.9% of dietary zinc was from grains, and 13.5% was from meat [
7]. By 2015, the consumption of grains had decreased by 13.1%, the consumption of meat had increased by 5.2%, and the average intake of dietary zinc had decreased. The reason may be related to the changes in food sources in the past 10 years. Meat consumption did not increase as much as grain consumption decreased, which might have improved dietary zinc density. However, the Chinese total food and energy intake was on the decline [
8], so zinc intake showed a downward trend.
Gender, age, education, income, region, and area differences may affect the dietary zinc intake. Men consumed more zinc than women. Since we found no difference in dietary zinc density between the genders, the dietary zinc intake differed from the total energy intake. The dietary zinc intake in the 50–64 age group was lower than in the 18–49 age group, possibly because of the lower dietary zinc density and total energy intake in the 50–64 group. Education, income, and regional development might have positive effects on dietary zinc intake. Higher levels of education, income, and regional development corresponded to higher dietary zinc intakes and higher zinc densities, but the study also found that the highest levels of zinc density were in the least developed western region. This result might be related to the higher meat consumption in that region, where 30.4% of dietary zinc intake was from livestock meat.
The zinc intake differences reflect the rates of dietary zinc deficiency. The higher the dietary zinc intake, the higher the rate of meeting the EAR and the RNI. The Chinese zinc evaluation standards for males and females are not the same, so although the mean value showed a difference of only 1.8 mg/day between the genders, we found a huge gap in the rates of dietary zinc deficiency. Only 14.8% of women did not reach the EAR, while nearly half of men did not reach it. In addition, 67.0% of women reached the RNI, while only 30.7% of men reached it, less than half the rate for women.
Food sources affected dietary zinc intake. As dietary zinc intake increased, the proportion of grain intake decreased, and the proportion of meat intake increased significantly. Therefore lower grain and higher livestock meat consumption characterizes a relatively good dietary zinc status for adults in China.
In comparison, in the United States, an economically developed country, the dietary zinc intakes for males and females over the age of 19 were 14.2 and 9.8 mg/day, respectively, in NHANES 2009–2010, and the rates of zinc deficiency were 11.0% and 17.0% for males and females, respectively, in HNANES 2001–2002 [
27]. Chinese women’s zinc intakes and inadequacies in this study were comparable to those of American women, but Chinese men’s zinc intakes and inadequacies in this study were far from those of American men. The top three food sources of dietary zinc in the United States in HNANES 2003–2006 were meats, grains, and dairy products, accounting for 35.0%, 15.0%, and 13.0%, respectively [
28,
29,
30]. The rough proportions of dietary zinc from grains and meats in China in this study were just the opposite, and dairy was a big difference. China’s dairy intake was low, so dairy products were not an important source of zinc. Although the average dietary zinc intake in China was lower than that in the United States, it was comparable to those in Canada [
31] and New Zealand [
32] and higher than those in the United Kingdom [
33,
34] and Chile [
35]. However, the adequacy of zinc intake depends not only on the amount of zinc but also on its bioavailability. People consuming a diet that provides marginal zinc may not absorb an adequate amount of zinc if they also consume foods high in phytates. The average phytate intake for people in China (1186 mg/day) [
22,
36] was higher than that in western countries, possibly because of the higher consumption of grains and lower consumption of meats and dairy products in China. Although Chinese dietary zinc intake was comparable with that of some western countries, Chinese dietary zinc absorption was not necessarily the same. By the way, it seems that the proportion of foods high in phytate was more prevalent in rural regions, where the zinc intake was also lower. This would mean that bioavailability was particularly low in the geographic population with the lowest intake, which may aggravate the problem of zinc deficiency in these areas.
Zinc is highly significant in the pathogenesis of metabolic syndrome, which suggests that zinc supplementation would have a positive effect in reducing metabolic syndrome. However, the results of previous studies on the association between zinc and metabolic indicators are controversial. For example, it has been reported that zinc may participate in blood pressure regulation and in the pathogenesis of hypertension [
37]. Inverse relationships between blood pressure and dietary zinc and serum zinc concentration have been documented in hypertensive subjects [
38,
39], but some studies have reported that zinc does not change the blood pressure in rats [
40,
41] or humans [
42]. It also has been suggested that zinc deficiency may be an important risk factor for type 2 diabetes mellitus [
43]. Several studies have observed a decreased concentration of zinc in diabetic patients compared to healthy people [
44,
45,
46,
47,
48,
49,
50,
51], and others have noticed a relation between inadequate zinc intake and raised insulin concentrations in blood in adolescents [
52]. Some recent studies showed that zinc supplementation improved glucose metabolism and insulin sensitivity in diabetic patients [
53,
54,
55,
56,
57]. However, other studies did not confirm the association between zinc and glucose metabolism and insulin resistance [
58,
59]. Numerous studies have indicated an association between serum zinc levels and lipid metabolism [
60]. Clinical and experimental studies have reported that zinc supplementation decreased total cholesterol, low-density lipoprotein cholesterol, and TG and increased high-density lipoprotein cholesterol [
53,
61]. In other studies, zinc deficiency exacerbated hepatic lipid metabolism, while zinc supplementation increased hepatocyte activity and improved lipid metabolism in the liver [
62,
63]. By contrast, E. Weigand and J. Egenolf [
64] have showed that moderate zinc deficiency did not alter lipid concentration and fatty acid composition in the livers of rats fed a high-fat diet. Moreover, short-term zinc supplementation in obese patients decreased weight and TG levels without significant changes in lipid and glucose profiles [
58,
65,
66], and, elsewhere, serum zinc levels in men were positively associated with elevated TG [
67].
In contrast with most of the above results, where the association of serum zinc status with metabolic syndrome were based on experimental or patient studies, our study emphasizes the effects of dietary zinc intake on metabolic syndrome indicators based on a health cohort. For females, the group with adequate dietary zinc intake (≥RNI) showed lower diastolic blood pressure and fasting glucose than the reference group (<EAR). Our systolic blood pressure difference was not statistically significant, although the results from a study showed that dietary zinc intake was inversely associated with systolic blood pressure in young obese Korean women [
68]. For males and females, the dietary zinc intake was positively associated with TG. Our study demonstrates that adequate dietary zinc intake was associated with reduced diastolic blood pressure and fasting glucose levels. However, we saw a rise in TG in the groups with adequate dietary zinc intakes, which seemed inconsistent with the improvement in lipid metabolism. The relationship between dietary zinc intake and serum zinc concentration was inconsistent because of high heterogeneity [
69], and the improvement in lipid metabolism was contradictory. Nevertheless, this study found that adequate dietary zinc was associated with reduced blood pressure and fasting glucose, as did previous studies of serum zinc levels. Further studies should investigate the role of serum zinc and urine zinc concentrations on metabolic syndrome, and further studies of gender-specific influences are needed to evaluate the effects of dietary zinc intake on metabolic syndrome.
This study has several limitations. The three-day, 24 h food intake recall may not reflect long-term dietary habits. Eating out is another source of potential measurement errors [
70]. Another limitation is that the study did not take into account zinc from dietary supplements. As the use of dietary supplements is less widespread in China (10.3% in urban residents, 2.9% in rural residents) [
71] than in the United States (39.5% overall) [
72], we assumed that our underestimation of zinc intake was small. Although we excluded patients affected by hypertension, diabetes, and cardiovascular diseases from the data collected by questionnaires, the questionnaires could not rule out undetected participant with metabolic disease which might have caused minor errors.


 ,
, 

{kind=link}