Association between Vegetable Consumption and Blood Pressure, Stratified by BMI, among Chinese Adolescents Aged 13–17 Years: A National Cross-Sectional Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
2.3. Physical Examination
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of Participants
3.2. Association between Vegetable Consumption and BP z Score
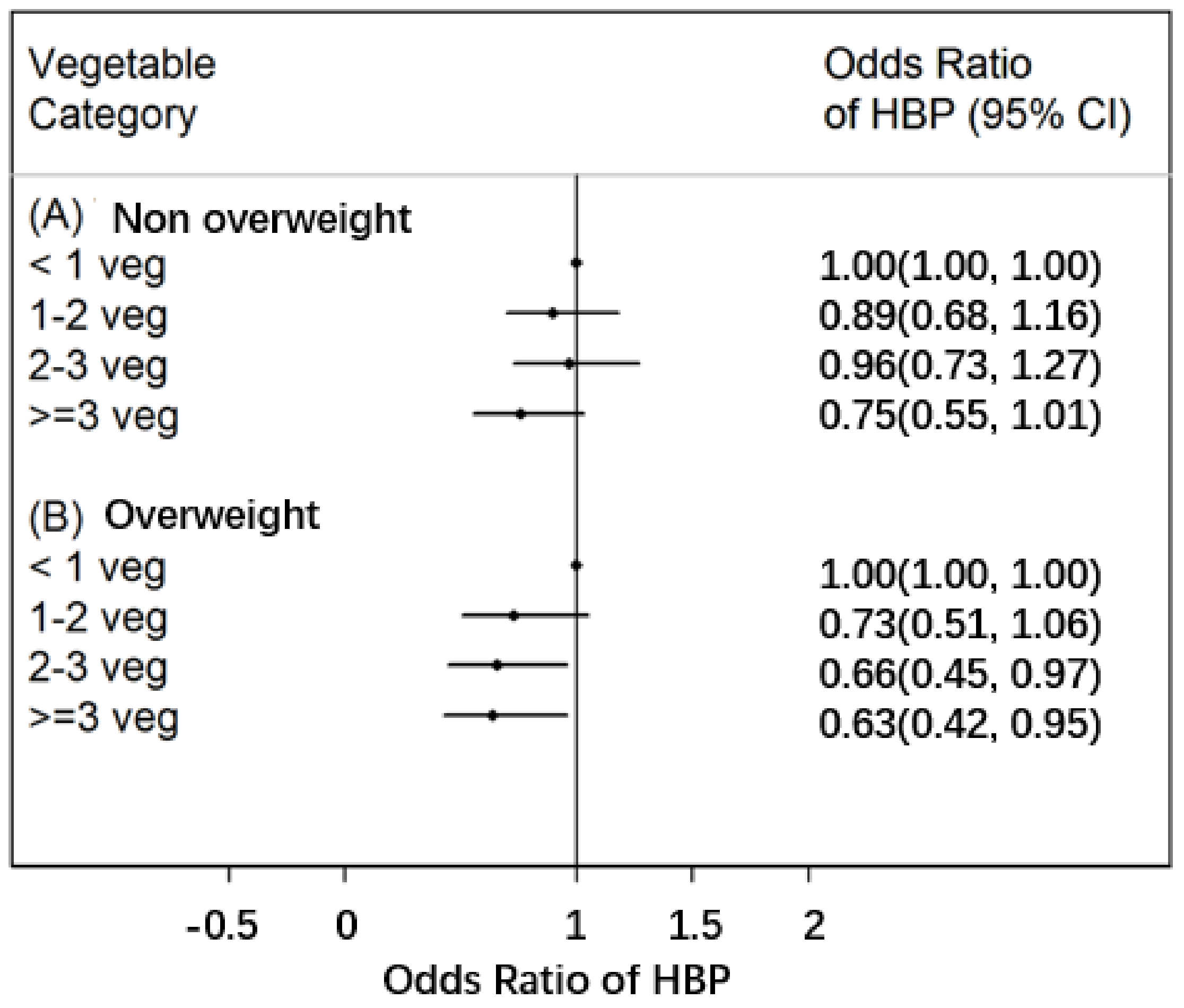
3.3. Risk of High BP in Adolescents in Various BMI Groups and Vegetable Consumption Groups
4. Discussion
4.1. Vegetable Consumption in Adolescents
4.2. Association between Vegetable Consumption and HBP in Adolescents
4.3. Implications
4.4. Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of interest
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Chen, X.; Wang, Y. Tracking of blood pressure from childhood to adulthood: A systematic review and meta-regression analysis. Circulation 2008, 117, 3171–3180. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Wu, Y.; Feng, X.X.; Ma, J.; Ma, Y.; Wang, H.; Zhang, J.; Yuan, J.; Lin, C.P.; Nowson, C.; et al. School based education programme to reduce salt intake in children and their families (School-EduSalt): Cluster randomised controlled trial. BMJ 2015, 350, h770. [Google Scholar] [CrossRef] [PubMed]
- Utsugi, M.T.; Ohkubo, T.; Kikuya, M.; Kurimoto, A.; Sato, R.I.; Suzuki, K.; Metoki, H.; Hara, A.; Tsubono, Y.; Imai, Y. Fruit and vegetable consumption and the risk of hypertension determined by self measurement of blood pressure at home: The Ohasama study. Hypertens. Res. 2008, 31, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Zhan, J.; Liu, Y.J.; Cai, L.B.; Xu, F.R.; Xie, T.; He, Q.Q. Fruit and vegetable consumption and risk of cardiovascular disease: A meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 1650–1663. [Google Scholar] [CrossRef] [PubMed]
- Collese, T.S.; Nascimento-Ferreira, M.V.; de Moraes, A.C.F.; Rendo-Urteaga, T.; Bel-Serrat, S.; Moreno, L.A.; Carvalho, H.B. Role of fruits and vegetables in adolescent cardiovascular health: A systematic review. Nutr. Rev. 2017, 75, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Mellendick, K.; Shanahan, L.; Wideman, L.; Calkins, S.; Keane, S.; Lovelady, C. Diets rich in fruits and vegetables are associated with lower cardiovascular disease risk in adolescents. Nutrients 2018, 10, 136. [Google Scholar] [CrossRef] [PubMed]
- Damasceno, M.M.; de Araujo, M.F.; de Freitas, R.W.; de Almeida, P.C.; Zanetti, M.L. The association between blood pressure in adolescents and the consumption of fruits, vegetables and fruit juice—An exploratory study. J. Clin. Nurs. 2011, 20, 1553–1560. [Google Scholar] [CrossRef] [PubMed]
- Mahfouz, A.A.; Shatoor, A.S.; Hassanein, M.A.; Mohamed, A.; Farheen, A. Gender differences in cardiovascular risk factors among adolescents in Aseer Region, southwestern Saudi Arabia. J. Saudi Heart Assoc. 2012, 24, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Krupp, D.; Remer, T. Salt, fruit and vegetable consumption and blood pressure development: A longitudinal investigation in healthy children. Br. J. Nutr. 2014, 111, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Danese, E.; Montagnana, M.; Fava, C. Searching for genes involved in hypertension development in special populations: Children and pre-eclamptic women. Where are we standing now? Clin. Chem. Lab. Med. 2013, 51, 2253–2269. [Google Scholar] [CrossRef] [PubMed]
- Chinese Nutrition Society. Dietary Guidelines for Chinese; People’s Medical Publishing House: Beijing, China, 2016. [Google Scholar]
- Dong, Y.H.; Zou, Z.Y.; Yang, Z.P.; Wang, Z.H.; Jing, J.; Luo, J.Y.; Zhang, X.; Luo, C.Y.; Wang, H.; Zhao, H.P.; et al. Association between high birth weight and hypertension in children and adolescents: A cross-sectional study in China. J. Hum. Hypertens. 2017, 31, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Song, J.Y.; Song, Q.Y.; Wang, S.; Ma, J.; Wang, H.J. Physical activity and sedentary behaviors modify the association between melanocortin 4 receptor gene variant and obesity in Chinese children and adolescents. PLoS ONE 2017, 12, e0170062. [Google Scholar] [CrossRef] [PubMed]
- Plawecki, K.L.; Evans, E.M.; Mojtahedi, M.C.; McAuley, E.; Chapman-Novakofski, K. Assessing calcium intake in postmenopausal women. Prev. Chronic Dis. 2009, 6, A124. [Google Scholar] [PubMed]
- Zou, Z.Y.; Yang, Y.D.; Wang, S.; Dong, B.; Li, X.H.; Ma, J. The importance of blood lipids in the association between BMI and blood pressure among Chinese overweight and obese children. Br. J. Nutr. 2016, 116, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Dong, B.; Wang, S.; Dong, Y.; Zou, Z.; Fu, L.; Ma, J. Prevalence of high blood pressure subtypes and its associations with BMI in Chinese children: A national cross-sectional survey. BMC Public Health 2017, 17, 598. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.Y. Working group on obesity in China. Report on childhood obesity in China (1)—Body mass index reference for screening overweight and obesity in Chinese school-age children. Biomed. Environ. Sci. 2005, 18, 390–400. [Google Scholar] [PubMed]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar]
- Epstein, L.H.; Gordy, C.C.; Raynor, H.A.; Beddome, M.; Kilanowski, C.K.; Paluch, R. Increasing fruit and vegetable intake and decreasing fat and sugar intake in families at risk for childhood obesity. Obes. Res. 2001, 9, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Pengpid, S. Fruits and vegetables consumption and associated factors among in-school adolescents in five Southeast Asian countries. Int. J. Environ. Res. Public Health 2012, 9, 3575–3587. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.A.; Piaseu, N. Prevalence and determinants of sufficient fruit and vegetable consumption among primary school children in Nakhon Pathom, Thailand. Nutr. Res. Pract. 2017, 11, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Krupp, D.; Shi, L.; Egert, S.; Wudy, S.A.; Remer, T. Prospective relevance of fruit and vegetable consumption and salt intake during adolescence for blood pressure in young adulthood. Eur. J. Nutr. 2015, 54, 1269–1279. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Bentley, M.E.; Zhai, F.; Popkin, B.M. Tracking of dietary intake patterns of Chinese from childhood to adolescence over a six-year follow-up period. J. Nutr. 2002, 132, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Fasting, M.H.; Nilsen, T.I.; Holmen, T.L.; Vik, T. Life style related to blood pressure and body weight in adolescence: Cross sectional data from the Young-HUNT study, Norway. BMC Public Health 2008, 8, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, H.; Li, L.; Bennett, D.; Guo, Y.; Key, T.J.; Bian, Z.; Sherliker, P.; Gao, H.; Chen, Y.; Yang, L.; et al. Fresh fruit consumption and major cardiovascular disease in China. N. Engl. J. Med. 2016, 374, 1332–1343. [Google Scholar] [CrossRef] [PubMed]
- Couch, S.C.; Saelens, B.E.; Levin, L.; Dart, K.; Falciglia, G.; Daniels, S.R. The efficacy of a clinic-based behavioral nutrition intervention emphasizing a DASH-type diet for adolescents with elevated blood pressure. J. Pediatr. 2008, 152, 494–501. [Google Scholar] [CrossRef] [PubMed]
- John, J.H.; Ziebland, S.; Yudkin, P.; Roe, L.S.; Neil, H.A. Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: A randomised controlled trial. Lancet 2002, 359, 1969–1974. [Google Scholar] [CrossRef]
- Dauchet, L.; Amouyel, P.; Hercberg, S.; Dallongeville, J. Fruit and vegetable consumption and risk of coronary heart disease: A meta-analysis of cohort studies. J. Nutr. 2006, 136, 2588–2593. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Vegetable Consumption Group | p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| <1 Servings/Day | 1~2 Servings/Day | 2~3 Servings/Day | ≥3 Servings/Day | Total | |||||||
| n | Freq/Median | n | Freq/Median | n | Freq/Median | n | Freq/Median | n | Freq/Median | ||
| N | 2285 | 12.20% | 7136 | 38.00% | 5377 | 28.70% | 3959 | 21.10% | 18,757 | 100.00% | |
| Sex | |||||||||||
| Boys | 1101 | 48.20% | 3443 | 48.20% | 2577 | 47.90% | 2067 | 52.20% | 9188 | 49.00% | <0.001 |
| Girls | 1184 | 51.80% | 3693 | 51.80% | 2800 | 52.10% | 1892 | 47.80% | 9569 | 51.00% | |
| Age, years | 2285 | 15 (13,16) | 7136 | 15 (13,16) | 5377 | 15 (13,16) | 3959 | 15 (13,16) | 18,757 | 15 (13,16) | <0.001 |
| Height (cm) | 2285 | 161.9 (156.9,168.3) | 7136 | 162.5 (157.2,169) | 5377 | 162.5 (157.3,169.1) | 3959 | 163.1 (157.9,169.4) | 18,757 | 162.6 (157.3,169) | <0.001 |
| Weight (kg) | 2285 | 52.2 (46.7,59.7) | 7136 | 53 (47,60.3) | 5377 | 53 (46.7,61) | 3959 | 53 (46.6,61.4) | 18,757 | 52.9 (46.9,60.6) | 0.083 |
| BMI (kg/m2) | 2285 | 19.8 (18.0,22.0) | 7136 | 19.8 (18.2,22.1) | 5377 | 19.8 (18.1,22.3) | 3959 | 19.7 (17.9,22.3) | 18,757 | 19.8 (18.1,22.2) | 0.283 |
| SBP (mmHg) | 2285 | 110 (101,118) | 7136 | 110 (100,120) | 5377 | 110 (100,119) | 3959 | 110 (100,119) | 18,757 | 110 (100,119) | 0.385 |
| DBP (mmHg) | 2285 | 70 (62,74) | 7136 | 70 (62,73) | 5377 | 70 (62,74) | 3959 | 70 (61,73) | 18,757 | 70 (62,73) | 0.009 |
| HBP group | 0.521 | ||||||||||
| Non-HBP | 2130 | 93.20% | 6711 | 94.00% | 5039 | 93.70% | 3719 | 93.90% | 17,599 | 93.80% | |
| HBP | 155 | 6.80% | 425 | 6.00% | 338 | 6.30% | 240 | 6.10% | 1158 | 6.20% | |
| Fruit intake (serving/day) | |||||||||||
| <1 | 1134 | 50.80% | 1913 | 27.10% | 1031 | 19.40% | 549 | 14.00% | 4627 | 25.00% | <0.001 |
| 1~2 | 778 | 34.80% | 3933 | 55.80% | 2803 | 52.70% | 1614 | 41.20% | 9128 | 49.30% | |
| 2~3 | 231 | 10.30% | 925 | 13.10% | 1111 | 20.90% | 1003 | 25.60% | 3270 | 17.70% | |
| ≥3 | 90 | 4.00% | 283 | 4.00% | 378 | 7.10% | 749 | 19.10% | 1500 | 8.10% | |
| BMI groups | |||||||||||
| Non-overweight | 1910 | 83.60% | 5969 | 83.60% | 4418 | 82.20% | 3201 | 80.90% | 15,498 | 82.60% | 0.001 |
| Overweight | 375 | 16.40% | 1167 | 16.40% | 959 | 17.80% | 758 | 19.10% | 3259 | 17.40% | |
| Physical activity (hour/day) | |||||||||||
| <1 | 925 | 41.40% | 2911 | 41.60% | 1897 | 35.90% | 1200 | 31.00% | 6933 | 37.70% | <0.001 |
| 1~2 | 719 | 32.20% | 2259 | 32.30% | 2006 | 37.90% | 1400 | 36.10% | 6384 | 34.70% | |
| 2~4 | 286 | 12.80% | 939 | 13.40% | 719 | 13.60% | 678 | 17.50% | 2622 | 14.20% | |
| ≥4 | 101 | 4.50% | 371 | 5.30% | 340 | 6.40% | 354 | 9.10% | 1166 | 6.30% | |
| not sure | 205 | 9.20% | 521 | 7.40% | 326 | 6.20% | 245 | 6.30% | 1297 | 7.00% | |
| Smoking | |||||||||||
| No | 2201 | 98.6% | 6917 | 99.1% | 5209 | 99.0% | 3841 | 98.8% | 18,168 | 99.0% | 0.069 |
| Yes | 32 | 1.4% | 60 | 0.9% | 50 | 1.0% | 47 | 1.2% | 189 | 1.0% | |
| Alcohol intake | |||||||||||
| No | 2094 | 93.7% | 6672 | 95.7% | 5005 | 95.4% | 3686 | 95.0% | 17,457 | 95.2% | 0.002 |
| Yes | 140 | 6.3% | 302 | 4.3% | 242 | 4.6% | 192 | 5.0% | 876 | 4.8% | |
| BMI groups | BP(mmHg) | Model | Coefficient | SE | p |
|---|---|---|---|---|---|
| Total | SBP z score | Crude model | −0.012 | 0.005 | 0.015 |
| Adjusted model | −0.018 | 0.005 | <0.001 | ||
| DBP z score | Crude model | −0.005 | 0.003 | 0.132 | |
| Adjusted model | −0.009 | 0.004 | 0.018 | ||
| Non-overweight | SBP z score | Crude model | −0.015 | 0.005 | 0.004 |
| Adjusted model | −0.016 | 0.006 | 0.003 | ||
| DBP z score | Crude model | −0.007 | 0.004 | 0.082 | |
| Adjusted model | −0.008 | 0.004 | 0.041 | ||
| Overweight | SBP z score | Crude model | −0.023 | 0.012 | 0.049 |
| Adjusted model | −0.027 | 0.012 | 0.029 | ||
| DBP z score | Crude model | −0.011 | 0.008 | 0.185 | |
| Adjusted model | −0.012 | 0.009 | 0.154 |
| Vegetable Consumption | non-HBP | HBP | OR * | p | ||
|---|---|---|---|---|---|---|
| n | Freq (%) | n | Freq (%) | |||
| <1 serving/day | 2130 | 12.10 | 155 | 13.39 | 1 (ref) | |
| 1–2 servings/day | 6711 | 38.13 | 425 | 36.70 | 0.85 (0.69–1.05) | 0.132 |
| 2–3 servings/day | 5039 | 28.63 | 338 | 29.19 | 0.86 (0.69–1.07) | 0.180 |
| ≥3 servings/day | 3719 | 21.13 | 240 | 20.73 | 0.73 (0.57–0.93) | 0.009 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Dong, B.; Zou, Z.; Wang, S.; Dong, Y.; Wang, Z.; Ma, J. Association between Vegetable Consumption and Blood Pressure, Stratified by BMI, among Chinese Adolescents Aged 13–17 Years: A National Cross-Sectional Study. Nutrients 2018, 10, 451. https://doi.org/10.3390/nu10040451
Yang Y, Dong B, Zou Z, Wang S, Dong Y, Wang Z, Ma J. Association between Vegetable Consumption and Blood Pressure, Stratified by BMI, among Chinese Adolescents Aged 13–17 Years: A National Cross-Sectional Study. Nutrients. 2018; 10(4):451. https://doi.org/10.3390/nu10040451
Chicago/Turabian StyleYang, Yide, Bin Dong, Zhiyong Zou, Shuo Wang, Yanhui Dong, Zhenghe Wang, and Jun Ma. 2018. "Association between Vegetable Consumption and Blood Pressure, Stratified by BMI, among Chinese Adolescents Aged 13–17 Years: A National Cross-Sectional Study" Nutrients 10, no. 4: 451. https://doi.org/10.3390/nu10040451