Vitamin D and Calcium Addition during Denosumab Therapy over a Period of Four Years Significantly Improves Lumbar Bone Mineral Density in Japanese Osteoporosis Patients


Abstract
:1. Introduction
2. Patients and Methods
3. Results
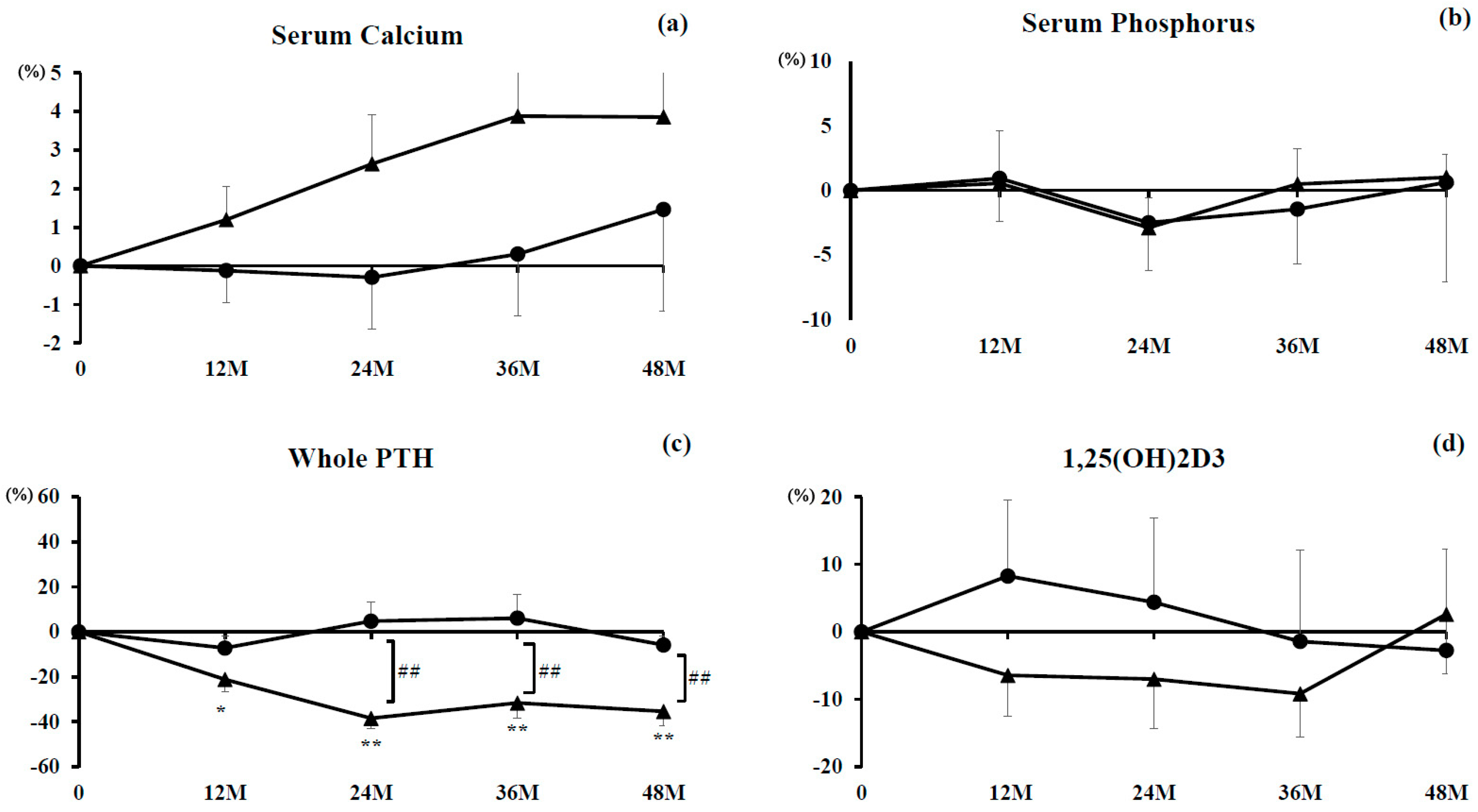
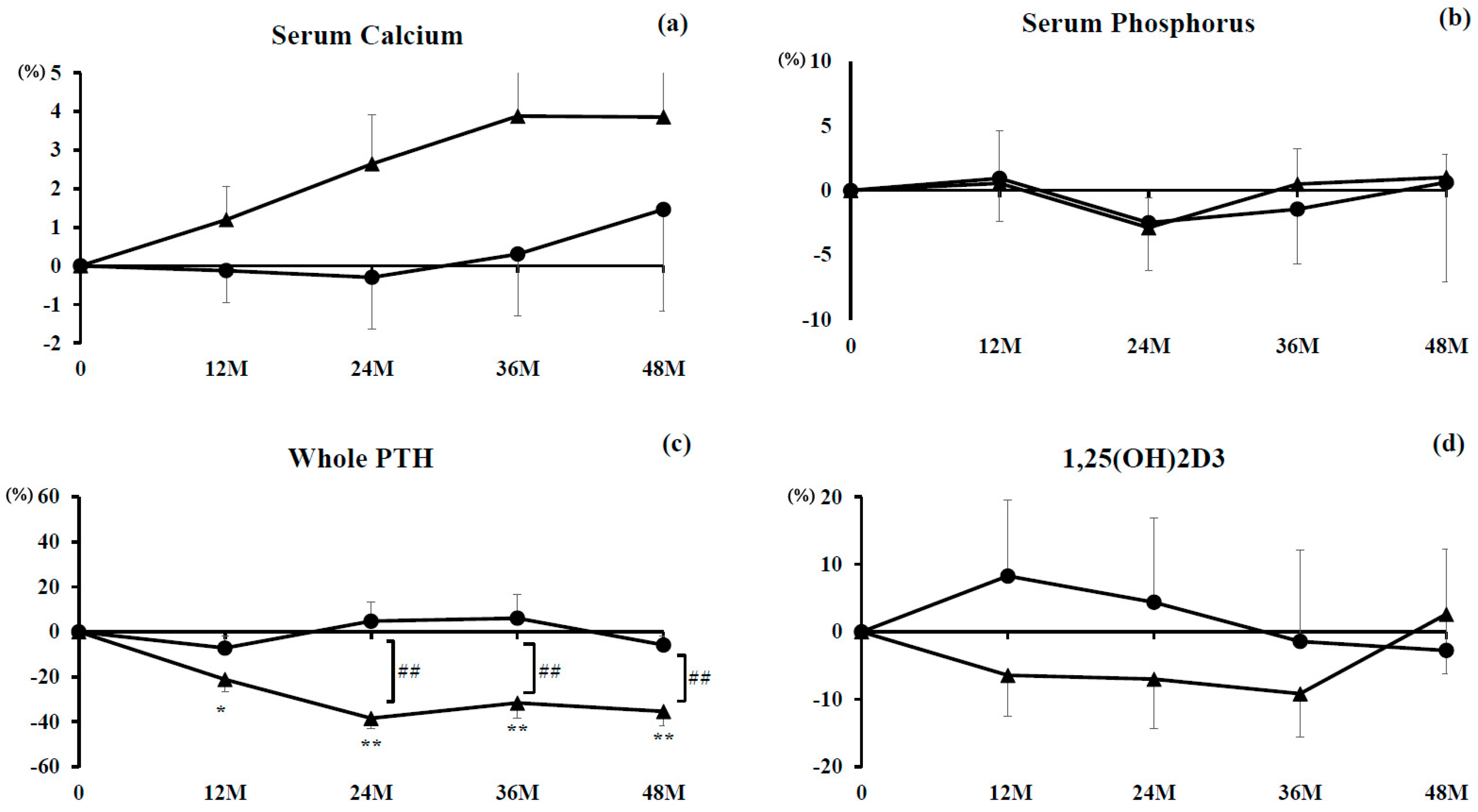
3.1. Serum Albumin-Corrected Concentrations of Calcium, Phosphorus, Whole PTH, and 1,25(OH)2D3
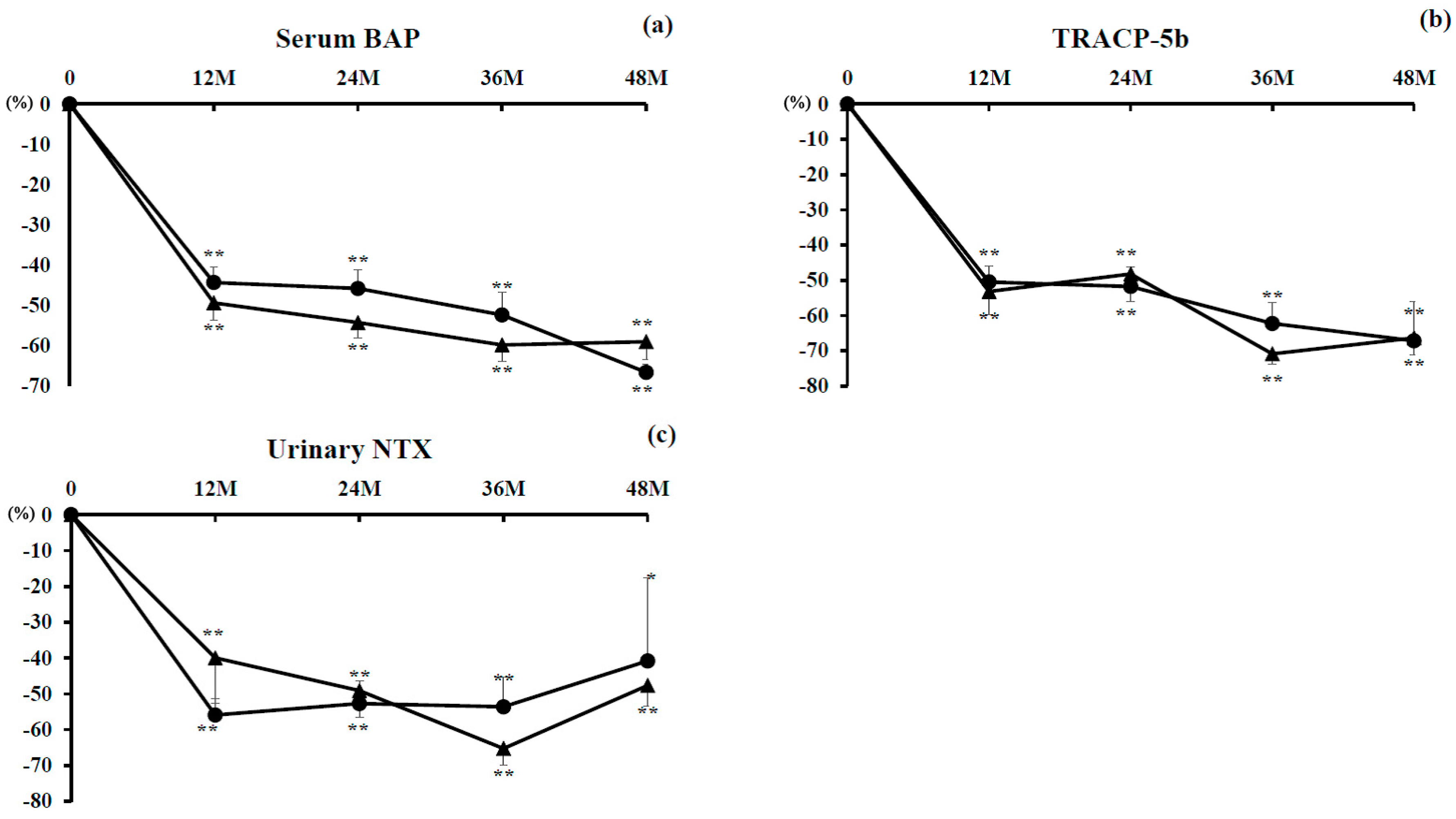
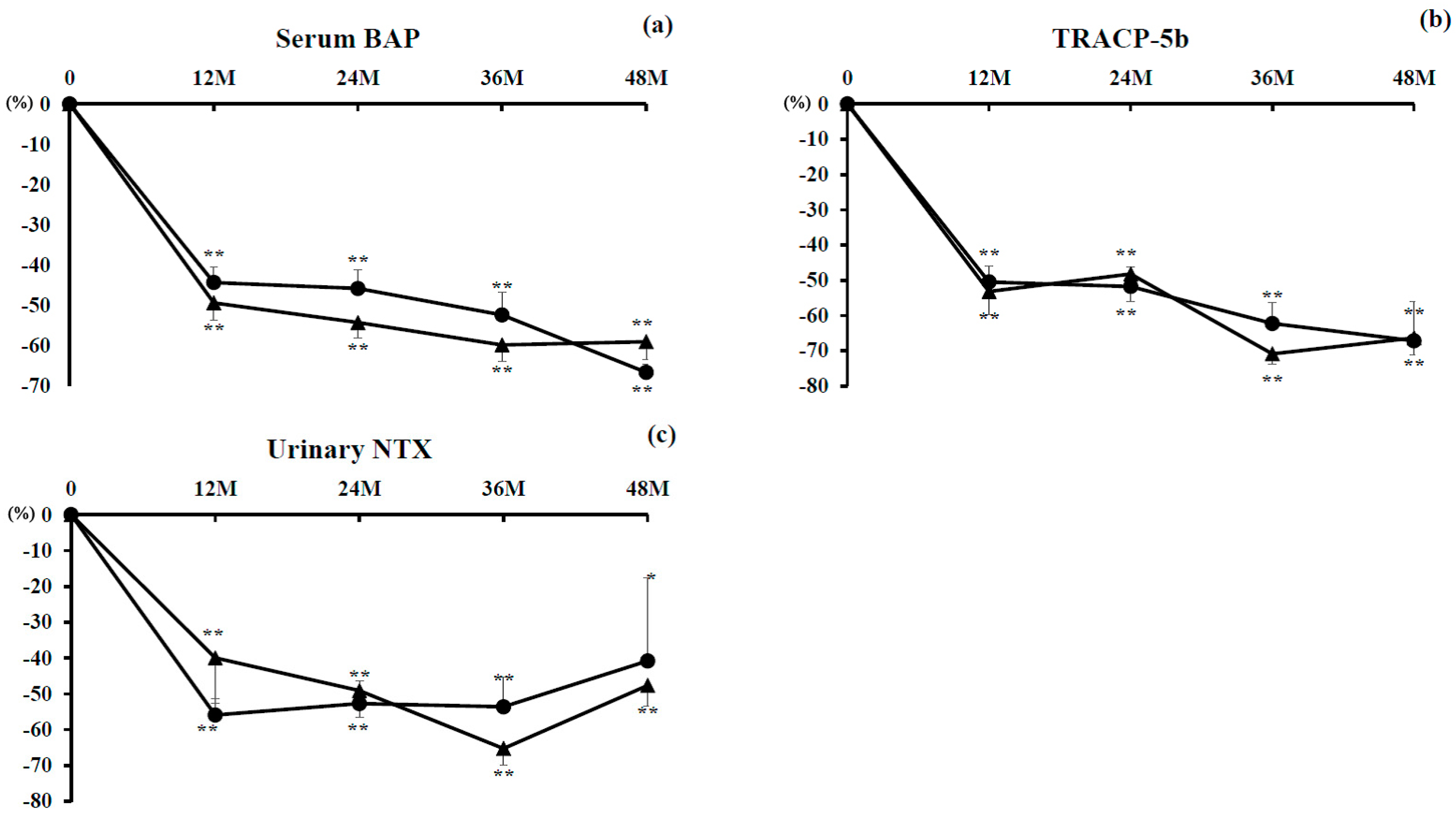
3.2. Markers of Bone Turnover
3.2.1. Marker of Bone Formation
3.2.2. Markers of Bone Resorption
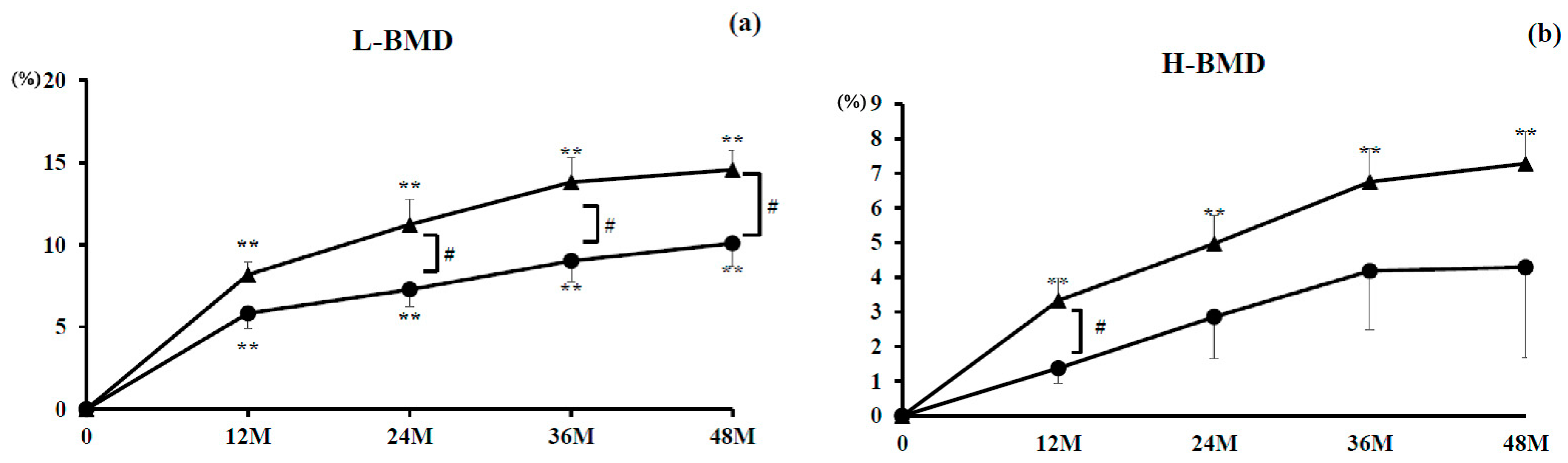
3.2.3. L-BMD and H-BMD
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Clarke, B.L.; Harris, S.T.; Hurley, D.L.; Kleerekoper, M.; Lewiecki, E.M.; Miller, P.D.; Narula, H.S.; et al. American association of clinical endocrinologists and American college of endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis-2016. Endocr. Pract. 2016, 22, 1–42. [Google Scholar] [CrossRef] [PubMed]
- McClung, M.R.; Lewiecki, E.M.; Cohen, S.B.; Bolognese, M.A.; Woodson, G.C.; Moffett, A.H.; Peacock, M.; Miller, P.D.; Lederman, S.N.; Chesnut, C.H.; et al. Denosumab in postmenopausal women with low bone mineral density. N. Engl. J. Med. 2006, 354, 821–831. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.; Branco, J.C. Denosumab: recent update in postmenopausal osteoporosis. Acta Reumatol. Port. 2012, 37, 302–313. [Google Scholar] [PubMed]
- Uehara, M.; Nakamura, Y.; Takahashi, J.; Kamimura, M.; Ikegami, S.; Suzuki, T.; Uchiyama, S.; Yamaguchi, T.; Kosho, T.; Kato, H. Efficacy of denosumab for osteoporosis in three female patients with osteogenesis imperfecta. Tohoku J. Exp. Med. 2017, 242, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Isobe, F.; Nakamura, Y.; Suzuki, T.; Kato, H. Effects of denosumab on osteoporosis in three cases with anorexia nervosa and a review of the literature. Mod. Rheumatol. Case Rep. 2017, 2, 104–116. [Google Scholar] [CrossRef]
- Kumaki, D.; Nakamura, Y.; Sakai, N.; Kosho, T.; Nakamura, A.; Hirabayashi, S.; Suzuki, T.; Kamimura, M.; Kato, H. Efficacy of denosumab for glucocorticoid-induced osteoporosis with duchenne muscular dystrophy. JBJS Case Connect. 2018, in press. [Google Scholar]
- Nakamura, Y.; Kamimura, M.; Ikegami, S.; Mukaiyama, K.; Uchiyama, S.; Taguchi, A.; Kato, H. Changes in serum vitamin D and PTH values using denosumab with or without bisphosphonate pre-treatment in osteoporotic patients: a short-term study. BMC Endocr. Disord. 2015, 15, 81. [Google Scholar] [CrossRef] [PubMed]
- Kamimura, M.; Nakamura, Y.; Ikegami, S.; Uchiyama, S.; Kato, H.; Taguchi, A. Significant improvement of bone mineral density and bone turnover markers by denosumab therapy in bisphosphonate-unresponsive patients. Osteoporos Int. 2017, 28, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Suzuki, T.; Kamimura, M.; Murakami, K.; Ikegami, S.; Uchiyama, S.; Kato, H. Vitamin D and calcium are required at the time of denosumab administration during osteoporosis treatment. Bone Res. 2017, 5, 17021. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Nakamura, Y.; Kato, H. Significant improvement of bone mineral density by denosumab without bisphosphonate pre-treatment in glucocorticoid-induced osteoporosis. Mod. Rheumatol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Ebina, K.; Kashii, M.; Hirao, M.; Hashimoto, J.; Noguchi, T.; Koizumi, K.; Kitaguchi, K.; Matsuoka, H.; Iwahashi, T.; Tsukamoto, Y.; et al. Comparison of the effects of denosumab between a native vitamin D combination and an active vitamin D combination in patients with postmenopausal osteoporosis. J. Bone Miner. Metab. 2017, 35, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Nakamura, Y.; Tanaka, M.; Kamimura, M.; Ikegami, S.; Uchiyama, S.; Kato, H. Comparison of the effects of denosumab with either active vitamin D or native vitamin D on bone mineral density and bone turnover markers in postmenopausal osteoporosis. Mod. Rheumatol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Nakamura, Y.; Kamimura, M.; Ikegami, S.; Uchiyama, S.; Kato, H. Compliance and discontinuation of denosumab treatment in postmenopausal Japanese women with primary osteoporosis or rheumatoid arthritis and osteoporosis. Osteoporos. Sarcopenia 2017, 3, 108–111. [Google Scholar] [CrossRef]
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689S–1696S. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Okamura, W.H.; Norman, A.W. Structure-function relationships in the vitamin D endocrine system. Endocr Rev. 1995, 16, 200–257. [Google Scholar] [PubMed]
- Kamimura, M.; Mukaiyama, K.; Koiwai, H.; Ikegami, S.; Nakamura, Y.; Kato, H. Additive effects of eldecalcitol for poorly responding long-term bisphosphonate treatment for osteoporosis. Ther. Clin. Risk Manag. 2018, in press. [Google Scholar]
- Nakamura, Y.; Uchiyama, S.; Kamimura, M.; Ikegami, S.; Komatsu, M.; Kato, H. Increased serum 25(OH)D3 levels in post-menopausal Japanese women with osteoporosis after 3-year bisphosphonate treatment. Tohoku J. Exp. Med. 2017, 242, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Soen, S. New Diagnostic criteria and guidelines on osteoporosis. Diagnostic criteria for primary osteoporosis: Year 2012 revision. Clin. Calcium 2014, 24, 323–329. (In Japanese) [Google Scholar] [PubMed]
- Sugimoto, T.; Matsumoto, T.; Hosoi, T.; Miki, T.; Gorai, I.; Yoshikawa, H.; Tanaka, Y.; Tanaka, S.; Fukunaga, M.; Sone, T.; et al. Three-year denosumab treatment in postmenopausal Japanese women and men with osteoporosis: Results from a 1-year open-label extension of the Denosumab Fracture Intervention Randomized Placebo Controlled Trial (DIRECT). Osteoporos Int. 2015, 26, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Body, J.J.; Bone, H.G.; de Boer, R.H.; Stopeck, A.; Van Poznak, C.; Damião, R.; Fizazi, K.; Henry, D.H.; Ibrahim, T.; Lipton, A.; et al. Hypocalcaemia in patients with metastatic bone disease treated with denosumab. Eur. J. Cancer 2015, 5, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Olmos, J.M.; Hernández, J.L.; Llorca, J.; Nan, D.; Valero, C.; González-Macías, J. Effects of 25-hydroxyvitamin D3 therapy on bone turnover markers and PTH levels in postmenopausal osteoporotic women treated with alendronate. J. Clin. Endocrinol. Metab. 2012, 97, 4491–4497. [Google Scholar] [CrossRef] [PubMed]
- Heckman, G.A.; Papaioannou, A.; Sebaldt, R.J.; Ioannidis, G.; Petrie, A.; Goldsmith, C.; Adachi, J.D. Effect of vitamin D on bone mineral density of elderly patients with osteoporosis responding poorly to bisphosphonates. BMC Musculoskel. Dis. 2002, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D status: Measurement, interpretation and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Denosumab (n = 22) | Combination (n = 21) | p-Value |
|---|---|---|---|
| Age (years) | 72.3 ± 2.0 | 72.1 ± 2.7 | 0.94 |
| Gender (F:M) | 20:2 | 18:3 | |
| BMI (kg/m2) | 21.8 ± 0.9 | 21.5 ± 0.7 | 0.74 |
| Serum-corrected calcium (mg/dL) | 9.2 ± 0.1 | 9.1 ± 0.1 | 0.19 |
| Serum phosphorus (mg/dL) | 3.7 ± 0.1 | 3.5 ± 0.2 | 0.40 |
| Serum BAP (μg/L) | 21.4 ± 2.3 | 22.1 ± 2.5 | 0.85 |
| TRACP-5b (mU/dL) | 595.1 ± 45.7 | 593.4 ± 49.2 | 0.98 |
| Urinary NTX (nmol BCE/mmol CRE) | 52.6 ± 5.6 | 49.7 ± 5.6 | 0.67 |
| 1,25(OH)2D3 (pg/mL) | 57.9 ± 4.7 | 57.6 ± 6.7 | 0.97 |
| Serum whole PTH (pg/mL) | 28.9 ± 2.8 | 30.0 ± 2.8 | 0.77 |
| Lumbar 1–4 BMD (g/cm2) | 0.789 ± 0.02 | 0.798 ± 0.04 | 0.84 |
| Total hip BMD (g/cm2) | 0.657 ± 0.02 | 0.672 ± 0.03 | 0.68 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, T.; Nakamura, Y.; Kato, H. Vitamin D and Calcium Addition during Denosumab Therapy over a Period of Four Years Significantly Improves Lumbar Bone Mineral Density in Japanese Osteoporosis Patients. Nutrients 2018, 10, 272. https://doi.org/10.3390/nu10030272
Suzuki T, Nakamura Y, Kato H. Vitamin D and Calcium Addition during Denosumab Therapy over a Period of Four Years Significantly Improves Lumbar Bone Mineral Density in Japanese Osteoporosis Patients. Nutrients. 2018; 10(3):272. https://doi.org/10.3390/nu10030272
Chicago/Turabian StyleSuzuki, Takako, Yukio Nakamura, and Hiroyuki Kato. 2018. "Vitamin D and Calcium Addition during Denosumab Therapy over a Period of Four Years Significantly Improves Lumbar Bone Mineral Density in Japanese Osteoporosis Patients" Nutrients 10, no. 3: 272. https://doi.org/10.3390/nu10030272