Association between Genetic Variant of Apolipoprotein C3 and Incident Hypertension Stratified by Obesity and Physical Activity in Korea


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. General Characteristics
2.3. Anthropometric and Biochemical Measurements
2.4. Genotyping
2.5. Definition of Incident HTN
2.6. Statistical Analyses
3. Results
3.1. Characteristics of Study Participants
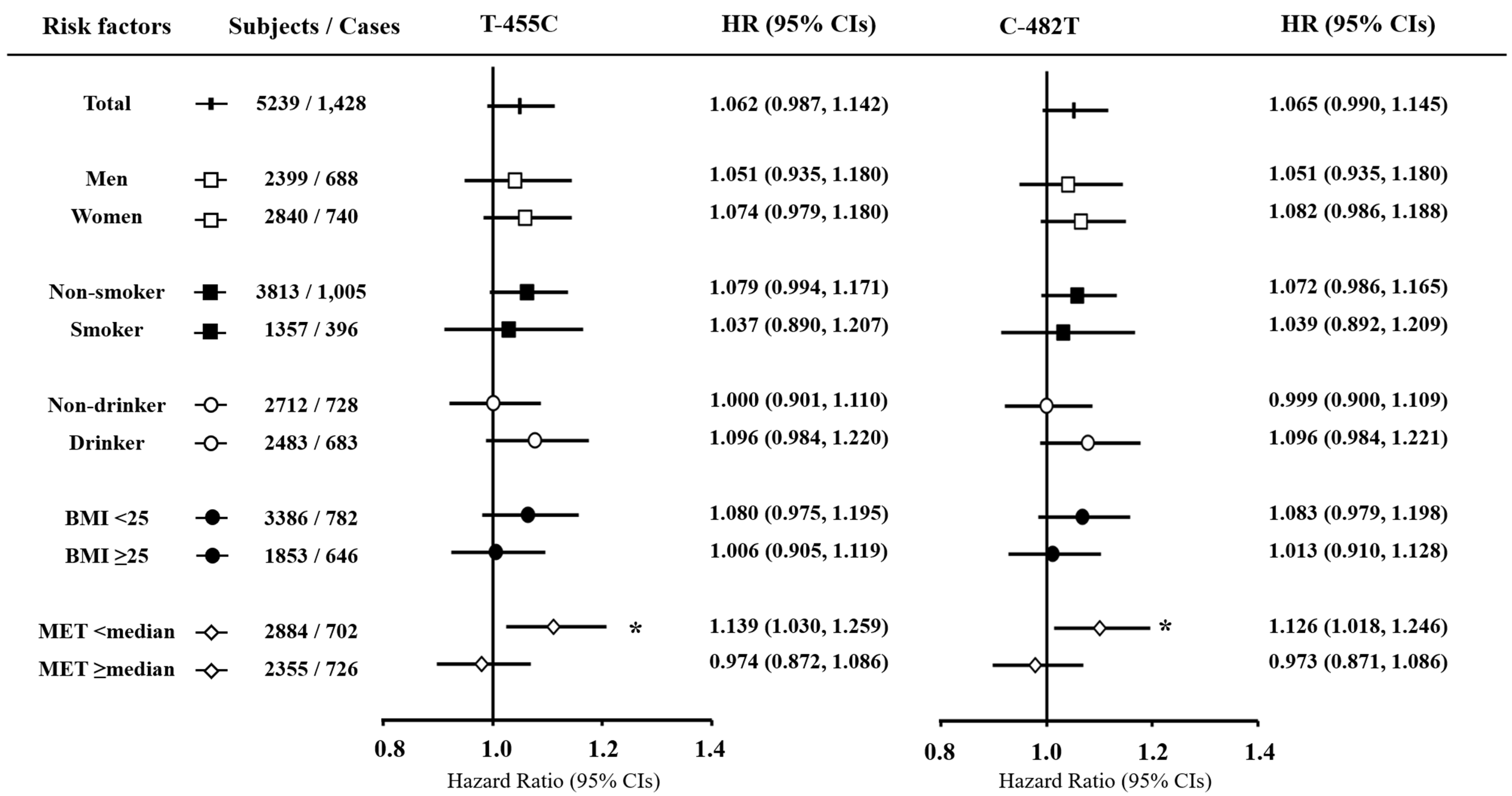
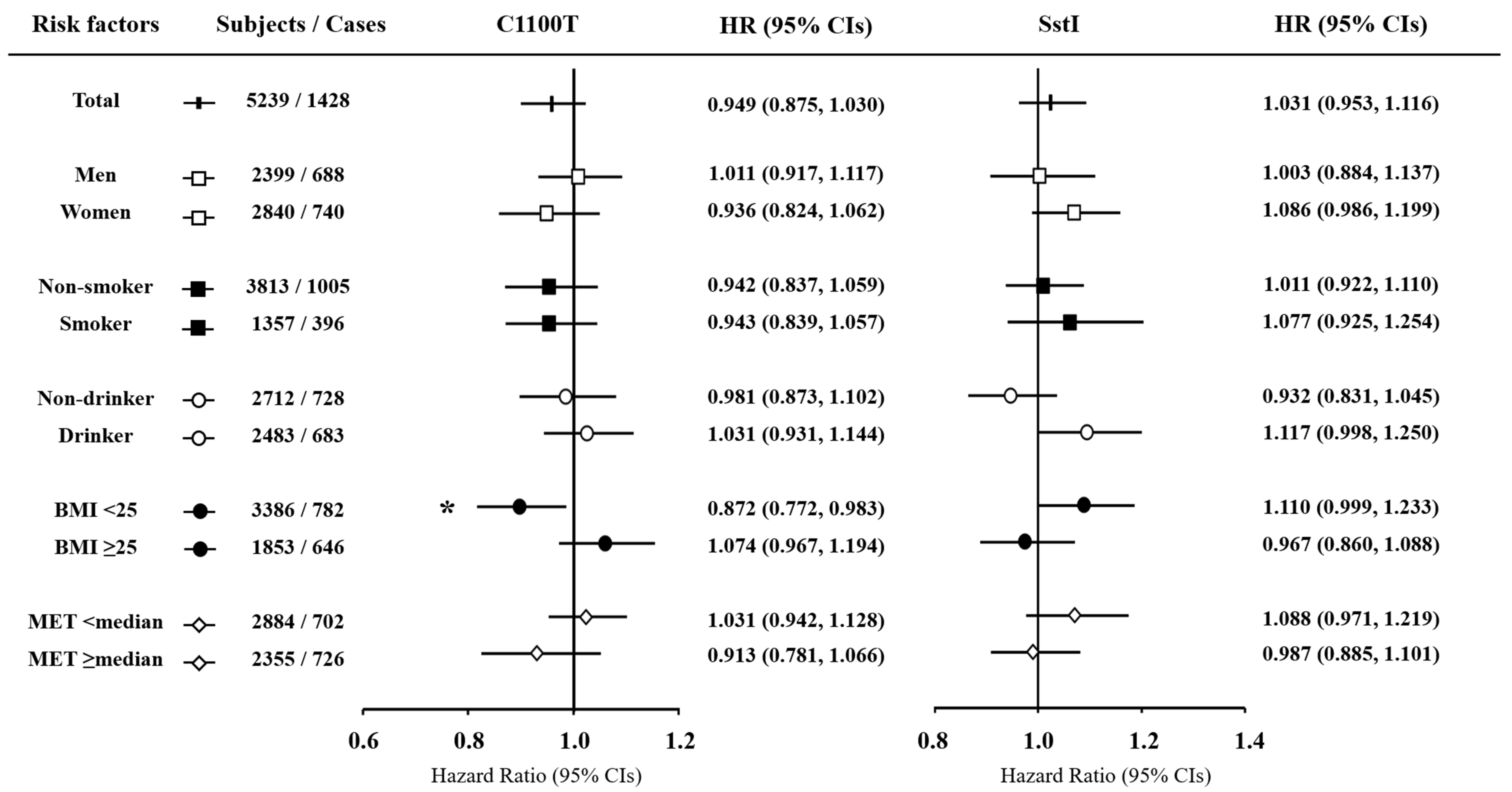
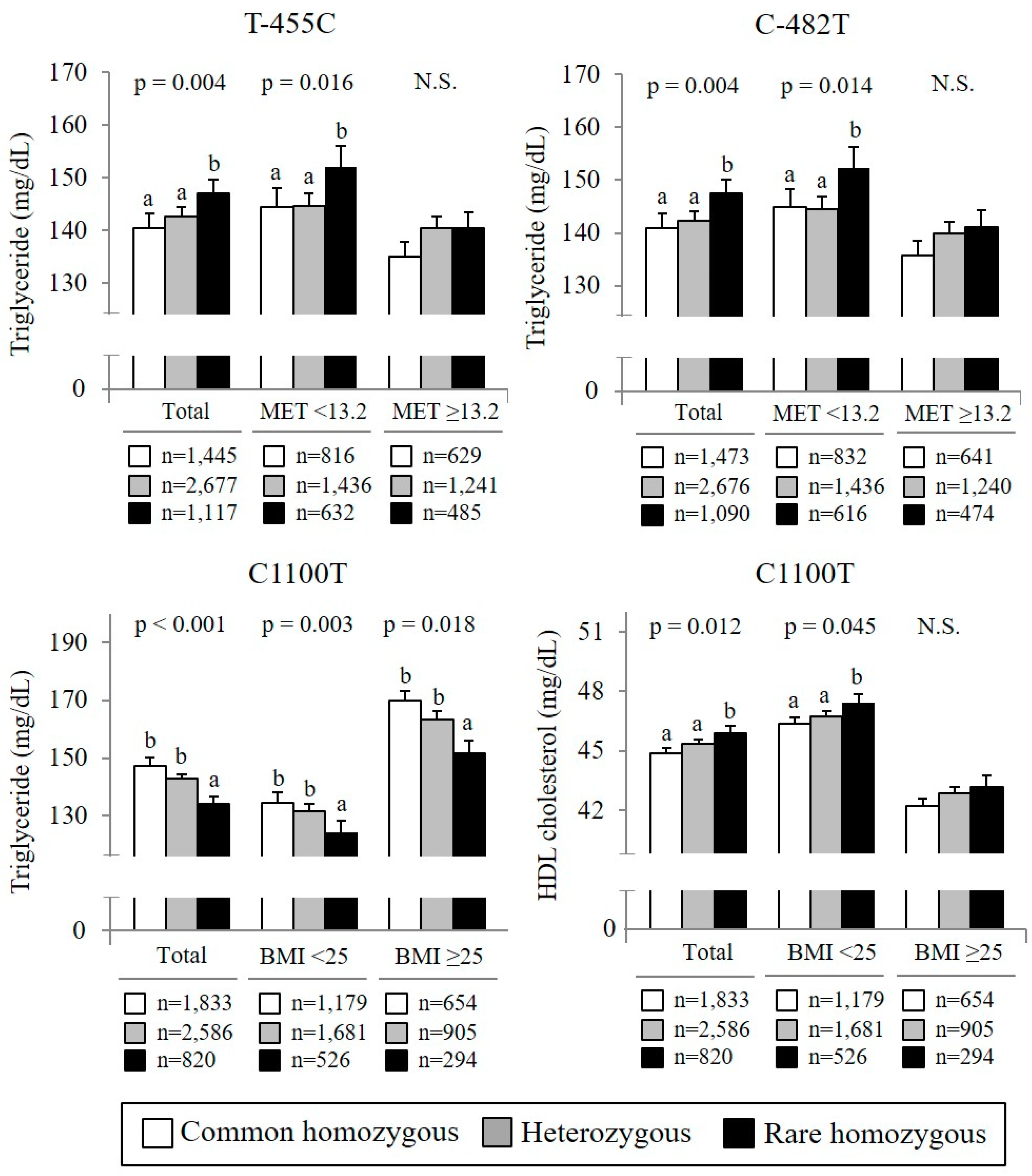
3.2. Associations of APOC3 Gene Polymorphism with HTN Risk According to Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- He, J.; Gu, D.; Chen, J.; Wu, X.; Kelly, T.N.; Huang, J.F.; Chen, J.C.; Chen, C.S.; Bazzano, L.A.; Reynolds, K.; et al. Premature deaths attributable to blood pressure in China: A prospective cohort study. Lancet 2009, 374, 1765–1772. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. Korea Health Statistics: Korea National Health and Nutrition Examination Survey (KNHANES VII); Ministry of Health & Welfare: Chungcheong Buk-Do, Korea, 2017. [Google Scholar]
- Xi, B.; Cheng, H.; Shen, Y.; Zhao, X.; Hou, D.; Wang, X.; Mi, J. Physical activity modifies the associations between genetic variants and hypertension in the Chinese children. Atherosclerosis 2012, 225, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Freiberg, J.J.; Tybjaerg-Hansen, A.; Jensen, J.S.; Nordestgaard, B.G. Nonfasting triglycerides and risk of ischemic stroke in the general population. JAMA 2008, 300, 2142–2152. [Google Scholar] [CrossRef] [PubMed]
- Laaksonen, D.E.; Niskanen, L.; Nyyssonen, K.; Lakka, T.A.; Laukkanen, J.A.; Salonen, J.T. Dyslipidaemia as a predictor of hypertension in middle-aged men. Eur. Heart. J. 2008, 29, 2561–2568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasahara, A.; Adachi, H.; Hirai, Y.; Enomoto, M.; Fukami, A.; Yoshikawa, K.; Esaki, E.; Yokoi, K.; Ogata, K.; Tsukagawa, E.; et al. High Level of Plasma Remnant-like Particle Cholesterol May Predispose to Development of Hypertension in Normotensive Subjects. Am. J. Hypertens. 2013, 26, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skarn, S.N.; Flaa, A.; Kjeldsen, S.E.; Rostrup, M.; Brunborg, C.; Reims, H.M.; Fossum, E.; Hoieggen, A.; Aksnes, T.A. Family history of hypertension and serum triglycerides predict future insulin sensitivity: A 17-year follow-up study of young men. J. Hypertens. 2015, 33, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Shimbo, D.; Muntner, P.; Mann, D.; Viera, A.J.; Homma, S.; Polak, J.F.; Barr, R.G.; Herrington, D.; Shea, S. Endothelial Dysfunction and the Risk of Hypertension: The Multi-Ethnic Study of Atherosclerosis. Hypertension 2010, 55, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Urbina, E.M.; Srinivasan, S.R.; Kieltyka, R.L.; Tang, R.; Bond, M.G.; Chen, W.; Berenson, G.S. Correlates of carotid artery stiffness in young adults: The Bogalusa heart study. Atherosclerosis 2004, 176, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Franco, O.H.; Massaro, J.M.; Civil, J.; Cobain, M.R.; O’Malley, B.; D’Agostino, R.B. Trajectories of Entering the Metabolic Syndrome: The Framingham Heart Study. Circulation 2009, 120, 1943–1950. [Google Scholar] [CrossRef] [PubMed]
- Norata, G.D.; Tsimikas, S.; Pirillo, A.; Catapano, A.L. Apolipoprotein C-III: From Pathophysiology to Pharmacology. Trends Pharmacol. Sci. 2015, 36, 675–687. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, A.; Aikawa, M.; Alcaide, P.; Luscinskas, F.W.; Libby, P.; Sacks, F.M. Apolipoprotein CIII induces expression of vascular cell adhesion molecule-1 in vascular endothelial cells and increases adhesion of monocytic cells. Circulation 2006, 114, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Xiong, Y.S.; Wang, H.M.; Chu, S.P.; Zhong, R.Q.; Wang, J.X.; Wang, G.H.; Ren, X.M.; Yu, J. APOC3 induces endothelial dysfunction through TNF-alpha and JAM-1. Lipids Health Dis. 2016, 15, 153. [Google Scholar] [CrossRef] [PubMed]
- Puppala, J.; Bhrugumalla, S.; Kumar, A.; Siddapuram, S.P.; Viswa, P.D.; Kondawar, M.; Akka, J.; Munshi, A. Apolipoprotein C3 gene polymorphisms in Southern Indian patients with nonalcoholic fatty liver disease. Indian J. Gastroenterol. 2014, 33, 524–529. [Google Scholar] [CrossRef] [PubMed]
- TG and HDL Working Group of the Exome Sequencing Project, National Heart, Lung, and Blood Institute; Crosby, J.; Peloso, G.M.; Auer, P.L.; Crosslin, D.R.; Stitziel, N.O.; Lange, L.A.; Lu, Y.; Tang, Z.Z.; Zhang, H.; et al. Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N. Engl. J. Med. 2014, 371, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Surguchov, A.P.; Page, G.P.; Smith, L.; Patsch, W.; Boerwinkle, E. Polymorphic markers in apolipoprotein C-III gene flanking regions and hypertriglyceridemia. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Huang, Y.W.; Zhang, M.Y.; Wang, J.; Wu, Y.H. Association between apolipoprotein C3 Sst I, T-455C, C-482T and C1100T polymorphisms and risk of coronary heart disease. BMJ Open 2014, 4, e004156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, K.F.; Dufour, S.; Hariri, A.; Nelson-Williams, C.; Foo, J.N.; Zhang, X.M.; Dziura, J.; Lifton, R.P.; Shulman, G.I. Apolipoprotein C3 Gene Variants in Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2010, 362, 1082–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corella, D.; Guillen, M.; Saiz, C.; Portoles, O.; Sabater, A.; Folch, J.; Ordovas, J.M. Associations of LPL and APOC3 gene polymorphisms on plasma lipids in a Mediterranean population: Interaction with tobacco smoking and the APOE locus. J. Lipid Res. 2002, 43, 416–427. [Google Scholar] [PubMed]
- Kozlitina, J.; Boerwinkle, E.; Cohen, J.C.; Hobbs, H.H. Dissociation Between APOC3 Variants, Hepatic Triglyceride Content and Insulin Resistance. Hepatology 2011, 53, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Kee, F.; Amouyel, P.; Fumeron, F.; Arveiler, D.; Cambou, J.P.; Evans, A.; Cambien, F.; Fruchart, J.C.; Ducimetiere, P.; Dallongeville, J. Lack of association between genetic variations of apo A-I-C-III-A-IV gene cluster and myocardial infarction in a sample of European male: ECTIM study. Atherosclerosis 1999, 145, 187–195. [Google Scholar] [CrossRef]
- Niu, T.H.; Jiang, M.; Xin, Y.N.; Jiang, X.J.; Lin, Z.H.; Xuan, S.Y. Lack of association between apolipoprotein C3 gene polymorphisms and risk of nonalcoholic fatty liver disease in a Chinese Han population. World J. Gastroenterol. 2014, 20, 3655–3662. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, L.; Xin, Y.; Lou, Y.; Liu, Y.; Xuan, S. Apolipoprotein c3 gene polymorphisms are not a risk factor for developing non-alcoholic Fatty liver disease: A meta-analysis. Hepat. Mon. 2014, 14, e23100. [Google Scholar] [CrossRef] [PubMed]
- Ribalta, J.; LaVille, A.E.; Vallve, J.C.; Humphries, S.; Turner, P.R.; Masana, L. A variation in the apolipoprotein C-III gene is associated with an increased number of circulating VLDL and IDL particles in familiar combined hyperlipidemia. J. Lipid Res. 1997, 38, 1061–1069. [Google Scholar] [PubMed]
- Tilly, P.; Sass, C.; Vincent-Viry, M.; Aguillon, D.; Siest, G.; Visvikis, S. Biological and genetic determinants of serum apoC-III concentration: Reference limits from the Stanislas Cohort. J. Lipid Res. 2003, 44, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G.; Grp, K. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium (vol 46, pg e20, 2016). Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of Physical Activities: An update of activity codes and MET intensities. Med. Sci. Sport Exerc. 2000, 32, S498–S516. [Google Scholar] [CrossRef]
- Cho, Y.S.; Go, M.J.; Kim, Y.J.; Heo, J.Y.; Oh, J.H.; Ban, H.J.; Yoon, D.; Lee, M.H.; Kim, D.J.; Park, M.; et al. A large-scale genome-wide association study of Asian populations uncovers genetic factors influencing eight quantitative traits. Nat. Genet. 2009, 41, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [PubMed]
- Zhang, R.N.; Zheng, R.D.; Mi, Y.Q.; Zhou, D.; Shen, F.; Chen, G.Y.; Zhu, C.Y.; Pan, Q.; Fan, J.G. APOC3 rs2070666 Is Associated with the Hepatic Steatosis Independently of PNPLA3 rs738409 in Chinese Han Patients with Nonalcoholic Fatty Liver Diseases. Dig. Dis. Sci. 2016, 61, 2284–2293. [Google Scholar] [CrossRef] [PubMed]
- Peter, A.; Kantartzis, K.; Machicao, F.; Machann, J.; Wagner, S.; Templin, S.; Konigsrainer, I.; Konigsrainer, A.; Schick, F.; Fritsche, A.; et al. Visceral obesity modulates the impact of apolipoprotein C3 gene variants on liver fat content. Int. J. Obes. 2012, 36, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Hosseini-Esfahani, F.; Mirmiran, P.; Daneshpour, M.S.; Mottaghi, A.; Azizi, F. The Effect of Interactions of Single Nucleotide Polymorphisms of APOA1/APOC3 with Food Group Intakes on the Risk of Metabolic Syndrome. Avicenna J. Med. Biotechnol. 2017, 9, 94–103. [Google Scholar] [PubMed]
- Olivieri, O.; Stranieri, C.; Bassi, A.; Zaia, B.; Girelli, D.; Pizzolo, F.; Trabetti, E.; Cheng, S.; Grow, M.A.; Pignatti, P.F.; et al. ApoC-III gene polymorphisms and risk of coronary artery disease. J. Lipid Res. 2002, 43, 1450–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, G.T.; Meigs, J.B.; Cupples, L.A.; Demissie, S.; Otvos, J.D.; Wilson, P.W.; Lahoz, C.; Cucinotta, D.; Couture, P.; Mallory, T.; et al. Association of the Sst-I polymorphism at the APOC3 gene locus with variations in lipid levels, lipoprotein subclass profiles and coronary heart disease risk: The Framingham offspring study. Atherosclerosis 2001, 158, 173–181. [Google Scholar] [CrossRef]
- Onat, A.; Erginel-Unaltuna, N.; Coban, N.; Cicek, G.; Yuksel, H. APOC3 -482C > T polymorphism, circulating apolipoprotein C-III and smoking: Interrelation and roles in predicting type-2 diabetes and coronary disease. Clin. Biochem. 2011, 44, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Song, Y.; Hu, F.B.; Niu, T.; Ma, J.; Gaziano, M.; Stampfer, M.J. A prospective study of the APOA1 XmnI and APOC3 SstI polymorphisms in the APOA1/C3/A4 gene cluster and risk of incident myocardial infarction in men. Atherosclerosis 2004, 177, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Ghattas, M.; Badawy, H.; Mesbah, N.; Abo-Elmatty, D. Apolipoprotein CIII3238C/G gene polymorphism influences oxidized low-density lipoprotein with a risk of essential hypertension. J. Biochem. Pharmacol. Res. 2013, 1, 143–147. [Google Scholar]
- Pollex, R.L.; Ban, M.R.; Young, T.K.; Bjerregaard, P.; Anand, S.S.; Yusuf, S.; Zinman, B.; Harris, S.B.; Hanley, A.J.G.; Connelly, P.W.; et al. Association between the −455T > C promoter polymorphism of the APOC3 gene and the metabolic syndrome in a multi-ethnic sample. BMC Med. Genet. 2007, 8, 80–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini-Esfahani, F.; Mirmiran, P.; Daneshpour, M.S.; Mehrabi, Y.; Hedayati, M.; Soheilian-Khorzoghi, M.; Azizi, F. Dietary patterns interact with APOA1/APOC3 polymorphisms to alter the risk of the metabolic syndrome: The Tehran Lipid and Glucose Study. Br. J. Nutr. 2015, 113, 644–653. [Google Scholar] [CrossRef] [PubMed]
- van Hoek, M.; van Herpt, T.W.; Dehghan, A.; Hofman, A.; Lieverse, A.G.; van Duijn, C.M.; Witteman, J.C.M.; Sijbrands, E.J.G. Association of an APOC3 promoter variant with type 2 diabetes risk and need for insulin treatment in lean persons. Diabetologia 2011, 54, 1360–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorgensen, A.B.; Frikke-Schmidt, R.; Nordestgaard, B.G.; Tybjaerg-Hansen, A. Loss-of-function mutations in APOC3 and risk of ischemic vascular disease. N. Engl. J. Med. 2014, 371, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Mostafavi, F.; Ghofranipour, F.; Feizi, A.; Pirzadeh, A. Improving Physical Activity and Metabolic Syndrome Indicators in Women: A Transtheoretical Model-Based Intervention. Int. J. Prev. Med. 2015, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Alkahtani, S.; Elkilany, A.; Alhariri, M. Association between sedentary and physical activity patterns and risk factors of metabolic syndrome in Saudi men: A cross-sectional study. BMC Public Health 2015, 15, 1234. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.J.; Zhang, D.D.; Liu, Y.; Sun, X.Z.; Han, C.Y.; Wang, B.Y.; Ren, Y.C.; Zhou, J.M.; Zhao, Y.; Shi, Y.Y.; et al. Dose-Response Association Between Physical Activity and Incident Hypertension A Systematic Review and Meta-Analysis of Cohort Studies. Hypertension 2017, 69, 813–820. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, B.J.; Genest, J. High-density lipoproteins and endothelial function. Circulation 2001, 104, 1978–1983. [Google Scholar] [CrossRef] [PubMed]
- Bey, L.; Hamilton, M.T. Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: A molecular reason to maintain daily low-intensity activity. J. Physiol. Lond. 2003, 551, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Augustine, J.; Tarzia, B.; Kasprowicz, A.; Heffernan, K.S. Effect of a Single Bout of Resistance Exercise on Arterial Stiffness Following a High-Fat Meal. Int. J. Sports Med. 2014, 35, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Petibois, C.; Cassaigne, A.; Gin, H.; Deleris, G. Lipid profile disorders induced by long-term cessation of physical activity in previously highly endurance-trained subjects. J. Clin. Endocr. Metab. 2004, 89, 3377–3384. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, A.; Aikawa, M.; Nitta, N.; Yoshida, M.; Libby, P.; Sacks, F.M. Apolipoprotein CIII-induced THP-1 cell adhesion to endothelial cells involves pertussis toxin-sensitive G protein- and protein kinase C alpha-mediated nuclear factor-kappa B activation. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Paynter, N.P.; Sesso, H.D.; Conen, D.; Otvos, J.D.; Mora, S. Lipoprotein Subclass Abnormalities and Incident Hypertension in Initially Healthy Women. Clin. Chem. 2011, 57, 1178–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colditz, G.A.; Martin, P.; Stampfer, M.J.; Willett, W.C.; Sampson, L.; Rosner, B.; Hennekens, C.H.; Speizer, F.E. Validation of Questionnaire Information on Risk-Factors and Disease Outcomes in a Prospective Cohort Study of Women. Am. J. Epidemiol. 1986, 123, 894–900. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 5239) | |
|---|---|
| Age, years | 50.0 (49.8, 50.3) |
| Male, % (n) | 45.8 (2399) |
| Area, % (n) | |
| Ansung, urban | 41.8 (2192) |
| Ansan, rural | 58.2 (3047) |
| Education level, % (n) | |
| ≤Elementary school | 26.8 (1392) |
| ≤Middle school | 23.8 (1236) |
| ≤High school | 35.1 (1825) |
| ≥University | 14.3 (744) |
| Metabolic equivalents, h/day | 18.5 (18.3, 18.7) |
| Current smoking, % (n) | 26.3 (1357) |
| Current drinking, % (n) | 47.8 (2483) |
| Body mass index, kg/m2 | 24.06 (24.02, 24.10) |
| Systolic BP, mmHg | 112.3 (112.0, 112.6) |
| Diastolic BP, mmHg | 74.8 (74.6, 75.0) |
| Biochemical markers | |
| Triglyceride, mg/dL | 143.0 (141.0, 145.0) |
| Total cholesterol, mg/dL | 187.4 (186.5, 188.3) |
| HDL cholesterol, mg/dL | 45.3 (45.0, 45.6) |
| LDL cholesterol, mg/dL | 114.0 (113.2, 114.8) |
| Fasting glucose, mg/dL | 82.4 (82.2, 82.6) |
| Genotype a | |
| T-455C (TT/TC/CC, %) | 27.6/51.1/21.3 |
| C-482T (CC/CT/TT, %) | 28.1/51.1/20.8 |
| C1100T (TT/TC/CC, %) | 35.0/49.4/15.7 |
| SstI (CC/CG/GG, %) | 45.1/44.9/10.0 |
| Genotype a | Triglyceride (mg/dL) b | Total Cholesterol (mg/dL) | HDL Cholesterol (mg/dL) | LDL Cholesterol (mg/dL) | Fasting Glucose (mg/dL) |
|---|---|---|---|---|---|
| T-455C | |||||
| T/T (n = 1445) | 140.9 (139.0, 142.8) c | 187.4 (186.5, 188.3) | 45.3 (45.0, 45.6) | 114.2 (113.4, 115.0) | 82.5 (82.3, 82.7) |
| T/C (n = 2677) | 142.4 (140.9, 143.9) cd | 187.3 (186.6, 188.0) | 45.4 (45.2, 45.6) | 113.9 (113.3, 114.5) | 82.3 (82.1, 82.5) |
| C/C (n = 1117) | 147.5 (145.2, 149.8) d | 187.8 (186.8, 188.8) | 44.9 (44.6, 45.2) | 114.1 (113.1, 115.1) | 82.4 (82.2, 82.6) |
| p value | 0.009 | 0.816 | 0.350 | 0.823 | 0.590 |
| C-482T | |||||
| C/C (n = 1473) | 140.4 (138.4, 142.4) c | 187.3 (186.4, 188.2) | 45.3 (45.0, 45.6) | 114.2 (113.4, 115.0) | 82.5 (82.3, 82.7) |
| C/T (n = 2676) | 142.7 (141.2, 144.2) cd | 187.5 (186.8, 188.2) | 45.4 (45.2, 45.6) | 113.9 (113.3, 114.5) | 82.3 (82.1, 82.5) |
| T/T (n = 1090) | 147.0 (144.7, 149.3) d | 187.6 (186.6, 188.6) | 44.9 (44.6, 45.2) | 114.0 (113.1, 114.9) | 82.3 (82.1, 82.5) |
| p value | 0.011 | 0.797 | 0.329 | 0.897 | 0.569 |
| C1100T | |||||
| T/T (n = 1833) | 147.2 (145.4, 149) d | 187.6 (186.8, 188.4) | 44.9 (44.7, 45.1) | 113.9 (113.2, 114.6) | 82.4 (82.2, 82.6) |
| T/C (n = 2586) | 142.8 (141.3, 144.3) d | 187.3 (186.6, 188.0) | 45.4 (45.2, 45.6) | 113.9 (113.3, 114.5) | 82.3 (82.1, 82.5) |
| C/C (n = 820) | 134.2 (131.8, 136.6) c | 187.2 (186.0, 188.4) | 45.9 (45.5, 46.3) | 114.7 (113.6, 115.8) | 82.4 (82.1, 82.7) |
| p value | <0.001 | 0.744 | 0.014 | 0.620 | 0.884 |
| SstI | |||||
| C/C (n = 2365) | 139.4 (137.9, 140.9) c | 187.2 (186.5, 187.9) | 45.5 (45.3, 45.7) | 114.2 (113.6, 114.8) | 82.3 (82.1, 82.5) |
| C/G (n = 2352) | 143.9 (142.4, 145.4) c | 187.4 (186.7, 188.1) | 45.3 (45.1, 45.5) | 113.9 (113.3, 114.5) | 82.4 (82.2, 82.6) |
| G/G (n = 522) | 155.4 (151.7, 159.1) d | 188.2 (186.7, 189.7) | 44.5 (44.1, 44.9) | 113.8 (112.4, 115.2) | 82.7 (82.3, 83.1) |
| p value | <0.001 | 0.590 | 0.052 | 0.697 | 0.302 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, G.; Kwak, S.-Y.; Kim, J.Y.; Lim, H.; Shin, M.-J. Association between Genetic Variant of Apolipoprotein C3 and Incident Hypertension Stratified by Obesity and Physical Activity in Korea. Nutrients 2018, 10, 1595. https://doi.org/10.3390/nu10111595
Jo G, Kwak S-Y, Kim JY, Lim H, Shin M-J. Association between Genetic Variant of Apolipoprotein C3 and Incident Hypertension Stratified by Obesity and Physical Activity in Korea. Nutrients. 2018; 10(11):1595. https://doi.org/10.3390/nu10111595
Chicago/Turabian StyleJo, Garam, So-Young Kwak, Ji Young Kim, Hyunjung Lim, and Min-Jeong Shin. 2018. "Association between Genetic Variant of Apolipoprotein C3 and Incident Hypertension Stratified by Obesity and Physical Activity in Korea" Nutrients 10, no. 11: 1595. https://doi.org/10.3390/nu10111595