Dietary Intake of Flavonoids and Ventilatory Function in European Adults: A GA2LEN Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The GA2LEN Study: Screening and Clinical Surveys
2.2. Estimates of Diet and Flavonoid Intake
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lago, J.H.G.; Toledo-Arruda, A.C.; Mernak, M.; Barrosa, K.H.; Martins, M.A.; Tibério, I.F.; Prado, C.M. Structure-activity association of flavonoids in lung diseases. Molecules 2014, 19, 3570–3595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, S.F.; Zoheir, K.M.; Abdel-Hamied, H.E.; Attia, S.M.; Bakheet, S.A.; Ashour, A.E.; Abd-Allah, A.R. Grape seed proanthocyanidin extract protects against carrageenan-induced lung inflammation in mice through reduction of pro-inflammatory markers and chemokine expressions. Inflammation 2014, 37, 500–511. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.Y.; Du, Q.; Li, R.R.; Huang, M.; Zhang, Q.; Wei, G.Z. Grape seed proanthocyanidin extract attenuates airway inflammation and hyperresponsiveness in a murine model of asthma by downregulating inducible nitric oxide synthase. Planta Med. 2011, 77, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.; Liang, B.; Srivastava, K.; Zeng, J.; Zhan, J.X.; Brown, L.V.; Sampson, H.; Goldfarb, J.; Emala, C.; Li, X.M. The Sophora flavescens flavonoid compound trifolirhizin inhibits acetylcholine induced airway smooth muscle contraction. Phytochemistry 2013, 95, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Hurst, S.M.; McGhie, T.K.; Cooney, J.M.; Jensen, D.J.; Gould, E.M.; Lyall, K.A.; Hurst, R.D. Blackcurrant proanthocyanidins augment IFN-γ-induced suppression of IL-4 stimulated CCL26 secretion in alveolar epithelial cells. Mol. Nutr. Food Res. 2010, 54, S159–S170. [Google Scholar] [CrossRef] [PubMed]
- Miedema, I.; Feskens, E.J.; Heederik, D.; Kromhout, D. Dietary determinants of long-term incidence of chronic nonspecific lung diseases: The Zutphen Study. Am. J. Epidemiol. 1993, 138, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Knekt, P.; Kumpulainen, J.; Järvinen, R.; Rissanen, H.; Heliövaara, M.; Reunanen, A.; Hakulinen, T.; Aromaa, A. Flavonoid intake and risk of chronic diseases. Am. J. Clin. Nutr. 2002, 76, 560–568. [Google Scholar] [PubMed]
- La Vecchia, C.; Decarli, A.; Pagano, R. Vegetable consumption and risk of chronic disease. Epidemiology 1998, 9, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Butland, B.K.; Strachan, D.P.; Anderson, H.R. Fresh fruit intake and asthma symptoms in young British adults: Confounding or effect modification by smoking? Eur. Respir. J. 1999, 13, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, S.O.; Sterne, J.A.; Thompson, R.L.; Songhurst, C.E.; Margetts, B.M.; Burney, P.G.J. Dietary antioxidants and asthma in adults: Population-based case-control study. Am. J. Respir. Crit. Care Med. 2001, 164, 1823–1828. [Google Scholar] [CrossRef] [PubMed]
- Garcia, V.; Arts, I.C.W.; Sterne, J.A.C.; Thompson, R.L.; Shaheen, S.O. Dietary intake of flavonoids and asthma in adults. Eur. Respir. J. 2005, 26, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Larsen, V.; Amigo, H.; Bustos, P.; Bakolis, I.; Rona, R.J. Ventilatory function in young adults and dietary antioxidant intake. Nutrients 2015, 7, 2879–2896. [Google Scholar] [CrossRef] [PubMed]
- Butland, B.K.; Fehily, A.M.; Elwood, P.C. Diet, lung function, and lung function decline in a cohort of 2512 middle aged men. Thorax 2000, 55, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Larsen, V.; Potts, J.F.; Omenaas, E.; Heinrich, J.; Svanes, C.; Garcia-Aymerich, J.; Burney, P.G.; Jarvis, D.L. Dietary antioxidants and 10-year lung function decline in adults from the ECRHS survey. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef] [PubMed]
- Bime, C.; Wei, C.Y.; Holbrook, J.; Smith, L.J.; Wise, R.A. Association of dietary soy genistein intake with lung function and asthma control: A post-hoc analysis of patients enrolled in a prospective multicentre clinical trial. Prim. Care Respir. J. 2012, 21, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Tomassen, P.E.T.E.R.; Newson, R.B.; Hoffmans, R.; Lötvall, J.; Cardell, L.O.; Gunnbjörnsdóttir, M.; Thilsing, T.; Matricardi, P.; Krämer, U.; Makowska, J.S.; et al. Reliability of EP3OS symptom criteria and nasal endoscopy in the assessment of chronic rhinosinusitis: A GA²LEN study. Allergy 2011, 66, 556–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Resp. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Larsen, V.; Luczynska, M.; Kowalski, M.L.; Voutilainen, H.; Ahlström, M.; Haahtela, T.; Toskala, E.; Bockelbrink, A. Use of a common food frequency questionnaire (FFQ) to assess dietary patterns and their relation to allergy and asthma in Europe: Pilot study of the GA2LEN FFQ. Eur. J. Clin. Nutr. 2011, 65, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Krebs, J. McCance and Widdowson’s the Composition of Foods: Summary Edition, 6th ed.; The Royal Society of Chemistry’s: London, UK, 2002. [Google Scholar]
- Bhagwat, S.; Gebhardt, S.; Haytowitz, D.; Holden, J.; Harnly, J. USDA Database for the Flavonoid Content of Selected Foods: Release 2.1; Nutrient Data Laboratory: Beltsville, MD, USA, 2007. [Google Scholar]
- United States Department of Agriculture (USDA). USDA Database for the Proanthocyanidin Content of Selected Foods; Nutrient Data Laboratory: Beltsville, MD, USA, 2004.
- Cassidy, A.; O’Reilly, E.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Simes, R.J. An improved Bonferroni procedure for multiple tests of significance. Biometrika 1986, 73, 751–754. [Google Scholar] [CrossRef]
- Tabak, C.; ARTS, I.C.; Smit, H.A.; Heederik, D.; Kromhout, D. Chronic obstructive pulmonary disease and intake of catechins, flavonols, and flavones: The MORGEN Study. Am. J. Respir. Crit. Care Med. 2001, 164, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Burney, P.G.; Hooper, R.L. The use of ethnically specific norms for ventilatory function in African-American and white populations. Int. J. Epidemiol. 2012, 41, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Kwon, H.S.; Bang, B.R.; Lee, Y.S.; Park, M.Y.; Moon, K.A.; Kim, T.B.; Lee, K.Y.; Moon, H.B.; Cho, Y.S. Grape seed proanthocyanidin extract attenuates allergic inflammation in murine models of asthma. J. Clin. Immunol. 2012, 32, 1292–1304. [Google Scholar] [CrossRef] [PubMed]
- Clifford, M.N.; van der Hooft, J.J.; Crozier, A. Human studies on the absorption, distribution, metabolism, and excretion of tea polyphenols. Am. J. Clin. Nutr. 2013, 98, 1619S–1630S. [Google Scholar] [CrossRef] [PubMed]
- De Ferrars, R.M.; Czank, C.; Zhang, Q.; Botting, N.P.; Kroon, P.A.; Cassidy, A.; Kay, C.D. The pharmacokinetics of anthocyanins and their metabolites in humans. Br. J. Pharmacol. 2014, 171, 3268–3282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czank, C.; Cassidy, A.; Zhang, Q.; Morrison, D.J.; Preston, T.; Kroon, P.A.; Botting, N.P.; Kay, C.D. Human metabolism and elimination of the anthocyanin, cyanidin-3-glucoside: A 13C-tracer study. Am. J. Clin. Nutr. 2013, 97, 995–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra, A.; Macià, A.; Rubió, L.; Anglès, N.; Ortega, N.; Morelló, J.R.; Romero, M.P.; Motilva, M.J. Distribution of procyanidins and their metabolites in rat plasma and tissues in relation to ingestion of procyanidin-enriched or procyanidin-rich cocoa creams. Eur. J. Nutr. 2013, 52, 1029–1038. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, T.; Horio, F.; Uchida, K.; Aoki, H.; Osawa, T. Dietary cyanidin 3-O-β-d-glucoside-rich purple corn color prevents obesity and ameliorates hyperglycemia in mice. J. Nutr. 2003, 133, 2125–2130. [Google Scholar] [PubMed]
- Aqil, F.; Vadhanam, M.V.; Jeyabalan, J.; Cai, J.; Singh, I.P.; Gupta, R.C. Detection of anthocyanins/anthocyanidins in animal tissues. J. Agric. Food Chem. 2014, 62, 3912–3918. [Google Scholar] [CrossRef] [PubMed]
- Benn, T.; Kim, B.; Park, Y.K.; Wegner, C.J.; Harness, E.; Nam, T.G.; Kim, D.O.; Lee, J.S.; Lee, J.Y. Polyphenol-rich blackcurrant extract prevents inflammation in diet-induced obese mice. J. Nutr. Biochem. 2014, 25, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Rovira, M.A.; Grau, M.; Castanier, O.; Covas, M.I.; Schroeder, H.; Investigators, R. Dietary supplement use and health-related behaviors in a mediterranean population. J. Nutr. Educ. Behav. 2013, 45, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Metabolomics 2016 Poster Abstracts. Available online: http://metabolomics2016.org/images/Poster-Abstracts-6-21-16.pdf (accessed on 15 October 2017).
- Mehta, A.J.; Cassidy, A.; Litonjua, A.A.; Sparrow, D.; Vokonas, P.; Schwartz, J. Dietary anthocyanin intake and age-related decline in lung function: Longitudinal findings from the VA Normative Aging Study. Am. J. Clin. Nutr. 2016, 103, 542–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosso, G.; Godos, J.; Lamuela-Raventos, R.; Ray, S.; Micek, A.; Pajak, A.; Sciacca, S.; D’Orazio, N.; Del Rio, D.; Galvano, F. A comprehensive meta-analysis on dietary flavonoid and lignan intake and cancer risk: Level of evidence and limitations. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Countries Participating in the GA2LEN Nutrition Survey | |||||||||
| Denmark | Finland | Sweden | UK | Portugal | ||||||
| Odense (268) | Helsinki (122) | Total (1085) | Total (139) | Coimbra (233) | ||||||
| Age, years; mean (SD) | 47.9 | (14.2) | 45.8 | (14.5) | 45.5 | (15) | 51.3 | (13.2) | 47.2 | (14.5) |
| Males, n (%) | 115 | (42.9) | 47 | (38.5) | 471 | (43.4) | 54 | (38.8) | 80 | (34.3) |
| Height, m (SD) | 1.7 | (0.1) | 1.7 | (0.1) | 1.7 | (0.1) | 1.7 | (0.1) | 1.6 | (0.1) |
| BMI (m2/kg) | 26.9 | (4.7) | 26.5 | (4.3) | 26 | (4.7) | 27.8 | (5.8) | 26.6 | (5.3) |
| Never smokers, n (%) | 119 | (44.4) | 60 | (49.2) | 578 | (53.3) | 63 | (45.3) | 148 | (63.5) |
| Ex-smokers, n (%) | 71 | (26.5) | 30 | (24.6) | 366 | (33.7) | 55 | (39.6) | 51 | (21.9) |
| Current smokers, n (%) | 78 | (29.1) | 32 | (26.2) | 141 | (13) | 21 | (15.1) | 34 | (14.6) |
| Cases/controls | 180/88 | 62/60 | 774/311 | 95/44 | 169/64 | |||||
| * FVC, L | 4.1 | (1.0) | 4.0 | (1.0) | 4.1 | (1.0) | 3.7 | (1.0) | 3.8 | (1.0) |
| * FEV1/FVC | 78.4 | (8.6) | 80 | (7.9) | 78.2 | (8.6) | 75.4 | (10.8) | 80.5 | (8.3) |
| FVC < LLN, n (%) | 36 | (13.4) | 10 | (8.2) | 141 | (13) | 20 | (14.4) | 16 | (6.9) |
| FEV1/FVC < LLN, n (%) | 32 | (11.9) | 6 | (4.9) | 130 | (12) | 25 | (18) | 25 | (10.7) |
| Nutritional supplements, n (%) | 107 | (39.9) | 52 | (42.6) | 285 | (26.3) | 49 | (35.3) | 15 | (6.4) |
| Total fruit intake, g/day | 328 | (263.8) | 278.2 | (219.4) | 320.7 | (242.5) | 328.8 | (238.3) | 549.2 | (403.7) |
| Total vegetable intake, g/day | 342.6 | (223.8) | 415.5 | (297.5) | 355.8 | (206.8) | 343.2 | (207.8) | 454.5 | (321.1) |
| Variables | Countries Participating in the GA2LEN Nutrition Survey | |||||||||
| Belgium | Germany | The Netherlands | Poland | Total | ||||||
| Ghent (107) | Total (305) | Amsterdam (174) | Total (166) | 2599 | ||||||
| Age, years, mean (SD) | 44.5 | (14.4) | 48.7 | (15.2) | 52.7 | (13.6) | 51.6 | (15) | 47.4 | (14.8) |
| Males, n (%) | 47 | (43.9) | 116 | (38) | 88 | (50.6) | 65 | (39.2) | 1083 | (41.7) |
| Height, m (SD) | 1.7 | (0.1) | 1.7 | (0.1) | 1.7 | (0.1) | 1.7 | (0.1) | 1.7 | (0.1) |
| BMI (m2/kg) | 24.5 | (4) | 26.9 | (5) | 27.1 | (4) | 27.7 | (5.2) | 26.5 | (4.8) |
| Never smokers, n (%) | 60 | (56.1) | 148 | (48.5) | 70 | (40.2) | 79 | (47.6) | 1,325 | (51) |
| Ex-smokers, n (%) | 32 | (29.9) | 108 | (35.4) | 67 | (38.5) | 48 | (28.9) | 828 | (31.9) |
| Current smokers, n (%) | 15 | (14) | 49 | (16.1) | 37 | (21.3) | 39 | (23.5) | 446 | (17.2) |
| Cases/Controls | 60/47 | 142/163 | 111/63 | 108/58 | 1701/898 | |||||
| * FVC, L | 4.3 | (1.0) | 3.9 | (1.0) | 4.1 | (1.0) | 3.8 | (1.0) | 4.0 | (1.0) |
| * FEV1/FVC | 79.4 | (9.5) | 78.8 | (7.7) | 77.1 | (8.4) | 77 | (10.4) | 78.3 | (8.8) |
| FVC < LLN, n (%) | 9 | (8.4) | 55 | (18) | 11 | (6.3) | 13 | (7.8) | 311 | (12) |
| FEV1/FVC < LLN, n (%) | 10 | (9.3) | 25 | (8.2) | 20 | (11.5) | 20 | (12) | 293 | (11.3) |
| Nutritional supplements, n (%) | 33 | (30.8) | 81 | (26.6) | 72 | (41.4) | 39 | (23.5) | 733 | (28.2) |
| Total fruit intake, g/day | 333.1 | (235.1) | 314.7 | (273.2) | 289.5 | (211.8) | 465.2 | (466.9) | 347.3 | (291.2) |
| Total vegetable intake, g/day | 244.8 | (126.1) | 261.9 | (187.2) | 224.5 | (130.5) | 482.8 | (429.6) | 349.1 | (246.9) |
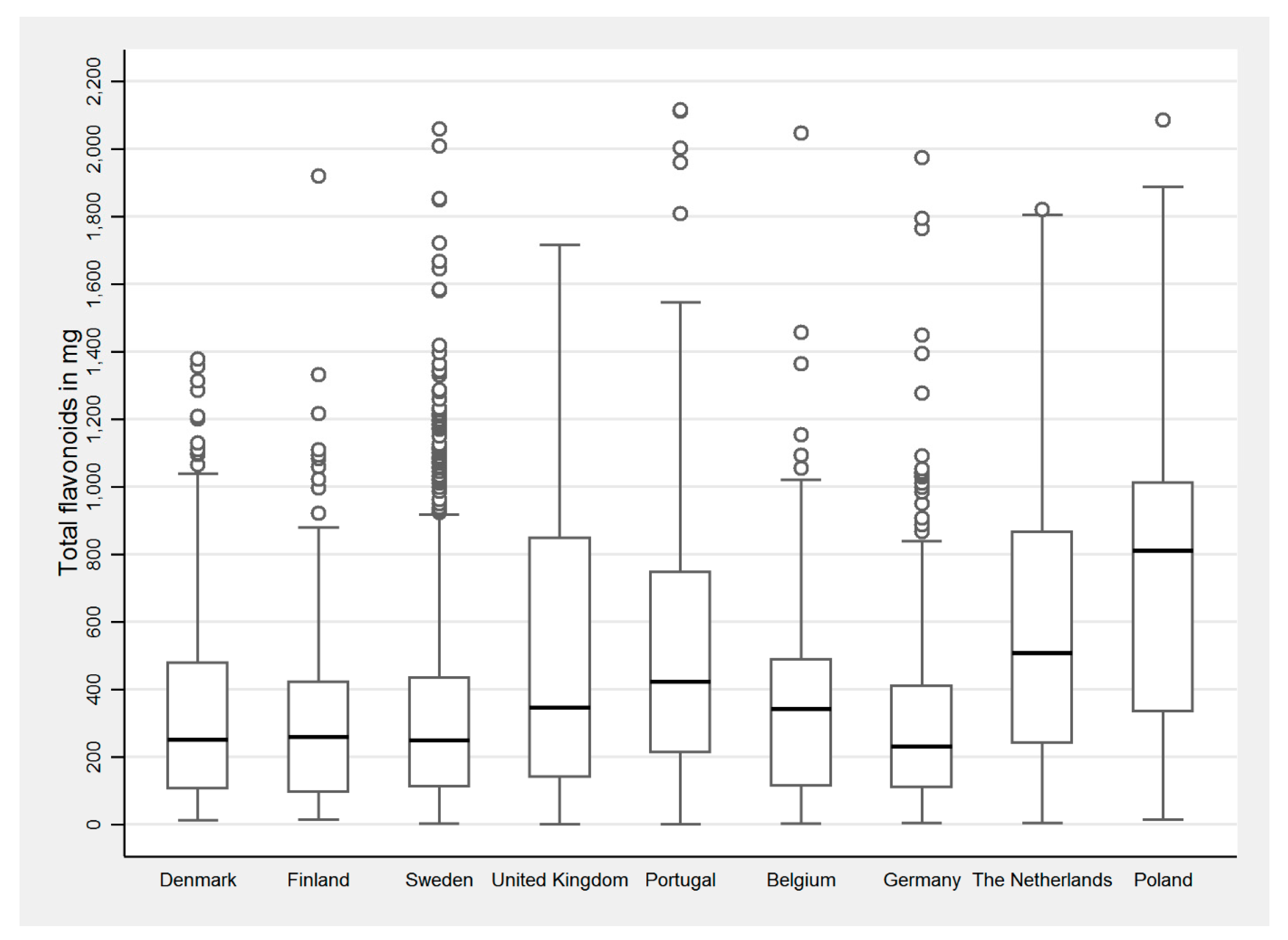
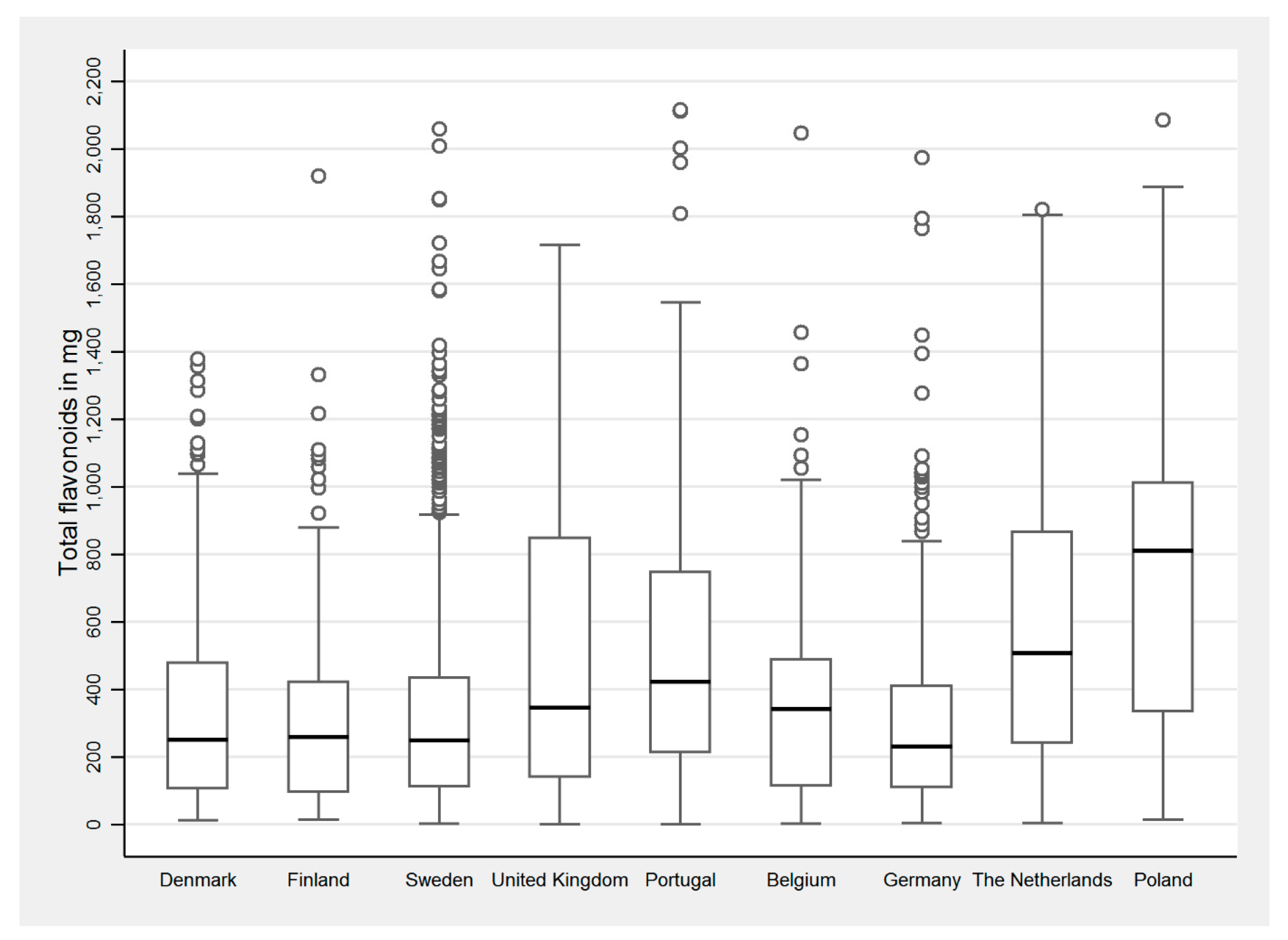
| Dietary Intake of Flavonoids across Countries (Median Intake in mg, IQR) | ||||||||||
| Flavonoid Subclass | Denmark | Finland | Sweden | UK | Portugal | |||||
| Odense (268) | Helsinki (122) | Total (1085) | Total (139) | Coimbra (233) | ||||||
| Total flavonoids | 251.1 | (106.3 to 479.7) | 260.5 | (95.2 to 427.2) | 249.4 | (113 to 439.1) | 345.5 | (140.3 to 848.8) | 426.5 | (215.8 to 749.1) |
| Flavanones | 4.5 | (1.3 to 20.9) | 8.3 | (1.8 to 23.6) | 5.3 | (1.4 to 21) | 5 | (1.8 to 18.3) | 17.1 | (2.9 to 60.3) |
| Anthocyanins | 7.5 | (2.4 to 16.3) | 5.9 | (2.1 to 13) | 6.5 | (2.1 to 15.1) | 9.8 | (3.7 to 30.3) | 22.1 | (6.9 to 47.5) |
| Flavan-3-ols | 30.6 | (14 to 69) | 24.4 | (10 to 56.3) | 29.4 | (13 to 65.3) | 43.7 | (14.8 to 183.5) | 44 | (20.9 to 78.2) |
| Flavanols | 16.3 | (9.3 to 29.3) | 19.5 | (10.8 to 33.1) | 16.9 | (9.2 to 28.2) | 16.7 | (9.1 to 32.7) | 26.6 | (12.9 to 44.6) |
| Flavones | 2.1 | (0.9 to 4.4) | 2.4 | (1.3 to 4.5) | 2 | (0.9 to 4.3) | 1.7 | (0.6 to 3.2) | 2.6 | (1.1 to 5.7) |
| Polymers | 175.7 | (66.1 to 316.3) | 162.9 | (62.5 to 260.2) | 159.5 | (66.4 to 283.3) | 251.5 | (75.7 to 601.5) | 266.8 | (106.5 to 459.8) |
| Pro-anthocyanidins | 135.3 | (68.6 to 261.1) | 152.8 | (58.7 to 270.7) | 126.6 | (62.9 to 245.7) | 195.2 | (76.7 to 376.6) | 286.7 | (113.1 to 465.1) |
| Dietary Intake of Flavonoids across Countries (Median Intake in mg, IQR) | ||||||||||
| Flavonoid Subclass | Belgium | Germany | The Netherlands | Poland | Total | |||||
| Ghent (107) | Total (305) | Amsterdam (174) | Total (166) | 2599 | ||||||
| Total flavonoids | 341.4 | (113.9 to 489.4) | 231.7 | (110.2 to 413.8) | 507 | (242.1 to 867.4) | 817.3 | (341.6 to 1029.3) | 291.2 | (126.8 to 569.4) |
| Flavanones | 10.3 | (2.3 to 27.9) | 4.9 | (1.1 to 21.6) | 7 | (2.3 to 29) | 6.7 | (1.8 to 28) | 5.7 | (1.5 to 22.5) |
| Anthocyanins | 10.5 | (2.7 to 21) | 5.5 | (1.7 to 13.3) | 8.1 | (2.8 to 22.1) | 9.2 | (2.3 to 26.3) | 7.5 | (2.4 to 19.6) |
| Flavan-3-ols | 32.9 | (13.6 to 83.8) | 38.1 | (13.2 to 77.3) | 84.1 | (35.5 to 186.2) | 176.3 | (54.9 to 200.1) | 37.9 | (15.4 to 90.4) |
| Flavanols | 13.1 | (7 to 23.7) | 11 | (5.2 to 20.2) | 17.8 | (9.2 to 30.6) | 34 | (21.3 to 51.8) | 17.2 | (9.2 to 30.8) |
| Flavones | 1.4 | (0.5 to 2.5) | 1.1 | (0.4 to 2.3) | 1.5 | (0.6 to 2.5) | 2.1 | (0.7 to 5.8) | 1.9 | (0.7 to 3.9) |
| Polymers | 216.5 | (71.1 to 325.5) | 132.1 | (63.7 to 268.1) | 341.7 | (129.5 to 622.3) | 585.9 | (243 to 687.5) | 198.4 | (72.9 to 375.2) |
| Pro-anthocyanidins | 214.9 | (80.5 to 343.8) | 136.1 | (69 to 261.4) | 190.8 | (101.5 to 327.8) | 192.7 | (105.5 to 311.8) | 154.6 | (72.5 to 284.3) |
| Food Groups (mg/% Total Dietary Sources) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Flavonoid Subclasses (mg) | All Fruit | Citrus Fruit | Hard Fruit | Berries | Other Fruit | Vegetables | Chocolate | Nuts | Legumes | Tea & Coffee | Wine & Beer |
| Total flavonoids | 289.93 | 36.58 | 124.08 | 2.91 | 64.09 | 14.9 | 30.87 | 1.43 | 0.23 | 152.9 | 21.07 |
| Flavanones | 7.51% | 59.21% | 0.00% | 0.10% | 0.19% | 2.08% | 0.00% | 0.06% | 0.00% | 0.00% | 2.47% |
| Anthocyanins | 5.66% | 9.00% | 4.38% | 28.94% | 13.18% | 1.96% | 0.00% | 2.59% | 0.42% | 0.00% | 9.43% |
| Flavan-3-ols | 6.86% | 1.58% | 7.07% | 4.61% | 8.93% | 0.00% | 16.33% | 3.26% | 21.38% | 31.41% | 26.85% |
| Flavonols | 3.45% | 1.49% | 4.41% | 1.17% | 1.87% | 79.15% | 0.00% | 1.38% | 21.62% | 2.91% | 9.00% |
| Flavones | 0.34% | 1.62% | 0.14% | 0.45% | 0.29% | 16.81% | 0.00% | 0.00% | 0.00% | 0.00% | 1.23% |
| Polymers | 76.18% | 27.11% | 84.02% | 64.74% | 75.54% | 0.00% | 83.67% | 92.71% | 56.59% | 65.68% | 51.02% |
| Pro-anthocyanidins | 234.07 | 10.11 | 110.84 | 1.98 | 50.75 | 0.00 | 34.64 | 1.40 | 0.18 | 15.1 | 14.92 |
| Flavonoid Subclass (Quintiles; mg) | FVC (Lt) (Continuous) | FVC < LLN (Binary) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect Size (Regression Coefficient and 95% Confidence Interval) Per-Quintile Increase in Flavonoid Intake | OR (95% Confidence Interval) Highest Vs. Lowest Quintile of Flavonoid Intake | ||||||||||||
| Model 1 (n = 2599) | p-Value | Model 2 (n = 2599) | p-Value | Model 1 (n = 2599) | p-Value | Model 2 (n = 2599) | p-Value | p-Value after Simes’ Procedure | |||||
| Total flavanoids | 0.03 | (0.02 to 0.05) | <0.0001 | 0.02 | (−0.002 to 0.03) | 0.09 | 0.47 | (0.31 to 0.71) | <0.0001 | 0.58 | (0.36 to 0.94) | 0.03 | 0.07 |
| Flavanones | 0.03 | (0.02 to 0.05) | <0.0001 | 0.02 | (−0.002 to 0.03) | 0.08 | 0.47 | (0.31 to 0.71) | 0.0003 | 0.60 | (0.37 to 0.97) | 0.04 | 0.07 |
| Anthocyanins | 0.04 | (0.02 to 0.05) | <0.0001 | 0.02 | (−0.01 to 0.04) | 0.14 | 0.37 | (0.24 to 0.57) | <0.0001 | 0.47 | (0.26 to 0.83) | 0.01 | 0.04 |
| Flavan-3-ols | 0.02 | (0.002 to 0.03) | 0.03 | <0.001 | (−0.02 to 0.02) | 0.97 | 0.58 | (0.39 to 0.86) | 0.01 | 0.75 | (0.49 to 1.14) | 0.17 | |
| Flavonols | 0.03 | (0.02 to 0.05) | 0.0001 | 0.01 | (−0.004 to 0.03) | 0.12 | 0.52 | (0.35 to 0.76) | 0.0008 | 0.66 | (0.41 to 1.04) | 0.07 | |
| Flavones | 0.02 | (0.01 to 0.04) | 0.003 | 0.01 | (−0.01 to 0.02) | 0.54 | 0.58 | (0.40 to 0.85) | 0.01 | 0.79 | (0.51 to 1.22) | 0.28 | |
| Polymers | 0.03 | (0.02 to 0.05) | 0.0001 | 0.01 | (−0.003 to 0.03) | 0.10 | 0.52 | (0.34 to 0.79) | 0.002 | 0.65 | (0.41 to 1.04) | 0.07 | |
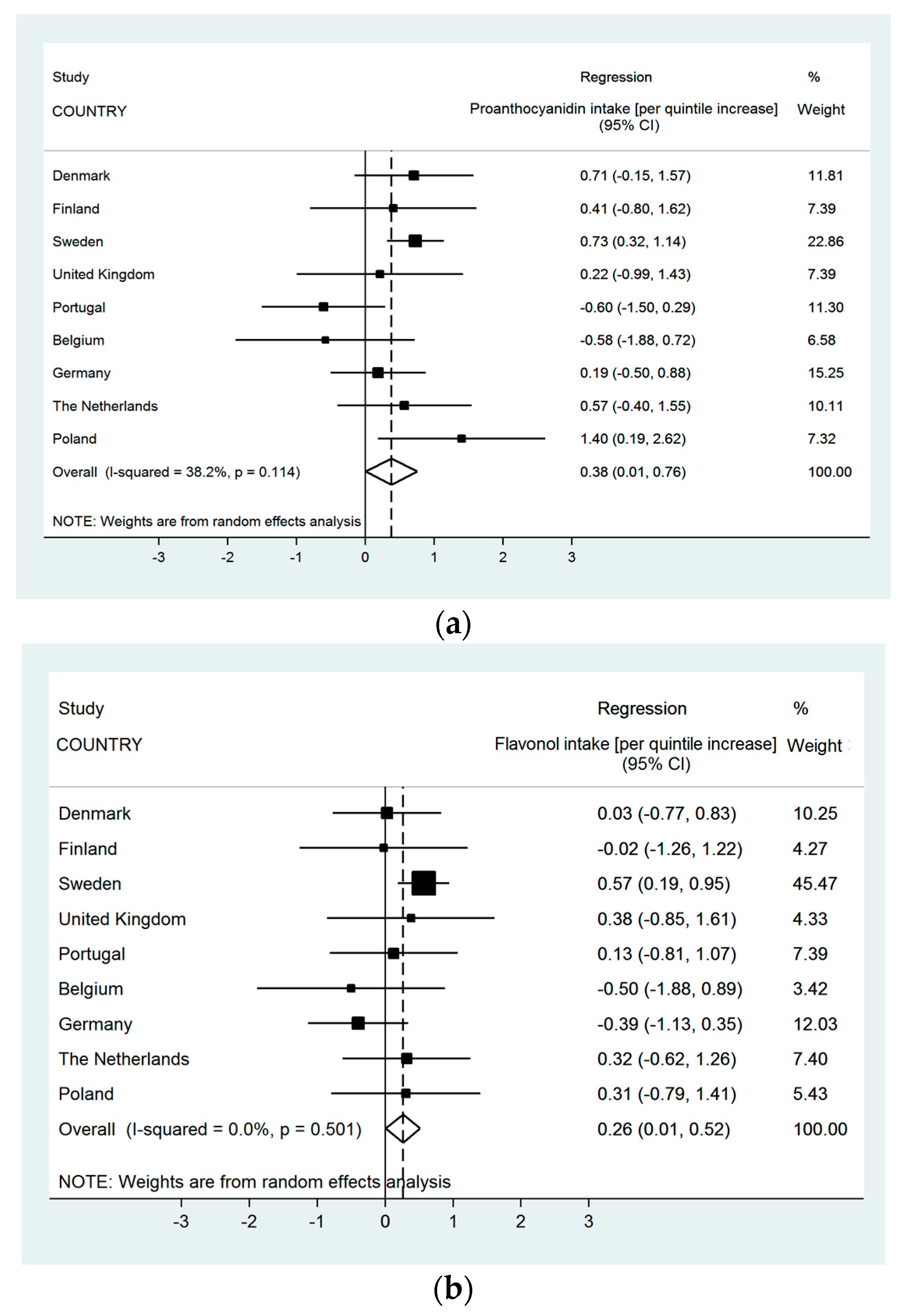
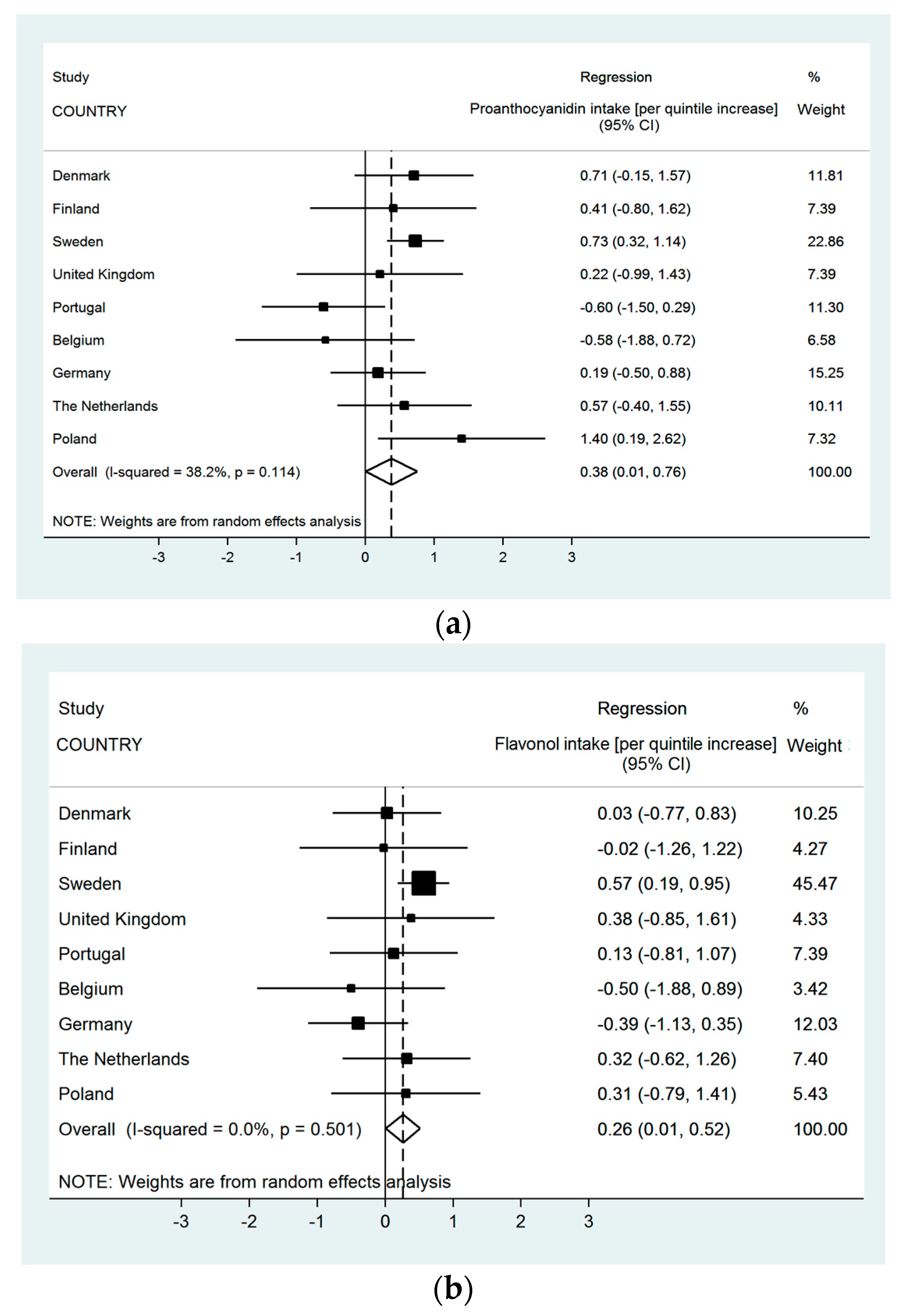
| Pro-anthocyanidins | 0.04 | (0.02 to 0.05) | <0.0001 | 0.02 | (−0.002 to 0.04) | 0.07 | 0.41 | (0.26 to 0.63) | 0.0001 | 0.47 | (0.27 to 0.81) | 0.01 | 0.04 |
| Flavonoid Subclass (Quintiles; mg) | FEV1/FVC (Continuous) | FEV1/FVC < LLN (Binary) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect Size (Regression Coefficient and 95% Confidence Interval) Per-Quintile Increase in Flavonoid Intake | OR (95% Confidence Interval) Highest vs. Lowest Quintile of Flavonoid Intake | |||||||||||||
| Model 1 (n = 2599) | p-Value | Model 2 (n = 2599) | p-Value | p-Value after Simes’ Procedure | Model 1 (n = 2599) | p-Value | Model 2 (n = 2599) | p-Value | p-Value after Simes’ Procedure | |||||
| Total flavanoids | 0.50 | (0.29 to 0.72) | <0.0001 | 0.33 | (0.10 to 0.57) | 0.01 | 0.02 | 0.58 | (0.39 to 0.86) | 0.01 | 0.61 | (0.39 to 0.97) | 0.04 | 0.12 |
| Flavanones | 0.16 | (−0.05 to 0.37) | 0.15 | 0.07 | (−0.30 to 0.17) | 0.57 | 0.71 | (0.47 to 1.08) | 0.11 | 0.84 | (0.51 to 1.37) | 0.49 | ||
| Anthocyanins | 0.34 | (0.13 to 0.56) | 0.002 | 0.12 | (−0.15 to 0.39) | 0.39 | 0.58 | (0.39 to 0.86) | 0.01 | 0.73 | (0.43 to 1.24) | 0.25 | ||
| Flavan-3-ols | 0.42 | (0.21 to 0.63) | 0.0001 | 0.20 | (−0.02 to 0.42) | 0.07 | 0.65 | (0.44 to 0.97) | 0.03 | 0.73 | (0.47 to 1.11) | 0.14 | ||
| Flavonols | 0.34 | (0.13 to 0.56) | 0.002 | 0.18 | (−0.06 to 0.42) | 0.14 | 0.77 | (0.52 to 1.14) | 0.19 | 0.92 | (0.58 to 1.47) | 0.74 | ||
| Flavones | 0.31 | (0.1 to 0.52) | 0.004 | 0.17 | (−0.07 to 0.4) | 0.16 | 0.80 | (0.54 to 1.18) | 0.26 | 1.01 | (0.63 to 1.6) | 0.97 | ||
| Polymers | 0.48 | (0.27 to 0.69) | <0.0001 | 0.32 | (0.09 to 0.55) | 0.01 | 0.02 | 0.55 | (0.37 to 0.81) | 0.002 | 0.56 | (0.36 to 0.88) | 0.01 | 0.09 |
| Pro-anthocyanidins | 0.58 | (0.37 to 0.79) | <0.0001 | 0.44 | (0.19 to 0.69) | 0.001 | 0.004 | 0.58 | (0.39 to 0.85) | 0.01 | 0.61 | (0.37 to 0.99) | 0.04 | 0.12 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Larsen, V.; Thawer, N.; Charles, D.; Cassidy, A.; Van Zele, T.; Thilsing, T.; Ahlström, M.; Haahtela, T.; Keil, T.; Matricardi, P.M.; et al. Dietary Intake of Flavonoids and Ventilatory Function in European Adults: A GA2LEN Study. Nutrients 2018, 10, 95. https://doi.org/10.3390/nu10010095
Garcia-Larsen V, Thawer N, Charles D, Cassidy A, Van Zele T, Thilsing T, Ahlström M, Haahtela T, Keil T, Matricardi PM, et al. Dietary Intake of Flavonoids and Ventilatory Function in European Adults: A GA2LEN Study. Nutrients. 2018; 10(1):95. https://doi.org/10.3390/nu10010095
Chicago/Turabian StyleGarcia-Larsen, Vanessa, Narjis Thawer, David Charles, Aedin Cassidy, Thibaut Van Zele, Trine Thilsing, Matti Ahlström, Tari Haahtela, Thomas Keil, Paolo M Matricardi, and et al. 2018. "Dietary Intake of Flavonoids and Ventilatory Function in European Adults: A GA2LEN Study" Nutrients 10, no. 1: 95. https://doi.org/10.3390/nu10010095