Developing Sustainable Workplaces with Leadership: Feedback about Organizational Working Conditions to Support Leaders in Health-Promoting Behavior


Abstract
:1. Introduction
1.1. Leadership and Health
1.2. Key Aspects of Health-Promoting Leadership
1.3. Development of an Instrument to Measure Health-Promoting Leadership
1.4. Health-Influencing Conditions in Organizations
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measures
2.2.1. Health-Promoting Leadership Conditions (HPLC)
2.2.2. Health-Oriented Leadership (HoL)
2.2.3. Maslach Burnout Inventory—General Survey German (MBI-GS-D)
2.2.4. Recovery-Stress-Questionnaire for Work (RESTQ-Work)
2.3. Analysis
3. Results
3.1. Item Analysis
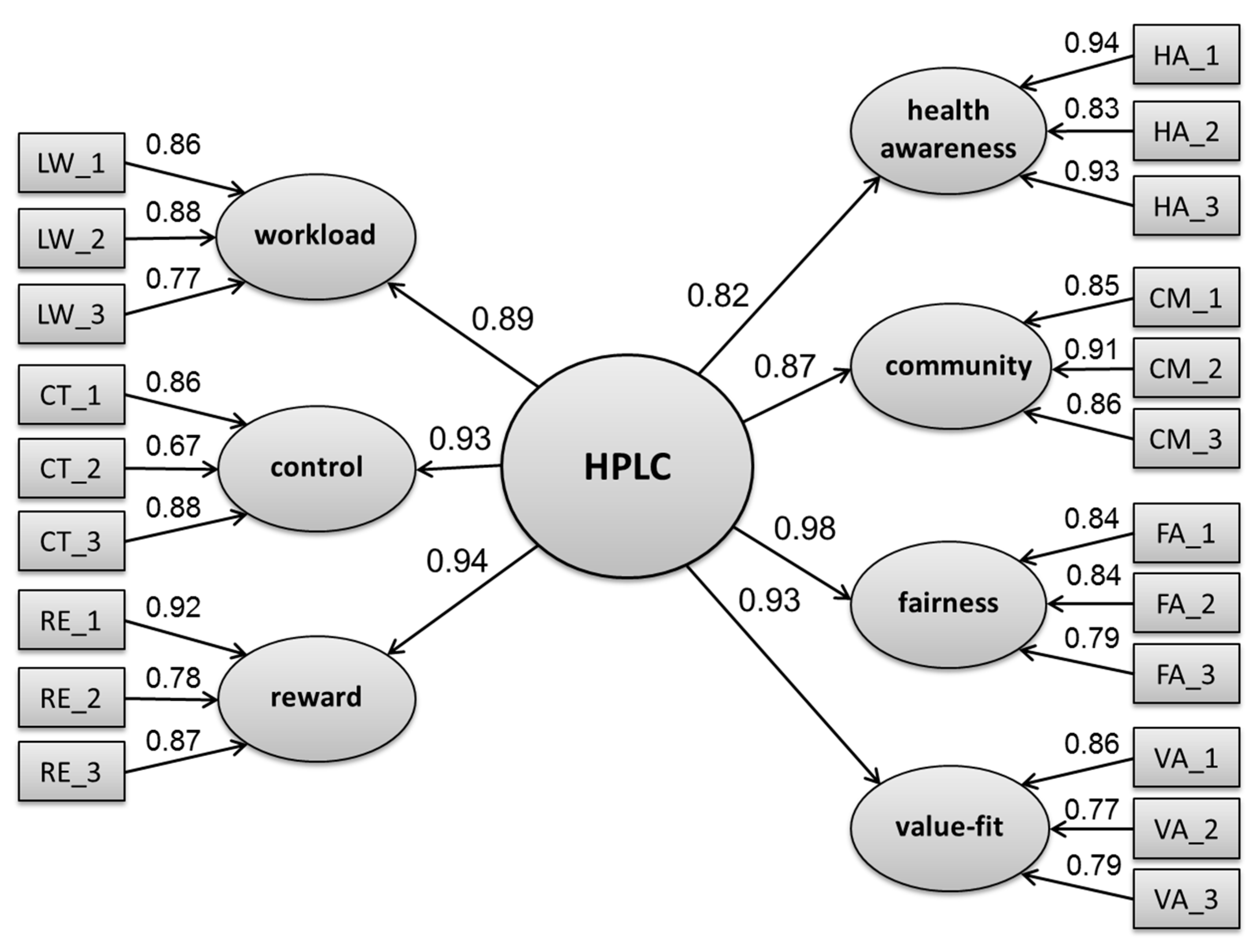
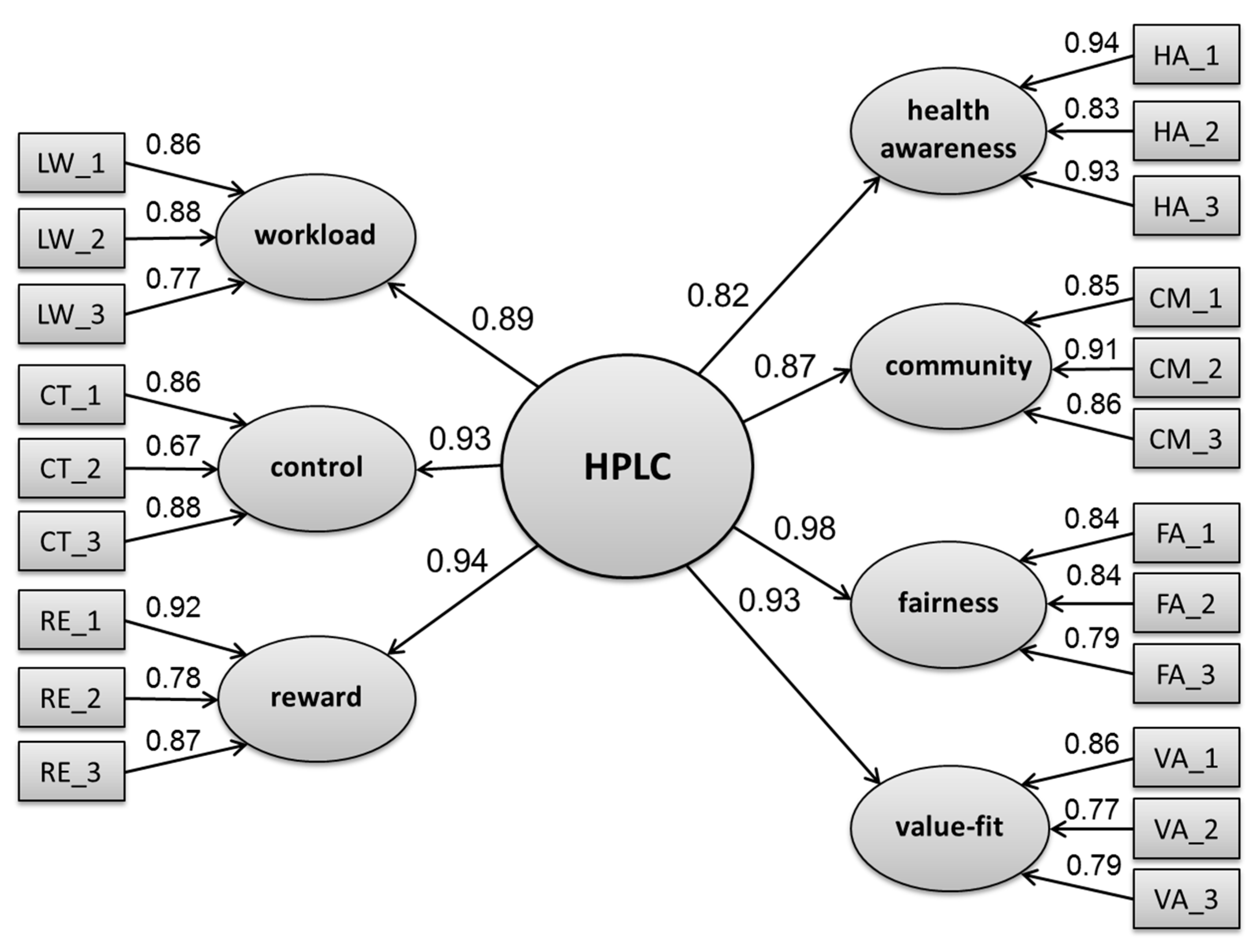
3.2. Structural Equation Modeling (SEM)
3.3. Validity Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Di Fabio, A. The Psychology of Sustainability and Sustainable Development for Well-Being in Organizations. Front. Psychol. 2017, 8, 1534. [Google Scholar] [CrossRef] [PubMed]
- Suriyankietkaew, S.; Avery, G. Sustainable Leadership Practices Driving Financial Performance. Empirical Evidence from Thai SMEs. Sustainability 2016, 8, 327. [Google Scholar] [CrossRef]
- Swerissen, H.; Crisp, B.R. The sustainability of health promotion interventions for different levels of social organization. Health Promot. Int. 2004, 19, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, P.; Winkler, B.; Dunkl, A. Creating a healthy working environment with leadership: The concept of health-promoting leadership. Int. J. Hum. Resour. Manag. 2017, 28, 2430–2448. [Google Scholar] [CrossRef]
- Atwater, L.E.; Brett, J.F.; Charles, A.C. Multisource feedback: Lessons learned and implications for practice. Hum. Resour. Manag. 2007, 46, 285–307. [Google Scholar] [CrossRef]
- Seifert, C.F.; Yukl, G. Effects of repeated multi-source feedback on the influence behavior and effectiveness of managers. A field experiment. Leadersh. Q. 2010, 21, 856–866. [Google Scholar] [CrossRef]
- European Network for Workplace Health Promotion (ENWHP). Luxembourg Declaration on Workplace Health Promotion in the European Union. Available online: http://www.enwhp.org/fileadmin/rs-dokumente/dateien/Luxembourg_Declaration.pdf (accessed on 27 September 2017).
- Kelloway, E.K.; Barling, J. Leadership development as an intervention in occupational health psychology. Work Stress 2010, 24, 260–279. [Google Scholar] [CrossRef]
- Anderson, D.; Plotnikoff, R.C.; Raine, K.; Barrett, L. Development of measures of individual leadership for health promotion. Leadersh. Health Serv. 2005, 18, 1–11. [Google Scholar] [CrossRef]
- Eriksson, A.; Axelsson, R.; Axelsson, S. Health promoting leadership—Different views of the concept. Work 2011, 40, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Gurt, J.; Schwennen, C.; Elke, G. Health-specific leadership: Is there an association between leader consideration for the health of employees and their strain and well-being? Work Stress 2011, 25, 108–127. [Google Scholar] [CrossRef]
- Hewison, A.; Griffiths, M. Leadership development in health care: A word of caution. J. Health Organ. Manag. 2004, 18, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Dunkl, A.; Jiménez, P.; Šarotar-Žižek, S.; Milfelner, B.; Kallus, K.W. Similarities and differences of health-promoting leadership and transformational leadership. Naše Gospod. 2015, 61, 3–13. [Google Scholar] [CrossRef]
- Semmer, N. Job stress interventions and the organization of work. Scand. J. Work Environ. Health 2006, 32, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, T.; Holstad, T.J.; Mohr, G.; Stempel, C.R.; Hansen, E.N.; Loeb, C.; Otto, K.; Kinnunen, U.; Perko, K. Rewarding and Sustainable Health-Promoting Leadership; Bundesanstalt für Arbeitsschutz und Arbeitsmedizin (BAuA): Dortmund/Berlin/Dresden, Germany, 2014. [Google Scholar]
- Wegge, J.; Shemla, M.; Haslam, A. Leader behavior as a determinant of health at work: Specification and evidence of five key pathways. Ger. J. Hum. Resour. Manag. 2014, 28, 6–23. [Google Scholar] [CrossRef]
- Skarholt, K.; Blix, E.H.; Sandsund, M.; Andersen, T.K. Health promoting leadership practices in four Norwegian industries. Health Promot. Int. 2015, 31, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Skakon, J.; Nielsen, K.; Borg, V.; Guzman, J. Are leaders’ well-being, behaviours and style associated with the affective well-being of their employees? A systematic review of three decades of research. Work Stress 2010, 24, 107–139. [Google Scholar] [CrossRef]
- Law, R.; Dollard, M.F.; Tuckey, M.R.; Dormann, C. Psychosocial safety climate as a lead indicator of workplace bullying and harassment, job resources, psychological health and employee engagement. Accid. Anal. Prev. 2011, 43, 1782–1793. [Google Scholar] [CrossRef] [PubMed]
- Goldgruber, J.; Ahrens, D. Effectiveness of workplace health promotion and primary prevention interventions: A review. J. Public Health 2010, 18, 75–88. [Google Scholar] [CrossRef]
- International Labour Office (ILO). Report of the Joint International Labour Office and World Health Organization on Occupational Health. In Psychosocial Factors at Work: Recognition and Control; International Labour Office: Geneva, Switzerland, 1986. [Google Scholar]
- Leka, S.; Jain, A.; Cox, T.; Kortum, E. The Development of the European Framework for Psychosocial Risk Management: PRIMA-EF. J. Occup. Health 2011, 53, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Aven, T.; Krohn, B.S. A new perspective on how to understand, assess and manage risk and the unforeseen. Reliab. Eng. Syst. Saf. 2014, 121, 1–10. [Google Scholar] [CrossRef]
- Leiter, M.P.; Maslach, C. Six areas of worklife: A model of the organizational context of burnout. J. Health Hum. Serv. Adm. 1999, 21, 472–489. [Google Scholar] [PubMed]
- Maslach, C.; Leiter, M.P. Early Predictors of Job Burnout and Engagement. J. Appl. Psychol. 2008, 93, 498–512. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, P.; Kallus, K.W. Stress and Recovery of Social Care Professionals: Development of a screening version of the Recovery-Stress-Questionnaire for Work. In Change and Quality in Human Service Work; Korunka, C., Hoffmann, P., Eds.; Hampp: Munich, Germany, 2005; pp. 311–323. [Google Scholar]
- Bakker, A.B.; Demerouti, E.; Euwema, M.C. Job Resources Buffer the Impact of Job Demands on Burnout. J. Occup. Health Psychol. 2005, 10, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990. [Google Scholar]
- Nahrgang, J.; Morgeson, F.; Hofmann, D. Safety at work: A meta-analytic investigation of the link between job demands, job resources, burnout, engagement, and safety outcomes. J. Appl. Psychol. 2011, 96, 71–94. [Google Scholar] [CrossRef] [PubMed]
- Grawitch, M.J.; Gottschalk, M.; Munz, D.C. The Path to a Healthy Workplace: A Critical Review Linking Healthy Workplace Practices, Employee Well-being, and Organizational Improvements. Consult. Psychol. J. Pract. Res. 2006, 58, 129–147. [Google Scholar] [CrossRef]
- Halbesleben, J.R.B. Sources of Social Support and Burnout: A Meta-Analytic Test of the Conservation of Resources Model. J. Appl. Psychol. 2006, 91, 1134–1145. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Cortina, L.M.; Magley, V.J. Personal and Workgroup Incivility: Impact on Work and Health Outcomes. J. Appl. Psychol. 2008, 93, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Forret, M.; Love, M.S. Employee justice perceptions and coworker relationships. Leadersh. Organ. Dev. J. 2008, 29, 248–260. [Google Scholar] [CrossRef]
- Robbins, J.M.; Ford, M.T.; Tetrick, L.E. Perceived Unfairness and Employee Health: A Meta-Analytic Integration. J. Appl. Psychol. 2012, 97, 235–272. [Google Scholar] [CrossRef] [PubMed]
- Leiter, M.P.; Gascón, S.; Martínez-Jarreta, B. Making Sense of Work Life: A Structural Model of Burnout. J. Appl. Soc. Psychol. 2010, 40, 57–75. [Google Scholar] [CrossRef]
- Franke, F.; Felfe, J. Diagnose gesundheitsförderlicher Führung—Das Instrument Health oriented leadership [Diagnosis of health-promoting leading culture—The instrument health oriented leadership]. In Fehlzeitenreport 2011 Schwerpunkt Führung und Gesundheit [Absenteeism Report 2011 Focus Leadership and Health]; Badura, B., Ducki, A., Schröder, H., Klose, J., Macco, K., Eds.; Springer: Heidelberg, Germany, 2011; pp. 3–13. [Google Scholar]
- Milner, K.; Greyling, M.; Goetzel, R.; Da Silva, R.; Kolbe-Alexander, T.; Patel, D.; Nossel, C.; Beckowski, M. The relationship between leadership support, workplace health promotion and employee wellbeing in South Africa. Health Promot. Int. 2015, 30, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Leiter, M.P.; Maslach, C. The Areas of Worklife Survey Manual, 4th ed.; Centre for Organizational Research & Development: Wolfville, NS, USA, 2006. [Google Scholar]
- Komljenovic, D.; Loiselle, G.; Kumral, M. Organization: A new focus on mine safety improvement in a complex operational and business environment. Int. J. Min. Sci. Technol. 2017, 27, 617–625. [Google Scholar] [CrossRef]
- Antonovsky, A. Salutogenese: Zur Entmystifizierung der Gesundheit [Salutogenesis. Unraveling the Mystery of Health]; dgvt-Verlag: Tübingen, Germany, 1997. [Google Scholar]
- Kelloway, K.E.; Day, A.L. Building Healthy Workplaces: What we know so far. Can. J. Behav. Sci. 2005, 37, 223–235. [Google Scholar] [CrossRef]
- Shain, M.; Kramer, D.M. Health promotion in the workplace: Framing the concept; reviewing the evidence. Occup. Environ. Med. 2004, 61, 643–648. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Healthy Workplaces: A Model for Action: For Employers, Workers, Policy-Makers and Practitioners; WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- Danna, K.; Griffin, R.W. Health and Well-Being in the Workplace. A Review and Synthesis of the Literature. J. Manag. 1999, 25, 357–384. [Google Scholar] [CrossRef]
- Aust, B.; Ducki, A. Comprehensive health promotion interventions at the workplace: Experiences with health circles in Germany. J. Occup. Health Psychol. 2004, 9, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Demerouti, E.; Bakker, A.; Nachreiner, F.; Ebbinghaus, M. From mental strain to burnout. Eur. J. Work Organ. Psychol. 2002, 11, 423–441. [Google Scholar] [CrossRef]
- Peiro, J.M.; Ayala, Y.; Tordera, N.; Lorente, L.; Rodriguez, I. Sustainable well-being at work: A review and reformulation. Pap. Psicól. 2014, 35, 5–14. [Google Scholar]
- Kallus, K.W. Stress and Recovery: An Overview. In The Recovery-Stress Questionnaires: User Manual; Kallus, K.W., Kellmann, M., Eds.; Pearson Assessment: Frankfurt, Germany, 2016; pp. 27–48. [Google Scholar]
- Kallus, K.W.; Kellmann, M. Burnout in Athletes and Coaches. In Emotions in Sports; Hanin, Y.L., Ed.; Human Kinetics: Champaign, IL, USA, 2000; pp. 209–230. ISBN 9780880118798. [Google Scholar]
- Schaufeli, W.B.; Leiter, M.P.; Maslach, C.; Jackson, S.E. Maslach Burnout Inventory—General Survey (MBI-GS). In Maslach Burnout Inventory Manual; Maslach, C., Jackson, S.E., Leiter, M.P., Eds.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996; pp. 208–212. ISBN 9789996345777. [Google Scholar]
- Büssing, A.; Glaser, J. Managerial Stress und Burnout. A Collaborative International Study (CISMS). Die Deutsche Untersuchung (Bericht Nr. 44); Technische Universität: München, Germany, 1998. [Google Scholar]
- Jiménez, P.; Kallus, W.K. EBF-Work (27) [RESTQ-Work (27)]; Pearson Assessment: Frankfurt, Germany, 2016. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Meth. Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- Beauducel, A.; Wittmann, W.W. Simulation Study on Fit Indexes in CFA Based on Data with Slightly Distorted Simple Structure. Struct. Equ. Model. 2005, 12, 41–75. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Marsh, H.W. The hierarchical structure of self-concept and the application of hierarchical confirmatory factor analysis. J. Educ. Meas. 1987, 24, 17–39. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hocevar, D. Application of Confirmatory Factor Analysis to the Study of Self-Concept: First- and Higher Order Factor Models and Their Invariance Across Groups. Psychol. Bull. 1985, 97, 562–582. [Google Scholar] [CrossRef]
- Tsai, Y. Relationship between organizational culture, leadership behavior and job satisfaction. BMC Health Serv. Res. 2011, 11, 98. [Google Scholar] [CrossRef] [PubMed]
- Aitken, P. Walking the talk: The nature and role of leadership culture within organisation culture/s. J. Gen. Manag. 2007, 32, 17–37. [Google Scholar] [CrossRef]
- Day, D.V. Leadership development: A review in context. Leadersh. Q. 2011, 11, 581–613. [Google Scholar] [CrossRef]
- Hollnagel, E. Resilience engineering and the built environment. Build. Res. Inf. 2014, 42, 221–228. [Google Scholar] [CrossRef]
- Schwarz, M.; Kallus, K.W.; Jimenez, P. Organisationale Resilienz und Sicherheitsverhalten in der Flugsicherung: Empirische Untersuchung von individuellen und tätigkeitsspezifischen Zusammenhängen [Organizational resilience and safety behavior in air traffic control: An empirical examination of individual and activity-specific correlates]. In Resilienz in Organisationen Stärken. Vorbeugung und Bewältigung von kritischen Situationen [Strenghtening Reslience in Organizations. Prevention and Coping in Critical Situations]; Bargstedt, U., Horn, G., van Vegten, A., Eds.; Verlag für Polizeiwissenschaft: Frankfurt, Germany, 2014; pp. 47–62. ISBN 978-3866763937. [Google Scholar]
- Weick, K.E. The Collapse of Sensemaking in Organizations: The Mann Gulch Disaster. Adm. Sci. Q. 1993, 38, 628–652. [Google Scholar] [CrossRef]
- Leveson, N.G. Engineering a Safer World: Systems Thinking Applied to Safety; Engineering Systems; MIT Press: Cambridge, MA, USA, 2011. [Google Scholar]

{kind=link}
| Item Shortcuts | Items My Leader Takes Care, that… | Item Total Correlation |
|---|---|---|
| HA_1 | … the health of all employees is promoted. | 0.89 |
| HA_2 | … all employees are motivated to take care of their health. | 0.81 |
| HA_3 | … the health of the employees is highly valued. | 0.86 |
| WL_1 | … there is enough time left for the work to be done. | 0.77 |
| WL_2 | … work under high pressure is not carried out over a longer period of time. | 0.80 |
| WL_3 | … work does not significantly affect private life. | 0.69 |
| CT_1 | … the resources and scope for personal development at work can be influenced. | 0.72 |
| CT_2 | … at work autonomous and independent action can be taken. | 0.63 |
| CT_3 | … all have the necessary scope to do their work. | 0.79 |
| RE_1 | … work is appreciated. | 0.81 |
| RE_2 | … efforts do not go unnoticed. | 0.76 |
| RE_3 | … all contributions are being acknowledged. | 0.83 |
| CM_1 | … work colleagues support each other. | 0.81 |
| CM_2 | … there is a good cooperation between all work colleagues. | 0.85 |
| CM_3 | … work colleagues talk openly to each other. | 0.80 |
| FA_1 | … all resources are fairly distributed. | 0.76 |
| FA_2 | … all employees are treated in a fair manner. | 0.74 |
| FA_3 | … one’s career depends on competencies and not on the connections someone has. | 0.72 |
| VA_1 | … the employees share the company’s values. | 0.75 |
| VA_2 | … the employees’ daily activities correspond with the company’s objectives. | 0.70 |
| VA_3 | … personal career interests are in line with the objectives of the company. | 0.70 |
| Dimension | Item Shortcuts | M | SD | α |
|---|---|---|---|---|
| Health awareness | HA_1, HA_2, HA_3 | 2.45 | 1.72 | 0.93 |
| Workload | WL_1, WL_2, WL_3 | 2.83 | 1.54 | 0.87 |
| Control | CT_1, CT_2, CT_3 | 3.51 | 1.43 | 0.84 |
| Reward | RE_1, RE_2, RE_3 | 3.05 | 1.61 | 0.90 |
| Community | CM_1, CM_2, CM_3 | 3.46 | 1.63 | 0.91 |
| Fairness | FA_1, FA_2, FA_3 | 3.17 | 1.58 | 0.86 |
| Value-fit | VA_1, VA_2, VA_3 | 3.10 | 1.46 | 0.85 |
| Dimension | HPLC: Health Awareness | HPLC: Workload | HPLC: Control | HPLC: Reward | HPLC: Community | HPLC: Fairness | HPLC: Value-Fit | HoL: Awareness | HoL: Values | HoL: Behavior | restq-W: Social Emotional Stress | RESTQ-W: Overall Recovery | RESTQ-W: Loss of Meaning/Burnout | RESTQ-W: Leisure/Breaks | RESTQ-W: Psycho- Social Resources | RESTQ-W: Work- Related Resources | MBI-GS-D: Emotional Exhaustion | MBI-GS-D: Personal Accomp- Lishment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HPLC: health awareness | ||||||||||||||||||
| HPLC: workload | 0.76 ** | |||||||||||||||||
| HPLC: control | 0.70 ** | 0.74 ** | ||||||||||||||||
| HPLC: reward | 0.77 ** | 0.75 ** | 0.84 ** | |||||||||||||||
| HPLC: community | 0.69 ** | 0.72 ** | 0.73 ** | 0.77 ** | ||||||||||||||
| HPLC: fairness | 0.78 ** | 0.80 ** | 0.82 ** | 0.87 ** | 0.78 ** | |||||||||||||
| HPLC: value-fit | 0.76 ** | 0.71 ** | 0.81 ** | 0.82 ** | 0.76 ** | 0.86 ** | ||||||||||||
| HoL: awareness | 0.65 ** | 0.63 ** | 0.51 ** | 0.65 ** | 0.63 ** | 0.68 ** | 0.68 ** | |||||||||||
| HoL: values | 0.76 ** | 0.61 ** | 0.57 ** | 0.61 ** | 0.49 ** | 0.69 ** | 0.58 ** | 0.65 ** | ||||||||||
| HoL: behavior | 0.84 ** | 0.70 ** | 0.54 ** | 0.61 ** | 0.52 ** | 0.64 ** | 0.58 ** | 0.67 ** | 0.78 ** | |||||||||
| RESTQ-W: social emotional stress | −0.23 ** | −0.31 ** | −0.35 ** | −0.31 ** | −0.23 ** | −0.36 ** | −0.29 ** | −0.13 | −0.09 | −0.12 | ||||||||
| RESTQ-W: overall recovery | 0.25 ** | 0.34 ** | 0.33 ** | 0.28 ** | 0.20 ** | 0.31 ** | 0.26 ** | 0.40 * | 0.48 ** | 0.35 * | −0.56 ** | |||||||
| RESTQ-W: loss of meaning/burnout | −0.35 ** | −0.48 ** | −0.47 ** | −0.44 ** | −0.36 ** | −0.48 ** | −0.42 ** | −0.48 ** | −0.28 | −0.34 * | 0.74 ** | −0.49 ** | ||||||
| RESTQ-W: leisure/breaks | 0.30 ** | 0.41 ** | 0.38 ** | 0.31 ** | 0.21 ** | 0.31 ** | 0.25 ** | 0.59 ** | 0.54 ** | 0.56 ** | −0.47 ** | 0.63 ** | −0.49 ** | |||||
| RESTQ-W: psychosocial resources | 0.33 ** | 0.31 ** | 0.35 ** | 0.36 ** | 0.50 ** | 0.36 ** | 0.34 ** | 0.43 ** | 0.28 | 0.28 | −0.09 | 0.26 ** | −0.17 ** | 0.29 ** | ||||
| RESTQ-W: work-related resources | 0.47 ** | 0.44 ** | 0.66 ** | 0.58 ** | 0.44 ** | 0.57 ** | 0.54 ** | 0.52 ** | 0.47 ** | 0.47 ** | −0.33 ** | 0.46 ** | −0.42 ** | 0.41 ** | 0.39 ** | |||
| MBI-GS-D: emotional exhaustion | −0.25 ** | −0.37 ** | −0.31 ** | −0.32 ** | −0.32 ** | −0.36 ** | −0.29 ** | −0.29 | −0.30 | −0.20 | 0.55 ** | −0.42 ** | 0.66 ** | −0.53 ** | −0.18 * | −0.29 ** | ||
| MBI-GS-D: cynicism | −0.40 ** | −0.41 ** | −0.53 ** | −0.57 ** | −0.51 ** | −0.58 ** | −0.52 ** | −0.40 * | −0.39 * | −0.23 | 0.48 ** | −0.36 ** | 0.70 ** | −0.32 ** | −0.27 ** | −0.55 ** | 0.58 ** | |
| MBI-GS-D: personal accomplishment | 0.23 ** | 0.22 ** | 0.37 ** | 0.30 ** | 0.25 ** | 0.31 ** | 0.34 ** | 0.24 | 0.32 | 0.18 | −0.30 ** | 0.44 ** | −0.36 ** | 0.30 ** | 0.25 ** | 0.58 ** | −0.18 ** | −0.42 ** |
| Model | χ2 | df | p | AGFI | GFI | CFI | RMSEA | T | T2 |
|---|---|---|---|---|---|---|---|---|---|
| unidimensional model | 959.000 | 184 | <0.001 | 0.780 | 0.825 | 0.906 | 0.099 | ||
| first-order model (uncorrelated) | 3213.897 | 184 | <0.001 | 0.322 | 0.460 | 0.634 | 0.196 | ||
| first-order model (correlated) | 426.059 | 163 | <0.001 | 0.873 | 0.910 | 0.968 | 0.061 | ||
| seven-factor with higher order factor model | 482.880 | 177 | <0.001 | 0.869 | 0.899 | 0.963 | 0.063 | 0.882 | 0.979 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez, P.; Winkler, B.; Bregenzer, A. Developing Sustainable Workplaces with Leadership: Feedback about Organizational Working Conditions to Support Leaders in Health-Promoting Behavior. Sustainability 2017, 9, 1944. https://doi.org/10.3390/su9111944
Jiménez P, Winkler B, Bregenzer A. Developing Sustainable Workplaces with Leadership: Feedback about Organizational Working Conditions to Support Leaders in Health-Promoting Behavior. Sustainability. 2017; 9(11):1944. https://doi.org/10.3390/su9111944
Chicago/Turabian StyleJiménez, Paul, Bianca Winkler, and Anita Bregenzer. 2017. "Developing Sustainable Workplaces with Leadership: Feedback about Organizational Working Conditions to Support Leaders in Health-Promoting Behavior" Sustainability 9, no. 11: 1944. https://doi.org/10.3390/su9111944