Analysis of Travel Decision-Making for Urban Elderly Healthcare Activities under Temporal and Spatial Constraints

School of Transportation, Southeast University, Nanjing 211189, China
*
Author to whom correspondence should be addressed.
Sustainability 2018, 10(5), 1560; https://doi.org/10.3390/su10051560
Submission received: 14 April 2018
/
Revised: 10 May 2018
/
Accepted: 11 May 2018
/
Published: 14 May 2018
(This article belongs to the Section Sustainable Transportation)
Abstract
:This paper explores the travel decision-making process of healthcare behavior of urban elderly under different temporal and spatial constraints. Firstly, based on time geography, a two-dimensional space-time trip chain is applied and the concept of healthcare constraint degree (HCD) is proposed. Then, the elderly’s medical treatment activities are divided into two categories: strong constraint activity and weak constraint activity, based on 625 samples in Kunming, China. Lastly, an improved multinomial logit model is adopted to determine the significant factors affecting the travel mode choice of these two types of activities. The results show that the travel mode choice of the elderly to healthcare facilities is not the same under different spatio-temporal constraints: strong constraint activity is mainly affected by external factors (such as travel time, travel distance, bus station distance and walking accessibility), whereas weak constraint activity is influenced by internal family factors (such as car pick-up, accompanied by family, and the number of family members with a driver’s license). These findings present a new perspective for understanding the healthcare behavior of the elderly and provide a convincing support for the formulation of urban transportation planning policies.
1. Introduction
The aging of societies has become a global phenomenon, especially in developing countries; the elderly population is expected to double its present size by 2025 and one in three persons in the world will be over 65 years of age [1]. With the emergence of this problem, the health of the elderly will become a worldwide challenge; it is necessary to study the health-seeking activities and behaviors of the elderly so that the specific requirements of this population segment are not ignored [2]. The aging of societies is related to many factors; among them, the transportation accessibility is an important factor in the process of medical treatment for the elderly. In particular, urban rapid expansion has resulted in the insufficient growth and the poor accessibility of medical facilities in China, leading to a shortage of basic healthcare services and difficulty in seeking healthcare helps for the urban elderly. Some scholars also suggest that the interaction among various transportation modes and urban space will increase with the accelerated modernization of the city [3]. In this situation, space-time constraints may change individual travel mode choice, resulting in obvious differences in resident behavior patterns, including the differences based on social, economic and spatial backgrounds [3,4]. Therefore, there is urgent need to pay attention to the travel patterns choice related to the healthcare activities of the elderly. A better understanding of travel behaviors within special travel circumstances may allow policy makers to make better decisions on elderly healthcare policy and optimize medical and health service resources for the elderly.
Many studies have examined the healthcare behavior of the elderly and they mainly focused on the attitudes toward the healthcare and the factors influencing the use of healthcare service [5,6]. In the case of the attitudes toward healthcare, Fisher et al. and Fyffe et al. [7,8] concluded that older respondents were less likely to seek the help of professional sources, including help from family or friends as well as services that require lots of physical effort. Diala et al. [9] found that individuals who endorsed negative attitudes toward the treatment were five times less likely to seek mental health services than those with more positive attitudes. As for the factors influencing the decision to seek the treatment, Bessho et al. [10] showed that the health status of the elderly was the main factor affecting medical behavior, and the more serious the elderly health situation was, the more active the elderly was. Borah [11] established a mixed multinomial logit model to explore the choice decision of the healthcare of the elderly by using the data from National Sample Survey Organization of India. The results suggested that price and distance were the greatest barriers in the choice decision of the healthcare. When the health status was poor, the distance played a less significant role, while price elasticity of demand for outpatient care varied with the income, and the low-income groups were more price-sensitive than the high-income ones. Samra et al. [12] applied a binomial logit model to analyze the influencing factors of healthcare for rural residents in India. The results showed that economic income and medical price were significant factors influencing the medical treatment of rural residents, and the distance to treatment was the greatest barrier. Fortney et al. [13] applied a joint choice model to analyze the decision of treatment based on 435 samples in Arkansans. The results showed that insurance coverage and availability significantly impact sector choice, subject-specific case mix factors (such as age, gender, employment status, depression severity, and psychiatric comorbidity) significantly affected the decision of seeking the treatment. In China, healthcare activities and travel behaviors of the urban elderly were examined in few studies. One study focused on demographic characteristics and social structure and selected indicators, designed questionnaires and analyzed the impact of medical insurance and family expenditure on medical demand [14]. Another study analyzed the impact of medical services for the elderly with regard to elderly individuals who were in poor health and need timely medical treatment at a hospital [15].
In addition, temporal and spatial constraints are important methods to study the patterns and decision-making mechanisms of the residents’ daily behaviors [16,17]. Kwan [18] explored gender differences in space-time constraints and their impacts on women’s and men’s activity-travel patterns from a time-geographic perspective. Based on travel data collected in Columbus, time-budget and fixity constraints of three population subgroups were examined, the results suggested that space-time constraints have a significant impact on individual travel choice. Based on the activity-travel diaries and seven-day GPS tracking data of 709 respondents in Beijing, temporal and spatial flexibilities were measured with the degree of variability in time and space of the respondents’ self-reported activities, the spatial and temporal characteristics of residents’ daily activities and their influencing factors were analyzed by Shen and Chai [19]. The results showed that temporal and spatial flexibility varied significantly among different activities, individuals and households; among the influencing factors, the type of activity was the most important factor. Chen and Chai [20] explored the relationship between the flexibility of the entire trip chains on the departure time of commuting trips and tried to verify that if flexible schedules contributed to the rush-hour avoidance. The results showed that flexible activity arrangement had a significant impact on early commuting time decision. In addition, temporal and spatial constraints have also been used in the analysis of resident activities, such as leisure, shopping, employment and commuting [21,22].
As is evident from the above review, there are abundant research results regarding the healthcare of the elderly. However, these explorations focus more on the attitudes and preferences toward the healthcare and they do not reflect the demand for transportation. Besides, although temporal and spatial constraints were used to study the travel behavior in many studies, they neglect that individual’s travel choice will change under different degree of time and space constraints. To fill the above research gap, the objective of this paper is to better understand the factors that influence the healthcare behavior of the urban elderly. First, the concept of the healthcare constraint degree (HCD) for the elderly is proposed based on the concept of temporal and spatial constraints in time geography; in particular, HCD is used to measure the accessibility of medical activities for the elderly. Then, the behavioral characteristics of the elderly are analyzed and healthcare behaviors of the elderly are divided into strong constraint activity and weak constraint activity. Lastly, based on an improved logit model, the factors influencing the travel modes choice under different constraints are discussed. Based on the findings of this current research, related policies for urban traffic can be developed by the government to promote the fair and reasonable development of urban traffic.
The remainder of the paper is organized as follows. Section 2 describes the concept of HCD. The research design and analysis are presented in Section 3. Section 4 provides the principle of the model. Section 5 presents the results. Finally, Section 6 summarizes the policy suggestions and study limitations.
2. Methods
2.1. Healthcare Constraint Degree
Accessibility is usually used to describe individual travel behavior and it is a measure of the difficulty of travel [23]. However, the relationship of the activities in individual trip chain is not considered; therefore, time geography was proposed and developed by Hagerstrand in the late 1960s and this framework focuses on the time and space characteristics of individual behavior under temporal and spatial constraints [24,25]. The framework has two basic concepts: space-time path and space-time prism. The space-time path describes the spatial-temporal trajectories between the starting point and the end point. The space-time prism is determined by the locations of activities, the distances between relevant locations, the amount of time available for travel and activity participation; in space-time prism, the time and space that an individual uses is called time and space resources, while the projection of the three-dimensional space-time prism onto two-dimensional geographical space is called the potential path area (PPA) [26,27]. Following the space-time prism approach, space-time accessibility of an individual can be measured [18].
Time and space resources are limited and not completely free in individual activity path, the movement between stops and the choice of transportation modes. Martino et al. [28] provided a framework of the decision-making mechanism for the choice of activities under time and space constraints and showed that there are many restrictions on individual behavior. It is important to examine healthcare with regard to temporal and spatial constraints because behavioral characteristics and the choice of travel modes differ under different HCDs. This paper explores the factors that influence the choice of transportation mode from the perspective of time and space constraints. We propose the concept of HCD, which is the ratio of the travel time-space resources to the time-space resources consumed in the healthcare activity. HCD illustrates the characteristics of urban elderly healthcare behavior and reflects the mobility and accessibility of the healthcare for the elderly.
2.2. Concept of HCD
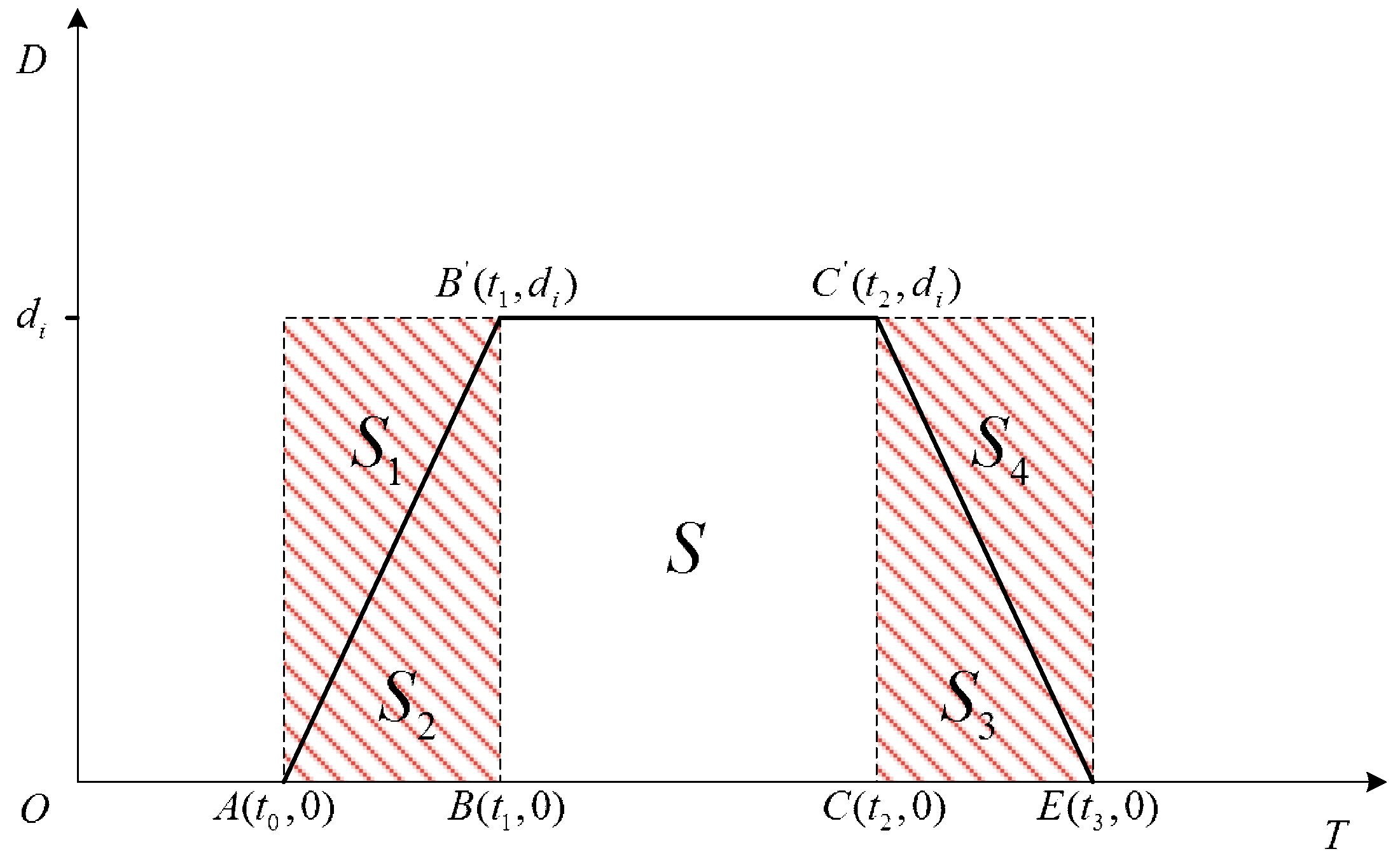
The more time and space resources consumed in healthcare activities, the less resources consumed in other activities, thus individual travel behavior characteristics are also affected. To accurately describe the meaning of HCD, a two-dimensional space-time trip chain of healthcare activities is applied to measure healthcare constraints, as shown in Figure 1.
In Figure 1, individual starts at the origin (home) at moment to reach the destination (hospital) at moment . The time and space resources available by transportation from to can be written as follows:
where is the available time and space resources from home to the hospital, is a potential loss opportunity due to travel time and space constraints (from home to the hospital), and is the space-time resources consumed by the individual (from home to the hospital) utilizing the mode of travel.
Similarly, the time and space resources consumed by an individual’s travel that starts at (hospital) to (home) can be written as:
where is the available time and space resources from the hospital to home, is the space-time resources consumed by the individual (from hospital to home) utilizing the mode of travel, and is the potential loss opportunity due to travel time and space constraints (from the hospital to home).
Then, individual participates in healthcare activity , which starts at (home), stops at (hospital) and (hospital), and returns to (home). The time and space resources consumed by healthcare can be expressed as:
where is the time and space resources consumed by the entire healthcare activity and represents the time and space resources consumed by the individual in the hospital for healthcare. Therefore, HCD can be written as follows:
where is the HCD of an individual in healthcare activity, which is used to measure individual healthcare accessibility under the influence of healthcare constraints.
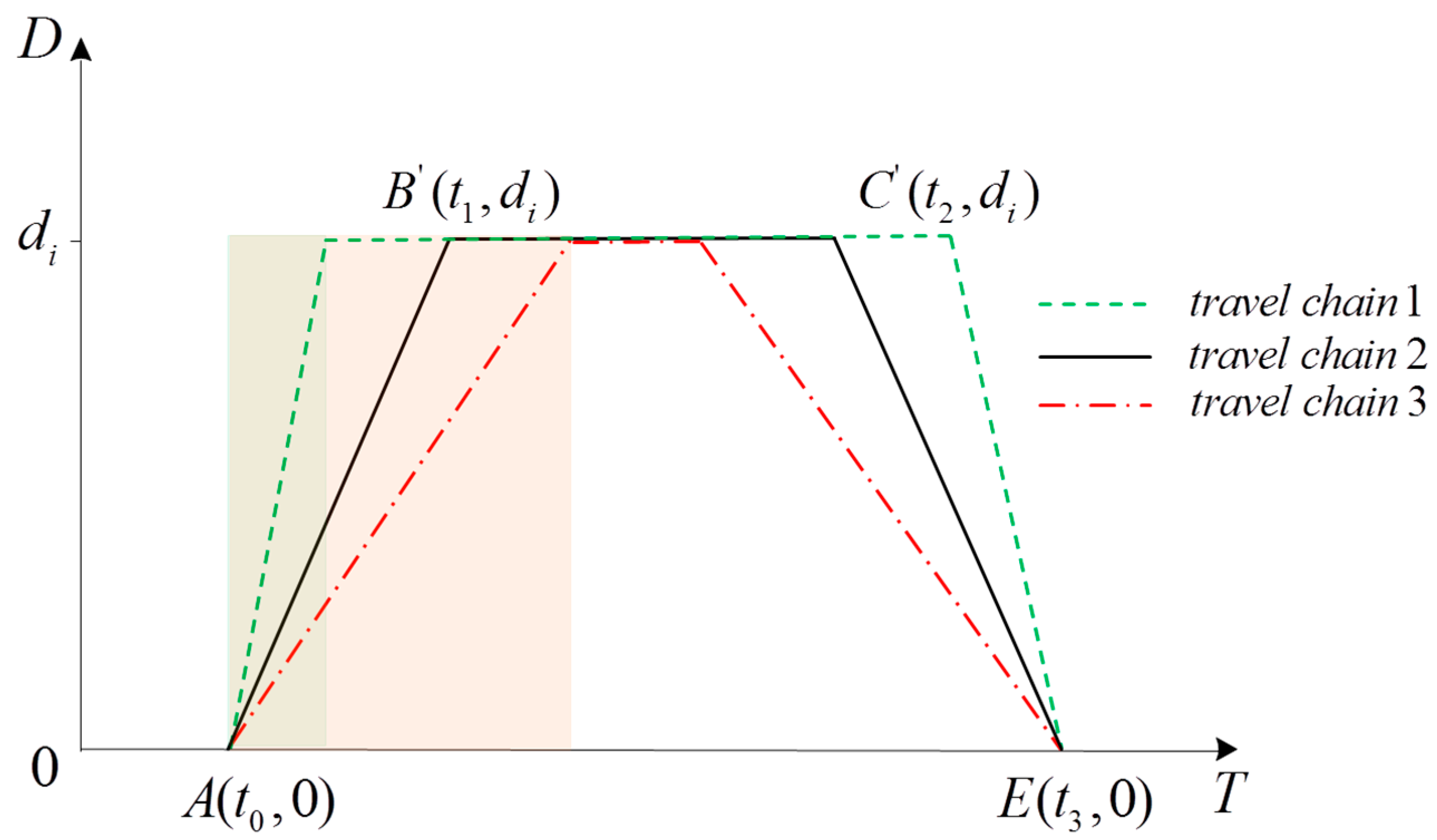
As shown in Figure 2, as the travel chain is changed from 1 to 2 and then to 3, available time and space resources between the hospital and home become larger, the space resources consumed by the entire healthcare activity become smaller, and, according to the Formula (4), the HCD become larger. In the actual trip, i.e., during travel, if the time-space resource is certain, the resource between the hospital and home link becomes larger, and the corresponding resource for medical services is reduced, therefore the mobility and accessibility of the medical service decrease, and, correspondingly, the constraints of the medical activities of the elderly increase.
3. Research Design and Analysis
3.1. Questionnaire Design
This study aimed to explore the healthcare behavior of the urban elderly under different degrees of constraint. Therefore, the respondents were urban elderly individuals over the age of 60. Based on the real situation and the elderly’s attributes as well as preference, we examined the real demand for healthcare behaviors under different degrees of constraint. The questionnaire was divided into four parts: personal attributes, healthcare demands, and the characteristics of healthcare and travel ability.
- (1)
- Personal attributes included sex, age, educational background, occupation, personal monthly income, living condition and medical insurance.
- (2)
- The characteristics of the demand for healthcare included types of diseases, medical facilities, waiting time for a healthcare service, medical charges, accessibility of medical treatment, and purpose of travel.
- (3)
- The characteristics of healthcare activities included the medical facilities, the consumption of entire healthcare activities, any accompaniment by a family member, the mode of travel, the distance of travel, travel time and travel frequency.
- (4)
- Travel ability included walking time and the time waiting for a bus.
3.2. Data Source
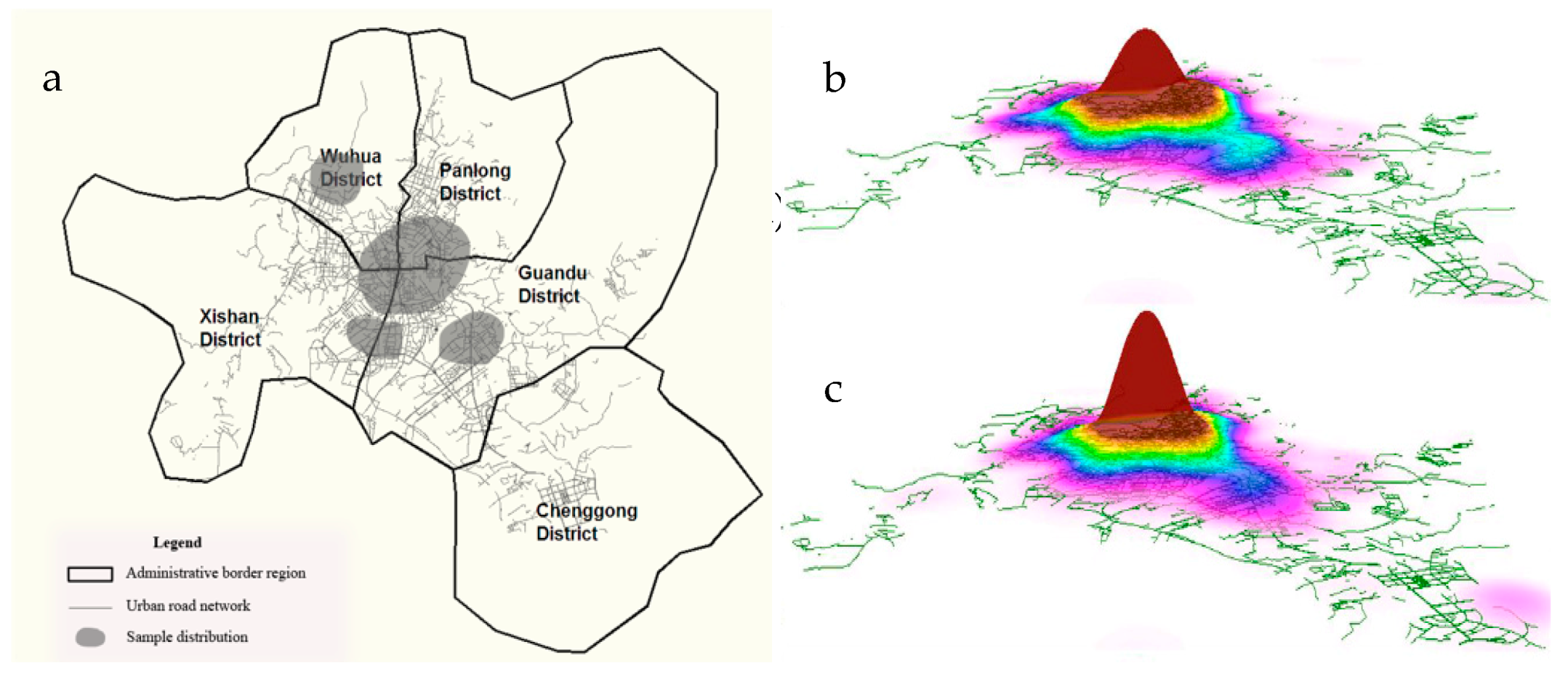
Four districts were investigated by stratified random sampling method: Wuhua, Panlong, Guandu and Xishan districts (Figure 3a). To select the sample, on the one hand, to ensure the balance and representativeness of the sample, the distribution of the sample proportion was made according to the occupation of the elderly before retirement. On the other hand, according to the number of hospitals in four districts, the proportion of investigators was allocated and data were collected in a single pen-and-paper interview at home or in hospitals to ensure the quality of the questionnaire. Additionally, GPS data from residents were used and visual analysis was conducted in GIS [29]. The results are shown in Figure 3b,c. Figure 3b is the morning peak, while Figure 3c is the evening peak. In the figure, we can clearly see that closer to the city center has a higher peak in the image, that is, the traffic is more congested (the study area is mainly urban centers).
To implement the questionnaire survey, firstly, a preliminary survey was conducted in one district in the intermediate zone, Wuhua district, which has a large elderly population. In total, 130 questionnaires were issued and 120 questionnaires were valid. Then, the real questionnaire survey time was 5–15 January 2017. In the process of the survey, the elderly was explained to answer the questionnaire as for a medical travel and the travel should not include any other activity. Finally, a total of 693 questionnaires were investigated, and 625 valid questionnaires were recovered with an effective rate of 90.1%. According to the survey data, the results show that the sample size is balanced among four districts; the ratios of male and female are 49.40% and 50.60%; the education level is relatively low, with only 18.6% having a university degree or above; healthcare is needed approximately 1.56 times a month; the elderly driver’s license rate is only 17%; 89% of the elderly purchase medical insurance; and approximately 73.6% of elderly patients need family accompaniment for healthcare. These findings not only show the characteristics of healthcare activities of the elderly, but also reflect that the healthcare activities of the elderly have a certain impact on urban transportation systems.
3.3. Data Analysis
3.3.1. Transportation Structure of Healthcare
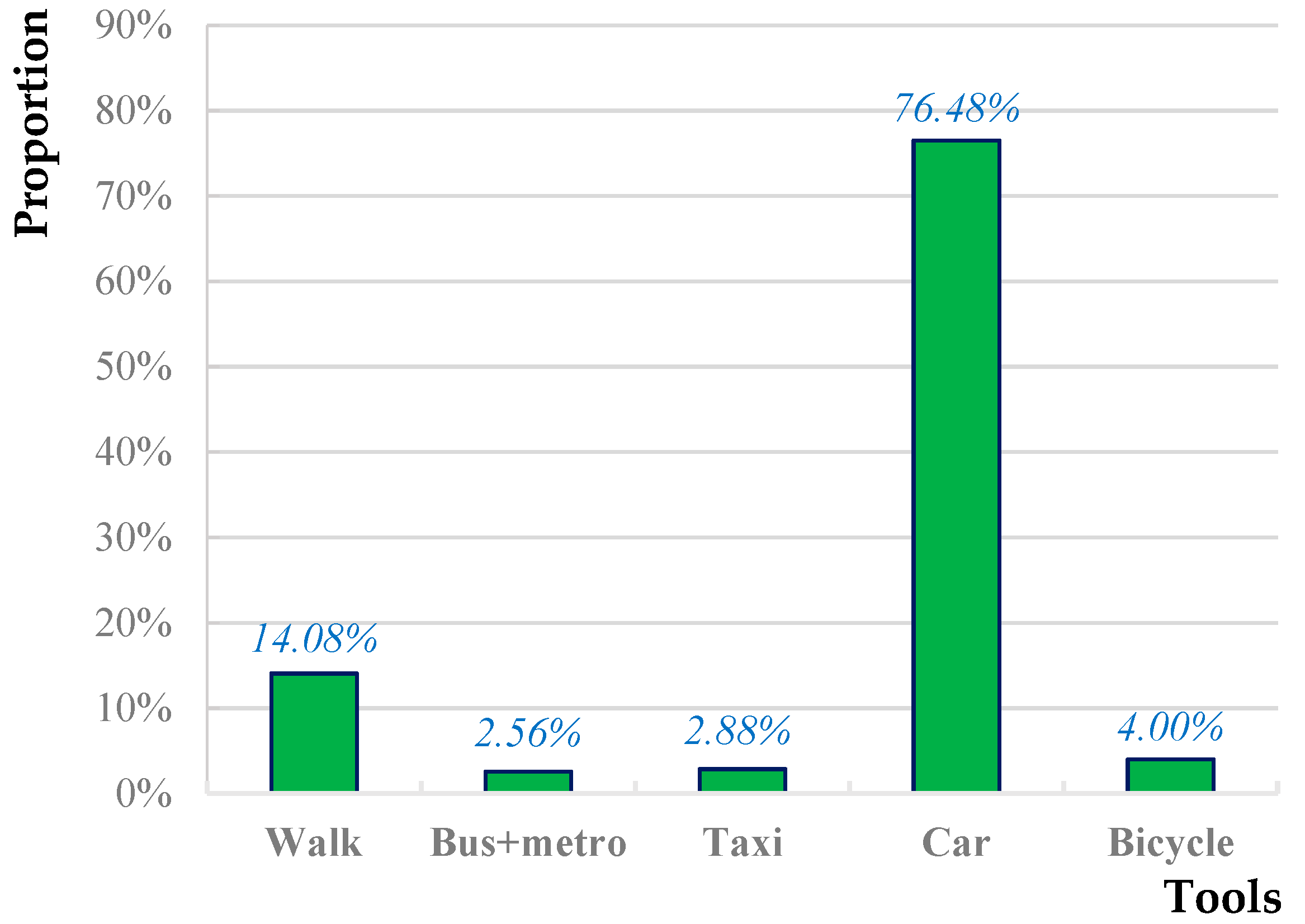
According to the questionnaire analysis, in the process of medical treatment, car is the main mode of travel, with a proportion of 76.48%, whereas the proportion of public transport (bus and metro) was only 2.56%, as shown in Figure 4. This may be because elderly healthcare activities often occur in the rush hour, and, during this period, the delay rate of the bus is high. In addition, crowded bus and metro lead to decreased comfort and satisfaction. Besides, the metro is not been free for the elderly, therefore, to a certain extent, the willingness to use the metro for the elderly is also reduced. On the contrary, the car can provide the door-to-door services and this travel mode is in line with the demand for healthcare and the elderly are more likely to use it.
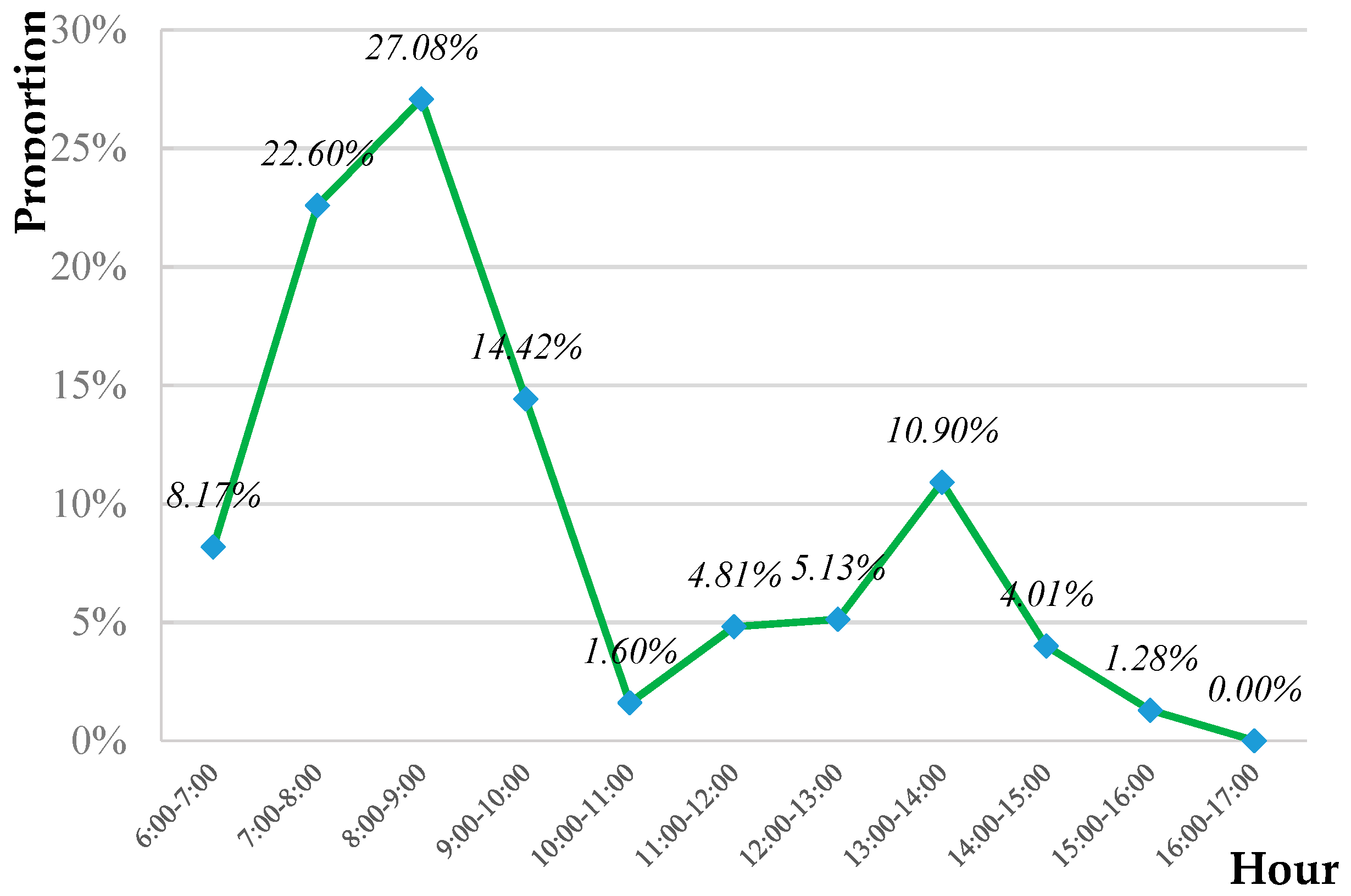
3.3.2. The Characteristics of Healthcare Time
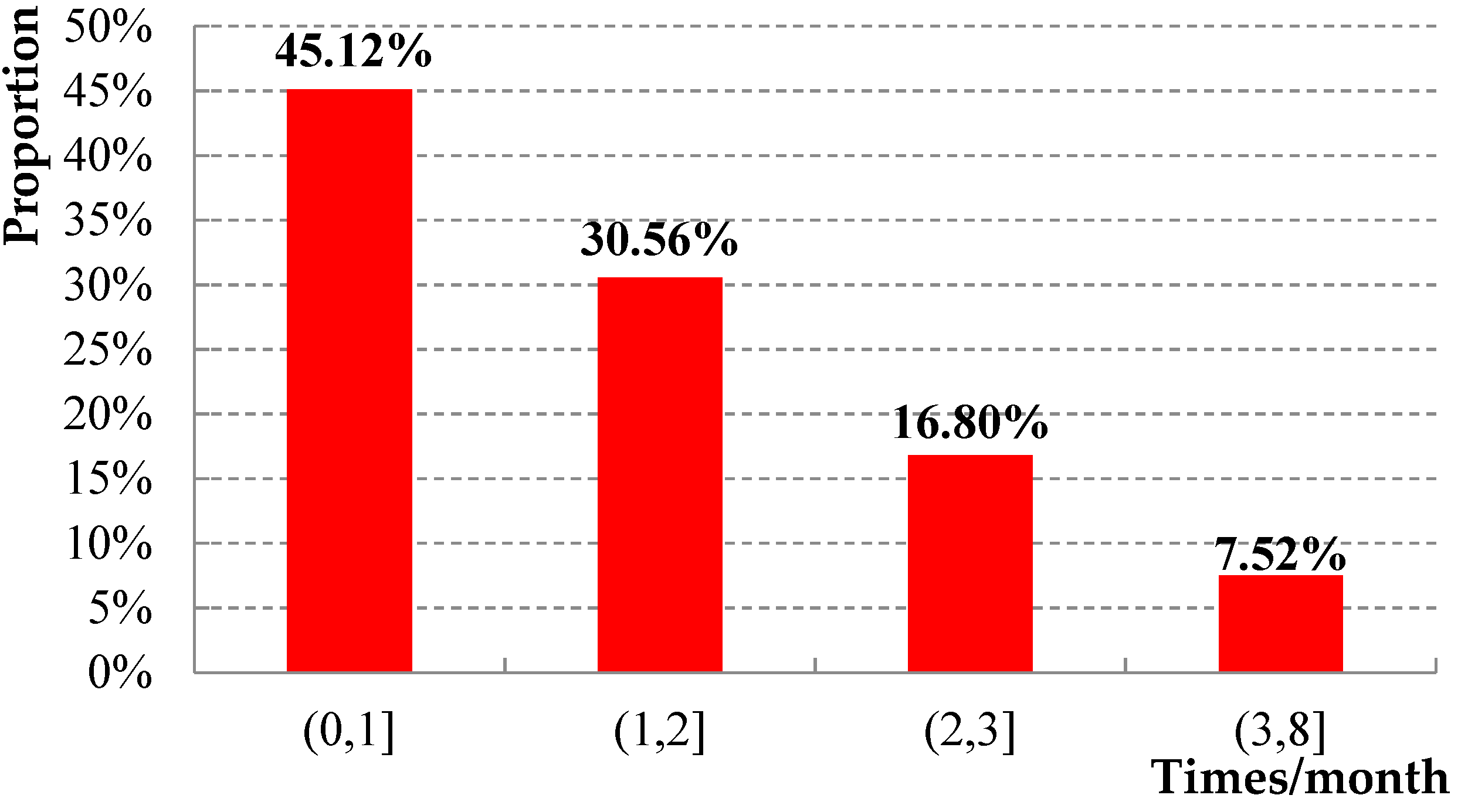
Travel time is mainly concentrated in the urban morning rush hour, from 7:00 to 9:00, with a proportion of 49.68%, as shown in Figure 5. This part of the elderly mostly traveled by car, therefore, elderly healthcare activities have a certain impact on urban traffic. We suspect that the reason may be the following: in China, owing to the limitation of the medical level, not all patients have an early appointment, and, if the patient goes to the hospital directly without an appointment, he/she usually needs to queue for a long time, the whole process needs to take a certain amount of time, thus the elderly choose to visit the doctor as early as possible. Additionally, according to the statistics, for the healthcare duration, the ratio is 45.12% within an hour, and the proportion for 1–2 h is 30.56%, as shown in Figure 6. In addition, the frequency is 1.37 times a month, the proportion of accompanying family members on the trip is 73.76%, and the travel mode mainly relies on the car during rush-hour. These findings indicate that medical travel of the elderly has become a non-ignorable part of city transportation and also affects family activities to a certain extent.
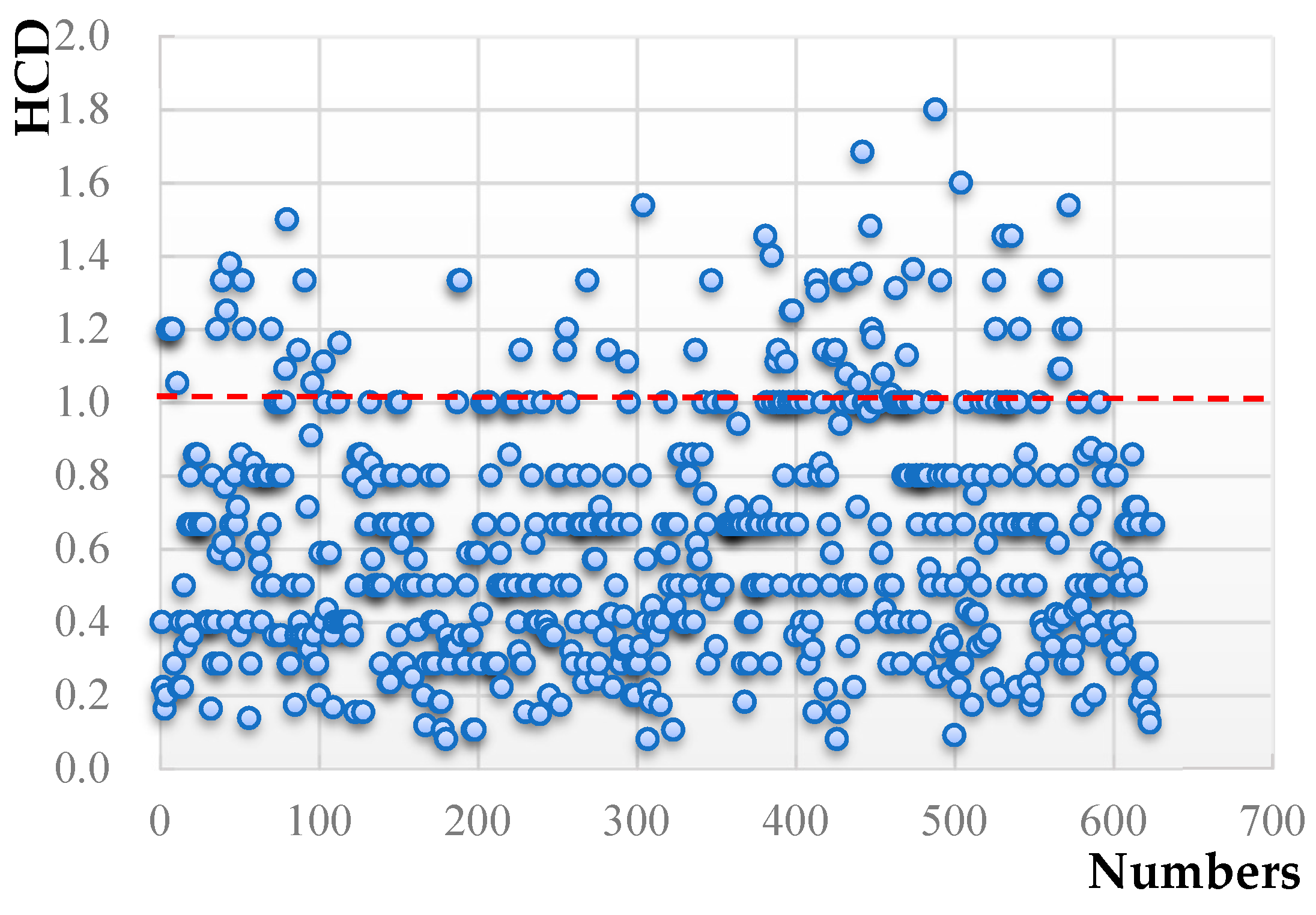
3.3.3. Healthcare Constraint Degree Measurement
HCD describes the accessibility of an individual under the influence of time and space and it is also a measure of the degree of freedom of personal medical activities and travel behaviors. According to the definition of HCD and its mathematical expression, the calculation value of HCD in the surveyed area is 0.63, which shows that the whole area is relatively favorable. However, there are still some elderly who encounter healthcare difficulties. As for the calculation results, the healthcare activities of the elderly are divided into two categories: strong constraint activity () and weak constraint activity (), as shown in Figure 7. When the HCD is greater than 1 (20.8%), it implies that the time and space resources spent by traffic between the hospital and home link exceed the time and space resources spent by the healthcare activity itself, and the accessibility of the healthcare for the elderly is poor. In contrast, the accessibility of the healthcare for the elderly is comparable better when the HCD is less than 1. The different activities have different effects on urban traffic; to formulate appropriate policies for the elderly, it is necessary to further explore the behavior choice mechanism of urban elderly under different types of activities.
4. Modeling Travel Mode Choice
4.1. Improved Logit Model
Domencich and McFadden, as well as Williams, have studied discrete choice based on the random utility theory. Under specific condition, the traveler selects the maximization of utility [30]. The multinomial logit model may be derived within a random utility framework, in which the utility , derived by the individual from the choice, can be written as:
where is a random error term, is the set of independent variables, and is a vector of unknown parameters.
The random term in Equation (5) obeys the double exponential distribution, and the probability that the individual will choose the mode of travel can be written as:
where equals the probability that a tourist with characteristics chooses the category of the dependent mode choice variable [31]. Based on the theory of time geography, individuals are mainly limited by time and space in the travel, thus, the choice of different travel modes is mainly influenced by the time and travel distance, and travel utility can be expressed as follows:
In Equation (7), , and are the parameters to be estimated and and are individual choices of travel mode, which need to consume travel distance and time. Combining Equations (6) and (7), the result can be expressed as:
However, the above model is still complex in the actual operation and we generally use the NerlovePress model to express . We regard and in Equation (8) as equivalent. Comparing the two travel modes of and , we can acquire the linear regression model shown by Equation (9):
where is the ratio of the selection probabilities between two alternative transportation modes and represents the superiority of an individual’s selection of mode relative to .
The model estimation was performed using statistical analysis system (SAS) simulation software. The stationary distribution of the estimation results reported in this paper was tested in several ways: (1) The maximum likelihood estimation method (MLE) for the preliminary 300 sample data simulated the maximum likelihood operator [32]. After many tests, the calibration result is convergent. (2) The trace plot and correlation in each parameter chain were checked. All results of the above methods show that the model reported in this paper converged.
4.2. Calibration of Influence Variables
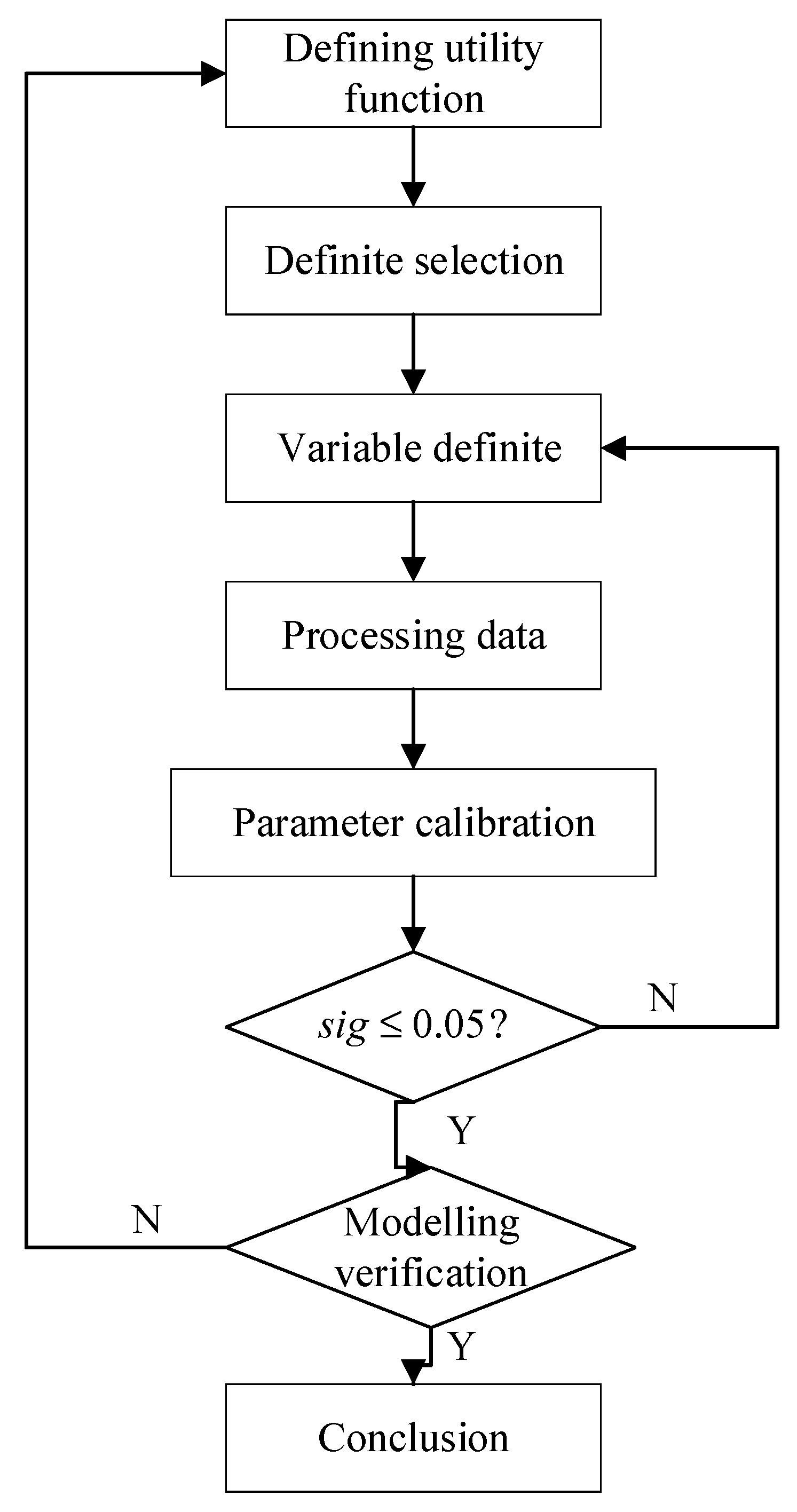
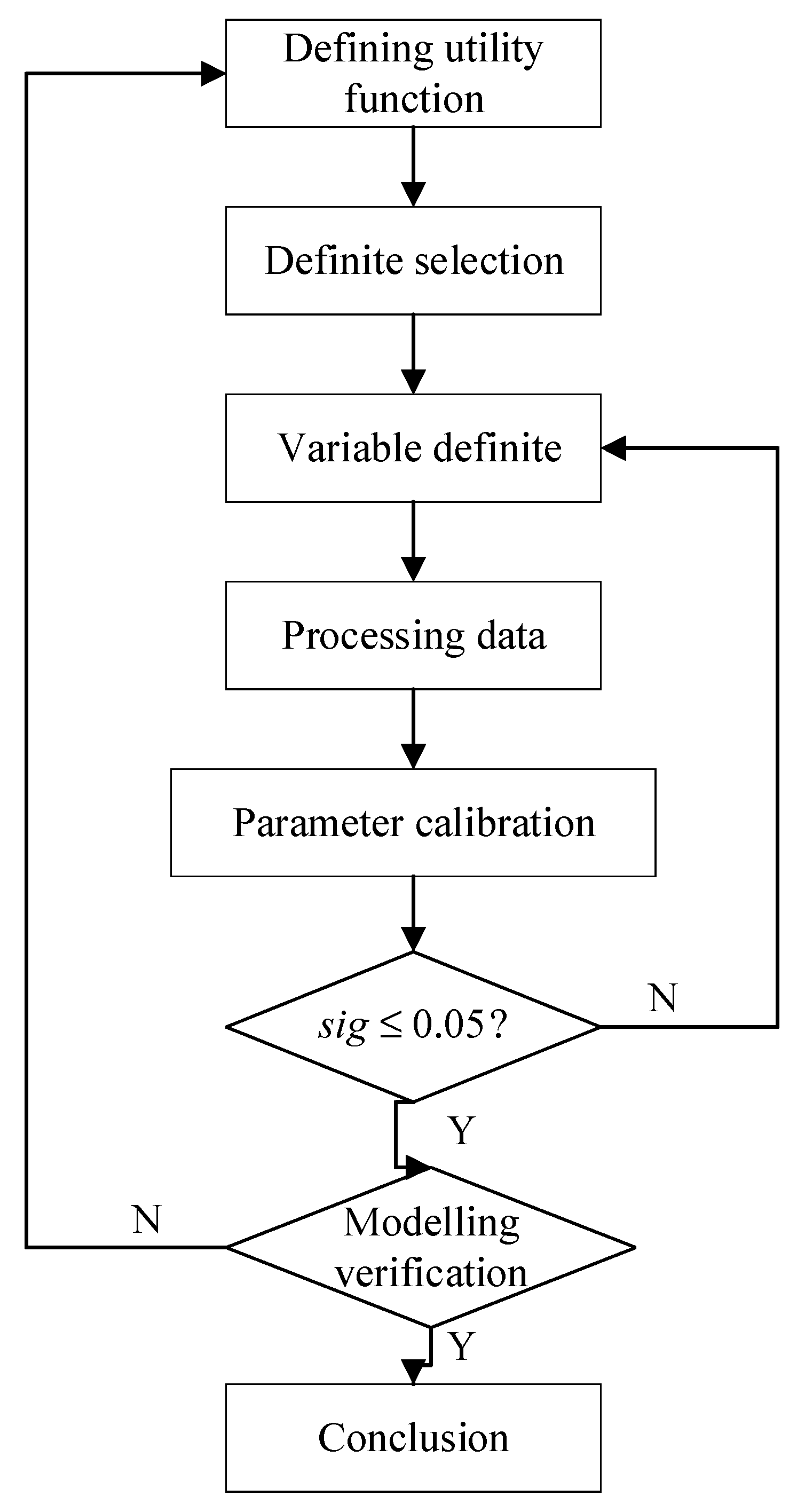
According to the results of the survey, the main travel modes for the elderly to seek healthcare are walking, bus, metro, taxi, car and bicycle. Because bus and metro accounted for small proportions and they both belong to the urban public transport category, this article combines the two modes for simplicity and convenience. The main factors that influence the travel mode choice of elderly patients can be divided into personal attributes, family attributes, and trip attributes. To explore the behavior choice mechanism of urban elderly under different constraints, two independent multinomial logit models are constructed by selecting dependent variables of traffic modes under different constraints. We analyzed the collinearity features of independent variables and then divided them into further categories and notes, as shown in Table 1. The calculation process of the model is shown in Figure 8.
5. Results and Discussion
5.1. Model Result
The model analyzed the modes choice of urban elderly in healthcare activities under strong constraint and weak constraint. The bicycle is regarded as reference category, and introducing probability of 0.05 and rejecting probability of 0.1 are obtained. Independent variables and results of significance tests are listed in Table 2 and Table 3. From the statistical theory, a value of significance less than 0.05 based on a confidence interval of 95% indicates that the variable has a significant effect on the selection result and should be retained. After selecting variables according to SAS, the variables that affect modes choice are screened out. In addition to evaluating each feature variable by significance separately, chi-square, McFadden, Nagelkerke R Square, Cox and Snell and other parameters are selected to evaluate the model. According to statistical theory, McFadden coefficients are 0.745 and 0.67 (more than 0.2) and Nagelkerke R Square, Cox and Snell and chi-square values are all in a reasonable range, thus proving that the model is preferable.
5.2. Model Discussion
When the type of healthcare activity is under a strong constraint, gender is positive to walking and negative to bus + metro and car, and for walking. This shows that elderly males are 4.30 times more likely to travel by walking than elderly females, and females are more likely to travel by bus + metro and car than males. This might be because females are less physically active than males. Travel time is negative to walking and bus + metro while it is positive to taxi and car. If travel time is increased by a level, the probability of walking is and bus + metro is , which shows that the willingness to travel by walking and public transportation is reduced while the probability of choosing taxi and car increase with the increase of the travel time. This might be because the increase of travel time makes the elderly become physically exhausted, the possibility of selecting walking is reduced correspondingly. At the same time, the punctuality rate of current Chinese public transport is low, which would affect the appointment time for medical treatment. The influence of travel distance on walking is negative, while the influence is positive on taxi and car. The influence of travel distance on public transport is not significant. The likely reason is that older people do not care about the travel distance, the stations and travel time are often the concerns. The distance from a bus station has a negative impact on walking and public transport, whereas the impact on cars is positive. This might be because, when the origin of the elderly is not within the service range of a bus station, the elderly will not transfer to take public transport for travel but choose a car instead. The frequency of healthcare has a positive effect on walking and a negative effect on public transport, taxis and cars. This might because the elderly is more sensitive to transportation costs, and tend to walk to save money if the frequency of the medical treatment is high. Walkability is positively related to travel by walking, whereas it is negatively related to public transport, taxis and cars. It indicates that the elderly is more likely to walk when the destination is within the walking distance.
When the type of healthcare activity is under a weak constraint, age has a negative effect on walking and a positive effect on public transportation, taxis and cars. This finding shows that, with the increase of the age, the elderly is less willing to seek healthcare by walking and is more inclined to choose cars, which are more flexible and convenient in reducing the travel time and the space constraints. According to the severity of the disease, the medical purpose is divided into three levels: take medicine, physical examination and treatment. The results show that the purpose of healthcare has a negative influence on the public transportation and a positive influence on other modes of transportation. If the severity of the disease is increased by a level, the probability of public transportation is , that is, the probability of choosing public transportation is reduced by 0.58 times. This may be because the healthcare activities of the elderly often occur during rush hour and, during this period, the bus punctuality rate cannot be guaranteed and the environment in a bus is too crowded. With the increase of the severity of the disease, the elderly is more inclined to use more comfortable and punctual travel modes, such as taxis or cars. Car pick-up has a positive effect on car and a negative effect on other modes of travel. This may be because, in China, the families of the elderly often pick them up, not only to reduce the time of the travel but also to care for them. The impact of travel distance on walking and public transport is negative, whereas it is positive for taxis and car. When the travel distance is increased by a level, the probabilities of walking, public transportation, taxis and cars are 0.19, 0.76, 4.17 and 12.67, respectively. This finding shows that, with the increase of travel distance, taxis and cars are preferred to walking and public transportation. Healthcare time is negatively related to walking and positively related to bus + metro, taxi, and cars. Thus, the shorter the time required for healthcare, the more likely the elderly choose walking. Family accompany has a negative effect on walking and public transportation and a positive effect on taxis and cars. This finding shows that they will choose the car as the main mode of travel when people travel with their families. The number of family members with driver’s licenses has a positive impact on car and a negative impact on other modes of transportation. Thus, with the increase in the number of family drivers, the travel possibility of relying heavily on cars sharply increases.
Comparing the two different types of healthcare activities, we find that these two types of activities are both affected by time and space. However, other factors show distinct differences. The strong constraint of healthcare activity for the elderly is mainly affected by external factors, such as travel time, travel distance, bus station distance and walking accessibility. The weak constraint of healthcare activity for the elderly is influenced by family internal factors, such as car pick-up, family accompaniment, and the number of family driver’s licenses. The reasons for weak constraints are the depletion of the temporal resources of other members in the family, another reason is that the flexibility of cars reduces spatial and temporal constraints.
6. Conclusions
In this current paper, the concept of HCD based on spatio-temporal constraints is proposed. The main purpose of this work is to explore the behavior choice mechanism of urban elderly under different HCDs. Based on the behavior data of the elderly in Kunming, the influencing factors of the healthcare activities of the elderly were verified under strong constraint and weak constraint. We draw the following conclusions: (1) Medical travel of the elderly has become a non-ignorable part of city transportation and affects family activities to a certain extent. (2) The strong constraint of elderly healthcare activity is mainly affected by external factors, such as travel time, travel distance, bus station distance and walking accessibility, whereas the weak constraint is influenced by family internal factors, such as car pick-up, family accompaniment, and the number of family driver’s licenses. Therefore, the healthcare demand of the elderly should not only be adjusted to the family internal activity model to reduce the constraints but also should be accompanied by better-quality urban transportation systems to meet the demand of medical care.
As mentioned above, some policy interventions are discussed to reduce the restriction degree of medical treatment for the elderly and improve the accessibility and convenience of medical treatment. Firstly, the spatial distribution of medical facilities should be balanced to give full play to the radiation effect of the medical facilities. At the same time, the level of medical facilities and service level in the peripheral area of the city should be improved, while the gap of medical service quality should be reduced. Secondly, the medical appointment service can be realized. A reasonable arrangement of the time for the elderly can not only alleviate the pressure of the medical facilities, but also avoid the rush hour travel in the city. It also helps family members arrange their time reasonably and avoid conflict with each other. Finally, special vehicles for the healthcare can be opened at a specific time in a day, which makes the elderly’s medical activities more convenient and safe, and is also an important reflection of the traffic equity.
Recently, free floating bike sharing (FFBS) has become increasingly prevalent in major Chinese cities; some elderly people have begun to use this new mode of transportation. The issues presented in this paper are of growing importance given that FFBS will increase in the future, and more studies can consider this mode of transportation for the growing demand for the healthcare of the elderly.
Author Contributions
Y.Z. and X.L. conceived and designed the experiments; X.L. performed the experiments; X.L. and analyzed the data; M.D. revised the English of this paper; X.L. contributed reagents/materials/analysis tools; and X.L. wrote the paper. X.L. and Y.Z. contributed equally to this work.
Funding
This research was funded by [National Natural Science Foundation of China] grant number [71372198], [Science and Technology Department of Jiangsu Province of China] grant number [BY2015070-25].
Acknowledgments
We are grateful for valuable improvement suggestions from the editor, anonymous reviewers and our colleagues.
Conflicts of Interest
The authors declare no conflict of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
References
- Rosenbloom, S. Sustainability and automobility among the elderly: An international assessment. Transportation 2001, 28, 375–408. [Google Scholar] [CrossRef]
- Alsnih, R.; Hensher, D.A. The mobility and accessibility expectations of seniors in an aging population. Transp. Res. Part A 2003, 37, 903–916. [Google Scholar] [CrossRef]
- Acker, V.V.; Goodwin, P.; Witlox, F. Key research themes on travel behavior, lifestyle, and sustainable urban mobility. Int. J. Sustain. Transp. 2016, 10, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Scheiner, J. Social inequalities in travel behaviour: Trip distances in the context of residential self-selection and lifestyles. J. Transp. Geogr. 2010, 18, 679–690. [Google Scholar] [CrossRef]
- Fernándezolano, C.; Hidalgo, J.D.; Cerdádíaz, R.; Requenagallego, M.; Sánchezcastaño, C.; Urbistondocascales, L.; Oteropuime, A. Factors associated with health care utilization by the elderly in a public health care system. Health Policy 2006, 75, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Owens, G.M. Gender differences in health care expenditures, resource utilization, and quality of care. J. Manag. Care Pharm. 2008, 14, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Fisher, L.J.; Goldney, R.D. Differences in community mental health literacy in older and younger Australians. Int. J. Geriatr. Psychiatry 2003, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Fyffe, D.C.; Brown, E.L.; Sirey, J.A.; Hill, E.G.; Bruce, M.L. Older Home-Care Patients’ Preferred Approaches to Depression Care: A Pilot Study. J. Gerontol. Nurs. 2008, 34, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Diala, C.; Muntaner, C.; Walrath, C.; Nickerson, K.J.; Laveist, T.A.; Leaf, P.J. Racial Differences in Attitudes Toward Professional Mental Health Care and in the Use of Services. Am. J. Orthopsych. 2000, 70, 455–464. [Google Scholar] [CrossRef]
- Bessho, S.; Ohkusa, Y. When do people visit a doctor? Health Care Manag. Sci. 2006, 9, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Borah, B.J. A mixed logit model of health care provider choice: Analysis of NSS data for rural India. J. Health Econ. 2006, 15, 915–932. [Google Scholar] [CrossRef] [PubMed]
- Sarma, S. Demand for outpatient healthcare: Empirical findings from rural India. Appl. Health Econ. Health Policy 2009, 7, 265. [Google Scholar] [CrossRef] [PubMed]
- Fortney, J.; Rost, K.; Zhang, M. A joint choice model of the decision to seek depression treatment and choice of provider sector. J. Med. Care 1998, 36, 307. [Google Scholar] [CrossRef]
- Zeng, Y.; Vaupel, J.W.; Xiao, Z.; Zhang, C.; Liu, Y. The Healthy Longevity Survey and the Active Life Expectancy of the Oldest Old in China. Popul. Engl. Sel. 2001, 13, 95–116. [Google Scholar]
- Liu, G.; Cai, C. Medical Insurance and Medical Care Demand for the Elderly in China. Econ. Res. J. 2011, 46, 95–107. [Google Scholar]
- Buliung, R.N.; Roorda, M.J.; Remmel, T.K. Exploring spatial variety in patterns of activity-travel behaviour: Initial results from the Toronto Travel-Activity Panel Survey (TTAPS). Transportation 2008, 35, 697. [Google Scholar] [CrossRef]
- Raubal, M.; Miller, H.J.; Bridwell, S. User-Centred Time Geography for Location-Based Services. Geografiska Annaler 2010, 86, 245–265. [Google Scholar] [CrossRef]
- Kwan, M.-P. Gender differences in space-time constraints. Area 2000, 32, 145–156. [Google Scholar] [CrossRef]
- Shen, Y.; Chai, Y. Space-time flexibility of daily activities and gender differences: A case study of Beijing. J. Acta Geogr. Sin. 2017, 72, 2214–2225. [Google Scholar]
- Chen, Z.; Chai, Y. Modelling the Choice of Departure Time for Commuting Trip Chains Incorporating Space-Time Flexibility Variables: Evidence from the Shangdi-Qinghe Area of Beijing. J. Urban Dev. Stud. 2014, 21, 65–76. [Google Scholar]
- Buliung, R.N.; Kanaroglou, P.S. Urban Form and Household Activity-Travel Behavior. Growth Chang. 2006, 37, 172–199. [Google Scholar] [CrossRef]
- Cervero, R. Built environments and mode choice: Toward a normative framework. Transp. Res. Part D Transp. Environ. 2002, 7, 265–284. [Google Scholar] [CrossRef]
- Geurs, K.T.; Wee, B.V. Accessibility evaluation of land-use and transport strategies: Review and research directions. J. Transp. Geogr. 2004, 12, 127–140. [Google Scholar] [CrossRef]
- Hägerstraand, T. What about people in regional science? Pap. Reg. Sci. Assoc. 1970, 24, 6–21. [Google Scholar] [CrossRef]
- Lenntorp, B. Paths in Space-Time Environments: A Time-Geographic Study of Movement Possibilities of Individuals; Lund Studies in Geography; Royal University of Lund: Lund, Sweden, 1976; p. 44. [Google Scholar]
- Kim, H.M.; Kwan, M.P. Space-time accessibility measures: A geocomputational algorithm with a focus on the feasible opportunity set and possible activity duration. J. Geogr. Syst. 2003, 5, 71–91. [Google Scholar] [CrossRef]
- Miller, H.J.; Wu, Y.H. Gis software for measuring space-time accessibility in transportation planning and analysis. Geoinformatica 2000, 4, 141–159. [Google Scholar] [CrossRef]
- Martino, S.D.; Bimonte, S.; Bertolotto, M.; Ferrucci, F.; Leano, V. Spatial OnLine Analytical Processing of Geographic Data through the Google Earth Interface; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Liu, Y.; Ji, Y.; Liu, Q.; He, M.; Ma, X. Escorting Mode Choice for Children’s School Trip Considering E-Bikes: A Case Study in Kunming, China. Transp. Res. Rec. J. Transp. Res. Board. 2017, 2634, 8–16. [Google Scholar]
- Mcfadden, D.; Train, K.; Tye, W.B. An application of diagnostic tests for the Independence from Irrelevant Alternatives property of the multinomial Logit model. Transp. Res. Rec. 1978, 637, 39–45. [Google Scholar]
- Greene William, W.H. Econometric Analysis, 4th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 1977. [Google Scholar]
- Littell, R.C.; Milliken, G.A.; Stroup, W.W.; Wolfinger, R.D.; Littell, R.C.; Milliken, G.A.; Stroup, W.W.; Wolfinger, R.D. SAS System for Mixed Models. Technometrics 1996, 39. [Google Scholar] [CrossRef]
Figure 1.
Two-dimensional space-time travel chain of healthcare.
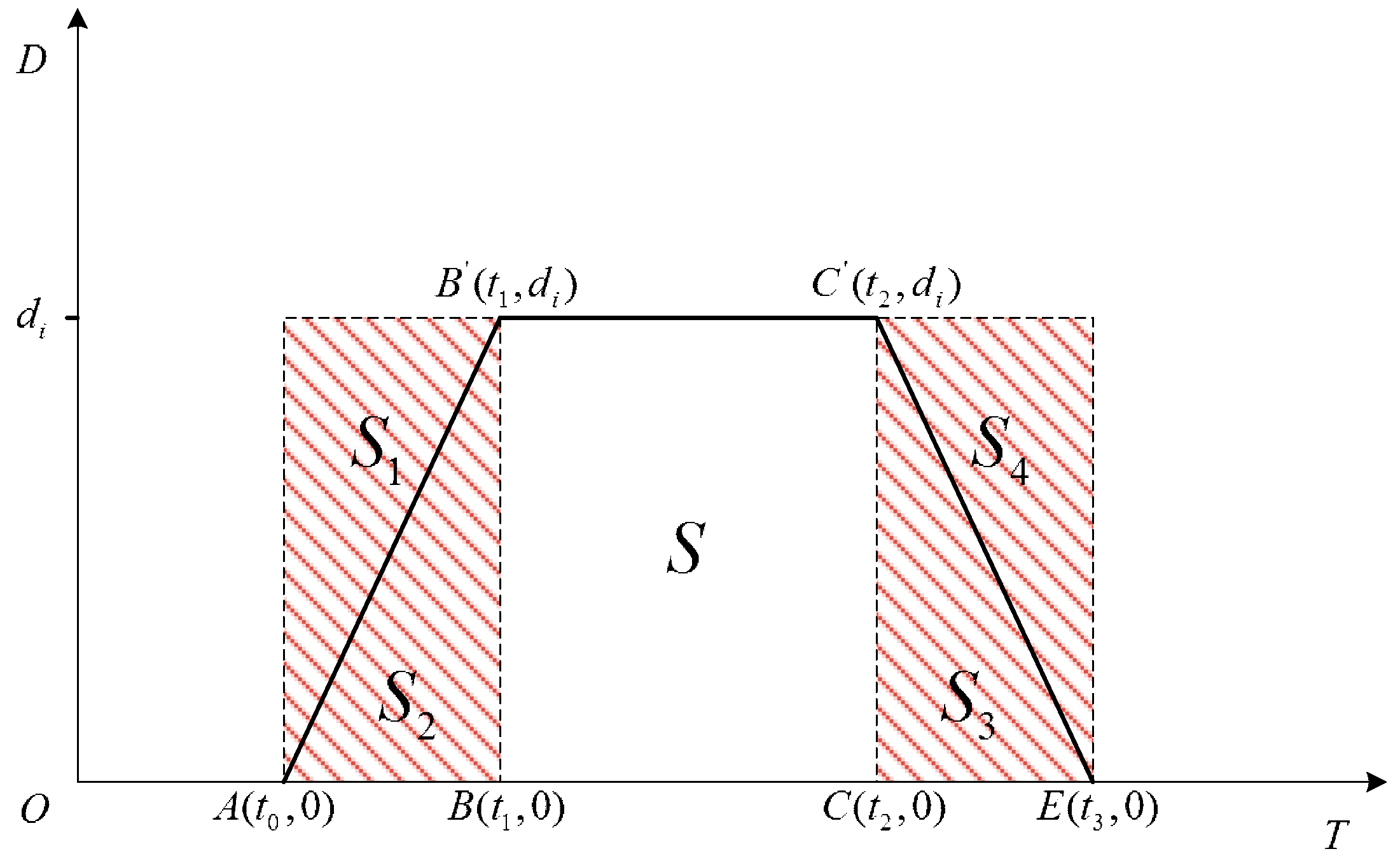
Figure 2.
The change of HCD in travel chain of healthcare.
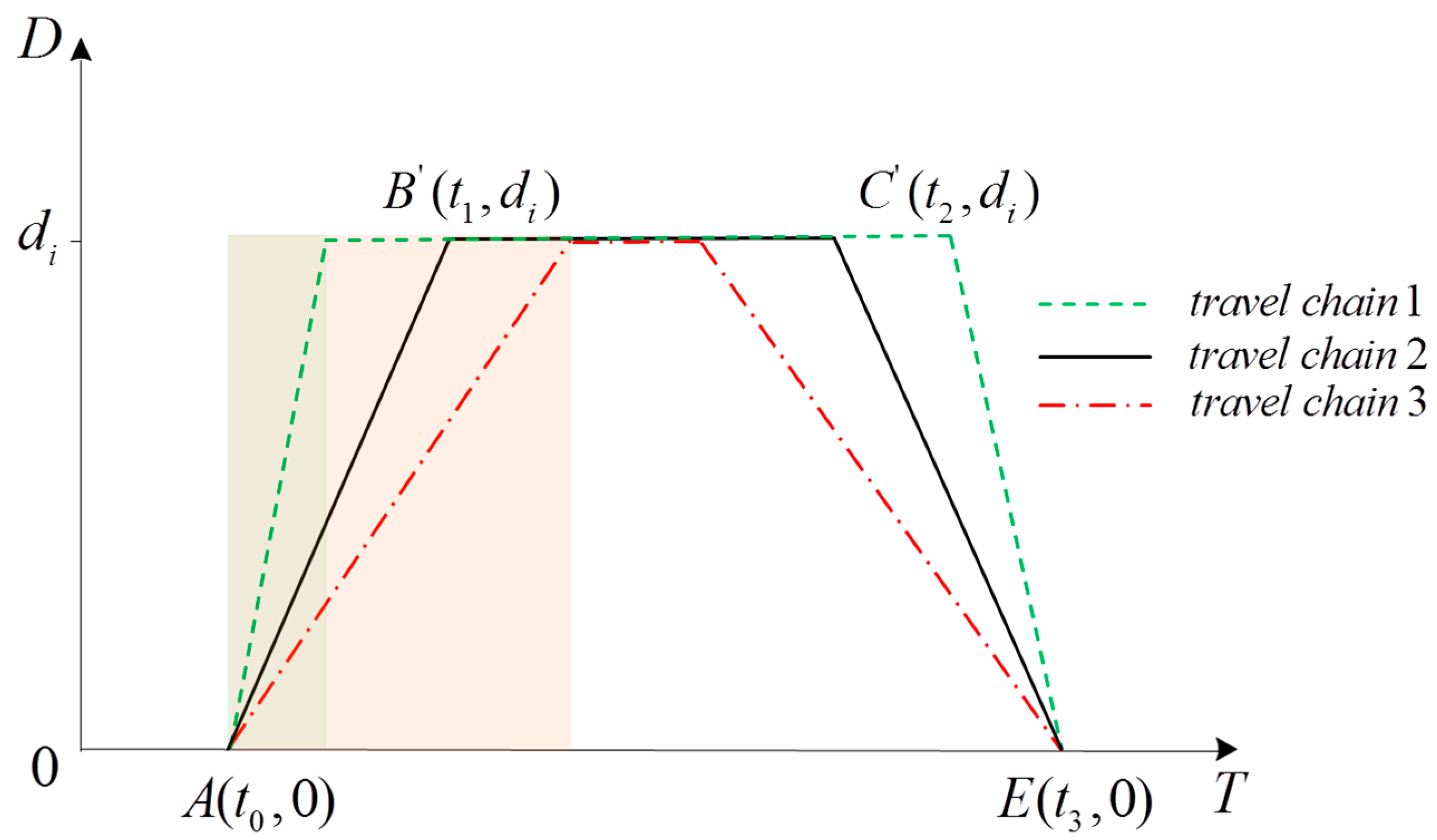
Figure 3.
Study area and peak hours.
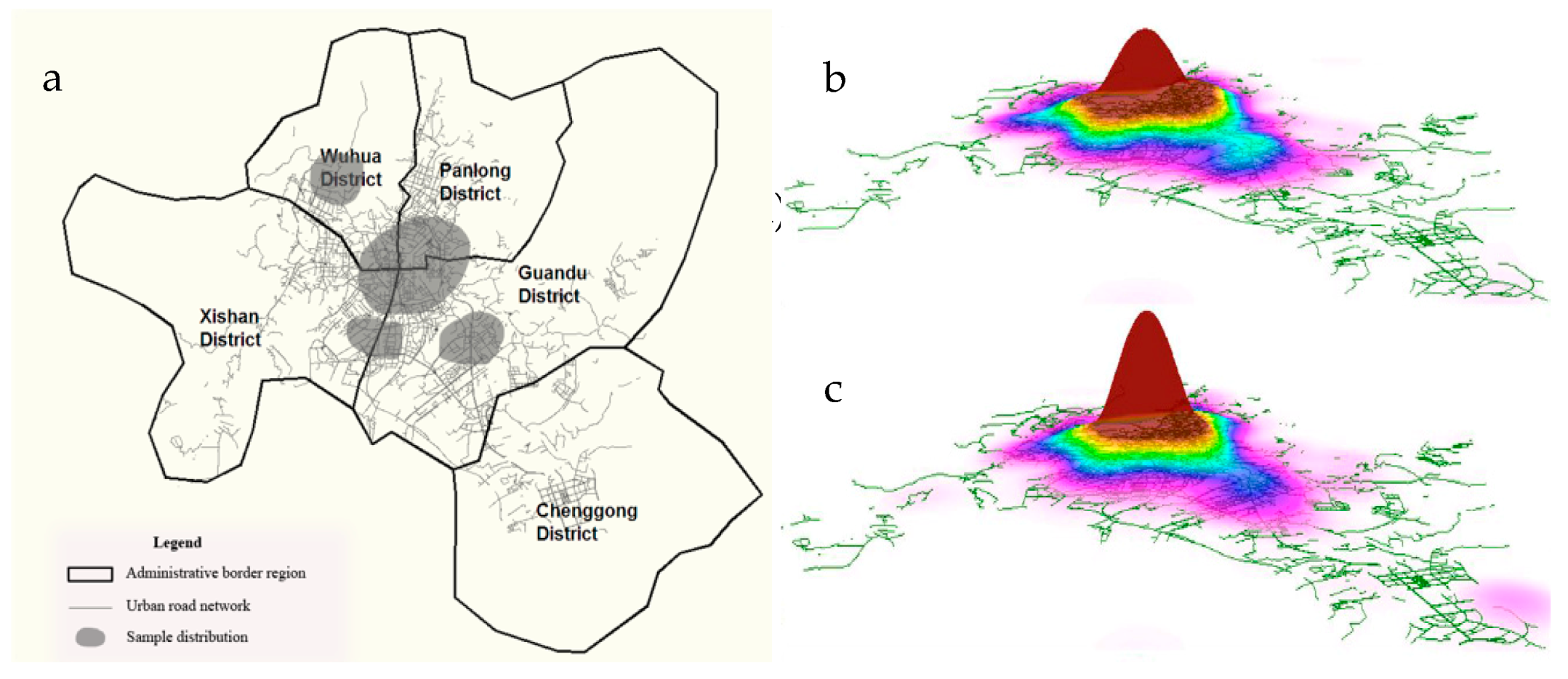
Figure 4.
Distribution of modes of transportation used by elderly for healthcare.
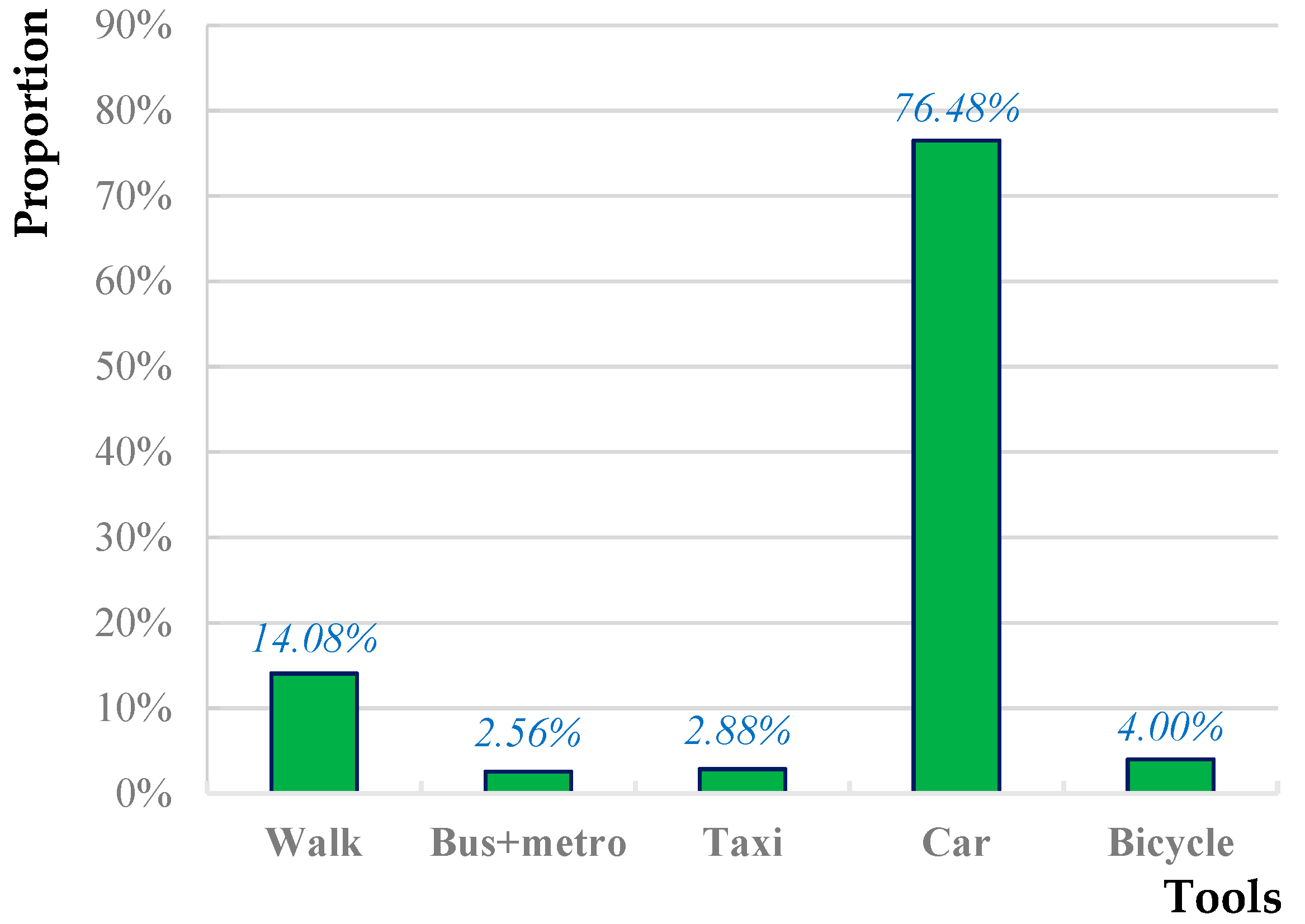
Figure 5.
Distribution of healthcare time of the elderly for healthcare.
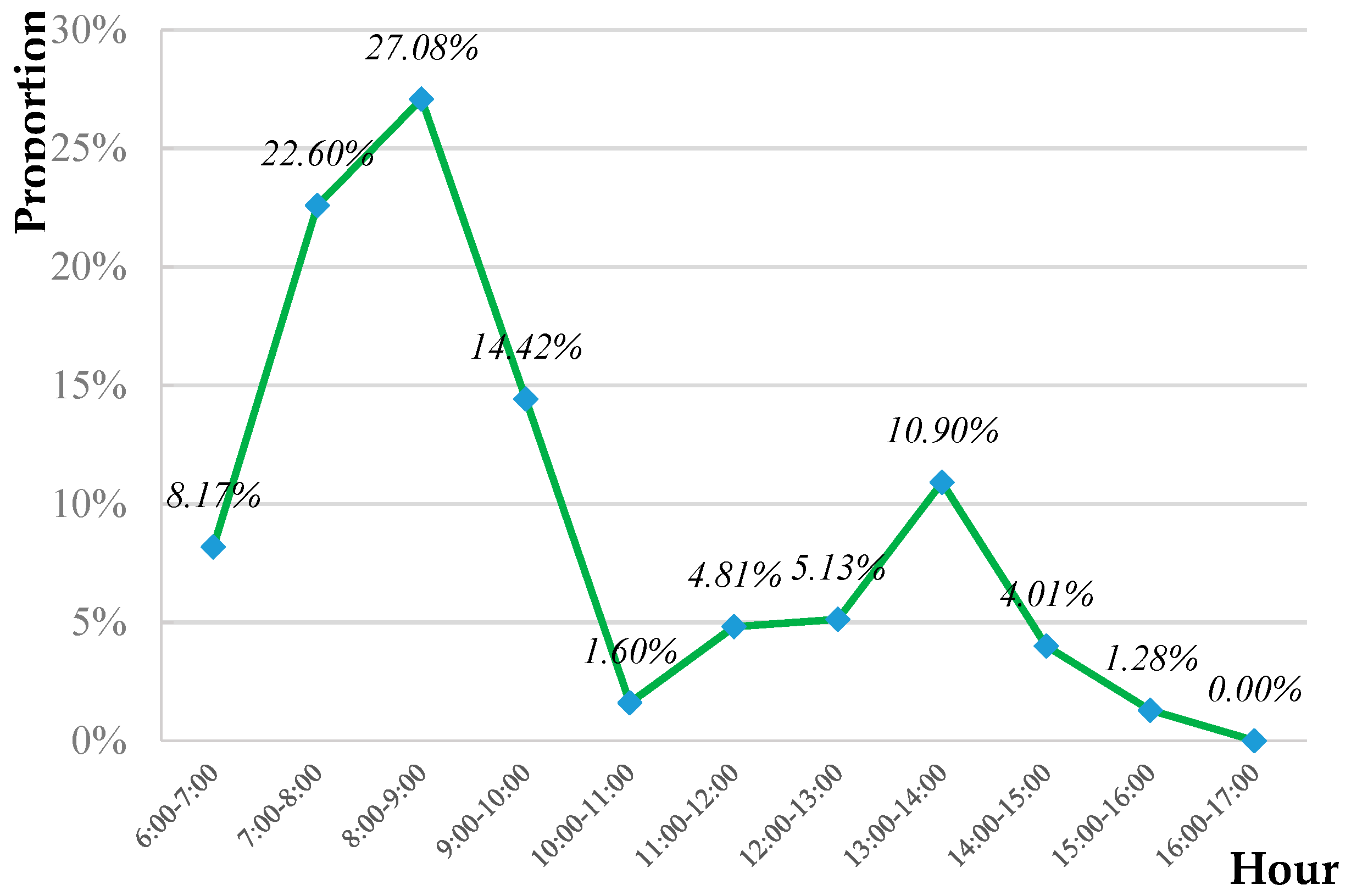
Figure 6.
Distribution of healthcare duration (hour) consumed by elderly for healthcare.
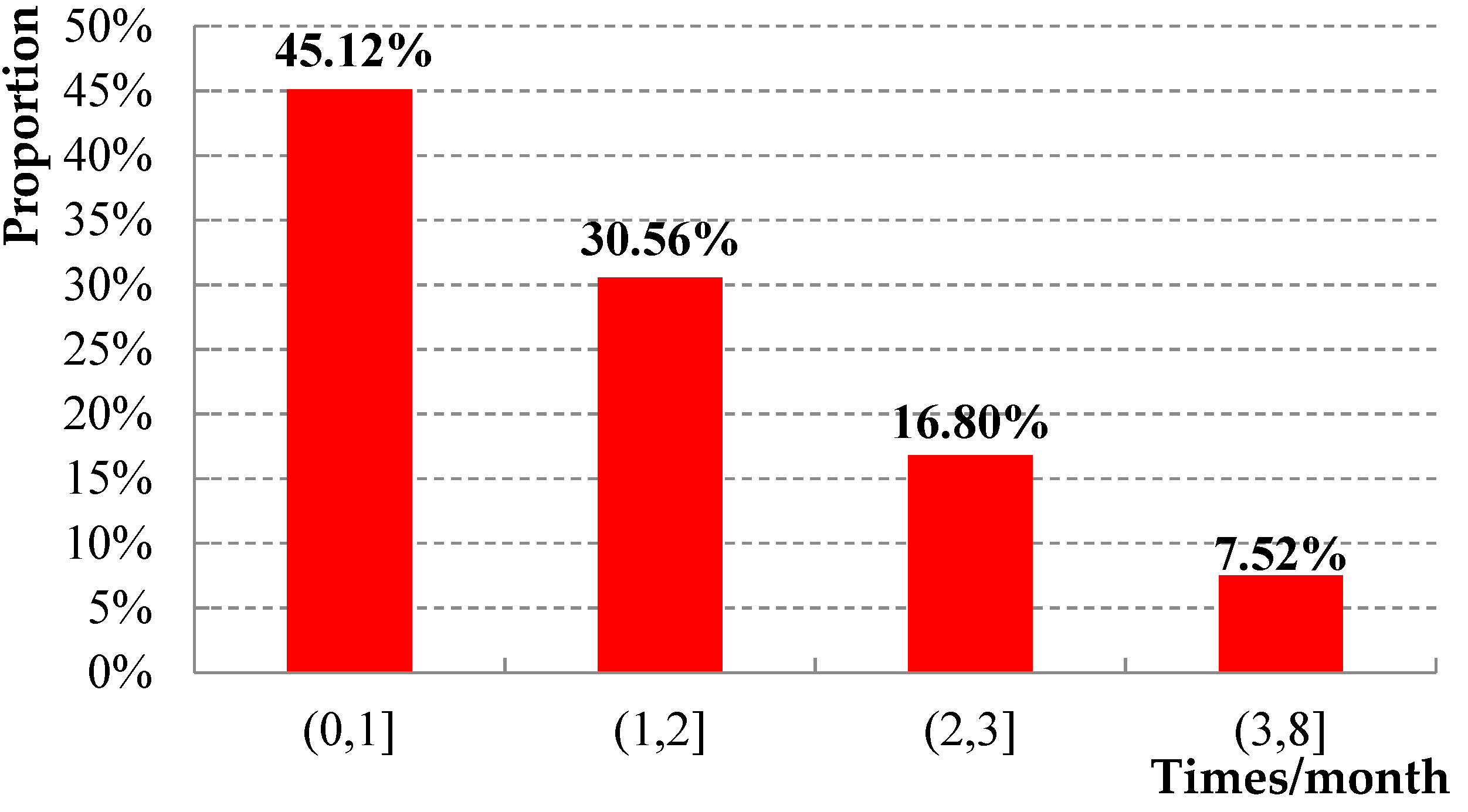
Figure 7.
Constraint degree of healthcare.
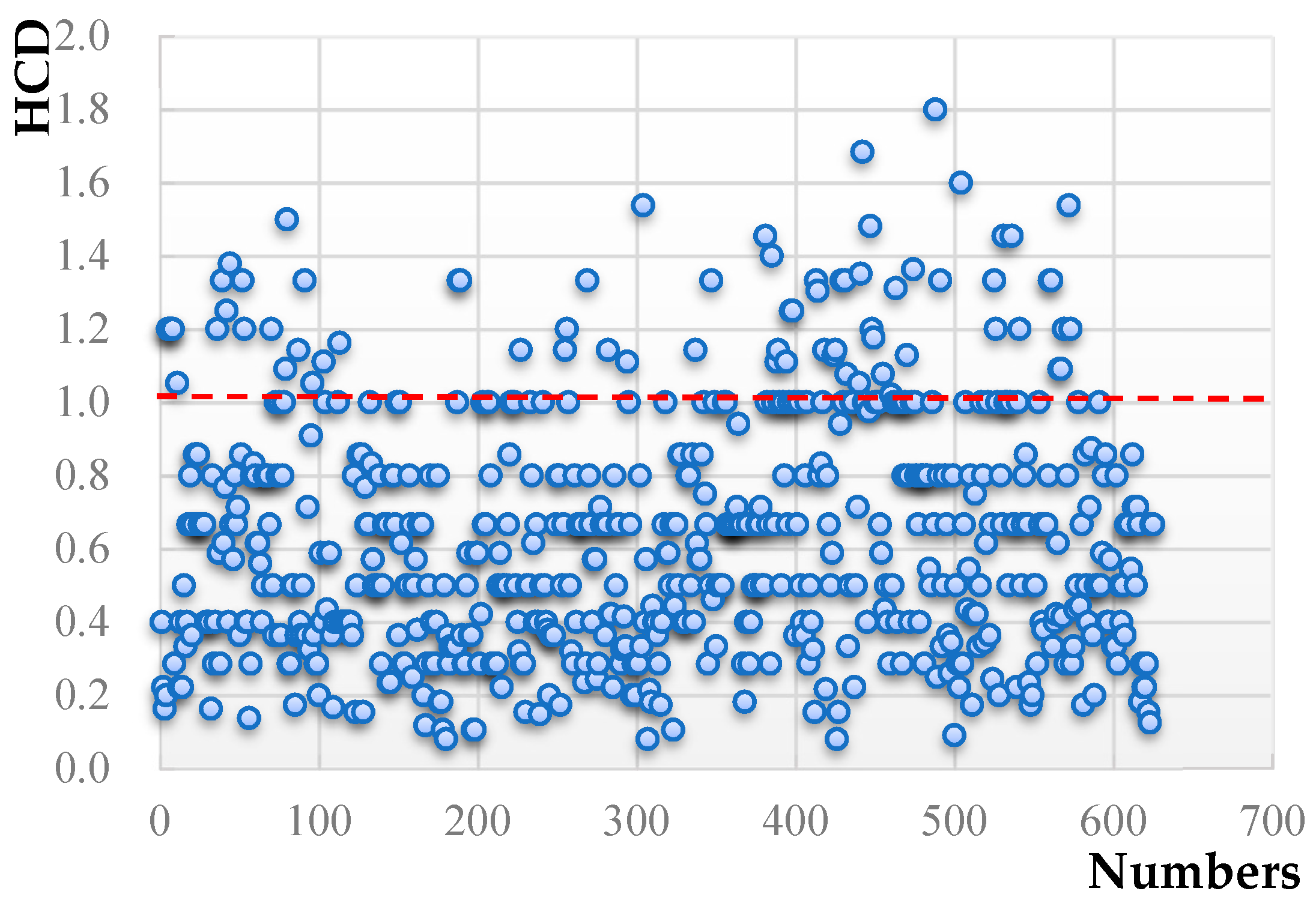
Figure 8.
Calculation process of the model.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristic variables definition and notes.
| Variable | Definition and Notes | |
|---|---|---|
| Personal attributes | Gender | Male = 1, Female = 2 |
| Age | [60,70) = 1, [70,80) = 2, >80 = 3 | |
| Family attribute | Car pick-up | Yes = 1, No = 0 |
| Number of family with driver’s license | 1 = 1, 2 = 2, >3 = 3 | |
| Accompanied by family | Yes = 1, No = 0 | |
| Travel attribute | Distance from bus stop (m) | [0,500) = 1, [500,1000) = 2, [1000,1500) = 3, >1500 = 4 |
| Travel time (min) | [0,30) = 1, [30,60) = 2, [60,90) = 3, >90 = 4 | |
| Travel distance (km) | [0,2) = 1, [2,5) = 2, [ 5,10) = 3, >10 = 4 | |
| Frequency of healthcare (time) | [0,1) = 1, [1,2) = 2, >2 = 3 | |
| Walkability | Walkable = 1, Walkable with difficulty = 2, Not walkable = 3 | |
| Healthcare purpose | Take medicine = 1, Physical examination = 2, Treatment = 3 | |
| Healthcare time (min) | [0,30) = 1, [30,60) = 2, [60,90) = 3, >90 = 4 | |
Table 2.
Strong constraint healthcare results by multinomial logit models.
| Activity Type | Strong Constraint () | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic Variable | Walk | Bus + Metro | Taxi | Car | ||||
| B | Sig. | B | Sig. | B | Sig. | B | Sig. | |
| Constant | 4.62 | 0.00 | −7.17 | 0.00 | 1.24 | 0.00 | 4.33 | 0.00 |
| Gender | 1.46 | 0.03 | −2.42 | 0.01 | - | - | −6.26 | 0.00 |
| Travel time | −3.63 | 0.00 | −1.14 | 0.01 | 2.37 | 0.00 | 3.21 | 0.04 |
| Travel distance | −2.11 | 0.01 | - | - | 0.82 | 0.01 | 4.22 | 0.00 |
| Distance from bus station | −0.21 | 0.00 | −0.11 | 0.00 | - | - | 1.12 | 0.01 |
| Frequency of healthcare | 0.43 | 0.00 | −0.22 | 0.00 | −1.22 | 0.02 | −0.12 | 0.01 |
| Walkability | 2.35 | 0.00 | −0.04 | 0.00 | −4.25 | 0.00 | −3.46 | 0.02 |
| Model Checking Correlation Coefficient | ||||||||
| Chi-square | 135 | Cox and Snell | 0.76 | |||||
| McFadden | 0.745 | Nagelkerke R Square | 0.86 | |||||
Table 3.
Weak constraint healthcare results by multinomial logit models.
| Activity Type | Weak Constraint () | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic Variable | Walk | Bus + Metro | Taxi | Car | ||||
| B | Sig. | B | Sig. | B | Sig. | B | Sig. | |
| Constant | 3.16 | 0.00 | −6.92 | 0.00 | 2.50 | 0.00 | −4.16 | 0.00 |
| Age | −1.87 | 0.00 | - | - | 4.81 | 0.02 | 9.62 | 0.00 |
| Healthcare purpose | 0.99 | 0.02 | −0.54 | 0.01 | 2.36 | 0.04 | 5.55 | 0.00 |
| Car pick-up | −9.14 | 0.04 | −6.22 | 0.02 | −7.45 | 0.00 | 14.61 | 0.00 |
| Travel distance | −1.66 | 0.03 | −0.27 | 0.00 | 1.43 | 0.00 | 2.54 | 0.01 |
| Healthcare time | −0.84 | 0.01 | 0.27 | 0.00 | 0.95 | 0.00 | 4.34 | 0.02 |
| Accompanied by family | −2.65 | 0.00 | −0.98 | 0.02 | 1.43 | 0.02 | 8.95 | 0.00 |
| Number of family with driver’s licenses | −1.15 | 0.00 | −0.67 | 0.03 | −1.32 | 0.01 | 4.37 | 0.00 |
| Model Checking Correlation Coefficient | ||||||||
| Chi-square | 148 | Cox and Snell | 0.611 | |||||
| McFadden | 0.67 | Nagelkerke R Square | 0.70 | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Li, X.; Zhang, Y.; Du, M. Analysis of Travel Decision-Making for Urban Elderly Healthcare Activities under Temporal and Spatial Constraints. Sustainability 2018, 10, 1560. https://doi.org/10.3390/su10051560
AMA Style
Li X, Zhang Y, Du M. Analysis of Travel Decision-Making for Urban Elderly Healthcare Activities under Temporal and Spatial Constraints. Sustainability. 2018; 10(5):1560. https://doi.org/10.3390/su10051560
Chicago/Turabian StyleLi, Xuefeng, Yong Zhang, and Mingyang Du. 2018. "Analysis of Travel Decision-Making for Urban Elderly Healthcare Activities under Temporal and Spatial Constraints" Sustainability 10, no. 5: 1560. https://doi.org/10.3390/su10051560
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.