Managing Sustainable Use of Antibiotics—The Role of Trust


1
Department of Political Science, University of Gothenburg, P.O. Box 711, SE 405 30 Gothenburg, Sweden
2
Department of Social and Behavioural Studies, University West, SE 461 32 Trollhättan, Sweden
*
Author to whom correspondence should be addressed.
Sustainability 2018, 10(1), 143; https://doi.org/10.3390/su10010143
Submission received: 6 December 2017
/
Revised: 3 January 2018
/
Accepted: 5 January 2018
/
Published: 9 January 2018
(This article belongs to the Special Issue Trust Management: Key Factor of the Sustainable Organizations Embedded in Network)
Abstract
:Human overuse of antibiotics is the main driver of antibiotic resistance. Thus, more knowledge about factors that promote sustainable antibiotic use is urgently needed. Based upon findings from the management of other sustainability and collective action dilemmas, we hypothesize that interpersonal trust is crucial for people’s propensity to cooperate for the common objective. The aim of this article is to further our understanding of people’s antibiotic consumption by investigating if individuals’ willingness to voluntarily abstain from antibiotic use is linked to interpersonal trust. To fulfill the aim, we implement two empirical investigations. In the first part, we use cross-section survey data to investigate the link between interpersonal trust and willingness to abstain from using antibiotics. The second part is based on a survey experiment in which we study the indirect effect of trust on willingness to abstain from using antibiotics by experimentally manipulating the proclaimed trustworthiness of other people to abstain from antibiotics. We find that interpersonal trust is linked to abstemiousness, also when controlling for potential confounders. The survey experiment demonstrates that trustworthiness stimulates individuals to abstain from using antibiotics. In conclusion, trust is an important asset for preserving effective antibiotics for future generations, as well as for reaching many of the United Nations’ Sustainable Development Goals.
1. Introduction
The growth of resistance to remedies against infections is one of the world’s utmost challenges. In fact, antimicrobial resistance is estimated by the World Health Organization to already cause more than 700,000 yearly deaths from infections with resistant microbes and the number will increase dramatically in the future, if this problem is left unchecked. The unsustainable behavior of human overconsumption has been identified as a major driver of this growth [1,2,3].
Limiting antibiotic resistance is a matter of sustainable development because today’s overconsumption of antibiotics compromises the ability of future generations to treat bacterial infections. However, already, antibiotic resistance dampens the potential to attain several of the United Nations’ Sustainable Development Goals (SDGs). The goals to end poverty, ensure food security, ensure access to water and sanitation, install sustainable economic growth as well as sustainable consumption and production are all likely to be impaired by the presence of untreatable infections [4,5].
However, like many other sustainability issues, promoting prudent human use of antibiotics has the ingredients of a collective action problem. Despite the fact that overconsumption breeds resistance, there are very limited incentives for patients or health-care providers to consider the effect of their decision about antibiotic use on the overall levels of resistance [6,7,8].
This paper builds on lessons drawn from the study of other sustainability collective action dilemmas. In particular, we hypothesize that interpersonal trust, known to promote collective action in relation to climate change, fisheries and water management, also makes individuals more willing to cooperate to fight antibiotic resistance by limiting their own use of antibiotics. The aim of this article is to further our understanding of people’s antibiotic consumption by investigating if individuals’ willingness to voluntarily abstain from antibiotic use is linked to interpersonal trust.
To fulfill the aim, we implement two separate empirical investigations. In the first part, we use cross-section survey data to investigate the link between interpersonal trust—the belief that most people can be trusted—and willingness to abstain from using antibiotics. The second part is based on a between-subject survey experiment where we study the role of interpersonal trust indirectly by experimentally manipulating the trustworthiness of other people. As such, we study the causal contribution of public willingness to limit antibiotic use on respondents’ own willingness to limit their use of antibiotics.
The results from the analysis of the cross-section data show that interpersonal trust is linked to willingness to limit antibiotic use, also when controlling for potential confounders. The survey experiment demonstrates that the general willingness to abstain from using antibiotics among the general public—our indicator of trustworthiness—stimulates individuals to abstain from using antibiotics themselves. In doing so, this study contributes to the understanding of the role of interpersonal trust for individual voluntary behavior in large-scale collective action dilemmas, such as antibiotic use. In addition, the paper shows that insights from other sustainability issues may also be useful when it comes to the struggle to limit unsustainable use of antibiotics.
The structure of the paper is as follows: Section 2 depicts previous research on antibiotics use and resistance, and we argue that when it comes to antibiotic overuse, more attention should be paid to the behavior of patients. In Section 3 we build on findings from other sustainability issues, account for the theoretical model of collective action and present the hypotheses about the link between trust and collective action to limit antibiotic use. Section 4 is dedicated to methods and materials, where the case of Sweden and subsequently the survey and survey experiment methods are presented. Section 5 reports the results from the survey and the survey experiment. Lastly, Section 6 is a concluding discussion on voluntary cooperation and proposes future studies and upcoming proposals for examining and attaining behavioral change.
2. Previous Research
Apart from variation in antibiotics use linked to different types of infections, there is also a variation related to non-medical factors [9]. For example, in a study by Bjerrum et al. [10] it was discovered that national differences in prescription rates do not tend to mirror the prevalence of bacterial infections, but are related to national recommendations, treatment traditions and pharmaceutical marketing. Other contextual factors found to be important in the previous literature are type of health-care system [9], corruption [11,12] and a number of cultural factors [13,14], for example, risk aversion [15,16].
Antibiotic use also varies by individual factors, such as knowledge [17], gender [18], education [17,19], age [20], trust in institutions [6] and interpersonal trust [6,21].
Around the world, initiatives are now taken to ensure that antibiotics are only attainable through prescription, in addition to various attempts to limit the amount of prescribed antibiotics. These efforts have been directed towards medical practitioners (e.g., by creating guidelines), which in many countries has had the intended effect of lowering overall consumption. A prominent example here is that medical practitioners can be educated in order to diminish the prescription rates [22]. This is the case for Sweden, which has managed to diminish the use of antibiotics, even if overconsumption still is a problem [23,24].
While much attention has been directed towards changing the behavior of prescribers, relatively little attention has been given to the behavior of patients. This is of interest since previous studies have shown that medical practitioners are confronted with demands for antibiotics from patients [25,26,27,28]. Time restrictions and high demand from patients jointly influence prescribers to prescribe antibiotics, even in cases where this might not be necessary in order to treat the infection. In a study in the UK, it was found that about 96% of all patients who request antibiotics also receive it, indicating that antibiotic consumption might involve a shared decision-making between doctors and patients [25].
This has led scholars to argue that in order to reduce prescription rates, programs intended to change behavior must be put in place for patients, which is crucial in the struggle to promote sustainable antibiotic use [29]. The importance of the patient perspective is further underscored by recent increases in awareness campaigns in Europe, intended to inform patients about when antibiotics are redundant [15].
However, it is known from many other sustainability issues that an understanding of the salience of the issue is a necessary, yet insufficient, condition for cooperation to occur. In solving sustainability issues such as climate change, fisheries management and clean water, trust is a key component in creating behavioral change towards sustainable use of resources. The more people believe that others will cooperate, the more likely that they will adopt cooperative behavior [30,31].
Interestingly, in a study by Blommaert, Marais, Hens, Coenen, Muller, Goossens and Beutels [21], the authors also discovered a relationship between country levels of interpersonal trust and levels of antibiotics use. This study was reinforced by individual-level evidence in a study by Rönnerstrand and Andersson Sundell [6], who found a link between interpersonal trust and the willingness to postpone antibiotic treatment.
The aim of this article is to further our understanding of people’s antibiotic consumption by investigating if individuals’ willingness to voluntarily abstain from antibiotic use is linked to interpersonal trust.
Many other sustainability issues—such as fisheries management, climate change and access to clean water—are examples of collective action problems. The next section describes why antibiotic resistance can also be understood as such a challenge, and, based on theory and previous research, hypothesize a link between interpersonal trust and willingness to limit personal use of antibiotics.
3. Theoretical Framework and Hypotheses
A collective action problem typically occurs when a group of people share a resource but where the gain for each individual is highest if he or she disregards the group benefit and acts in self-interest, no matter what other group members do. This is valid, while the profit for everyone is nonetheless higher if all were to cooperate, since the joint resource will otherwise gradually be impoverished or depleted [32]. Simultaneously, if a person understands the potential negative outcome, and thus chooses to cooperate (i.e., reduce his or her resource usage), he or she may easily end up in a position of a “sucker” [33]. That means that the person is losing twofold: not receiving the individual profit and also suffering from the collective damage.
With the example of antibiotics, the key driver of resistance is overuse, but there are limited incentives for each patient or health-care provider to consider the overall consequences of antibiotic use [7,8]. Over time, overconsumption or lack of cooperation can turn into a tragedy of the commons, where the resource is depleted, or in the case of antibiotic resistance, when the healing properties of antibiotics are exhausted. To illustrate, it is often perceived as a sacrifice both by the patient and the treating doctor not to rely on antibiotics when the patient has an infection, even when there is no or weak evidence that such treatment would in fact cure the infection. The benefits of such a sacrifice are, on the other hand, dispersed and remote.
When it comes to resource collective action dilemmas in general, the level of worry that individuals experience and/or express is connected to whether these individuals are willing to act in favor of group concerns and resources, or not [34,35,36]. Furthermore, the main focus of this paper is that we know that interpersonal trust is positively related to cooperation in collective action dilemmas [37]. For example, there is a well-studied relationship between interpersonal trust and cooperation in small-scale dilemmas involving a limited number of actors [31,38,39,40,41]. However, we know less about if and how interpersonal trust works in relation to cooperation in large-scale dilemmas, such as antibiotics use.
In fact, there are several differences between small-scale and large-scale collective action situations. Importantly, Olson’s argument is that—without an external enforcer—collective action in small groups may come about but is destined to fail in large groups. In a small group setting, social pressure and the quest for reputation and social prestige may stimulate cooperation, as long as members of the group can interact face-to-face. In large groups, Olson argues, collective action is impossible without external enforcement [42].
However, despite Olson’s prediction, a few studies have found that interpersonal trust may also stimulate voluntary cooperation also in a large-scale setting [43,44,45]. Based upon findings from the study of collective action dilemmas, we theorize that interpersonal trust is crucial for people’s propensity to cooperate to fight antibiotic resistance by limiting their own use of antibiotics. Hypothetically, people who have higher levels of interpersonal trust (the belief that most people can be trusted), will be more willing to decrease their own use of antibiotics.
Hypothesis 1 (H1).
Higher levels of interpersonal trust are positively correlated with a higher propensity to take voluntary action to decrease one’s own use of antibiotics.
Previous studies of collective action show that trustworthy behavior of others elicits pro-social behavior in other collective action problems [30,31]. People who trust that peers will contribute or cooperate are more compelled to cooperate themselves [30,46,47,48]. However, this can also have the opposite effect, if it is believed that others are not acting pro-socially [49]. Based on these findings, a second hypothesis concerns whether people who receive information about the trustworthiness of other people (i.e., there is a high willingness among others to limit their own antibiotic use) will have a higher propensity to abstain from using antibiotics:
Hypothesis 2 (H2).
Higher belief in the trustworthiness of others has a positive effect on the propensity to take voluntary action to decrease one’s own use of antibiotics.
4. Materials and Methods
In order to test our two hypotheses, the study is separated into two parts. Making use of cross-section survey data, the first part examines the link between interpersonal trust and individual willingness to limit antibiotic use. The second part utilizes a survey experimental approach to allow for causal inference and to study the causal contribution of the proclaimed trustworthiness of other people on individuals’ willingness to limit antibiotic use.
By combining both survey data and survey experiment, we utilize the major strengths of the two methods: compensating external validity with survey data and addressing causality through the survey experiment [50]. Furthermore, this combination also makes it possible to control for common confounders of trust and trustworthiness. [51].
The choice of Sweden as the case was motivated by the fact that Sweden has among the highest levels of interpersonal trust in the world [52,53]. This is thus a so-called tough test for our theory, because interpersonal trust will likely have a stronger relationship with cooperative behavior either by the lower the general levels of trust and/or the larger the relative differences in levels of trust. This means that if we even find support for the relationship between interpersonal trust and cooperation in Sweden, where the general level of interpersonal trust is high and the relative differences among individuals is presumably rather low, then this connection is likely to be even stronger in other countries where the level of interpersonal trust is generally lower.
Another reason for the focus on Sweden is that knowledge about antibiotic treatment and antibiotic resistance is high in this country [15,54]. This means that in the experiment, extensive information on the issue did not have to be provided for the experiment to materialize successfully, but was instead assumed to be endogenous.
4.1. Design of the Cross-Section Survey Study
To test our first hypothesis, we used an annual survey conducted by the Society, Opinion and Media Institute (the SOM Institute) at the University of Gothenburg. This survey captures both our main independent and dependent variables, including many other variables associated with antibiotic consumption. The survey is well established in Sweden and is based on a probability sample of the Swedish population, drawn from the public register. The sample was slightly skewed towards more educated and male participants, which motivated us to systematically control for level of education and gender in our studies. The total number of respondents in the SOM survey was 9828. However, all respondents were not asked all questions, and 3400 is the number of people who were invited to answer questions about antibiotics, thus, the number of survey respondents who answered all the questions required to be included in the analysis was 1293. The AAPOR response rate was 47%.
The question that is the dependent variable was “to what extent would you say that you are willing to abstain from using antibiotics, even if you risk additional sick days?” The four options are 1 = would certainly not abstain, 2 = would not abstain, 3 = would abstain and 4 = would certainly abstain. A majority of the respondents answered that they are willing to abstain from using antibiotics and hence this variable was skewed. We argue that the group that would certainly abstain from using antibiotics is more likely to behave this way than all others and we therefore dichotomized the four response alternatives into 1 = would certainly abstain and 0 = all other groups.
Since the dependent variable was dichotomous, a binary logistic regression, and more specifically, an odds ratio, was used [55]. We did this in order to assess whether higher levels of interpersonal trust are associated with a higher propensity to abstain from using antibiotics.
There are several factors that can potentially affect the relationship between interpersonal trust and willingness to abstain from using antibiotics. The first is age, since older patients have been found to consume more antibiotics [20], while this group also tends to report higher levels of interpersonal trust [56,57]. A second aspect is that gender has been related to cooperation in some collective action dilemmas [58], while women consume more antibiotics [18]. Furthermore, subjective health is linked to higher levels of interpersonal trust [59], and positive health decisions [60], while people with higher stated well-being are more willing to wait to consume antibiotics [6]. Lastly, education can influence the focal relationship through higher levels of education being associated with more knowledge on appropriate use [17,19], while people who are more educated also tend to be more worried about the growth of resistance [6]. Controlling for education is also important since it could be related to levels of interpersonal trust [61].
4.2. Design of the Survey Experiment
For the survey experiment, we make use of a web survey called The Citizen Panel, accessible through the Laboratory of Opinion Research at the University of Gothenburg, where 5000 participants in the panel received the survey and 3605 responded, resulting in a participation rate of 72.1%. The recruitment of participants in the Citizen Panel is mostly comprised of self-selection yet some are recruited using random probability sampling [62].
We manipulate the mechanism hypothesized to be the link between interpersonal trust and cooperation, that is, the belief about the trustworthiness of others. Group means are assumed to be equal and this null hypothesis is rejected if differences are larger than would be expected to occur in repeated trials on a 95% confidence level. ANOVA is used to compare group means and a post-hoc test, Tukey’s HSD, is used to discern if and which group means are different from one another. The effect size of the manipulation is measured in eta squared.
A between-subject design is used and respondents are randomly assigned to one out of four treatment groups and receive a vignette with a hypothetical scenario. In Table 1 the information given to the different groups is displayed. Groups 1 and 2 are the main experiment groups who receive information on the cooperation of others (see Appendix A for vignettes). Group 1 receives information that 80% of people with a similar infection and situation tend to cooperate and choose to abstain from using antibiotics whereas Group 2 receives information that only 20% tend to cooperate. Both groups receive information on the salience of the issue, such as the problem of growing resistance dampening the effectiveness of modern medicine (e.g., in treating severe infections) [5]. They also receive information that a physician has prescribed antibiotics and that it is not always necessary to consume antibiotics to treat this illness. Lastly, Groups 1 and 2 are told to imagine that they have a minor infection and are asked how likely they are to abstain from using antibiotics, even if they risk additional sick days. Group 3 is then installed to disentangle if there is an independent effect of the said cooperation of others on the cooperativeness that does not depend on the salience of the issue. Group 4 is a pure control group that only receives the question about their willingness to abstain from using antibiotics. Control variables are used to ensure random selection to the treatment groups (see Supplementary Materials for proof of random selection).
The dependent variable is measured through the question “Imagine that you have a respiratory tract infection. How likely are you to abstain from using antibiotics, even if you risk additional sick days?” The options are numbered from 1 to 5 where 1 = not at all likely, 2 = not likely, 3 = neither likely nor unlikely, 4 = likely and 5 = very likely.
4.3. Ethics
Those responsible for the SOM survey and the Citizen Panel at the University of Gothenburg conducted internal ethical reviews of the protocols before the studies were approved and underway. The participants of the survey experiment were informed that the vignettes were hypothetical.
5. Results
5.1. Results from the Analysis of Cross-Section Data
A logistic regression model is created to analyze the relationship between interpersonal trust and stated willingness to abstain from using antibiotics. The results from the logistic regression models are presented in Table 2. Model 1 is a significant improvement from Model 0 to estimate the odds of a respondent being willing to abstain from antibiotics. Interpersonal trust is a significant predictor of odds to abstain from using antibiotics on a p-level = 0.01. This is interpreted as for each increase in level of interpersonal trust the odds of abstaining from using antibiotics increases with 11%.
In Model 2, potential confounders and control variables are introduced. These are how worried people are for increasing antibiotic resistance in the future, the number of antibiotic courses people have taken in the last year and a measure of self-estimated health. We expect that higher values of worry, consumption and health are correlated with an increased propensity to limit one’s consumption of antibiotics. When these variables are added, the individual contribution of interpersonal trust still remains, where the odds of certainly wanting to abstain from taking antibiotics increases by 8% for every one-step increase in interpersonal trust on the p-level = 0.01. In general, the added variables follow the prediction, a person who consumes the highest number of antibiotics courses has lower odds to answer that they most certainly would abstain from using antibiotics (p = 0.1). The group that only consumed one course of antibiotics has higher odds to abstain from using antibiotics than any other category (p = 0.01). These results are curved and indicate that the number of antibiotics courses does not contribute a lot to explaining abstention decisions. Worry about increased resistance in the future sometimes contributes to explain abstention decisions. For example, if you are not worried at all, you have lower odds of abstaining from using antibiotics and are significantly different than other categories. The group that is most worried is four times more likely to abstain from using antibiotics than the other categories. However, only the lowest and highest levels of worry are statistically significant. Higher levels of self-estimated health increase the odds of certainly abstaining from using antibiotics. A one-step increase in self-estimated health results in 43% increased odds of certainly abstaining from using antibiotics. Most of the model fit estimates show an increase in model fit, however not all of them, indicating that Model 2 only offers a slightly better prediction of abstention decisions.
In Model 3, level of education and institutional trust are added to the model. We expect that higher levels of institutional trust and education are linked to a higher likelihood of abstaining from using antibiotics. This holds true for education since respondents with the highest level of education have almost two and a half times higher odds of abstaining from using antibiotics. Interestingly, institutional trust does not explain any of the variation in likelihood to abstain from using antibiotics. When these variables are introduced, the relationship between interpersonal trust and willingness to certainly abstain from using antibiotics diminishes (from Exp(B) = 1.08 to Exp(B) = 1.06). While education contributes most to explaining abstemiousness, interpersonal trust remains significant on the p-level = 0.05. The individual relationship between self-estimated health and antibiotics use on the willingness to abstain from using antibiotics diminish when education and institutional trust are in the model. All model fit estimates indicate a model improvement when education and institutional trust are introduced.
In Model 4, age and gender are added as explanatory variables of abstemiousness. Women are 6% less likely than men to abstain from using antibiotics, yet this difference is not statistically significant. The oldest age category is 36% less likely to abstain from using antibiotics (p-level = 0.05). The two oldest age groups are less likely to abstain from using antibiotics than the youngest groups, however, not all of these differences are significant. When age and gender are added to the model, the individual contribution from the independent variable interpersonal trust remains at 6% and is still significant on the p-level = 0.05. Education continues to have an individual contribution. Level of worry contributes to predict the outcome in the lowest and highest categories. Self-estimated health does not contribute to explain the outcome in Model 4 on the p-level = 0.1. Lastly, only the most frequent users of antibiotics predict the outcome on the p-level = 0.05.
Model 4 has a lower—2 Log Likelihood (−2 LL) and a high, as well as significant, model chi2 indicating a better model fit compared to the other models. Nagelkerke’s R2 has increased while the Hosmer and Lemeshow statistic remains insignificant, which indicates a good fit. While the number of correct classifications remain at 63.9%, we argue that this model best explains the variation in the data.
5.2. Results from the Analysis of Survey Experimental Data
To attain causality of our findings, we conducted a survey experiment. First, we perform an ANOVA (between group Sum of Squares = 313.54, F = 52.87, df = 3, p = 0.00), where at least one experiment group is found to have a significantly different mean than other experiment groups (within groups SSQ = 7135.77, df = 3610).
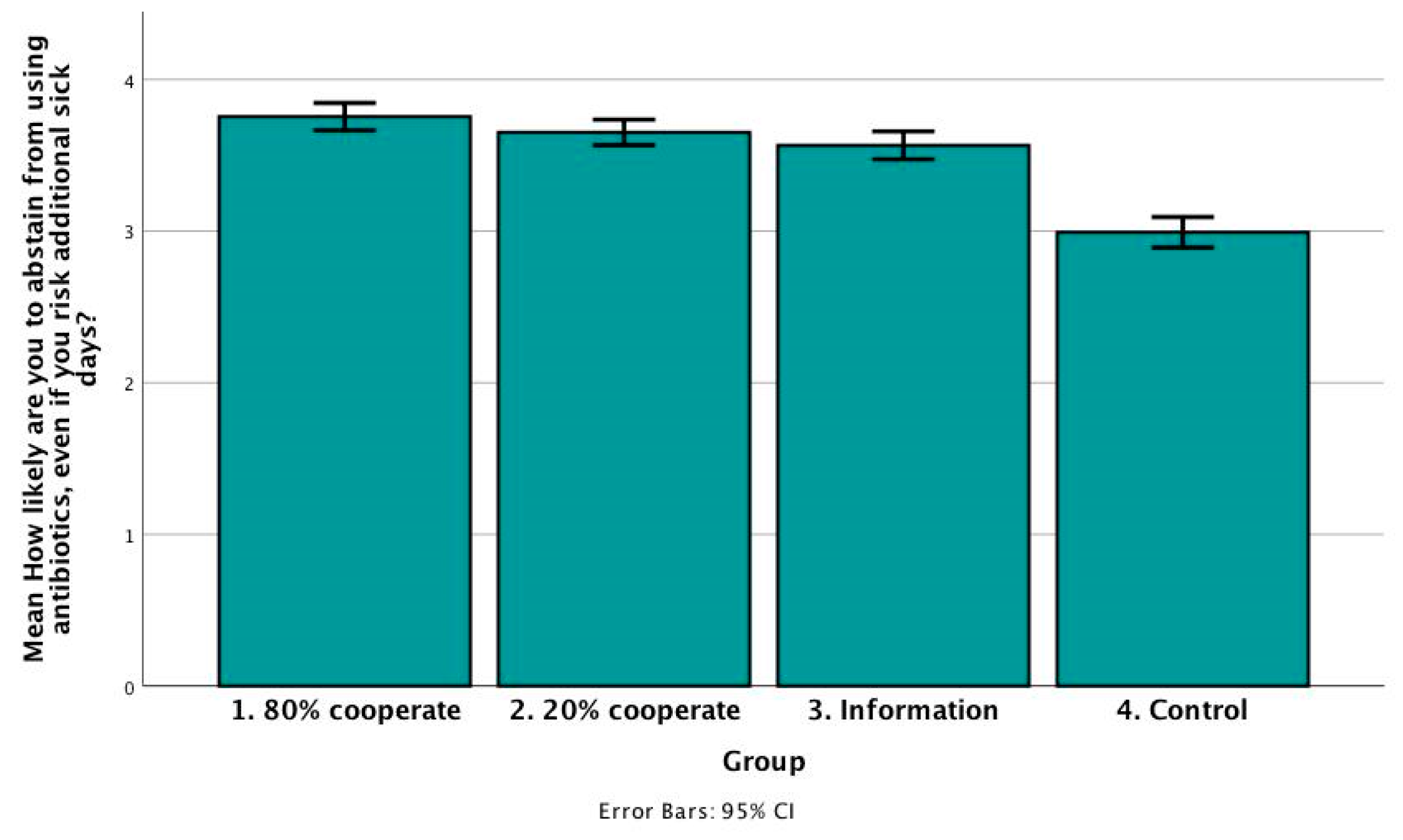
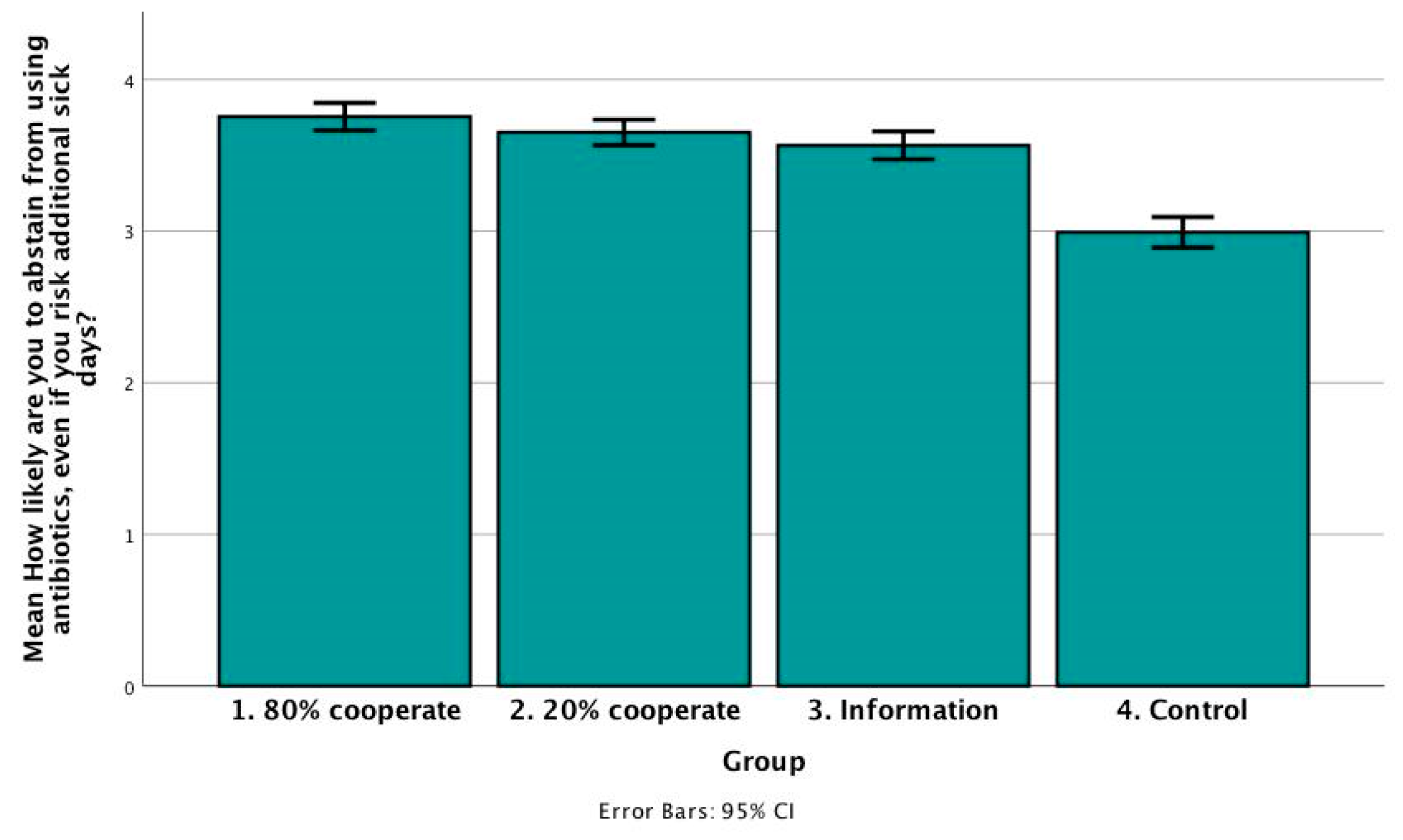
Figure 1 presents the group means. As in the logistic regression model, Swedes have a generally high level of cooperation. The groups do not seem to have significantly different group means since some of the confidence intervals overlap. Group 1 estimated the likelihood to abstain from using antibiotics to a mean of 3.75 (N = 885, std. dev = 1.36, std. err = 0.05, 95% CI = 3.66–3.84). Group 2 estimated the likelihood of abstention to be slightly lower with a mean of 3.65 (N = 958, std. dev = 1.33, std. err = 0.04, 95% CI = 3.57–3.74). Group 3 does not differ as much from group 2 with a mean of 3.57 (N = 877, std. dev = 1.39, std. err = 0.05, 95% CI = 3.47–3.66) Yet the control group has a significantly lower group mean of 2.99 (N = 894, std. dev = 1.54, std. err = 0.05, 95% CI = 2.89–3.09).
To discern which group means are significantly different from each other, we conducted a post-hoc test. With this test, it is possible to observe how successful the manipulations were. Groups 1 and 2 do not have group means that show a significant difference on the p-level = 0.05 (mean diff. = 0.10, std. err. = 0.06). This means that people who receive information that 80% cooperate compared to 20% do not necessarily estimate a higher likelihood to abstain from using antibiotics. Notably, the group means differ significantly between Group 1 and Group 3 (mean diff. = 0.19, std. err. = 0.06, p = 0.05), meaning that if you also receive information that a lot of people cooperate you state you are more likely to abstain compared to the groups that only received information on the salience of the issue. It is also interesting to note that there is no difference in means between the group that only received information on the salience of the issue and the group that received information that 20% cooperate (mean diff. = −0.09, std. err. = 0.07, p = 0.56). The control group is significantly different from all other groups on the p-level = 0.00 (mean diff. from Group 1 = −0.76, std. err. = 0.07, mean diff. from Group 2 = −0.66, std. err. = 0.07, mean diff. from Group 3 = −0.57, std. err. = 0.07).
The effect size estimate, eta squared, tests how much of the variance can be related to group differences, or in other words how much of the variance is affected by the experimental condition. It was calculated to be 0.21 which entails that 21% of the variance is explained by the stimuli.
6. Discussion
Making use of unique cross-section data, we find that interpersonal trust, the belief that most people can be trusted, is associated with a willingness to limit personal use of antibiotics, also when controlling for a number of potential confounders. We thus find support for the first hypothesis of this paper and add to the emerging literature about the link between interpersonal trust and large-scale collective action.
The survey experiment demonstrates that respondents in the stimuli group who received information that 80% of other people cooperate were significantly more willing to limit their own use of antibiotics, as compared to respondents in the group who did not get any information about other people’s cooperativeness. However, contrary to the theoretical expectations, there was no significant difference in the willingness to limit antibiotic use between the “20%” and the “80%” treatment groups. Thus, while not finding unanimous support for our hypothesis, there is still an interesting relation between the trustworthiness of others and respondents’ own decisions to cooperate.
Thus, similar to many other sustainability and collective action resource dilemmas, the results of this study signify that trust and trustworthiness may be important for individuals’ willingness to reduce their personal use of antibiotics in order to prevent antibiotic resistance. However, contrasting the theoretical prediction, the experiment did not show any significant difference in the willingness to abstain from using antibiotics between the groups that received information that 20% cooperate or 80% cooperate. What could be the reason for this? This could possibly be due to the fact that 20% cooperation in large-scale collective action situations in fact shows that many people are ready to bear the cost of cooperation for the common good. To illustrate, 20% of Sweden’s population would entail that as many as 2 million people cooperate. However, if this occurred in a small-scale interaction, it would signify that the actual number of people cooperating is quite small. Further research may study the potential difference in the cut-off point for what is considered trustworthy behavior among other people in large-scale and small-scale collective action.
Antibiotics overuse and the development of antibiotic resistance is a transboundary and global problem. Hence, it is important to know who is being trusted in studies like this one. Future studies could replicate the current study but also compare the results with local and global framings.
Indeed, the results from this study are unique and an important contribution to the existing knowledge about factors that influence citizens’ willingness to limit antibiotic consumption for the sake of preventing resistance. In doing so, the study also adds to what is known about the role of interpersonal trust in stimulating large-scale collective action. Even so, the study has several limitations. Firstly, social desirability might make people more disposed to answer that they would be willing to limit their use of antibiotics to prevent resistance, and this bias may be more pronounced among high-trusting individuals. Secondly, the evidence found in the survey experiment could be an effect of “bandwagoning” rather than being about the trustworthiness of other people. Thirdly, the survey experiment is hypothetical and it can be brought into question to what extent the findings travel to a real-world setting.
In conclusion, using a mixed-methods approach, this paper demonstrates a link between interpersonal trust and willingness to limit personal use of antibiotics in order to prevent antibiotic resistance. Thus, interpersonal trust seems to be an invaluable asset for preserving the therapeutic capacity of antibiotics for future generations, as well as for successful realization of many of the Sustainable Development Goals.
Supplementary Materials
The following are available online at www.mdpi.com/2071-1050/10/1/143/s1, Complete models 0–4 including Wald’s Z. Randomization check for age, sex and level of education.
Acknowledgments
This research was enabled by generous funding from Centre for Antibiotic Resistance Research (CARe) and Centre for Collective Action Research (CeCAR), both at University of Gothenburg, Sweden.
Author Contributions
Felicia Robertson (F.R.) conceived and designed the study; F.R., Sverker C. Jagers (S.C.J.) and Björn Rönnerstrand (B.R.) contributed to the data collection. F.R. analyzed the data; F.R. wrote the first draft of the article, F.R. coordinated subsequent work. F.R., S.C.J. and B.R. contributed to the writing of the manuscript. F.R., S.C.J. and B.R. contributed to critical revisions and approved the final version of the article.
Conflicts of Interest
The authors declare no conflict of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
Appendix A
Appendix A.1. Coding of Control Variables
To what extent people worry about increased antibiotic resistance is measured with the question “how worried would you say you are about increased antibiotic resistance in the future?” The four response options are 1 = not at all worried, 2 = not very worried, 3 = worried, and 4 = very worried. Trust in institutions is asked as “how much confidence do you have that the health-care institution is performing in line with its objective?” The four alternatives are 1 = no confidence at all, 2 = not much confidence, 3 = confidence and 4 = very much confidence. Self-estimated health is measured by “how would you describe your general health?” where 0 = very bad and 10 = very good, and the responses are dichotomized into 0–6 = bad and 7–10 = good. Antibiotics consumption is measured from “how many times have you used antibiotics during the last 12 months?” The options are 1 = more than 5 times, 2 = 2–5 times, 3 = once, and 4 = never. Level of education is coded into four categories: low, middle low, middle high and high. Low education is primary school, middle low is up until high school, middle high is post high school but not a university degree and high is a university degree. Gender is measured with the categories man, woman or other. Due to few responses, other was excluded. Age was recoded into four different categories: 16–29 years, 30–49 years, 50–64 years, 65–85 years.
Appendix A.2. Vignette
One reason to avoid antibiotics is that a high level of overuse of antibiotics increases the growth of antibiotic resistant bacteria.
Imagine the following: You suffer from a respiratory infection with cough, fever and chest pain. You have visited a medical practitioner who assesses that the infection will heal by itself in a few days, yet prescribed antibiotics (penicillin) to accelerate the recovery by a few days.
[Research has shown that four out of five people (80%) tend to regard the interests of society when making decisions for themselves and choose to abstain from using antibiotics/Research has shown that one out of five people (20%) tend to regard the interests of society when making decisions for themselves and choose to abstain from using antibiotics.]
Imagine that you have a respiratory infection, how likely are you to abstain from using antibiotics, when possible, even when you risk additional sick days? 1 = No, probably not, 5 = Yes, probably.
References and Notes
- Bronzwaer, S.L.A.M.; Cars, O.; Buchholz, U.; Mölstad, S.; Goettsch, W.; Veldhuijzen, I.K.; Kool, J.L.; Sprenger, M.J.W.; Degener, J.E. Participants in the European Antimicrobial Resistance Surveillance, S. The relationship between antimicrobial use and antimicrobial resistance in Europe. Emerg. Infect. Dis. 2002, 8, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Goossens, H. Antibiotic consumption and link to resistance. Clin. Microbiol. Infect. 2009, 15, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- SDGs Numbers 1, 2, 6, 8 and 12.
- Jasovsky, D.; Littmann, J.; Zorzet, A.; Cars, O. Antimicrobial resistance-a threat to the world’s sustainable development. Upsala J. Med. Sci. 2016, 121, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Rönnerstrand, B.; Andersson Sundell, K. Trust, reciprocity and collective action to fight antibiotic resistance. An experimental approach. Soc. Sci. Med. 2015, 142, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, P.S.; Wernli, D.; Carroll, S.P.; Dunn, R.R.; Harbarth, S.; Levin, S.A.; So, A.D.; Schlüter, M.; Laxminarayan, R. Use antimicrobials wisely. Nature 2016, 537, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Heymann, D.L. Challenges of drug resistance in the developing world. BMJ 2012, 344, e1567. [Google Scholar] [CrossRef] [PubMed]
- Cars, O.; Mölstad, S.; Melander, A. Variation in antibiotic use in the European Union. Lancet 2001, 357, 1851–1853. [Google Scholar] [CrossRef]
- Bjerrum, L.; Boada, A.; Cots, J.M.; Llor, C.; Garcia, D.F.; Gahrn-Hansen, B.; Munck, A. Respiratory tract infections in general practice: Considerable differences in prescribing habits between general practitioners in Denmark and Spain. Eur. J. Clin. Pharmacol. 2004, 60, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Collignon, P.; Athukorala, P.-C.; Senanayake, S.; Khan, F. Antimicrobial resistance: The major contribution of poor governance and corruption to this growing problem. PLoS ONE 2015, 10, e0116746. [Google Scholar] [CrossRef] [PubMed]
- Rönnerstrand, B.; Lapuente, V. Corruption and use of antibiotics in regions of Europe. Health Policy 2017, 121, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Touboul-Lundgren, P.; Jensen, S.; Drai, J.; Lindbæk, M. Identification of cultural determinants of antibiotic use cited in primary care in Europe: A mixed research synthesis study of integrated design “Culture is all around us”. BMC Public Health 2015, 15, 908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbarth, S.; Monnet, D.L. Cultural and socioeconomic determinants of antibiotic use. In Antibiotic Policies: Fighting Resistance; Springer: Boston, MA, USA, 2008; pp. 29–40. [Google Scholar]
- Borg, M.A. National cultural dimensions as drivers of inappropriate ambulatory care consumption of antibiotics in Europe and their relevance to awareness campaigns. J. Antimicrob. Chemother. 2012, 67, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Borg, M.A. Cultural determinants of infection control behaviour: Understanding drivers and implementing effective change. J. Hosp. Infect. 2014, 86, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Vallin, M.; Polyzoi, M.; Marrone, G.; Rosales-Klintz, S.; Wisell, K.T.; Lundborg, C.S. Knowledge and attitudes towards antibiotic use and resistance-a latent class analysis of a Swedish population-based sample. PLoS ONE 2016, 11, e0152160. [Google Scholar] [CrossRef] [PubMed]
- Schröder, W.; Sommer, H.; Gladstone, B.P.; Foschi, F.; Hellman, J.; Evengard, B.; Tacconelli, E. Gender differences in antibiotic prescribing in the community: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2016, 71, 1800–1806. [Google Scholar] [CrossRef] [PubMed]
- McNulty, C.A.M.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. The public’s attitudes to and compliance with antibiotics. J. Antimicrob. Chemother. 2007, 60 (Suppl. S1), i63–i68. [Google Scholar] [CrossRef] [PubMed]
- European Commission, Directorate-General for Health and Food Safety. Special Eurobarometer 445 Report on Antimicrobial Resistance; European Union: Brussels, Belgium, 2016; Available online: https://ec.europa.eu/health/amr/sites/amr/files/eb445_amr_generalreport_en.pdf (accessed on 9 January 2018).
- Blommaert, A.; Marais, C.; Hens, N.; Coenen, S.; Muller, A.; Goossens, H.; Beutels, P. Determinants of between-country differences in ambulatory antibiotic use and antibiotic resistance in Europe: A longitudinal observational study. J. Antimicrob. Chemother. 2014, 69, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Mölstad, S.; Lundborg, C.S.; Karlsson, A.-K.; Cars, O. Antibiotic prescription rates vary markedly between 13 European countries. Scand. J. Infect. Dis. 2002, 34, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Swedres-Swarm. Consumption of Antibiotics and Occurrence of Antibiotic Resistance in Sweden; Public Health Agency of Sweden and National Veterinary Institute: Solna, Sweden; Uppsala, Sweden, 2015.
- Mölstad, S.; Löfmark, S.; Carlin, K.; Erntell, M.; Aspevall, O.; Blad, L.; Hanberger, H.; Hedin, K.; Hellman, J.; Norman, C. Lessons learnt during 20 years of the Swedish strategic programme against antibiotic resistance. Bull. World Health Organ. 2017, 95, 764. [Google Scholar] [CrossRef] [PubMed]
- McNulty, C.A.M.; Nichols, T.; French, D.P.; Joshi, P.; Butler, C.C. Expectations for consultations and antibiotics for respiratory tract infection in primary care: The RTI clinical iceberg. Br. J. Gen. Pract. 2013, 63, e429–e436. [Google Scholar] [CrossRef] [PubMed]
- Mangione-Smith, R.; Elliott, M.N.; Stivers, T.; McDonald, L.; Heritage, J.; McGlynn, E.A. Racial/Ethnic variation in parent expectations for antibiotics: Implications for public health campaigns. Pediatrics 2004, 113, e385–e394. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.P. Uncomfortable prescribing decisions: A critical incident study. BMJ 1992, 304, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.P. Factors which influence the decision whether or not to prescribe: The dilemma facing general practitioners. Br. J. Gen. Pract. 1992, 42, 454–458. [Google Scholar] [PubMed]
- Väänänen, M.H.; Pietilä, K.; Airaksinen, M. Self-medication with antibiotics—Does it really happen in Europe? Health Policy 2006, 77, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Gächter, S.; Herrmann, B. Reciprocity, culture and human cooperation: Previous insights and a new cross-cultural experiment. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 791–806. [Google Scholar] [CrossRef] [PubMed]
- Van Lange, P.A.M.; Joireman, J.; Parks, C.D.; Van Dijk, E. The psychology of social dilemmas: A review. Organ. Behav. Hum. Decis. Process. 2013, 120, 125–141. [Google Scholar] [CrossRef]
- Dawes, R.M. Social dilemmas. Annu. Rev. Psychol. 1980, 31, 169–193. [Google Scholar] [CrossRef]
- Kollock, P. Social dilemmas: The anatomy of cooperation. Annu. Rev. Sociol. 1998, 24, 183–214. [Google Scholar] [CrossRef]
- Stern, P.C.; Dietz, T.; Abel, T.; Guagnano, G.A.; Kalof, L. A value-belief-norm theory of support for social movements: The case of environmentalism. Hum. Ecol. Rev. 1999, 6, 81–98. [Google Scholar]
- Stern, P.C. Toward a coherent theory of environmentally significant behavior. J. Soc. Issues 2000, 56, 407–424. [Google Scholar] [CrossRef]
- Harring, N.; Jagers, S.C. Should we trust in values? Explaining public support for pro-environmental taxes. Sustainability 2013, 5, 210–227. [Google Scholar] [CrossRef]
- Dietz, T.; Dolšak, N.; Ostrom, E.; Stern, P.C. The Drama of the Commons. In The Drama of the Commons; Ostrom, E., Dietz, T., Dolšak, N., Stern, P.C., Stonich, S., Weber, E.U., Eds.; National Academy Press: Washington, DC, USA, 2002. [Google Scholar]
- Ostrom, E. Governing the Commons: The Evolution of Institutions for Collective Action; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Fehr, E.; Gächter, S. Cooperation and punishment in public goods experiments. Am. Econ. Rev. 2000, 90, 980–994. [Google Scholar] [CrossRef]
- Gächter, S.; Herrmann, B.; Thöni, C. Trust, voluntary cooperation, and socio-economic background: Survey and experimental evidence. J. Econ. Behav. Organ. 2004, 55, 505–531. [Google Scholar] [CrossRef]
- De Rooij, E.A.; Green, D.P.; Gerber, A.S. Field experiments on political behavior and collective action. Annu. Rev. Political Sci. 2009, 12, 389–395. [Google Scholar] [CrossRef]
- Olson, M. The Logic of Collective Action: Public Goods and the Theory of Groups; Harvard University Press: Cambridge, MA, USA, 1965; Volume 124. [Google Scholar]
- Mannemar Sønderskov, K. Different goods, different effects: Exploring the effects of generalized social trust in large-N collective action. Public Choice 2009, 140, 145–160. [Google Scholar] [CrossRef]
- Scholz, J.T.; Lubell, M. Trust and taxpaying: Testing the heuristic approach to collective action. Am. J. Political Sci. 1998, 398–417. [Google Scholar] [CrossRef]
- Thöni, C.; Tyran, J.-R.; Wengström, E. Microfoundations of social capital. J. Public Econ. 2012, 96, 635–643. [Google Scholar] [CrossRef]
- Levi, M. A state of trust. In Trust and Governance; Braithwaite, V., Levi, M., Eds.; Russell Sage Foundation: New York, NY, USA, 1998; pp. 77–101. [Google Scholar]
- Fischbacher, U.; Gächter, S.; Fehr, E. Are people conditionally cooperative? Evidence from a public goods experiment. Econ. Lett. 2001, 71, 397–404. [Google Scholar] [CrossRef] [Green Version]
- Kocher, M.G.; Cherry, T.; Kroll, S.; Netzer, R.J.; Sutter, M. Conditional cooperation on three continents. Econ. Lett. 2008, 101, 175–178. [Google Scholar] [CrossRef]
- Ostrom, E. A behavioral approach to the rational choice theory of collective action: Presidential address, American political science association, 1997. Am. Political Sci. Rev. 1998, 92, 1–22. [Google Scholar] [CrossRef]
- Atzmuller, C.; Steiner, P.M. Experimental vignette studies in survey research. Methodol.-Eur. J. Res. Methods Behav. Soc. Sci. 2010, 6, 128–138. [Google Scholar] [CrossRef]
- Levi, M. Trust, sociology of. In International Encyclopedia of the Social & Behavioral Sciences; Smelser, N.J., Baltes, P.B., Eds.; Pergamon: Oxford, UK, 2001; pp. 15922–15926. [Google Scholar]
- Rothstein, B.; Stolle, D. Introduction: Social capital in Scandinavia. Scand. Political Stud. 2003, 26, 1–26. [Google Scholar] [CrossRef]
- Medrano, J.D. World Map of Interpersonal Trust. 2013. Availabel online: http://www.jdsurvey.net/jds/jdsurveyMaps.jsp?Idioma=I&SeccionTexto=04&NOID=104 (accessed on 9 January 2018).
- Grigoryan, L.; Burgerhof, J.G.M.; Degener, J.E.; Deschepper, R.; Lundborg, C.S.; Monnet, D.L.; Scicluna, E.A.; Birkin, J.; Haaijer-Ruskamp, F.M. Attitudes, beliefs and knowledge concerning antibiotic use and self-medication: A comparative European study. Pharmacoepidemiol. Drug Saf. 2007, 16, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- We have also implemented multinomial regression models with the full four response category outcome variable and the results are similar. In the paper we report odds ratios from the binary logistic regression because they can be interpreted more easily, as compared to the coefficients from the multinomial regression.
- Li, T.; Fung, H.H. Age differences in trust: An investigation across 38 countries. J. Gerontol. Ser. B 2013, 68, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Sutter, M.; Kocher, M.G. Trust and trustworthiness across different age groups. Games Econ. Behav. 2007, 59, 364–382. [Google Scholar] [CrossRef]
- Kopelman, S.; Weber, J.M.; Messick, D.M. Facors influencing cooperation in commons dilemmas: A review of experimental psychological research. In The Drama of the Commons; National Academy Press: Washington, DC, USA, 2002; pp. 113–156. [Google Scholar]
- Mohseni, M.; Lindstrom, M. Social capital, trust in the health-care system and self-rated health: The role of access to health care in a population-based study. Soc. Sci. Med. 2007, 64, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Lindström, M. Social capital and health-related behaviors. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D., Eds.; Springer: New York, NY, USA, 2008; pp. 215–238. [Google Scholar]
- Charron, N.; Rothstein, B. Does education lead to higher generalized trust? The importance of quality of government. Int. J. Educ. Dev. 2016, 50, 59–73. [Google Scholar] [CrossRef]
- For More Information on Sampling Method Visit www.lore.gu.se.
Figure 1.
Mean levels of likelihood to abstain from using antibiotics divided by experiment groups. Source: The Citizen Panel 26 2017.
Figure 1.
Mean levels of likelihood to abstain from using antibiotics divided by experiment groups. Source: The Citizen Panel 26 2017.

{kind=link}
Table 1.
Design—Experimental groups and treatments.
| Group 1 | Group 2 | Group 3 | Group 4 | |
|---|---|---|---|---|
| Information about resistance | x | x | x | |
| Physician prescribes antibiotics | x | x | ||
| Trustworthiness of others | x | x | ||
| Question to abstain antibiotics | x | x | x | x |
Table 2.
Logistic probability models of willingness to abstain from using antibiotics by the variables interpersonal trust, antibiotics use, self-estimated health, worry about increased resistance, level of education, institutional trust, gender, and age.
Table 2.
Logistic probability models of willingness to abstain from using antibiotics by the variables interpersonal trust, antibiotics use, self-estimated health, worry about increased resistance, level of education, institutional trust, gender, and age.
| Model 0 | Model 1 | Model 2 | Model 3 | Model 4 | |
|---|---|---|---|---|---|
| Interpersonal trust | 1.11 *** (0.03) | 1.08 *** (0.03) | 1.06 ** (0.03) | 1.07 ** (0.03) | |
| Antibiotics use (1) | ** | ** | ** | ||
| 2–5 times (2) | 1.48 (0.38) | 1.35 (0.39) | 1.36 (0.29) | ||
| Once (3) | 1.20 (0.35) | 1.13 (0.35) | 1.06 (0.36) | ||
| Never (4) | 1.80 * (0.33) | 1.66 (0.34) | 1.56 (0.34) | ||
| Worry low (1) | *** | *** | *** | ||
| Worry (2) | 0.97 (0.57) | 0.92 (.57) | 1.01 (0.58) | ||
| Worry (3) | 1.93 (0.54) | 1.78 (0.54) | 1.99 (0.55) | ||
| Worry high (4) | 4.02 *** (0.53) | 3.74 ** (0.54) | 4.40 *** (0.55) | ||
| Health (well) | 1.43 ** (0.14) | 1.33 * (0.15) | 1.28 * (0.15) | ||
| Education low (1) | *** | ** | |||
| Education (2) | 1.87 *** (0.22) | 1.53 * (0.23) | |||
| Education (3) | 2.42 *** (0.23) | 1.95 *** (0.24) | |||
| Education high (4) | 2.39 *** (0.22) | 1.86 *** (0.23) | |||
| Institutional trust low (1) | |||||
| Institutional trust (2) | 0.99 (0.35) | 1.00 (0.35) | |||
| Institutional trust (3) | 1.04 (0.34) | 1.10 (0.35) | |||
| Institutional trust high (4) | 1.16 (0.37) | 1.24 (0.37) | |||
| Gender (f) | 0.94 (0.12) | ||||
| Age (1) | *** | ||||
| 30–49 years (2) | 1.14 (0.21) | ||||
| 50–64 years (3) | 0.95 (0.21) | ||||
| 65–85 years (4) | 0.64 ** (0.22) | ||||
| Intercept | 0.82 *** (0.06) | 0.42 *** (0.18) | 0.09 *** (0.66) | 0.06 *** (0.73) | 0.07 *** (0.76) |
| Cases | 1293 | 1293 | 1293 | 1293 | 1293 |
| −2 LL | 1779.99 | 1763.94 | 1674.07 | 1653.84 | 1640.79 |
| Nagelkerke’s R2 | 0.016 | 0.105 | 0.124 | 0.137 | |
| Model Chi2 | 16.05 *** | 105.92 *** | 126.140 *** | 139.20 *** | |
| Hosmer & Lemeshow | 8.25 | 13.61 * | 6.18 | 4.36 | |
| Classification | 54.9% | 57.3% | 62.1% | 63.9% | 63.9% |
Notes: * p < 0.10; ** p < 0.05; *** p < 0.01 for Wald’s Z, Standard Error in brackets, Method = enter, Variables entered: “Are you willing to abstain from using antibiotics, if possible, even when you risk additional sick days.” The options are 1 = no, absolutely not, 2 = no, most likely not, 3 = yes, most likely, and 4 = yes, absolutely, and is dichotomized to 1 = yes, absolutely and 0 = other. Interpersonal trust was posed as “to what extent can you say that other people can be trusted?” Where 0 = one cannot trust other people and 10 = you can trust other people. See Supplementary Materials for coding and full models including Wald’s Z. Source: The national SOM survey 2016.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Robertson, F.; Jagers, S.C.; Rönnerstrand, B. Managing Sustainable Use of Antibiotics—The Role of Trust. Sustainability 2018, 10, 143. https://doi.org/10.3390/su10010143
AMA Style
Robertson F, Jagers SC, Rönnerstrand B. Managing Sustainable Use of Antibiotics—The Role of Trust. Sustainability. 2018; 10(1):143. https://doi.org/10.3390/su10010143
Chicago/Turabian StyleRobertson, Felicia, Sverker C. Jagers, and Björn Rönnerstrand. 2018. "Managing Sustainable Use of Antibiotics—The Role of Trust" Sustainability 10, no. 1: 143. https://doi.org/10.3390/su10010143
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.