
The Role of Caveolin 1 in HIV Infection and Pathogenesis

Department of Infectious Diseases and Pathology, University of Florida, Gainesville, FL 32611, USA
Viruses 2017, 9(6), 129; https://doi.org/10.3390/v9060129
Submission received: 23 March 2017
/
Revised: 2 May 2017
/
Accepted: 22 May 2017
/
Published: 26 May 2017
Abstract
:Caveolin 1 (Cav-1) is a major component of the caveolae structure and is expressed in a variety of cell types including macrophages, which are susceptible to human immunodeficiency virus (HIV) infection. Caveolae structures are present in abundance in mechanically stressed cells such as endothelial cells and adipocytes. HIV infection induces dysfunction of these cells and promotes pathogenesis. Cav-1 and the caveolae structure are believed to be involved in multiple cellular processes that include signal transduction, lipid regulation, endocytosis, transcytosis, and mechanoprotection. Such a broad biological role of Cav-1/caveolae is bound to have functional cross relationships with several molecular pathways including HIV replication and viral-induced pathogenesis. The current review covers the relationship of Cav-1 and HIV in respect to viral replication, persistence, and the potential role in pathogenesis.
1. Introduction
Human immunodeficiency virus (HIV) has an extraordinary survival advantage in the host, confounding existing therapies. Anti-retroviral therapy (ART) suppresses HIV replication to undetectable levels and has been effective in prolonging the lives of HIV infected individuals. The suppression of viral replication by ART in many patients raised hopes for virus eradication. However, ART is not capable of eradicating HIV from infected individuals mainly due to HIV’s persistence in small reservoirs of latently infected resting CD4+ cells [1,2,3,4,5,6]. Furthermore, the rise of drug-resistant viruses in some patients under ART treatment remains a concern [7,8,9,10,11,12]. In addition, ultrasensitive assays show that many patients under ART still have low-level viremia [13,14,15,16]. A complete understanding of where HIV persists, and how latency is established and maintained in patients on ART is critical in developing strategies to cure HIV infection. Although more work is still needed, there are significant developments in our understanding of a persistent HIV infection in patients under drug therapy.
Latently infected resting memory CD4+ cells are present in the blood and lymphoid tissues of patients under ART [17,18]. In blood, central and transitional memory cells are the predominant population of latently infected cells [19]. Albeit at a lower frequency, persistent HIV DNA is also found in naive CD4+ T cell populations of patients on ART [19,20]. Residual viral reservoirs in the gastrointestinal (GI) and genitourinary tract as well as lymphoid tissues in patients under drug treatment can be an additional obstacle for curing HIV [20,21,22,23,24,25,26]. Recent evidence also shows HIV infection in multi-potent hematopoietic progenitor cells in the bone marrow where some of the cells are latently infected [27,28]. Furthermore, it has been confirmed that monocytes, dendritic cells, and macrophages can be infected latently or with a low-level replication and can contribute to viral persistence [29,30,31,32,33,34].
HIV persistence in monocytes/macrophages helps the virus disseminate into the central nervous system. Initial brain infection is thought to occur through an infected monocyte-macrophage traversing the blood-brain barrier [35]. Infected monocytes that enter the brain can then repopulate the resident macrophages with subsequent infection of the existing resident macrophages, microglial cells [36,37,38], astrocytes [38,39,40], and possibly pericytes [41]. Productive HIV replication within the brain mainly occurs in microglial cells and perivascular macrophages whereas the virus does not productively infect neurons [37]. Many drugs are restricted from crossing the blood brain and blood cerebrospinal fluid barrier and are therefore suboptimal in penetrating the central nervous system [42,43]. Consequently, the virus can persist in these cells serving as a reservoir and can escape the immune system and ART. Furthermore, infected macrophages are present in lung and duodenal tissues of patients receiving ART [44,45,46]. Macrophages are therefore important HIV targets that can serve as a sanctuary for viral persistence. However, less attention has been given to macrophage persistent infection compared to studies of latent and persistent infection in T cells. This could be due to the difficulties of accessing macrophages in human tissues for thorough investigations.
The induction of a progressive depletion of T cells leading to immune dysfunction and the formation of a viral reservoir are a hallmark of HIV infection [47,48]. The cytopathic effects that lead to T-cell depletion are induced by several mechanisms. Infected macrophages, on the other hand, are relatively resistant to the cytopathic effect and consequently play an essential role in viral dissemination to host tissues and organs [49,50,51,52,53,54]. Current evidence indicates that the sustained persistent infection of macrophages, contrary to the productive infection of CD4+ T cells, is due to differences with HIV protein trafficking and virus release between the two cell types [55,56,57]. In macrophages, HIV assembles and matured viral particles accumulate in intracellular compartments [56,58,59,60,61,62,63]. Other studies have described the plasma membrane to be the primary site of virus assembly and budding in macrophages [64,65,66]. Emerging studies brings these two different observations together and reveal that HIV assembles and accumulates in intracellular compartments and is connected to the extracellular space [67,68]. Intracellular virus maturation in macrophages protects HIV from immune responses and helps the virus to persist in patients under ART. Furthermore, in this viral reservoir, HIV infection appears to not be associated with apoptosis but with a chronic productive infection [69,70]. In support of this observation, evidence has been established for chronically infected circulating monocytes in which there is a steady stable expression of antiapoptotic genes [71]. The half-life of infected macrophages is, therefore, substantially longer than that of T cells [53,54]. As a result, these cells continue to accumulate replication-competent HIV for prolonged periods of time, even in patients receiving ART [52]. We still do not have a complete picture as to the mechanism by which these persistently infected cells can promote an antiapoptotic environment while T cells cannot. Furthermore, it is not clear whether a lack of apoptosis is related to persistent infection in macrophages.
The relationship between HIV and host factors determines the modulation of cellular function and replication of the virus within an infected individual. Interaction of these viral and cellular proteins is evident in all steps of virus replication and their associations may be an important factor in the modification of host cell functions during a chronic viral infection [49,52,72,73,74]. HIV has also managed strategies that counter host innate viral restriction factors and consequently establish persistent infection [75,76,77,78,79]. There is a growing list of restriction factors that suppresses virus replication which include apolipoprotein B messenger RNA (mRNA) editing enzyme catalytic polypeptide-like (APOBEC) 3F and G, tripartite motif protein 5 alpha (TRIM5α) and TRIMcyp, sterile alpha motif histidine/aspartic 1 (SamHD1), and tetherin [75,76,77,78,79]. These factors restrict HIV at different stages of replication. APOBEC gets packaged into viral particles and inhibits viral copy DNA (cDNA) synthesis by affecting the processivity of reverse transcription and by causing the inactivation of G-to-A hypermutations in the proviral genome [80,81]. TRIM5α targets incoming HIV capsids and blocks viral replication by preventing viral cDNA synthesis [82]. Thetherin is a type II transmembrane protein that restricts the propagation of many enveloped viruses including HIV by tethering progeny budding virions onto the plasma membrane [83,84]. This consequently prevents virus release. SamHD1 suppresses reverse transcription through the depletion of nucleoside pools required for effective cDNA synthesis [85,86]. It may also repress reverse transcription by degrading viral RNA. HIV and simian immune deficiency virus (SIV) have managed to counter these restriction factors by accessory proteins. The HIV viral infectivity factor (VIF) protein, which is essential for effective propagation of the virus in vivo, prevents the encapsidation of APOBEC into virions [81]. The antagonist to tetherin is the viral protein U (Vpu) for the HIV-1 strains and viral negative factor (Nef) for other primate lentiviruses [78,83,84]. Viral protein X or R (Vpx or Vpr) counter the antiviral activity of SAMHD1 for HIV-2 and SIV [85,86]. Additional cellular antiviral factors with relevance beyond HIV include interferon-induced transmembrane (IFITM) proteins, cholesterol 25-hydroxylase (CH25H), KRAB-associated protein-1/TRIM28 (KAP1/TRIM28), 90K, putative helicase moloney leukemia 10 homolog (MOV10), interferon-induced GTP-binding protein (MxB), Schlafen family member 11 (SLFN11), and zinc-finger antiviral protein (ZAP) [76]. HIV can also counter these antiviral activities and establish infection. Therefore, the persistent infection and survival of macrophages is potentially regulated by the contest between viral and cellular factors at different steps in virus replication, implying that there may be several mechanisms for HIV longevity in macrophages. Gene expression profiles that are unique to macrophages [71,87,88] when compared to those of activated CD4+ T cells should help determine the mechanism of persistent infection in macrophages. One molecule with multiple functions that is expressed in macrophages while being absent in T cells is caveolin 1 (Cav-1). This review will cover the functional importance of Cav-1 in HIV replication and its potential contribution to HIV persistence and pathogenesis.
2. Caveolin 1 and Its Function
Caveolin 1 (Cav-1), a 21–24-kDa scaffolding protein, is an important structural component of the caveolae organelle [89]. Caveolae are flask-shaped small invaginations of 50–100 nm diameter in the plasma membrane that are highly enriched in cholesterol, phospholipids, and sphingolipids, and are abundant in various cell types [90,91,92,93,94]. Cav-1 is highly expressed in terminally differentiated or quiescent cells including muscle cells, adipocytes, endothelial cells, monocytes, macrophages, dendritic cells, microglia, and astrocytes, while human T cells appear to lack the Cav-1 protein [90,91,92,93,94,95,96,97,98,99,100,101]. Along with Cav-1, the caveolae structure is composed of Cav-2 and Cav-3 as well as four additional proteins known as cavin 1–4 [102,103,104]. Cav-1 and Cav-2 are found in abundance in most cells of the cardiovascular system, whereas Cav-3 is limited to skeletal muscle and some smooth muscle cells [103,105,106]. For caveolae structural integrity, Cav-1 or Cav-3 is important, while Cav-2 is dispensable [99,107,108,109,110]. The role of Cav-2 is less well defined. Cavins are important as regulators of caveolin and are required for the assembly and function of caveolae [104]. Recent electron cryomicroscopy studies revealed a regular polyhedron architecture of caveolae with cavins [111]. The caveolar architecture is connected with unstructured cavin filaments by coiled-coil domains into a polygonal net-like complex. This complex is believed to provide scaffolding for compartmented cellular processes and participates in multiple cellular functions, including endocytosis, transcytosis, membrane homeostasis, inflammation, and signal transduction [94,104,111,112,113,114,115,116,117,118,119,120,121].
The mechanisms of the multiple functions described for caveolae are not fully understood and remain controversial. These are further complicated by the findings and emerging evidence that caveolae serve as mechanosensing organelles and may play a role in the protection of cells from mechanical stress by stretching or internalizing the caveolae structure [122,123,124,125]. Caveolae are present in abundance in mechanically stressed cells such as muscle cells, fibroblasts, endothelial cells, and adipocytes compared to other cell types, strengthening their role in the protection of cells from mechanical stress [124,126]. Therefore, the many different functions described previously have to be reexamined in concert with the model of mechanosensing to establish a complete understanding of the role of caveolae in cell physiology.
Cav-1 is also present in cells independent of the caveolae structure, suggesting additional cellular functions. Along with being a component of caveolae, Cav-1 is involved in several cellular processes that include cell cycle regulation, cholesterol trafficking and efflux, senescence, signal transduction, angiogenesis, endocytosis, transcytosis, and apoptosis (Table 1) [95,127,128,129,130,131,132]. Multiple lines of evidence indicate that Cav-1 interacts with a variety of signal molecules such as Src tyrosine kinases, glycosylphosphatidylinositol linked receptors, small guanosine triphosphate hydrolyzing enzymes (GTPases, heteromeric G protein, ion channels, endothelial nitric oxide synthase (eNOS), protein kinase A, and mitogen-activated protein kinases [132,133,134]. Cav-1, therefore, acts as a scaffolding molecule and can directly associate and modulate several signal transducing molecules.
3. Cav-1 Mediated HIV Inhibition
The multifaceted functions of Cav-1 that include signal transduction, cell division, and cholesterol homeostasis suggest that Cav-1 has functional relationships with virus replications and viral induced pathogenesis. The first evidence that Cav-1 may play a role in HIV replication is the demonstration of the inhibition of HIV particle production from provirus-transfected cells [135]. Further studies showed that the level of group specific antigen (Gag) production was significantly reduced. This observation, and the fact that Cav-1 is expressed in macrophages while being absent in T cells, prompted the idea that Cav-1 can restrict HIV replication and consequently contribute to macrophage HIV persistent infection. Since Cav-1 has multiple functions, the mechanisms of HIV inhibition by Cav-1 can be complex and involve multiple steps in virus replication. The finding that Gag production is reduced in cells expressing Cav-1 suggests that one mechanism of the inhibition of HIV replication by Cav-1 can be the post integration of the proviral DNA. In fact, Wang et al. demonstrated that Cav-1 inhibits HIV replication at the transcriptional level in macrophages [136]. Site specific mutational analysis of the HIV long terminal repeat (LTR) cis-acting elements reveals that the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) is important for Cav-1 mediated repression of HIV transcription. The two NF-κB sites in the LTR have to be mutated to abrogate the transcriptional inhibition of Cav-1. Further studies showed that Cav-1 affects the NF-κB pathway by reducing the phosphorylation/activation of the Inhibitor of NF-κB kinase subunit beta (IKKβ), IKK alpha (IKKα), inhibitor of kappa B (IκBα), and p65 as well as subsequent translocation of the NF-κB p65 protein into the nucleus. This consequently decreases the level of p65 binding to target DNA and HIV transcription. The finding that IKKα and IKKβ phosphorylation is reduced implies that the influence of Cav-1 on the NF-κB pathway is upstream of the IKK activation step. Simmons et al. reported similar results showing that Cav-1 inhibits HIV replication by influencing the NF-κB pathway and reducing HIV transcription [137]. Their finding reveals that the mechanism of transcription inhibition is mediated by Cav-1 induced hypoacylation of NF-κB. Further studies by Simmons et al. reveals no reduction in nucleus translocation of NF-κB p65 and binding to target DNA. The discrepancy of these findings with the study by Wang et al., in which they found that Cav-1 reduced nucleus translocation of NF-κB and binding to target DNA, is not clear. However, the discovery by both groups reveals and convincingly establishes that HIV transcription repression by Cav-1 involves the NF-κB pathway.
The NF-κB pathway is involved in the broad regulation of gene expressions including pro-inflammatory molecules. Cav-1, therefore, can be an important direct and/or indirect regulator of the innate and adaptive immune systems. Immune activation plays a central role in T cell depletion by high turnover of both CD4+ and CD8+ cells, resulting in a shorter half-life of T cells during HIV infection [138,139,140,141]. Increased serum levels of pro-inflammatory cytokines and chemokines are also a consequence of immune activation [142]. The significant gastrointestinal (GI) tract damage due to HIV infection has been linked to immune activation and microbial translocation to the blood circulation with heightened levels of circulating lipopolysaccharide (LPS) [143,144,145,146]. Microbial translocation can influence HIV disease progression partly by the LPS triggering of monocyte activation by way of CD14 and Toll like receptor (TLR) 4-mediated signaling, resulting in a release of soluble CD14 and pro-inflammatory cytokines [145,146]. Further studies suggest a correlation of plasma LPS levels with T-cell activation markers indicating that T-cell activation is an indirect consequence of LPS induced monocyte stimulation, subsequently resulting in the immune activation observed in HIV infected individuals [145,147]. LPS binding to the extracellular domain of TLR4 initiates the recruitment of adaptors triggering signal-transduction cascades, which eventually leads to the activation of transcription factor NF-κB [148,149,150]. The recruitment of adaptors also activates mitogen-activated protein kinases (MAPKs) resulting in the activation of activator protein 1 (AP-1) transcription as well as the activation of interferon response element 3 (IRF-3). These subsequently enhance the transcription of pro-inflammatory molecules, type 1 interferon, and chemokines. Interestingly, LPS is shown to up-regulate Cav-1 expression in macrophages and Cav-1 subsequently blocks the TLR4 pathway by interacting with TLR4 molecules [151,152,153]. The production of pro-inflammatory molecules is tightly regulated by factors that promote the inhibition of enhanced expression, thereby resolving inflammation [149,154,155,156,157]. The finding that Cav-1 suppresses HIV transcription through NF-κB and Cav-1 blocks the TLR4 pathway suggests a role for Cav-1 in regulating inflammatory responses. Although there is an overall induction of inflammatory molecules during HIV infection, Cav-1 may be involved in the regulation of cytokine storms seen after infection.
HIV induced immune activation also leads to the clonal exhaustion of T cells, causing a reduction in memory T cell populations [158,159,160]. Interaction of programed death 1 (PD-1) with its ligand such as PD-L1 or PD-L2 delivers an inhibitory signal to T cells that affects cell proliferation and cytokine production [161]. HIV infection enhances the expressions of PD-1 in T cells and PD-L1 and PD-L2 in macrophages [161,162,163,164]. PD-1 engagement with its ligands has been described to play a role in T cell exhaustion as a result of chronic HIV infection [162,165,166]. The NF-κB signaling pathway is a key participant of the induction of PD-L1 expression in macrophages [167]. Furthermore, LPS up-regulates the expression of PD-L1 through TLR4 mediated NF-κB activation and the four potential NF-κB binding sites on the PD-L1 promoter [167,168]. Since Cav-1 inhibits the NF-κB and TLR4 pathways, it may have an essential role during HIV infection in regulating the PD-1/PD-L1 interactions influencing T cell exhaustion. The role of Cav-1 in regulating the PD-1/PD-L1 pathway, however, could be masked due to continuous antigen stimulations, tipping the balance toward the T-cell exhaustion phenotype.
4. HIV Induces Cav-1 Up-Regulation
The associations of restriction factors with HIV replication may be important in the modification of host cell processes during a chronic viral infection and the establishment of viral persistence. Along with the conventional innate antiviral response, these factors can serve as a first line defense against HIV infection. The counter by the HIV accessory proteins, however, leads to a robust replication of the virus and potentially could contribute to HIV persistent infection in vivo [76,77,78,79]. These restriction factors are constitutively expressed and/or can be induced by interferon during viral replication depending on the cell type [75,76,77]. Low-level constitutive expression of Cav-1 is evident in macrophages, microglial cells, and astrocytes [169,170,171]. It is not clear whether Cav-1 can be induced by interferon during virus infection. However, there are several molecules including LPS that modulate the expression of Cav-1 by different mechanisms. LPS stimulates Cav-1 expression in macrophages and endothelial cells [172]. Similarly, macrophage treatment with oxidized low-density lipoprotein (oxLDL) or simvastatin up-regulates the expression of Cav-1 [173,174]. In addition, the induction or repression of Cav-1 expression has been observed by different cellular factors at the transcriptional level [175,176,177,178]. Interestingly, HIV infection up-regulates the expression of Cav-1 in macrophages [169]. Cav-1 up-regulation by HIV infection and the observation that the overexpression of Cav-1 inhibits virus replication [135,179] suggests that Cav-1 participates in maintaining a low-level persistent infection of macrophages in a feedback loop (Figure 1). Although distinct, such a mechanism of virus repression appears to be similar to the innate immune response where the virus infection stimulates restriction factors and consequently leads to inhibition of virus replication. Similarly, unrelated to HIV, the overexpression of Cav-1 is shown to suppress NF-κB activation in murine macrophages [180]. Furthermore, human cancer cell lines treatment with growth hormone-releasing hormone (GHRH) antagonist MIA-602 show an increase in Cav-1 expression with a consequence of down-modulation of NF-κB [181]. These observations support the finding that the inhibition of HIV replication by suppressing NF-κB activity is due to enhanced Cav-1 expression during HIV infection.
The mechanisms of the stimulation of Cav-1 expression during HIV infection can be complex and indirect influence of viral protein activities on cellular pathways. Lin et al. has shown that HIV infection up-regulates the expression of Cav-1 at the transcriptional level and the HIV transactivator protein (Tat) is responsible for the enhancement of Cav-1 expression [169]. There is limited information as to how Tat up-regulates the expression of Cav-1. Cis-acting elements in the Cav-1 gene promoter include sequences for the binding transcription factors specific protein 1 (Sp1), transcription factor E2F, and NF-κB, as well as G/C rich box consensus for sterol response elements binding protein 1 (SREBP-1) and p53 [182,183,184,185]. The complex formations and binding of p53, E2F, Sp1, and SREBP1 to the promoter region activates Cav-1 expression [182,183,184]. Thus far, limited analysis of these factors for HIV or Tat mediated Cav-1 up-regulation reveal that reducing the level of Sp1 by targeting with small interfering RNA (siRNA) has no influence [169]. However, p53 activity is essential for Tat mediated induction of Cav-1 expression and correlates with enhanced phosphorylation of p53 Ser residues at amino acid positions 15 and 46. The requirement of p53 activity is not clear and needs further studies to understand the mechanisms of Tat mediated Cav-1 up-regulation. Both LPS and statin promote SREBP activation in macrophages [186,187], and this activation could enhance the SREBP binding to the Cav-1 promoter with the subsequent induction of Cav-1 expression. HIV infection leading to microbial translocations into the blood stream with elevated levels of LPS thus may result in increased Cav-1 expression by inducing SREBP binding to the Cav-1 promoter. Similarly, statins are often used to treat dyslipidemias associated with HIV disease and this may also promote Cav-1 up-regulation by enhanced SREBP interaction with the Cav-1 promoter.
An important factor that has relevance to Cav-1 up-regulation is oxidative stress which is a central contributing priming cause to many parameters leading to pathogenesis in HIV infected individuals, whether patients are under ART treatment or not. Several studies have shown that oxidative stress enhances the expression of Cav-1 [131]. p38 MAPK, Sp1, and NF-κB, cyclooxygenase 2 (COX2), and phosphatidycholine-specific phospholipase activates cav-1 gene promoter during oxidative stress resulting in enhanced Cav-1 expression [172,188,189,190,191]. The HIV proteins Tat, Nef, Vpr, and Gp120 have been shown to independently increase reactive oxygen species (ROS) while decreasing antioxidants, establishing HIV-mediated oxidative stress [192]. Interestingly, the inhibition of p38 MAPK can block HIV or Tat alone mediated up-regulation of Cav-1 [169]. Furthermore, the inhibition of p38 MAPK can suppress the phosphorylation of p53 in the presence of Tat and subsequently decreases Cav-1 up-regulation. These findings imply that Tat’s effect on Cav-1 expression is indirect without physical association with the Cav-1 promoter and possibly involves HIV/Tat induced oxidative stress. During HIV infection it is likely that there is a functional cross-link with molecules and pathways that enhance the Cav-1 expression. Zhong et al. described caveolae-associated signaling in the disruption of the cellular tight junctions of the human brain microvascular endothelial cells upon Tat exposure [193]. The disruption in tight junctions correlates with Tat activated RAS and RhoA along with Cav-1 up-regulation, leading a decrease in junction proteins. The silencing of Cav-1 reduced the effect of caveolae associated signaling, implying a role for Cav-1 in the disruption of those cell-to-cell junctions. Human brain endothelial cells co-cultured with HIV infected cells show an induction of phosphorylation of extracellular signal–regulated kinases (ERK) 1/2 and Akt with subsequent activation of Sp1, AP-1, and NF-κB transcription that leads to an increase of the matrix methalloproteinases 9 (MMP-9) promoter and enzyme activity [194,195,196]. Silencing Cav-1 with siRNA treatment attenuates the HIV induced phosphorylation of ERK/Akt and MMP-9 activity. The ERK1/2 and Akt pathways are stimulated in response to oxidative stress, which subsequently enhance the expression of the MMP9 protein [197]. Thus, enhancing Cav-1 expression during HIV infection may involve Tat induced oxidative stress along with other mechanisms of HIV mediated oxidative stress. Such stimulated Cav-1 expression is, therefore, one of the likely host factors that HIV modifies in its effort to establish a persistent infection.
5. Cav-1 Mediated Cholesterol Balance and Role in HIV Macrophage Infection
Cholesterol trafficking is a complex event in which the molecular pathways are controlled by several molecules that include Cav-1, SREBP-1, ATP-binding membrane cassette transport protein A1 (ABCA1) and G1 (ABCG1), and scavenger receptor B1 (SR-B1) [198,199,200,201,202,203]. Since Cav-1 is critical in the formation and structural integrity of caveolae, optimal levels of cholesterol are important in caveolae for efficient compartmented cellular processes and downstream signaling [94,204,205,206]. Cholesterol depletion can result in the disruption of efficient communication of the cellular processes [207,208,209,210]. Cav-1 plays an essential role in maintaining cholesterol balance [94,120,204,211,212,213,214]. It mediates the transport of newly synthesized cholesterol from the endoplasmic reticulum (ER) to the plasma membrane [204,205,215,216,217,218,219,220,221] and indirectly influences the transfer to extracellular acceptors such as high-density lipoprotein (HDL) or lipid free apolipoprotein A-I (apoA-I). Cav-1 is, therefore, an important molecule in the maintenance of cellular cholesterol homeostasis. Furthermore, Cav-1 is shown to interact with sterol carrier protein-2 (SCP-2) and this protein is also involved in cholesterol transfer from the ER to the plasma membrane [222,223]. ABCA1 participates in cholesterol efflux to apoA-I through the reorganization of plasma membrane microdomains [224,225,226,227].
Cav-1 can influence HIV replication through its role in cholesterol homeostasis. Cholesterol is an important structural component that modulates the fluidity of biological membranes and is critical for the uptake of HIV as well as the budding of virus particles from infected cells [228,229,230,231,232,233,234]. Its depletion significantly reduces HIV particle production. There is also a marked decrease in the infectivity of virions produced from such cells [235]. Therefore, the level of membrane cholesterol composition influences HIV production and virus infectivity. The increase in Cav-1 in macrophages during HIV infection can result in enhanced cholesterol transport to the cell membrane, facilitating increased efflux. This can lead to the depletion of cholesterol, subsequently decreasing virus production. In fact, Lin et al. have demonstrated a reduction in virus production that correlates with enhanced cholesterol efflux in cells overexpressing Cav-1 [236]. Virus particles released from these cells have a decreased cholesterol composition and lower infectivity capacity.
HIV manipulates cholesterol metabolism in order to produce a sufficient supply of cholesterol for efficient virus production [229,235,237,238]. The HIV accessory protein Nef plays an essential role in altering cholesterol metabolism to the benefit of HIV replication [239,240]. Nef impairs ABCA-1 dependent cholesterol efflux by apoA-l [241]. Further studies by Lin et al. reveal that Cav-1 counters Nef and enhances apoA-I mediated cholesterol efflux, resulting in the inhibition of HIV replication [236]. The exact mechanism by which Cav-1 counters impaired cholesterol efflux by Nef is not clear. Nef can down-regulate the expression of ABCA-1 as well as alter its cellular distribution [241]. Such changes in ABCA-1 can impair apoA-I mediated cholesterol efflux. The physical interaction of ABCA-1 and Nef has been established [241,242,243]. However, this interaction does not appear to be important for the down-modulation of ABCA-1. Nef induces degradation of ABCA-1 by proteaosomal activity and/or other undiscovered mechanisms are suggested as a possible explanation for the down-modulation of ABCA-1 [242]. Cav-1 is also shown to co-immunoprecipitate with Nef, implying a potential physical association [236]. It remains to be determined whether this potential association counters the down-regulation of ABCA-1 expression. ABCA-1 is reduced in Cav-1 defective animals, suggesting that Cav-1 positively promotes the expression of ABCA-1 [204]. However, in cells overexpressing Cav-1, the level of ABCA-1 does not change as compared to cells expressing normal levels of Cav-1 [236]. In HIV infected cells, Tat up-regulates Cav-1 while Nef down modulates ABCA-1 expression [169,241]. The mechanism by which Cav-1 restores impaired ABCA-1 dependent cholesterol efflux by apoA-l could therefore be complex and may not have to do with the expression levels of ABCA-1. Nonetheless, it is clear from the studies by Lin et al. [236] that Cav-1 can inhibit HIV replication in macrophages by promoting apoA-I mediated cholesterol efflux and thereby could contribute to a low-level viral replication and persistence in macrophages (Figure 1).
Relevant to the role of Cav-1 in cholesterol mediated HIV inhibition, there is also a significant suppression of envelope (Env) induced membrane hemifusion by Cav-1. Reduction in virion infectivity caused by cholesterol depletion is mainly due to the effect on the fusion step during infection [234,244]. The HIV Env interacts with Cav-1 via the gp41 trans-membrane domain [245,246,247]. This interaction is mediated by the Cav-1 scaffolding domain and WNNMTWMQW in the ectodomain (in the C-terminal heptad repeat region) of HIV transmembrane envelope glycoprotein Gp41 [245,246]. Membrane fraction analysis reveals that the binding of Cav-1 with HIV Env appears to be at the plasma membrane of the caveolae lipid raft [247]. Interaction of these two molecules at the plasma membrane blocks HIV envelope mediated fusion with target cells and reduces virus replication. The ability of Cav-1 to block Env mediated hemifusion and its up-regulation by HIV infection suggests that the Cav-1 interaction with Env, possibly, in concert with enhanced cholesterol efflux, blocks virus production and infectivity (Figure 1).
6. HIV Infection and Influence on Aortic Endothelial Cell Cav-1 Function
Cav-1 plays a key role in several important endothelial cell functions including innate immunity and inflammation, vascular permeability, and leukocyte migrations [153,248,249,250,251,252,253,254]. HIV infection is associated with endothelial dysfunction and increased expression of inflammatory cytokines and adhesion molecules, which results in recruitment and activation of leukocytes and platelets [255,256,257,258]. In addition, HIV infection can lead to pulmonary artery hypertension (PAH) and atherosclerosis [259,260,261,262]. In nonhuman primate models, PAH is observed with the infection of chimeric SIV containing the HIV Nef (SHIV), while the control SIV shows no PAH, suggesting a role for Nef in PAH pathology [263]. Other studies show a significant increase in superoxide release during ex vivo exposure of porcine pulmonary arteries or human pulmonary artery endothelial cells to Nef with concurrent decreases in eNOS and nitric oxide (NO) production [264]. The reduction in NO leads to a decrease in vasorelaxation. In vivo administration of NO can diminish PAH [260,261,262]. Since Cav-1 and caveolae are abundant and play essential roles in endothelial cell function, there has to be link with HIV induced endothelial dysfunction. It is well established that NO is a critical molecule in vascular physiology [265,266,267,268]. Cav-1 is a regulator of eNOS. Depending on cell physiology, Cav-1 inhibits the function of eNOS and negatively regulates the production of NO [269,270,271,272]. Interestingly, mutation in Cav-1 has been linked to generalized lipodystrophy (CGL) and PAH [273,274,275,276]. However, whether there is a direct correlation of HIV or Nef induced PAH with Cav-1 remains to be determined.
A recent finding show that the co-culture of aortic endothelial cells with HIV infected cells promotes redistribution of endothelial Cav-1 leading to the disruption of HDL mediated cholesterol efflux [277]. Further studies reveal, although with a high dose used, that recombinant Nef exerts similar effects on the redistribution of Cav-1 and impacts the HDL mediated cholesterol efflux. Comparative investigations between wild type and Nef defective HIV reveal no significant differences in the reduction of HDL mediated cholesterol efflux from endothelial cells, suggesting that multiple factors are involved that include Nef to alter cholesterol efflux. The influence of HIV on Cav-1 redistribution and cholesterol efflux can alter cholesterol homeostasis and membrane molecule compositions which can impact caveolae/Cav-1 functions and the caveolae structure. This subsequently could affect the regulation of eNOS by Cav-1 and bioactive NO production, as well as other endothelial cell functions that can lead to HIV induced pathology (Figure 2). Alternatively, Cav-1 redistribution may be related to the mechanostress induced on endothelial cells by HIV and its proteins along with HIV stimulated alterations in cytokine and chemokine productions in the microenvironment. The internalization of caveolae can repair wounded cells and muscle fibers [278]. The Cav-1 redistribution, therefore, could be due to the internalization of caveolae to repair distressed endothelial cells. In support of this notion, pulmonary dysfunction linked to a lack of caveaole is suggested to be a consequence of loss of mechanoprotection [112]. Thus, the cumulative effect of HIV infection with the alteration of the microenvironment could lead to irreversible mechanostress, leading to endothelial cell dysfunction.
In addition to HIV infection, the cardiac risks in acquired immune deficiency syndrome (AIDS) patients have been linked to ART treatments [279,280,281,282,283,284,285,286,287,288], particularly the previously used protease inhibitors [289,290,291]. Ritonavir decreases the expression of Cav-1 and inhibits cholesterol efflux in macrophage-derived foam cells [292]. Nelfinavir also reduces Cav-1 expression in macrophages [293]. Drug induced accumulation of cholesterol within macrophages due to the inhibition of cholesterol efflux could be related to the reduction of Cav-1 expression. This may be one factor attributed to the progression of atherosclerosis in HIV infected individuals under drug therapy. Endothelial cells may suffer from a similar reduction in Cav-1 due to drug therapy, resulting in endothelial dysfunction.
7. Conclusions
Cav-1 and the caveolae structure may participate in several steps of HIV infection and pathogenesis. The mechanisms of HIV persistent infection in macrophages are not completely understood. There are three possible mechanisms that Cav-1 could contribute to HIV persistent infection in macrophages. HIV infection up-regulates the expression of Cav-1 and the enhanced level of Cav-1 subsequently represses virus replication by suppressing the activity of NF-κB, promoting cholesterol efflux, and blocking the fusion steps of virus infectivity. Thus, through such bidirectional relationships with HIV, Cav-1 can contribute to a low-level HIV persistence in macrophages. Since Cav-1 is also expressed in microglial and astrocytes along with macrophages, it could be a contributing factor to HIV persistence in the central nervous system. However, in vivo data is crucial to confirm that Cav-1 plays an essential role in establishing HIV persistent infections.
The most widely recognized health problems are vascular complications, including coronary heart disease, pulmonary hypertension, and atherosclerosis [279,280,281,282,283,284,285,286,287,288]. Vascular complications also appear to accelerate in HIV infected patients under ART compared to uninfected cardiac patients [294,295]. A similar cardiac disease risk has also been observed in HIV infected individuals without ART treatment [284,286,288,296]. The influence of HIV on Cav-1 mediated cholesterol efflux in both macrophages and aortic endothelial cells is intriguing and requires further investigation. This may be linked to macrophage foam cell formation and endothelial cell dysfunction with the relatively high incidence of cardiovascular disease seen in HIV infected patients. In addition, the inverse relation of Cav-1 with PAH and the link between PAH and Nef are important areas that need more exploration. Furthermore, the induction of the redistribution of Cav-1 by HIV in endothelial cells requires additional studies to determine the possible consequence on endothelial cell functions including caveolae related mechanosensing. Investigations on whether HIV induced Cav-1 redistribution is due to internalization and/or stretching of caveolae, would enhance such notions and open new venues for understanding HIV pathogenesis.
The higher incidence of risks from Non-AIDS events in HIV infected individuals, especially as they get older, can be related in part to alterations in ROS and antioxidant levels that are noted in numerous tissues in HIV infected individuals [192]. In addition, multiple studies suggest that antiretroviral drugs induce ROS production in HIV infected individuals [192]. Since increased ROS production enhances Cav-1 expression, which is a key player of cellular senescence, there may be a link to non-AIDS related risks with Cav-1 mediated cellular senescence. Thus, up-regulation of the multifunctional Cav-1 by elevated ROS production as a consequence of HIV infection and continuous anti-HIV drug treatments may result in premature cellular senescence accumulation overtime, subsequently causing cellular dysfunction and pathology.
Acknowledgments
The author thanks Pankaj Singh and Margaret Hitchcock for reading the manuscript and for their helpful suggestions. The work is supported in part by a grant from the National Institutes of Health (AI39126) to Ayalew Mergia. Publication of this article was funded in part by the University of Florida Open Access Publishing Fund.
Conflicts of Interest
The author declares no competing or financial interests
References
- Chun, T.W.; Moir, S.; Fauci, A.S. HIV reservoirs as obstacles and opportunities for an HIV cure. Nat. Immunol. 2015, 16, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Siliciano, J.D.; Siliciano, R.F. Recent developments in the effort to cure HIV infection: Going beyond n = 1. J. Clin. Investig. 2016, 126, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Kline, C.; Ndjomou, J.; Franks, T.; Kiser, R.; Coalter, V.; Smedley, J.; Piatak, M., Jr.; Mellors, J.W.; Lifson, J.D.; Ambrose, Z. Persistence of viral reservoirs in multiple tissues after antiretroviral therapy suppression in a macaque RT-SHIV model. PLoS ONE 2013, 8, e84275. [Google Scholar] [CrossRef] [PubMed]
- Blankson, J.N.; Persaud, D.; Siliciano, R.F. The challenge of viral reservoirs in HIV-1 infection. Annu. Rev. Med. 2002, 53, 557–593. [Google Scholar] [CrossRef] [PubMed]
- Finzi, D.; Blankson, J.; Siliciano, J.D.; Margolick, J.B.; Chadwick, K.; Pierson, T.; Smith, K.; Lisziewicz, J.; Lori, F.; Flexner, C.; et al. Latent infection of CD4+ T cells provides a mechanism for lifelong persistence of HIV-1, even in patients on effective combination therapy. Nat. Med. 1999, 5, 512–557. [Google Scholar] [PubMed]
- Archin, N.M.; Sung, J.M.; Garrido, C.; Soriano-Sarabia, N.; Margolis, D.M. Eradicating HIV-1 infection: Seeking to clear a persistent pathogen. Nat. Rev. Microbiol. 2014, 12, 750–764. [Google Scholar] [CrossRef] [PubMed]
- Montagna, C.; Mazzuti, L.; Falasca, F.; Maida, P.; Bucci, M.; D’Ettorre, G.; Mezzaroma, I.; Fantauzzi, A.; Alvaro, N.; Vullo, V.; et al. Trends in drug resistance-associated mutations in a real-life cohort of italian patients infected with HIV-1. J. Glob. Antimicrob. Resist. 2015, 3, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Lu, J.; Wang, J.; Yan, H.; Li, J.; Xu, X.; Zhang, Z.; Qiu, T.; Ding, P.; Fu, G.; et al. Prevalence of HIV antiretroviral drug resistance and its impacts on HIV-1 virological failures in Jiangsu, China: A cross-sectional study. Biomed Res. Int. 2016, 2016, 1752437. [Google Scholar] [CrossRef] [PubMed]
- Barral, M.F.; Sousa, A.K.; Santos, A.F.; Abreu, C.M.; Tanuri, A.; Soares, M.A. Identification of novel resistance-related polymorphisms in HIV-1 subtype C RT connection and RNAse H domains from patients under virological failure in brazil. AIDS Res. Hum. Retrovir. 2017, 33, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Little, S.J.; Holte, S.; Routy, J.P.; Daar, E.S.; Markowitz, M.; Collier, A.C.; Koup, R.A.; Mellors, J.W.; Connick, E.; Conway, B.; et al. Antiretroviral-drug resistance among patients recently infected with HIV. N. Engl. J. Med. 2002, 347, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Lucas, G.M. Antiretroviral adherence, drug resistance, viral fitness and HIV disease progression: A tangled web is woven. J. Antimicrob. Chemother. 2005, 55, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Lucas, G.M.; Chaisson, R.E.; Moore, R.D. Highly active antiretroviral therapy in a large urban clinic: Risk factors for virologic failure and adverse drug reactions. Ann. Intern. Med. 1999, 131, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Havlir, D.V.; Bassett, R.; Levitan, D.; Gilbert, P.; Tebas, P.; Collier, A.C.; Hirsch, M.S.; Ignacio, C.; Condra, J.; Gunthard, H.F.; et al. Prevalence and predictive value of intermittent viremia with combination HIV therapy. JAMA 2001, 286, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Havlir, D.V.; Koelsch, K.K.; Strain, M.C.; Margot, N.; Lu, B.; Ignacio, C.C.; Miller, M.D.; Wong, J.K. Predictors of residual viremia in HIV-infected patients successfully treated with efavirenz and lamivudine plus either tenofovir or stavudine. J. Infect. Dis. 2005, 191, 1164–1168. [Google Scholar] [CrossRef] [PubMed]
- Maldarelli, F.; Palmer, S.; King, M.S.; Wiegand, A.; Polis, M.A.; Mican, J.; Kovacs, J.A.; Davey, R.T.; Rock-Kress, D.; Dewar, R.; et al. ART suppresses plasma HIV-1 RNA to a stable set point predicted by pretherapy viremia. PLoS Pathog. 2007, 3, e46. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.; Wiegand, A.P.; Maldarelli, F.; Bazmi, H.; Mican, J.M.; Polis, M.; Dewar, R.L.; Planta, A.; Liu, S.; Metcalf, J.A.; et al. New real-time reverse transcriptase-initiated PCR assay with single-copy sensitivity for human immunodeficiency virus type 1 RNA in plasma. J. Clin. Microbiol. 2003, 41, 4531–4536. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.; Josefsson, L.; Coffin, J.M. HIV reservoirs and the possibility of a cure for HIV infection. J. Intern. Med. 2011, 270, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.Z.; Wightman, F.; Lewin, S.R. HIV reservoirs and strategies for eradication. Curr. HIV/AIDS Rep. 2012, 9, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Chomont, N.; El-Far, M.; Ancuta, P.; Trautmann, L.; Procopio, F.A.; Yassine-Diab, B.; Boucher, G.; Boulassel, M.R.; Ghattas, G.; Brenchley, J.M.; et al. HIV reservoir size and persistence are driven by T cell survival and homeostatic proliferation. Nat. Med. 2009, 15, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Chun, T.W.; Carruth, L.; Finzi, D.; Shen, X.; DiGiuseppe, J.A.; Taylor, H.; Hermankova, M.; Chadwick, K.; Margolick, J.; Quinn, T.C.; et al. Quantification of latent tissue reservoirs and total body viral load in HIV-1 infection. Nature 1997, 387, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Chun, T.W.; Nickle, D.C.; Justement, J.S.; Meyers, J.H.; Roby, G.; Hallahan, C.W.; Kottilil, S.; Moir, S.; Mican, J.M.; Mullins, J.I.; et al. Persistence of HIV in gut-associated lymphoid tissue despite long-term antiretroviral therapy. J. Infect. Dis. 2008, 197, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Cu-Uvin, S.; DeLong, A.K.; Venkatesh, K.K.; Hogan, J.W.; Ingersoll, J.; Kurpewski, J.; De Pasquale, M.P.; D'Aquila, R.; Caliendo, A.M. Genital tract HIV-1 RNA shedding among women with below detectable plasma viral load. AIDS 2010, 24, 2489–2497. [Google Scholar] [CrossRef] [PubMed]
- Thacker, T.C.; Zhou, X.; Estes, J.D.; Jiang, Y.; Keele, B.F.; Elton, T.S.; Burton, G.F. Follicular dendritic cells and human immunodeficiency virus type 1 transcription in CD4+ T cells. J. Virol. 2009, 83, 150–158. [Google Scholar] [CrossRef] [PubMed]
- van Leeuwen, E.; Ter Heine, R.; van der Veen, F.; Repping, S.; Beijnen, J.H.; Prins, J.M. Penetration of atazanavir in seminal plasma of men infected with human immunodeficiency virus type 1. Antimicrob. Agents Chemother. 2007, 51, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Yukl, S.A.; Gianella, S.; Sinclair, E.; Epling, L.; Li, Q.; Duan, L.; Choi, A.L.; Girling, V.; Ho, T.; Li, P.; et al. Differences in HIV burden and immune activation within the gut of HIV-positive patients receiving suppressive antiretroviral therapy. J. Infect. Dis. 2010, 202, 1553–1561. [Google Scholar] [CrossRef] [PubMed]
- Yukl, S.A.; Shergill, A.K.; McQuaid, K.; Gianella, S.; Lampiris, H.; Hare, C.B.; Pandori, M.; Sinclair, E.; Gunthard, H.F.; Fischer, M.; et al. Effect of raltegravir-containing intensification on HIV burden and T-cell activation in multiple gut sites of HIV-positive adults on suppressive antiretroviral therapy. AIDS 2010, 24, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.C.; Onafuwa-Nuga, A.; McNamara, L.A.; Riddell, J.t.; Bixby, D.; Savona, M.R.; Collins, K.L. HIV-1 infects multipotent progenitor cells causing cell death and establishing latent cellular reservoirs. Nat. Med. 2010, 16, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.C.; McNamara, L.A.; Onafuwa-Nuga, A.; Shackleton, M.; Riddell, J., 4th; Bixby, D.; Savona, M.R.; Morrison, S.J.; Collins, K.L. HIV-1 utilizes the CXCR4 chemokine receptor to infect multipotent hematopoietic stem and progenitor cells. Cell Host Microbe 2011, 9, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.R.; Sedaghat, A.R.; Kieffer, T.; Brennan, T.; Lee, P.K.; Wind-Rotolo, M.; Haggerty, C.M.; Kamireddi, A.R.; Liu, Y.; Lee, J.; et al. Residual human immunodeficiency virus type 1 viremia in some patients on antiretroviral therapy is dominated by a small number of invariant clones rarely found in circulating CD4+ T cells. J. Virol. 2006, 80, 6441–6457. [Google Scholar] [CrossRef] [PubMed]
- Keele, B.F.; Tazi, L.; Gartner, S.; Liu, Y.; Burgon, T.B.; Estes, J.D.; Thacker, T.C.; Crandall, K.A.; McArthur, J.C.; Burton, G.F. Characterization of the follicular dendritic cell reservoir of human immunodeficiency virus type 1. J. Virol. 2008, 82, 5548–5561. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.; Muthui, D.; Holte, S.; Nickle, D.; Feng, F.; Brodie, S.; Hwangbo, Y.; Mullins, J.I.; Corey, L. Evidence for human immunodeficiency virus type 1 replication in vivo in CD14(+) monocytes and its potential role as a source of virus in patients on highly active antiretroviral therapy. J. Virol. 2002, 76, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Alexaki, A.; Liu, Y.; Wigdahl, B. Cellular reservoirs of HIV-1 and their role in viral persistence. Curr. HIV Res. 2008, 6, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Alexaki, A.; Wigdahl, B. HIV-1 infection of bone marrow hematopoietic progenitor cells and their role in trafficking and viral dissemination. PLoS Pathog. 2008, 4, e1000215. [Google Scholar] [CrossRef] [PubMed]
- Coleman, C.M.; Wu, L. HIV interactions with monocytes and dendritic cells: Viral latency and reservoirs. Retrovirology 2009, 6, 51. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Smith, T.; Croul, S.; Adeniyi, A.; Rybicka, K.; Morgello, S.; Khalili, K.; Rappaport, J. Macrophage/microglial accumulation and proliferating cell nuclear antigen expression in the central nervous system in human immunodeficiency virus encephalopathy. Am. J. Pathol. 2004, 164, 2089–2099. [Google Scholar] [CrossRef]
- Cosenza, M.A.; Zhao, M.L.; Si, Q.; Lee, S.C. Human brain parenchymal microglia express CD14 and CD45 and are productively infected by HIV-1 in HIV-1 encephalitis. Brain Pathol. 2002, 12, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.; Collman, R.G. CNS inflammation and macrophage/microglial biology associated with HIV-1 infection. J. Neuroimmune Pharmacol. 2009, 4, 430–447. [Google Scholar] [CrossRef] [PubMed]
- Churchill, M.; Nath, A. Where does HIV hide? A focus on the central nervous system. Curr. Opin. HIV AIDS 2013, 8, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Tornatore, C.; Meyers, K.; Atwood, W.; Conant, K.; Major, E. Temporal patterns of human immunodeficiency virus type 1 transcripts in human fetal astrocytes. J. Virol. 1994, 68, 93–102. [Google Scholar] [PubMed]
- Gorry, P.R.; Ong, C.; Thorpe, J.; Bannwarth, S.; Thompson, K.A.; Gatignol, A.; Vesselingh, S.L.; Purcell, D.F. Astrocyte infection by HIV-1: Mechanisms of restricted virus replication, and role in the pathogenesis of HIV-1-associated dementia. Curr. HIV Res. 2003, 1, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Castro, V.; Toborek, M. Infection of human pericytes by HIV-1 disrupts the integrity of the blood-brain barrier. J. Cell. Mol. Med. 2012, 16, 2950–2957. [Google Scholar] [CrossRef] [PubMed]
- Varatharajan, L.; Thomas, S.A. The transport of anti-HIV drugs across blood-CNS interfaces: Summary of current knowledge and recommendations for further research. Antivir. Res. 2009, 82, A99–109. [Google Scholar] [CrossRef] [PubMed]
- Ene, L.; Duiculescu, D.; Ruta, S.M. How much do antiretroviral drugs penetrate into the central nervous system? J. Med. Life 2011, 4, 432–439. [Google Scholar] [PubMed]
- Cribbs, S.K.; Lennox, J.; Caliendo, A.M.; Brown, L.A.; Guidot, D.M. Healthy HIV-1-infected individuals on highly active antiretroviral therapy harbor HIV-1 in their alveolar macrophages. AIDS Res. Hum. Retrovir. 2015, 31, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Zalar, A.; Figueroa, M.I.; Ruibal-Ares, B.; Bare, P.; Cahn, P.; de Bracco, M.M.; Belmonte, L. Macrophage HIV-1 infection in duodenal tissue of patients on long term haart. Antivir. Res. 2010, 87, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.; Mattapallil, J.J. Gastrointestinal tract and the mucosal macrophage reservoir in HIV infection. Clin. Vaccine Immunol. 2014, 21, 1469–1473. [Google Scholar] [CrossRef] [PubMed]
- Gougeon, M.-L. To kill or be killed: How HIV exhausts the immune system. Cell Death Differ. 2005, 12, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Herbein, G.; Kashif, K.A. Is HIV infection a TNF receptor signalling-driven disease? Trends Immunol. 2008, 29, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Gartner, S.; Markovits, P.; Markovitz, D.M.; Kaplan, M.H.; Gallo, R.C.; Popovic, M. The role of mononuclear phagocytes in HTLV-III/LAV infection. Science 1986, 233, 215–219. [Google Scholar] [CrossRef] [PubMed]
- McElrath, M.J.; Pruett, J.E.; Cohn, Z.A. Mononuclear phagocytes of blood and bone marrow: Comparative roles as viral reservoirs in human immunodeficiency virus type 1 infections. Proc. Natl. Acad. Sci. USA 1989, 86, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, J.M.; Fox, C.; Wahl, S.M. Macrophages as a source of HIV during opportunistic infections. Science 1997, 276, 1857–1861. [Google Scholar] [CrossRef] [PubMed]
- Sharova, N.; Swingler, C.; Sharkey, M.; Stevenson, M. Macrophages archive HIV-1 virions for dissemination in trans. EMBO J. 2005, 24, 2481–2489. [Google Scholar] [CrossRef] [PubMed]
- Verani, A.; Gras, G.; Pancino, G. Macrophages and HIV-1: Dangerous liaisons. Mol. Immunol. 2005, 42, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Perno, C.F.; Svicher, V.; Schols, D.; Pollicita, M.; Balzarini, J.; Stefano, A. Therapeutic strategies towards HIV-1 infection in macrophages. Antivir. Res. 2006, 71, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Blom, J.; Nielsen, C.; Rhodes, J.M. An ultrastructural study of HIV-infected human dendritic cells and monocytes/macrophages. Apmis 1993, 101, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Gendelman, H.E.; Orenstein, J.M.; Martin, M.A.; Ferrua, C.; Mitra, R.; Phipps, T.; Wahl, L.A.; Lane, H.C.; Fauci, A.S.; Burke, D.S.; et al. Efficient isolation and propagation of human immunodeficiency virus on recombinant colony-stimulating factor 1-treated monocytes. J. Exp. Med. 1998, 167, 1428–1441. [Google Scholar] [CrossRef]
- Orenstein, J.M.; Meltzer, M.S.; Phipps, T.; Gendelman, H.E. Cytoplasmic assembly and accumulation of human immunodeficiency virus types 1 and 2 in recombinant human colony-stimulating factor-1-treated human monocytes: An ultrastructural study. J. Virol. 1998, 62, 2578–2586. [Google Scholar]
- Orenstein, J.M.; Jannotta, F. Human immunodeficiency virus and papovavirus infections in acquired immunodeficiency syndrome: An ultrastructural study of three cases. Hum. Pathol. 1988, 19, 350–361. [Google Scholar] [CrossRef]
- Demirov, D.G.; Orenstein, J.M.; Freed, E.O. The late domain of human immunodeficiency virus type 1 p6 promotes virus release in a cell type-dependent manner. J. Virol. 2002, 76, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.G.; Booth, A.; Gould, S.J.; Hildreth, J.E. Evidence that HIV budding in primary macrophages occurs through the exosome release pathway. J. Biol. Chem. 2003, 278, 52347–52354. [Google Scholar] [CrossRef] [PubMed]
- Pelchen-Matthews, A.; Kramer, B.; Marsh, M. Infectious HIV-1 assembles in late endosomes in primary macrophages. J. Cell. Biol. 2003, 162, 443–455. [Google Scholar] [CrossRef] [PubMed]
- Chertova, E.; Chertov, O.; Coren, L.V.; Roser, J.D.; Trubey, C.M.; Bess, J.W., Jr.; Sowder, R.C., II; Barsov, E.; Hood, B.L.; Fisher, R.J.; et al. Proteomic and biochemical analysis of purified human immunodeficiency virus type 1 produced from infected monocyte-derived macrophages. J. Virol. 2006, 80, 9039–9052. [Google Scholar] [CrossRef] [PubMed]
- Jouve, M.; Sol-Foulon, N.; Watson, S.; Schwartz, O.; Benaroch, P. HIV-1 buds and accumulates in “nonacidic” endosomes in macrophages. Cell Host Microbe 2007, 2, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Jouvenet, N.; Neil, S.J.D.; Bess, C.; Johnson, M.C.; Virgen, C.A.; Simon, S.M.; Bieniasz, P.D. Plasma membrane is the site of productive HIV-1 particle assembly. PLoS Biol. 2006, 4, 2296–2310. [Google Scholar] [CrossRef] [PubMed]
- Deneka, M.; Pelchen-Matthews, A.; Byland, R.; Ruiz-Mateos, E.; Marsh, M. Macrophages, HIV-1 assembles into an intracellular plasma membrane domain containing the tetraspanins CD81, CD9, and CD53. J. Cell Biol. 2007, 177, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Welsch, S.; Keppler, O.T.; Habermann, A.; Allespach, I.; Krijnse-Locker, J.; Usslich, H.-G.K. HIV-1 buds predominantly at the plasma membrane of primary human macrophages. PLoS Pathog. 2007, 3, 0001–0011. [Google Scholar] [CrossRef] [PubMed]
- Nkwe, D.O.; Pelchen-Matthews, A.; Burden, J.J.; Collinson, L.M.; Marsh, M. The intracellular plasma membrane-connected compartment in the assembly of HIV-1 in human macrophages. BMC Biol. 2016, 14, 50. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Sattentau, Q.J. The HIV-1-containing macrophage compartment: A perfect cellular niche? Trends Microbiol. 2013, 21, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Salahuddin, S.Z.; Rose, R.M.; Groopman, J.E.; Markham, P.D.; Gallo, R.C. Human T lymphotropic virus typeIII infection of human alveolar macrophages. Blood 1986, 68, 281–284. [Google Scholar] [PubMed]
- Guillemard, E.; Jacquemot, C.; Aillet, F.; Schmitt, N.; Barre-Sinoussi, F.; Israel, N. Human immunodeficiency virus 1 favors the persistence of infection by activating macrophages through TNF. Virology 2004, 329, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Giri, M.S.; Nebozyhn, M.; Raymond, A.; Gekonge, B.; Hancock, A.; Creer, S.; Nicols, C.; Yousef, M.; Foulkes, A.S.; Mounzer, K.; et al. Circulating monocytes in HIV-1-infected viremic subjects exhibit an antiapoptosis gene signature and virus- and host-mediated apoptosis resistance1. J. Immunol. 2009, 182, 4459–4470. [Google Scholar] [CrossRef] [PubMed]
- Freed, E.O. HIV-1 and the host cell: An intimate association. Trends Microbiol. 2004, 12, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Malim, M.H.; Emerman, M. HIV-1 accessory proteins. Ensuring viral survival in a hostile environment. Cell Host Microbe 2008, 3, 388–398. [Google Scholar] [CrossRef] [PubMed]
- Wolf, D.; Goff, S.P. Host restriction factors blocking retroviral replication. Annu. Rev. Genet. 2008, 42, 143–163. [Google Scholar] [CrossRef] [PubMed]
- Neil, S.; Bieniasz, P. Human immunodeficiency virus, restriction factors, and interferon. J. Interferon Cytokine Res. 2009, 29, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Kluge, S.F.; Sauter, D.; Kirchhoff, F. Snapshot: Antiviral restriction factors. Cell 2015, 163, 774–774.e1. [Google Scholar] [CrossRef] [PubMed]
- Kirchhoff, F. Immune evasion and counteraction of restriction factors by HIV-1 and other primate lentiviruses. Cell Host Microbe 2010, 8, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Malim, M.H.; Bieniasz, P.D. HIV restriction factors and mechanisms of evasion. Cold Spring Harb. Perspect. Med. 2012, 2, a006940. [Google Scholar] [CrossRef] [PubMed]
- Bergamaschi, A.; Pancino, G. Host hindrance to HIV-1 replication in monocytes and macrophages. Retrovirology 2010, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Sheehy, A.M.; Gaddis, N.C.; Choi, J.D.; Malim, M.H. Isolation of a human gene that inhibits HIV-1 infection and is suppressed by the viral Vif protein. Nature 2002, 418, 646–650. [Google Scholar] [CrossRef] [PubMed]
- Wissing, S.; Galloway, N.L.; Greene, W.C. HIV-1 Vif versus the APOBEC3 cytidine deaminases: An intracellular duel between pathogen and host restriction factors. Mol. Asp. Med. 2010, 31, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Stremlau, M.; Owens, C.M.; Perron, M.J.; Kiessling, M.; Autissier, P.; Sodroski, J. The cytoplasmic body component TRIM5α restricts HIV-1 infection in old world monkeys. Nature 2004, 427, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, N.; Goff, D.; Katsura, C.; Jorgenson, R.L.; Mitchell, R.; Johnson, M.C.; Stephens, E.B.; Guatelli, J. The interferon-induced protein BST-2 restricts HIV-1 release and is downregulated from the cell surface by the viral Vpu protein. Cell Host Microbe 2008, 3, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Neil, S.J.; Zang, T.; Bieniasz, P.D. Tetherin inhibits retrovirus release and is antagonized by HIV-1 Vpu. Nature 2008, 451, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Hrecka, K.; Hao, C.; Gierszewska, M.; Swanson, S.K.; Kesik-Brodacka, M.; Srivastava, S.; Florens, L.; Washburn, M.P.; Skowronski, J. Vpx relieves inhibition of HIV-1 infection of macrophages mediated by the SAMHD1 protein. Nature 2011, 474, 658–661. [Google Scholar] [CrossRef] [PubMed]
- Laguette, N.; Sobhian, B.; Casartelli, N.; Ringeard, M.; Chable-Bessia, C.; Segeral, E.; Yatim, A.; Emiliani, S.; Schwartz, O.; Benkirane, M. SAMHD1 is the dendritic- and myeloid-cell-specific HIV-1 restriction factor counteracted by Vpx. Nature 2011, 474, 654–657. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, N.; Greenwell-Wild, T.; Marinos, N.J.; Swaim, W.D.; Nares, S.; Ott, D.E.; Schubert, U.; Henklein, P.; Orenstein, J.M.; Sporn, M.B.; et al. Human Immunodeficiency Virus Type 1-induced macrophage gene expression includes p21, a target for viral regulation. J. Virol. 2005, 79, 4479–4491. [Google Scholar] [CrossRef] [PubMed]
- Giri, M.S.; Nebozhyn, M.; Showe, L.; Montaner, L.J. Microarray data on gene modulation by HIV-1 in immune cells: 2000–2006. J. Leukoc. Biol. 2006, 80, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Rothberg, K.G.; Heuser, J.E.; Donzell, W.C.; Ying, Y.S.; Glenney, J.R.; Anderson, R.G. Caveolin, a protein component of caveolae membrane coats. Cell 1992, 68, 673–682. [Google Scholar] [CrossRef]
- Palade, G.E. Fine structure of blood capillaries. J. Appl. Phys. 1953, 24, 1424. [Google Scholar]
- Yamada, E. The fine structures of the gall bladder epithelium of the mouse. J. Biophys. Biochem. Cytol. 1955, 1, 445–458. [Google Scholar] [CrossRef] [PubMed]
- Stan, R.V. Structure of caveolae. Biochim. Biophys. 2005, 1746, 334–348. [Google Scholar] [CrossRef] [PubMed]
- Stan, R.V.; Tkachenko, E.; Niesman, I.R. PV1 is a key structural component for the formation of the stomatal and fenestral diaphragms. Mol. Biol. Cell 2004, 15, 3615–3630. [Google Scholar] [CrossRef] [PubMed]
- Parton, R.G.; Simons, K. The multiple faces of caveolae. Nat. Rev. 2007, 8, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Gargalovic, P.; Dory, L. Caveolins and macrophage lipid metabolism. J. Lipid Res. 2003, 44, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Werling, D.; Koss, M.; Monaghan, P.; Taylor, G.; Howard, C.J. Expression of caveolin by bovine lymphocytes and antigen-presenting cells. Immunology 2002, 105, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Quest, A.F.G.; Leyton, L.; Párraga, M. Caveolins, caveolae, and lipid rafts in cellular transport, signaling, and disease. Biochem. Cell. Biol. 2004, 82, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Mercier, I.; Jasmin, J.-F.; Pavlides, S.; Minetti, C.; Flomenberg, N.; Pestell, R.G.; Frank, P.G.; Sotgia, F.; Lisanti1, M.P. Clinical and translational implications of the caveolin gene family: Lessons from mouse models and human genetic disorders. Lab. Investig. 2009, 89, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Fra, A.M.; Williamson, E.; Simons, K.; Parton, R.G. De novo formation of caveolae in lymphocytes by expression of VIP21-caveolin. Proc. Natl. Acad. Sci. USA 1995, 92, 8655–8659. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, M.; Maeda, T.; Ikemoto, T.; Mori, H.; Seya, T.; Shimizu, A. Expression of caveolin-1 in human T cell leukemia cell lines. Biochem. Biophys. Res. Commun. 1998, 253, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, J.; Hardin, C.D. Expression of caveolin-1 in lymphocytes induces caveolae formation and recruitment of phosphofructokinase to the plasma membrane. FASEB J. 2005, 16, 586–587. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.M.; Bastiani, M.; Luetterforst, R.; Kirkham, M.; Kirkham, A.; Nixon, S.J.; Walser, P.; Abankwa, D.; Oorschot, V.M.; Martin, S.; et al. PTRF-Cavin, a conserved cytoplasmic protein required for caveola formation and function. Cell 2008, 132, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Ariotti, N.; Parton, R.G. Snapshot: Caveolae, caveolins, and cavins. Cell 2013, 154, 704–704.e1. [Google Scholar] [CrossRef] [PubMed]
- Chidlow, J.H., Jr.; Sessa, W.C. Caveolae, caveolins, and cavins: Complex control of cellular signalling and inflammation. Cardiovasc. Res. 2010, 86, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Way, M.; Parton, R.G. M-caveolin, a muscle-specific caveolin-related protein. FEBS Lett. 1995, 376, 108–112. [Google Scholar] [CrossRef]
- Tang, Z.; Scherer, P.E.; Okamoto, T.; Song, K.; Chu, C.; Kohtz, D.S.; Nishimoto, I.; Lodish, H.F.; Lisanti, M.P. Molecular cloning of caveolin-3, a novel member of the caveolin gene family expressed predominantly in muscle. J. Biol. Chem. 1996, 271, 2255–2261. [Google Scholar] [PubMed]
- Sowa, G.; Pypaert, M.; Fulton, D.; Sessa, W.C. The phosphorylation of caveolin-2 on serines 23 and 36 modulates caveolin-1-dependent caveolae formation. Proc. Natl. Acad. Sci. USA 2003, 100, 6511–6516. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, U.; Honsho, M.; Parton, R.G.; Simons, K.; Verkade, P. Involvement of caveolin-2 in caveolar biogenesis in MDCK cells. FEBS Lett. 2003, 538, 85–88. [Google Scholar] [CrossRef]
- Drab, M.; Verkade, P.; Elger, M.; Kasper, M.; Lohn, M.; Lauterbach, B.; Menne, J.; Lindschau, C.; Mende, F.; Luft, F.C.; et al. Loss of caveolae, vascular dysfunction, and pulmonary defects in caveolin-1 gene-disrupted mice. Science 2001, 293, 2449–2452. [Google Scholar] [CrossRef] [PubMed]
- Galbiati, F.; Engelman, J.A.; Volonte, D.; Zhang, X.L.; Minetti, C.; Li, M.; Hou, H., Jr.; Kneitz, B.; Edelmann, W.; Lisanti, M.P. Caveolin-3 null mice show a loss of caveolae, changes in the microdomain distribution of the dystrophin–glycoprotein complex, and T-tubule abnormalities. J. Biol. Chem. 2001, 276, 21425–21433. [Google Scholar] [CrossRef] [PubMed]
- Stoeber, M.; Schellenberger, P.; Siebert, C.A.; Leyrat, C.; Helenius, A.; Grunewald, K. Model for the architecture of caveolae based on a flexible, net-like assembly of cavin1 and caveolin discs. Proc. Natl. Acad. Sci. USA 2016, 113, E8069–E8078. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.P.; Nichols, B.J. Caveolae: One function or many? Trends Cell Biol. 2016, 26, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Lisanti, M.P.; Tang, Z.; Scherer, P.E.; Kübler, E.; Koleske, A.J.; Sargiacomo, M. Caveolae, transmembrane signalling and cellular transformation. Mol. Membr. Biol. 1995, 12, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Schlegel, A.; Scherer, P.E.; Lisanti, M.P. Caveolins, a family of scaffolding proteins for organizing “preassembled signaling complexes” at the plasma membrane. J. Biol. Chem. 1998, 273, 5419–5422. [Google Scholar] [CrossRef] [PubMed]
- Kurzchalia, T.V.; Parton, R.G. Membrane microdomains and caveolae. Curr. Opin. Cell Biol. 1999, 11, 424–431. [Google Scholar] [CrossRef]
- Liu, P.; Rudick, M.; Anderson, R.G. Multiple functions of caveolin-1. J. Biol. Chem. 2002, 277, 41295–41298. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.S.; Gao, Z.; Abraham, S.N. Involvement of cellular caveolae in bacterial entry into mast cells. Science 2000, 289, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Pelkmans, L.; Kartenbeck, J.; Helenius, A. Caveolar endocytosis of simian virus 40 reveals a new two-step vesicular-transport pathway to the ER. Nat. Cell Biol. 2001, 3, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.M.; Lisanti, M.P. Caveolin-1 in oncogenic transformation, cancer, and metastasis. Am. J. Physiol. Cell Physiol. 2005, 288, C494–C506. [Google Scholar] [CrossRef] [PubMed]
- Frank, P.G.; Pavlides, S.; Cheung, M.W.; Daumer, K.; Lisanti, M.P. Role of caveolin-1 in the regulation of lipoprotein metabolism. Am. J. Physiol Cell Physiol. 2008, 295, C242–C248. [Google Scholar] [CrossRef] [PubMed]
- Frank, P.G.; Pavlides, S.; Lisanti, M.P. Caveolae and transcytosis in endothelial cells: Role in atherosclerosis. Cell Tissue Res. 2009, 335, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Spisni, E.; Bianco, M.C.; Griffoni, C.; Toni, M.; D'Angelo, R.; Santi, S.; Riccio, M.; Tomasi, V. Mechanosensing role of caveolae and caveolar constituents in human endothelial cells. J. Cell. Physiol. 2003, 197, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Spisni, E.; Toni, M.; Strillacci, A.; Galleri, G.; Santi, S.; Griffoni, C.; Tomasi, V. Caveolae and caveolae constituents in mechanosensing: Effect of modeled microgravity on cultured human endothelial cells. Cell Biochem. Biophys. 2006, 46, 155–164. [Google Scholar] [CrossRef]
- Parton, R.G.; del Pozo, M.A. Caveolae as plasma membrane sensors, protectors and organizers. Nat. Rev. Mol. Cell Biol. 2013, 14, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Echarri, A.; Del Pozo, M.A. Caveolae - mechanosensitive membrane invaginations linked to actin filaments. J. Cell Sci 2015, 128, 2747–2758. [Google Scholar] [CrossRef] [PubMed]
- Nassoy, P.; Lamaze, C. Stressing caveolae new role in cell mechanics. Trends Cell Biol. 2012, 22, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Galbiati, F.; Volonte, D.; Liu, J.; Capozza, F.; Frank, P.G.; Zhu, L.; Pestell, R.G.; Lisanti, M.P. Caveolin-1 expression negatively regulates cell cycle progression by inducing G0/G1 arrest via a p53/p21WAF1/Cip1-dependent mechanism. Mol. Biol. Cell 2001, 12, 2229–2244. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Werling, D.; Hope, J.C.; Taylor, G.; Howard, C.J. Caveolae and caveolin in immune cells: Distribution and functions. Trends Immunol. 2002, 23, 158–164. [Google Scholar] [CrossRef]
- Lee, S.W.; Reimer, C.L.; Oh, P.; Campbell, D.B.; Schnitzer, J.E. Tumor cell growth inhibition by caveolin re-expression in human breast cancer cells. Oncogene 1998, 16, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Uittenbogaard, A.; Everson, W.V.; Matveev, S.V.; Smart, E.J. Cholesteryl ester is transported from caveolae to internal membranes as part of a caveolin-annexin II lipid-protein complex. J. Biol. Chem. 2002, 277, 4925–4931. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Stoppani, E.; Volonte, D.; Galbiati, F. Caveolin-1, cellular senescence and age-related diseases. Mech. Ageing Dev. 2011, 132, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Lamaze, C.; Torrino, S. Caveolae and cancer: A new mechanical perspective. Biomed. J. 2015, 38, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.H.; Murray, F.; Insel, P.A. Caveolae as organizers of pharmacologically relevant signal transduction molecules. Annu. Rev. Pharmacol. Toxicol. 2008, 48, 359–391. [Google Scholar] [CrossRef] [PubMed]
- Fridolfsson, H.N.; Roth, D.M.; Insel, P.A.; Patel, H.H. Regulation of intracellular signaling and function by caveolin. FASEB J. 2014, 28, 3823–3831. [Google Scholar] [CrossRef] [PubMed]
- Llano, M.; Kelly, T.; Vanegas, M.; Peretz, M.; Peterson, T.E.; Simari, R.D.; Poeschla, E.M. Blockade of human immunodeficiency virus type 1 expression by caveolin-1. J. Virol. 2002, 76, 9152–9164. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-M.; Nadeau, P.E.; Lin, S.; Abbott, J.E.; Mergia, A. Caveolin 1 inhibits HIV replication by transcriptional repression mediated through NF-κB. J. Virol. 2011, 85, 5483–5493. [Google Scholar] [CrossRef] [PubMed]
- Simmons, G.E., Jr.; Taylor, H.E.; Hildreth, J.E. Caveolin-1 suppresses human immunodeficiency virus-1 replication by inhibiting acetylation of NF-κB. Virology 2012, 432, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, J.A.; Lempicki, R.A.; Sidorov, I.A.; Adelsberger, J.W.; Herpin, B.; Metcalf, J.A.; Sereti, I.; Polis, M.A.; Davey, R.T.; Tavel, J.; et al. Identification of dynamically distinct subpopulations of T lymphocytes that are differentially affected by HIV. J. Exp. Med. 2001, 194, 1731–1741. [Google Scholar] [CrossRef] [PubMed]
- McCune, J.M.; Hanley, M.B.; Cesar, D.; Halvorsen, R.; Hoh, R.; Schmidt, D.; Wieder, E.; Deeks, S.; Siler, S.; Neese, R.; et al. Factors influencing T-cell turnover in HIV-1-seropositive patients. J. Clin. Investig. 2000, 105, R1–R8. [Google Scholar] [CrossRef] [PubMed]
- Hellerstein, M.; McCune, J. T cell turnover in HIV-1 disease. Immunity 1997, 7, 583–589. [Google Scholar] [CrossRef]
- Hellerstein, M.; Hanley, M.B.; Cesar, D.; Siler, S.; Papageorgopoulos, C.; Wieder, E.; Schmidt, D.; Hoh, R.; Neese, R.; Macallan, D.; et al. Directly measured kinetics of circulating T lymphocytes in normal and HIV-1-infected humans. Nat. Med. 1999, 5, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Valdez, H.; Lederman, M.M. Cytokines and cytokine therapies in HIV infection. AIDS Clin. Rev. 1998, 1997–1998, 187–228. [Google Scholar]
- Epple, H.J.; Schneider, T.; Troeger, H.; Kunkel, D.; Allers, K.; Moos, V.; Amasheh, M.; Loddenkemper, C.; Fromm, M.; Zeitz, M.; et al. Impairment of the intestinal barrier is evident in untreated but absent in suppressively treated HIV-infected patients. Gut 2009, 58, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Nazli, A.; Chan, O.; Dobson-Belaire, W.N.; Ouellet, M.; Tremblay, M.J.; Gray-Owen, S.D.; Arsenault, A.L.; Kaushic, C. Exposure to HIV-1 directly impairs mucosal epithelial barrier integrity allowing microbial translocation. PLoS Pathog. 2010, 6, e1000852. [Google Scholar] [CrossRef] [PubMed]
- Brenchley, J.M.; Price, D.A.; Schacker, T.W.; Asher, T.E.; Silvestri, G.; Rao, S.; Kazzaz, Z.; Bornstein, E.; Lambotte, O.; Altmann, D.; et al. Microbial translocation is a cause of systemic immune activation in chronic HIV infection. Nat. Med. 2006, 12, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Ancuta, P.; Kamat, A.; Kunstman, K.J.; Kim, E.Y.; Autissier, P.; Wurcel, A.; Zaman, T.; Stone, D.; Mefford, M.; Morgello, S.; et al. Microbial translocation is associated with increased monocyte activation and dementia in AIDS patients. PLoS ONE 2008, 3, e2516. [Google Scholar] [CrossRef] [PubMed]
- Cassol, E.; Malfeld, S.; Mahasha, P.; van der Merwe, S.; Cassol, S.; Seebregts, C.; Alfano, M.; Poli, G.; Rossouw, T. Persistent microbial translocation and immune activation in HIV-1-infected south africans receiving combination antiretroviral therapy. J. Infect. Dis. 2010, 202, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.; Kawai, T.; Akira, S. Toll-like receptors and innate immunity. Biochem. Biophys. Res. Commun. 2009, 388, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Akira, S. The role of pattern-recognition receptors in innate immunity: Update on toll-like receptors. Nat. Immunol. 2010, 11, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Akira, S. Toll-like receptors and their crosstalk with other innate receptors in infection and immunity. Immunity 2011, 34, 637–650. [Google Scholar] [CrossRef] [PubMed]
- Lei, M.G.; Morrison, D.C. Differential expression of caveolin-1 in lipopolysaccharide-activated murine macrophages. Infect. Immun. 2000, 68, 5084–5089. [Google Scholar] [CrossRef] [PubMed]
- Lei, M.G.; Tan, X.; Qureshi, N.; Morrison, D.C. Regulation of cellular caveolin-1 protein expression in murine macrophages by microbial products. Infect. Immun. 2005, 73, 8136–8143. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.M.; Kim, H.P.; Nakahira, K.; Ryter, S.W.; Choi, A.M. The heme oxygenase-1/carbon monoxide pathway suppresses tlr4 signaling by regulating the interaction of TLR4 with caveolin-1. J. Immunol. 2009, 182, 3809–3818. [Google Scholar] [CrossRef] [PubMed]
- Lang, T.; Mansell, A. The negative regulation of Toll-like receptor and associated pathways. Immunol. Cell Biol. 2007, 85, 425–434. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, L.A. Tampering with Toll-like receptor signaling. Cell 2007, 131, 1039–1041. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, L.A. ‘Fine tuning’ TLR signaling. Nat. Immunol. 2008, 9, 459–461. [Google Scholar] [CrossRef] [PubMed]
- Trinchieri, G.; Sher, A. Cooperation of Toll-like receptor signals in innate immune defence. Nat. Rev. Immunol. 2007, 7, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Effros, R.B.; Allsopp, R.; Chiu, C.P.; Hausner, M.A.; Hirji, K.; Wang, L.; Harley, C.B.; Villeponteau, B.; West, M.D.; Giorgi, J.V. Shortened telomeres in the expanded CD28-CD8+ cell subset in HIV disease implicate replicative senescence in HIV pathogenesis. AIDS 1996, 10, F17–22. [Google Scholar] [CrossRef] [PubMed]
- Brenchley, J.M.; Karandikar, N.J.; Betts, M.R.; Ambrozak, D.R.; Hill, B.J.; Crotty, L.E.; Casazza, J.P.; Kuruppu, J.; Migueles, S.A.; Connors, M.; et al. Expression of CD57 defines replicative senescence and antigen-induced apoptotic death of CD8+ T cells. Blood 2003, 101, 2711–2720. [Google Scholar] [CrossRef] [PubMed]
- Grossman, Z.; Meier-Schellersheim, M.; Sousa, A.E.; Victorino, R.M.; Paul, W.E. CD4+ T-cell depletion in HIV infection: Are we closer to understanding the cause? Nat. Med. 2002, 8, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Dyck, L.; Mills, K.H.G. Immune checkpoints and their inhibition in cancer and infectious diseases. Eur. J. Immunol. 2017, 47, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Trautmann, L.; Janbazian, L.; Chomont, N.; Said, E.A.; Gimmig, S.; Bessette, B.; Boulassel, M.R.; Delwart, E.; Sepulveda, H.; Balderas, R.S.; et al. Upregulation of PD-1 expression on HIV-specific CD8+ T cells leads to reversible immune dysfunction. Nat. Med. 2006, 12, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, D.E.; Walker, B.D. Programmed death-1 as a factor in immune exhaustion and activation in HIV infection. Curr. Opin. HIV AIDS 2008, 3, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Garcia, M.; Porichis, F.; de Jong, O.G.; Levi, K.; Diefenbach, T.J.; Lifson, J.D.; Freeman, G.J.; Walker, B.D.; Kaufmann, D.E.; Kavanagh, D.G. Expression of PD-l1 and PD-l2 on human macrophages is up-regulated by HIV-1 and differentially modulated by IL-10. J. Leukoc. Biol. 2011, 89, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Petrovas, C.; Casazza, J.P.; Brenchley, J.M.; Price, D.A.; Gostick, E.; Adams, W.C.; Precopio, M.L.; Schacker, T.; Roederer, M.; Douek, D.C.; et al. PD-1 is a regulator of virus-specific CD8+ T cell survival in HIV infection. J. Exp. Med. 2006, 203, 2281–2292. [Google Scholar] [CrossRef] [PubMed]
- Day, C.L.; Kaufmann, D.E.; Kiepiela, P.; Brown, J.A.; Moodley, E.S.; Reddy, S.; Mackey, E.W.; Miller, J.D.; Leslie, A.J.; DePierres, C.; et al. PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression. Nature 2006, 443, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Wen, Q.; Zhao, Y.; Gao, Q.; Bai, Y. NF-κB plays a key role in inducing CD274 expression in human monocytes after lipopolysaccharide treatment. PLoS ONE 2013, 8, e61602. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, T.; Akiba, H.; Iwai, H.; Matsuda, H.; Aoki, M.; Tanno, Y.; Shin, T.; Tsuchiya, H.; Pardoll, D.M.; Okumura, K.; et al. Expression of programmed death 1 ligands by murine T cells and APC. J. Immunol. 2002, 169, 5538–5545. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; X-M, W.; Nadeau, P.E.; Mergia, A. HIV infection upregulates caveolin 1 (Cav-1) expression to restrict virus production. J. Virol. 2010, 84, 9487–9496. [Google Scholar] [CrossRef] [PubMed]
- Ito, J.; Nagayasu, Y.; Miura, Y.; Yokoyama, S.; Michikawa, M. Astrocytes endogenous apoE generates HDL-like lipoproteins using previously synthesized cholesterol through interaction with ABCA1. Brain Res. 2014, 1570, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Qiao, H.; He, X.; Zhang, Q.; Zhang, N.; Li, L.; Hui, Y.; Li, W.; Wang, D.; Wu, Z. Alpha-synuclein induces microglial cell migration through stimulating HIF-1α accumulation. J. Neurosci. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Tiruppathi, C.; Shimizu, J.; Miyawaki-Shimizu, K.; Vogel, S.M.; Bair, A.M.; Minshall, R.D.; Predescu, D.; Malik, A.B. Role of NF-κB-dependent caveolin-1 expression in the mechanism of increased endothelial permeability induced by lipopolysaccharide. J. Biol. Chem. 2008, 283, 4210–4218. [Google Scholar] [CrossRef] [PubMed]
- Gargalovic, P.; Dory, L. Cellular apoptosis is associated with increased caveolin-1 expression in macrophages. J. Lipid Res. 2003, 44, 1622–1632. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Wang, S.H.; Kuan, I.I.; Tseng, W.K.; Chen, M.F.; Wu, J.C.; Chen, Y.L. OXLDL upregulates caveolin-1 expression in macrophages: Role for caveolin-1 in the adhesion of OXLDL-treated macrophages to endothelium. J. Cell. Biochem. 2009, 107, 460–472. [Google Scholar] [CrossRef] [PubMed]
- Engelman, J.A.; Lee, R.J.; Karnezis, A.; Bearss, D.J.; Webster, M.; Siegel, P.; Muller, W.J.; Windle, J.J.; Pestell, R.G.; Lisanti, M.P. Reciprocal regulation of Neu tyrosine kinase activity and caveolin-1 protein expression in vitro and in vivo. Implications for human breast cancer. J. Biol. Chem. 1998, 273, 20448–20455. [Google Scholar] [CrossRef] [PubMed]
- Koleske, A.J.; Baltimore, D.; Lisanti, M.P. Reduction of caveolin and caveolae in oncogenically transformed cells. Proc. Natl. Acad. Sci. USA 1995, 92, 1381–1385. [Google Scholar] [CrossRef] [PubMed]
- Park, D.S.; Razani, B.; Lasorella, A.; Schreiber-Agus, N.; Pestell, R.G.; Iavarone, A.; Lisanti, M.P. Evidence that Myc isoforms transcriptionally repress caveolin-1 gene expression via an INR-dependent mechanism. Biochemistry 2001, 40, 3354–3362. [Google Scholar] [CrossRef] [PubMed]
- Timme, T.L.; Goltsov, A.; Tahir, S.; Li, L.; Wang, J.; Ren, C.; Johnston, R.N.; Thompson, T.C. Caveolin-1 is regulated by c-myc and suppresses c-myc-induced apoptosis. Oncogene 2000, 19, 3256–3265. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.T.; Nadeau, P.E.; Lin, S.; Mergia, A. Establishing restricted expression of caveolin-1 in HIV infected cells and inhibition of virus replication. Open Microbiol. J. 2014, 8, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.M.; Kim, H.P.; Song, R.; Choi, A.M. Caveolin-1 confers antiinflammatory effects in murine macrophages via the MKK3/p38 MAPK pathway. Am. J. Respir. Cell Mol. Biol. 2006, 34, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Bellyei, S.; Schally, A.V.; Zarandi, M.; Varga, J.L.; Vidaurre, I.; Pozsgai, E. GHRH antagonists reduce the invasive and metastatic potential of human cancer cell lines in vitro. Cancer Lett. 2010, 293, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Bist, A.; Fielding, C.J.; Fielding, P.E. P53 regulates caveolin gene transcription, cell cholesterol, and growth by a novel mechanism. Biochemistry 2000, 39, 1966–1972. [Google Scholar] [CrossRef] [PubMed]
- Bist, A.; Fielding, P.E.; Fielding, C.J. Two sterol regulatory element-like sequences mediate up-regulation of caveolin gene transcription in response to low density lipoprotein free cholesterol. Proc. Natl. Acad. Sci. USA 1997, 94, 10693–10698. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Fernandez-Zapico, M.E.; Jin, D.; Puri, V.; Cook, T.A.; Lerman, L.O.; Zhu, X.Y.; Urrutia, R.; Shah, V. KLF11-mediated repression antagonizes Sp1/sterol-responsive element-binding protein-induced transcriptional activation of caveolin-1 in response to cholesterol signaling. J. Biol. Chem. 2005, 280, 1901–1910. [Google Scholar] [CrossRef] [PubMed]
- Fielding, C.J.; Bist, A.; Fielding, P.E. Intracellular cholesterol transport in synchronized human skin fibroblasts. Biochemistry 1999, 38, 2506–2513. [Google Scholar] [CrossRef] [PubMed]
- Costales, P.; Castellano, J.; Revuelta-Lopez, E.; Cal, R.; Aledo, R.; Llampayas, O.; Nasarre, L.; Juarez, C.; Badimon, L.; Llorente-Cortes, V. Lipopolysaccharide downregulates CD91/low-density lipoprotein receptor-related protein 1 expression through SREBP-1 overexpression in human macrophages. Atherosclerosis 2013, 227, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Feig, J.E.; Shang, Y.; Rotllan, N.; Vengrenyuk, Y.; Wu, C.; Shamir, R.; Torra, I.P.; Fernandez-Hernando, C.; Fisher, E.A.; Garabedian, M.J. Statins promote the regression of atherosclerosis via activation of the CCR7-dependent emigration pathway in macrophages. PLoS ONE 2011, 6, e28534. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Bartholomew, J.N.; Volonte, D.; Galbiati, F. Oxidative stress induces premature senescence by stimulating caveolin-1 gene transcription through p38 mitogen-activated protein kinase/Sp1-mediated activation of two GC-rich promoter elements. Cancer Res. 2006, 66, 10805–10814. [Google Scholar] [CrossRef] [PubMed]
- Chretien, A.; Piront, N.; Delaive, E.; Demazy, C.; Ninane, N.; Toussaint, O. Increased abundance of cytoplasmic and nuclear caveolin 1 in human diploid fibroblasts in H2O2-induced premature senescence and interplay with p38αMAPK. FEBS Lett. 2008, 582, 1685–1692. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Lin, J.C.; Yang, S.C.; Lin, C.W.; Chen, J.J.; Shih, J.Y.; Hong, T.M.; Yang, P.C. Modulation of the expression of the invasion-suppressor CRMP-1 by cyclooxygenase-2 inhibition via reciprocal regulation of Sp1 and C/EBPα. Mol. Cancer Ther. 2008, 7, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wang, N.; Huang, J.; Xin, J.; Peng, F.; Ren, Y.; Zhang, S.; Miao, J. Inhibition of phosphatidylcholine-specific phospholipase C prevents bone marrow stromal cell senescence in vitro. J. Cell. Biochem. 2009, 108, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.M.; Sutliff, R.L. HIV-1, reactive oxygen species, and vascular complications. Free Radic. Biol. Med. 2012, 53, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Smart, E.J.; Weksler, B.; Couraud, P.O.; Hennig, B.; Toborek, M. Caveolin-1 regulates human immunodeficiency virus-1 TAT-induced alterations of tight junction protein expression via modulation of the Ras signaling. J. Neurosci. 2008, 28, 7788–7796. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Andras, I.E.; Rha, G.B.; Hennig, B.; Toborek, M. PPARα and PPARγ protect against HIV-1-induced MMP-9 overexpression via caveolae-associated ERK and Akt signaling. FASEB J. 2011, 25, 3979–3988. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Feng, X.; Xie, X.; Zhang, J.; Wu, D.; Xu, L. HIV-1 TAT protein increases the permeability of brain endothelial cells by both inhibiting occludin expression and cleaving occludin via matrix metalloproteinase-9. Brain Res. 2012, 1436, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.L.; Song, J.N.; Zhang, M. Role of caveolin-1 in the biology of the blood-brain barrier. Rev. Neurosci. 2014, 25, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.K.; Choi, E.J. Pathological roles of MAPK signaling pathways in human diseases. Biochim. Biophys. Acta 2010, 1802, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Klucken, J.; Buchler, C.; Orso, E.; Kaminski, W.E.; Porsch-Ozcurumez, M.; Liebisch, G.; Kapinsky, M.; Diederich, W.; Drobnik, W.; Dean, M.; et al. ABCG1 (ABC8), the human homolog of the Drosophila white gene, is a regulator of macrophage cholesterol and phospholipid transport. Proc. Natl. Acad. Sci. USA 2000, 97, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Bodzioch, M.; Orso, E.; Klucken, J.; Langmann, T.; Bottcher, A.; Diederich, W.; Drobnik, W.; Barlage, S.; Buchler, C.; Porsch-Ozcurumez, M.; et al. The gene encoding ATP-binding cassette transporter 1 is mutated in Tangier disease. Nat. Genet. 1999, 22, 347–351. [Google Scholar] [PubMed]
- De La Llera-Moya, M.; Connelly, M.A.; Drazul, D.; Klein, S.M.; Favari, E.; Yancey, P.G.; Williams, D.L.; Rothblat, G.H. Scavenger receptor class B type I affects cholesterol homeostasis by magnifying cholesterol flux between cells and HDL. J. Lipid Res. 2001, 42, 1969–1978. [Google Scholar] [PubMed]
- Arakawa, R.; Abe-Dohmae, S.; Asai, M.; Ito, J.I.; Yokoyama, S. Involvement of caveolin-1 in cholesterol enrichment of high density lipoprotein during its assembly by apolipoprotein and THP-1 cells. J. Lipid Res. 2000, 41, 1952–1962. [Google Scholar] [PubMed]
- Escher, G.; Krozowski, Z.; Croft, K.D.; Sviridov, D. Expression of sterol 27-hydroxylase (CYP27A1) enhances cholesterol efflux. J. Biol. Chem. 2003, 278, 11015–11019. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.X.; Cao, D.L.; Xiong, Y.; Peng, X.H.; Liao, D.F. A novel model of cholesterol efflux from lipid-loaded cells. Acta Pharmacol. Sin. 2010, 31, 1243–1257. [Google Scholar] [CrossRef] [PubMed]
- Frank, P.G.; Cheung, M.W.; Pavlides, S.; Llaverias, G.; Park, D.S.; Lisanti, M.P. Caveolin-1 and the regulation of cellular cholesterol homeostasis. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H677–H686. [Google Scholar] [CrossRef] [PubMed]
- Fielding, C.J.; Fielding, P.E. Caveolae and intracellular trafficking of cholesterol. Adv. Drug Deliv. Rev. 2001, 49, 251–264. [Google Scholar] [CrossRef]
- Razani, B.; Woodman, S.E.; Lisanti, M.P. Caveolae: From cell biology to animal physiology. Pharmacol. Rev. 2002, 54, 431–467. [Google Scholar] [CrossRef] [PubMed]
- Kabouridis, P.S.; Janzen, J.; Magee, A.L.; Ley, S.C. Cholesterol depletion disrupts lipid rafts and modulates the activity of multiple signaling pathways in T lymphocytes. Eur. J. Immunol. 2000, 30, 954–963. [Google Scholar] [CrossRef]
- Parpal, S.; Karlsson, M.; Thorn, H.; Stralfors, P. Cholesterol depletion disrupts caveolae and insulin receptor signaling for metabolic control via insulin receptor substrate-1, but not for mitogen-activated protein kinase control. J. Biol. Chem. 2001, 276, 9670–9678. [Google Scholar] [CrossRef] [PubMed]
- Mahammad, S.; Dinic, J.; Adler, J.; Parmryd, I. Limited cholesterol depletion causes aggregation of plasma membrane lipid rafts inducing T cell activation. Biochim. Biophys. Acta 2010, 1801, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.Z.; McIntosh, V.J.; Abou Samra, A.B.; Mohammad, R.M.; Lasley, R.D. Cholesterol depletion alters cardiomyocyte subcellular signaling and increases contractility. PLoS ONE 2016, 11, e0154151. [Google Scholar] [CrossRef] [PubMed]
- Le Lay, S.; Hajduch, E.; Lindsay, M.R.; Le Liepvre, X.; Thiele, C.; Ferre, P.; Parton, R.G.; Kurzchalia, T.; Simons, K.; Dugail, I. Cholesterol-induced caveolin targeting to lipid droplets in adipocytes: A role for caveolar endocytosis. Traffic 2006, 7, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Van Meer, G. Caveolin, cholesterol, and lipid droplets? J. Cell Biol. 2001, 152, F29–34. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, M.; Signore, S.C.; Zerr, I.; Althaus, H.H. Oligodendroglial process formation is differentially affected by modulating the intra- and extracellular cholesterol content. J. Mol. Neurosci. 2013, 49, 457–469. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Zhu, N.; Ao, B.X.; Liu, C.; Shi, Y.N.; Du, K.; Chen, J.X.; Zheng, X.L.; Liao, D.F. Caveolae and caveolin-1 integrate reverse cholesterol transport and inflammation in atherosclerosis. Int. J. Mol. Sci. 2016, 17, 429. [Google Scholar] [CrossRef] [PubMed]
- Murata, M.; Peranen, J.; Schreiner, R.; Wieland, F.; Kurzchalia, T.V.; Simons, K. VIP21/caveolin is a cholesterol-binding protein. Proc. Natl. Acad. Sci. USA 1995, 92, 10339–10343. [Google Scholar] [CrossRef] [PubMed]
- Smart, E.J.; Ying, Y.; Donzell, W.C.; Anderson, R.G.W. A role for caveolin in transport of cholesterol from endoplasmic reticulum to plasma membrane. J. Biol. Chem. 1996, 271, 29427–29435. [Google Scholar] [PubMed]
- Uittenbogaard, A.; Ying, Y.; Smart, E.J. Characterization of a cytosolic heat-shock protein-caveolin chaperone complex. Involvement in cholesterol trafficking. J. Biol. Chem. 1998, 273, 6525–6532. [Google Scholar] [CrossRef] [PubMed]
- Pol, A.; Luetterforst, R.; Lindsay, S.; Heino, S.; Ikonen, E.; Parton, R.G. A caveolin dominant negative mutant associates with lipid bodies and induces intracellular cholesterol imbalance. J. Cell Biol. 2001, 152, 1057–1070. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Hoang, A.; Escher, G.; Parton, R.G.; Krozowski, Z.; Sviridov, D. Expression of caveolin-1 enhances cholesterol efflux in hepatic cells. J. Biol. Chem. 2004, 279, 14140–14146. [Google Scholar] [CrossRef] [PubMed]
- Pol, A.; Martin, S.; Fernandez, M.A.; Ferguson, C.; Carozzi, A.; Luetterforst, R.; Enrich, C.; Parton, R.G. Dynamic and regulated association of caveolin with lipid bodies: Modulation of lipid body motility and function by a dominant negative mutant. Mol. Biol. Cell 2004, 15, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Meshulam, T.; Simard, J.R.; Wharton, J.; Hamilton, J.A.; Pilch, P.F. Role of caveolin-1 and cholesterol in transmembrane fatty acid movement. Biochemistry 2006, 45, 2882–2893. [Google Scholar] [CrossRef] [PubMed]
- Puglielli, L.; Rigotti, A.; Greco, A.V.; Santos, M.J.; Nervi, F. Sterol carrier protein-2 is involved in cholesterol transfer from the endoplasmic reticulum to the plasma membrane in human fibroblasts. J. Biol. Chem. 1995, 270, 18723–18726. [Google Scholar] [PubMed]
- Zhou, M.; Parr, R.D.; Petrescu, A.D.; Payne, H.R.; Atshaves, B.P.; Kier, A.B.; Ball, J.M.; Schroeder, F. Sterol carrier protein-2 directly interacts with caveolin-1 in vitro and in vivo. Biochemistry 2004, 43, 7288–7306. [Google Scholar] [CrossRef] [PubMed]
- Jessup, W.; Gelissen, I.C.; Gaus, K.; Kritharides, L. Roles of ATP binding cassette transporters A1 and B1, scavenger receptor BI and membrane lipid domains in cholesterol export from macrophages. Curr. Opin. Lipidol. 2006, 17, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Oram, J.F.; Lawn, R.M. ABCA1. The gatekeeper for eliminating excess tissue cholesterol. J. Lipid Res. 2001, 42, 1173–1179. [Google Scholar] [PubMed]
- Argmann, C.A.; Edwards, J.Y.; Sawyez, C.G.; O’Neil, C.H.; Hegele, R.A.; Pickering, J.G.; Huff, M.W. Regulation of macrophage cholesterol efflux through hydroxymethylglutaryl-CoA reductase inhibition: A role for RhoA in ABCA1-mediated cholesterol efflux. J. Biol. Chem. 2005, 280, 22212–22221. [Google Scholar] [CrossRef] [PubMed]
- Landry, Y.D.; Denis, M.; Nandi, S.; Bell, S.; Vaughan, A.M.; Zha, X. ATP-binding cassette transporter A1 expression disrupts raft membrane microdomains through its ATPase-related functions. J. Biol. Chem. 2006, 281, 36091–36101. [Google Scholar] [CrossRef] [PubMed]
- Aloia, R.C.; Tian, H.; Jensen, F.C. Lipid composition and fluidity of the human immunodeficiency virus envelope and host cell plasma membranes. Proc. Natl. Acad. Sci. USA 1993, 90, 5181–5185. [Google Scholar] [CrossRef] [PubMed]
- Maziere, J.C.; Landureau, J.C.; Giral, P.; Auclair, M.; Fall, L.; Lachgar, A.; Achour, A.; Zagury, D. Lovastatin inhibits HIV-1 expression in H9 human T lymphocytes cultured in cholesterol-poor medium. Biomed. Pharmacother. 1994, 48, 63–67. [Google Scholar] [CrossRef]
- Nguyen, D.H.; Hildreth, J.E. Evidence for budding of human immunodeficiency virus type 1 selectively from glycolipid-enriched membrane lipid rafts. J. Virol. 2000, 74, 3264–3272. [Google Scholar] [CrossRef] [PubMed]
- Espeseth, A.S.; Felock, P.; Wolfe, A.; Witmer, M.; Grobler, J.; Anthony, N.; Egbertson, M.; Melamed, J.Y.; Young, S.; Hamill, T.; et al. HIV-1 integrase inhibitors that compete with the target DNA substrate define a unique strand transfer conformation for integrase. Proc. Natl. Acad. Sci. USA 2000, 97, 11244–11249. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Derdowski, A.; Wang, J.J.; Spearman, P. Independent segregation of human immunodeficiency virus type 1 Gag protein complexes and lipid rafts. J. Virol. 2003, 77, 1916–1926. [Google Scholar] [CrossRef] [PubMed]
- Holm, K.; Weclewicz, K.; Hewson, R.; Suomalainen, M. Human immunodeficiency virus type 1 assembly and lipid rafts: Pr55gag associates with membrane domains that are largely resistant to Brij98 but sensitive to Triton X-100. J. Virol. 2003, 77, 4805–4817. [Google Scholar] [CrossRef] [PubMed]
- Bukrinsky, M.; Sviridov, D. Human immunodeficiency virus infection and macrophage cholesterol metabolism. J. Leukoc. Biol. 2006, 80, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.H.; Plemenitas, A.; Linnemann, T.; Fackler, O.T.; Peterlin, B.M. Nef increases infectivity of HIV via lipid rafts. Curr. Biol. 2001, 11, 875–879. [Google Scholar] [CrossRef]
- Lin, S.; Nadeau, P.E.; Wang, X.; Mergia, A. Caveolin-1 reduces HIV-1 infectivity by restoration of HIV Nef mediated impairment of cholesterol efflux by apoA-I. Retrovirology 2012, 9, 85. [Google Scholar] [CrossRef] [PubMed]
- Liao, Z.; Graham, D.R.; Hildreth, J.E. Lipid rafts and HIV pathogenesis: Virion-associated cholesterol is required for fusion and infection of susceptible cells. AIDS Res. Hum. Retrovir. 2003, 19, 675–687. [Google Scholar] [CrossRef] [PubMed]
- Carter, G.C.; Bernstone, L.; Sangani, D.; Bee, J.W.; Harder, T.; James, W. HIV entry in macrophages is dependent on intact lipid rafts. Virology 2009, 386, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.H.; Plemenitas, A.; Fielding, C.J.; Peterlin, B.M. Nef increases the synthesis of and transports cholesterol to lipid rafts and HIV-1 progeny virions. Proc. Natl. Acad. Sci. USA 2003, 100, 8460–8465. [Google Scholar] [CrossRef] [PubMed]
- Van‘t Wout, A.B.; Swain, J.V.; Schindler, M.; Rao, U.; Pathmajeyan, M.S.; Mullins, J.I.; Kirchhoff, F. Nef induces multiple genes involved in cholesterol synthesis and uptake in human immunodeficiency virus type 1-infected T cells. J. Virol. 2005, 79, 10053–10058. [Google Scholar] [CrossRef] [PubMed]
- Mujawar, Z.; Rose, H.; Morrow, M.P.; Pushkarsky, T.; Dubrovsky, L.; Mukhamedova, N.; Fu, Y.; Dart, A.; Orenstein, J.M.; Bobryshev, Y.V.; et al. Human immunodeficiency virus impairs reverse cholesterol transport from macrophages. PLoS Biol. 2006, 4, 1970–1983. [Google Scholar] [CrossRef] [PubMed]
- Mujawar, Z.; Tamehiro, N.; Grant, A.; Sviridov, D.; Bukrinsky, M.; Fitzgerald, M.L. Mutation of the ATP cassette binding transporter A1 (ABCA1) c-terminus disrupts HIV-1 Nef binding but does not block the Nef enhancement of ABCA1 protein degradation. Biochemistry 2010, 49, 8338–8349. [Google Scholar] [CrossRef] [PubMed]
- Jennelle, L.; Hunegnaw, R.; Dubrovsky, L.; Pushkarsky, T.; Fitzgerald, M.L.; Sviridov, D.; Popratiloff, A.; Brichacek, B.; Bukrinsky, M. HIV-1 protein Nef inhibits activity of ATP-binding cassette transporter A1 by targeting endoplasmic reticulum chaperone calnexin. J. Biol. Chem. 2014, 289, 28870–28884. [Google Scholar] [CrossRef] [PubMed]
- Kalyana Sundaram, R.V.; Li, H.; Bailey, L.; Rashad, A.A.; Aneja, R.; Weiss, K.; Huynh, J.; Bastian, A.R.; Papazoglou, E.; Abrams, C.; et al. Impact of HIV-1 membrane cholesterol on cell-independent lytic inactivation and cellular infectivity. Biochemistry 2016, 55, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.H.; Lu, L.; Hong, L.; Chen, X.; Jiang, S.; Chen, Y.-H. Identification of the HIV-1 gp41 core-binding motif in the scaffolding domain of caveolin-1. J. Biol. Chem. 2007, 282, 6143–6152. [Google Scholar] [CrossRef] [PubMed]
- Hovanessian, A.G.; Briand, J.P.; Said, E.A.; Svab, J.; Ferris, S.; Dali, H.; Muller, S.; Desgranges, C.; Krust, B. The caveolin-1 binding domain of HIV-1 glycoprotein gp41 is an efficient B cell epitope vaccine candidate against virus infection. Immunity 2004, 21, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.M.; Nadeau, P.E.; Lo, Y.-T.; Mergia, A. Caveolin-1 modulates HIV-1 envelope induced bystander apoptosis through gp41. J. Virol. 2010, 84, 6515–6526. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.K.; Yuan, J.; Gao, X.P.; Garrean, S.; Brovkovych, V.; Malik, A.B.; Tiruppathi, C.; Zhao, Y.Y. Caveolin-1 deficiency dampens Toll-like receptor 4 signaling through eNOS activation. Am. J. Pathol. 2010, 176, 2344–2351. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.H.; Chen, S.F.; Huang, T.Y.; Tzeng, C.F.; Chiang, A.S.; Kou, Y.R.; Lee, T.S.; Shyue, S.K. Impaired CD14 and CD36 expression, bacterial clearance, and Toll-like receptor 4-Myd88 signaling in caveolin-1-deleted macrophages and mice. Shock 2011, 35, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Yi, F.; Dai, Z.; Huang, X.; Zhao, Y.D.; Mirza, M.K.; Xu, J.; Vogel, S.M.; Zhao, Y.Y. Loss of caveolin-1 and adiponectin induces severe inflammatory lung injury following LPS challenge through excessive oxidative/nitrative stress. Am. J. Physiol. Lung Cell. Mol. Physiol. 2014, 306, L566–L573. [Google Scholar] [CrossRef] [PubMed]
- Medina, F.A.; de Almeida, C.J.; Dew, E.; Li, J.; Bonuccelli, G.; Williams, T.M.; Cohen, A.W.; Pestell, R.G.; Frank, P.G.; Tanowitz, H.B.; et al. Caveolin-1-deficient mice show defects in innate immunity and inflammatory immune response during Salmonella enterica serovar typhimurium infection. Infect. Immun. 2006, 74, 6665–6674. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.; Guo, L.; Song, Z.; Gao, H.; Wang, D.; Fu, W.; Han, J.; Li, Z.; Huang, B.; Li, X.A. Caveolin-1 protects against sepsis by modulating inflammatory response, alleviating bacterial burden, and suppressing thymocyte apoptosis. J. Biol. Chem. 2010, 285, 25154–25160. [Google Scholar] [CrossRef] [PubMed]
- Sathish, V.; Thompson, M.A.; Sinha, S.; Sieck, G.C.; Prakash, Y.S.; Pabelick, C.M. Inflammation, caveolae and CD38-mediated calcium regulation in human airway smooth muscle. Biochim. Biophys. Acta 2014, 1843, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Jiao, H.; Zhang, Y.; Yan, Z.; Wang, Z.G.; Liu, G.; Minshall, R.D.; Malik, A.B.; Hu, G. Caveolin-1 Tyr14 phosphorylation induces interaction with TLR4 in endothelial cells and mediates MyD88-dependent signaling and sepsis-induced lung inflammation. J. Immunol. 2013, 191, 6191–6199. [Google Scholar] [CrossRef] [PubMed]
- Hazenberg, M.D.; Otto, S.A.; van Benthem, B.H.; Roos, M.T.; Coutinho, R.A.; Lange, J.M.; Hamann, D.; Prins, M.; Miedema, F. Persistent immune activation in HIV-1 infection is associated with progression to aids. AIDS 2003, 17, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- Appay, V.; Sauce, D. Immune activation and inflammation in HIV-1 infection: Causes and consequences. J. Pathol. 2008, 214, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, J.; Jacobs, D.R., Jr.; Baker, J.V.; Calmy, A.; Duprez, D.; La Rosa, A.; Kuller, L.H.; Pett, S.L.; Ristola, M.; Ross, M.J.; et al. Markers of inflammation, coagulation, and renal function are elevated in adults with HIV infection. J. Infect. Dis. 2010, 201, 1788–1795. [Google Scholar] [CrossRef] [PubMed]
- Ipp, H.; Zemlin, A. The paradox of the immune response in HIV infection: When inflammation becomes harmful. Clin. Chim. Acta 2013, 416, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Voelkel, N.F.; Cool, C.D.; Flores, S. From viral infection to pulmonary arterial hypertension: A role for viral proteins? AIDS 2008, 22 (Suppl. 3), S49–S53. [Google Scholar] [CrossRef] [PubMed]
- Petitpretz, P.; Brenot, F.; Azarian, R.; Parent, F.; Rain, B.; Herve, P.; Simonneau, G. Pulmonary hypertension in patients with human immunodeficiency virus infection. Comparison with primary pulmonary hypertension. Circulation 1994, 89, 2722–2727. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.J.; Khan, I.A.; Mehta, R.N.; Sepkowitz, D.A. HIV-related pulmonary hypertension: Analytic review of 131 cases. Chest 2000, 118, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Limsukon, A.; Saeed, A.I.; Ramasamy, V.; Nalamati, J.; Dhuper, S. HIV-related pulmonary hypertension. Mt. Sinai J. Med. 2006, 73, 1037–1044. [Google Scholar] [PubMed]
- Marecki, J.; Cool, C.; Voelkel, N.; Luciw, P.; Flores, S. Evidence for vascular remodeling in the lungs of macaques infected with simian immunodeficiency virus/HIV Nef recombinant virus. Chest 2005, 128, 621S–622S. [Google Scholar] [CrossRef] [PubMed]
- Duffy, P.; Wang, X.; Lin, P.H.; Yao, Q.; Chen, C. HIV Nef protein causes endothelial dysfunction in porcine pulmonary arteries and human pulmonary artery endothelial cells. J. Surg. Res. 2009, 156, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, R.M.; Draznin, M.B.; Murad, F. Endothelium-dependent vasodilator-and nitrovasodilator-induced relaxation may be mediated through cyclic GMP formation and cyclic GMP-dependent protein phosphorylation. Trans. Assoc. Am. Physicians 1983, 96, 19–30. [Google Scholar] [PubMed]
- Palmer, R.M.; Ferrige, A.G.; Moncada, S. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature 1987, 327, 524–526. [Google Scholar] [CrossRef] [PubMed]
- Moncada, S.; Palmer, R.M.; Higgs, E.A. Nitric oxide: Physiology, pathophysiology, and pharmacology. Pharmacol. Rev. 1991, 43, 109–142. [Google Scholar] [PubMed]
- Cooke, J.P. The pivotal role of nitric oxide for vascular health. Can. J. Cardiol. 2004, 20 (Suppl. B), 7B–15B. [Google Scholar] [PubMed]
- Garcia-Cardena, G.; Martasek, P.; Masters, B.S.; Skidd, P.M.; Couet, J.; Li, S.; Lisanti, M.P.; Sessa, W.C. Dissecting the interaction between nitric oxide synthase (NOS) and caveolin. Functional significance of the NOS caveolin binding domain in vivo. J. Biol. Chem. 1997, 272, 25437–25440. [Google Scholar] [CrossRef] [PubMed]
- Sowa, G.; Pypaert, M.; Sessa, W.C. Distinction between signaling mechanisms in lipid rafts vs. Caveolae. Proc. Natl. Acad. Sci. USA 2001, 98, 14072–14077. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.; Gratton, J.P.; Rudic, R.D.; Acevedo, L.; Roviezzo, F.; Cirino, G.; Sessa, W.C. In vivo delivery of the caveolin-1 scaffolding domain inhibits nitric oxide synthesis and reduces inflammation. Nat. Med. 2000, 6, 1362–1367. [Google Scholar] [PubMed]
- Forstermann, U.; Sessa, W.C. Nitric oxide synthases: Regulation and function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.Y.; Liu, Y.; Stan, R.V.; Fan, L.; Gu, Y.; Dalton, N.; Chu, P.H.; Peterson, K.; Ross, J., Jr.; Chien, K.R. Defects in caveolin-1 cause dilated cardiomyopathy and pulmonary hypertension in knockout mice. Proc. Natl. Acad. Sci. USA 2002, 99, 11375–11380. [Google Scholar] [CrossRef] [PubMed]
- Austin, E.D.; Ma, L.; LeDuc, C.; Berman Rosenzweig, E.; Borczuk, A.; Phillips, J.A., III; Palomero, T.; Sumazin, P.; Kim, H.R.; Talati, M.H.; et al. Whole exome sequencing to identify a novel gene (caveolin-1) associated with human pulmonary arterial hypertension. Circ. Cardiovasc. Genet. 2012, 5, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Kircher, M.; Del Campo, M.; Amato, R.S.; Agarwal, A.K.; University of Washington Center for Mendelian Genomics. Whole exome sequencing identifies de novo heterozygous CAV1 mutations associated with a novel neonatal onset lipodystrophy syndrome. Am. J. Med. Genet. A 2015, 167A, 1796–1806. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Copeland, C.A.; Kawano, Y.; Rosenzweig, E.B.; Austin, E.D.; Shahmirzadi, L.; Tang, S.; Raghunathan, K.; Chung, W.K.; Kenworthy, A.K. Characterization of a caveolin-1 mutation associated with both pulmonary arterial hypertension and congenital generalized lipodystrophy. Traffic 2016, 17, 1297–1312. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Nadeau, P.E.; Mergia, A. HIV inhibits endothelial reverse cholesterol transport through impacting subcellular caveolin-1 trafficking. Retrovirology 2015, 12, 62. [Google Scholar] [CrossRef] [PubMed]
- Corrotte, M.; Almeida, P.E.; Tam, C.; Castro-Gomes, T.; Fernandes, M.C.; Millis, B.A.; Cortez, M.; Miller, H.; Song, W.; Maugel, T.K.; et al. Caveolae internalization repairs wounded cells and muscle fibers. eLife 2013, 2, e00926. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.; Samaras, K.; Chisholm, D.J.; Cooper, D.A. Pathogenesis of HIV-1-protease inhibitor-associated peripheral lipodystrophy, hyperlipidaemia, and insulin resistance. Lancet 1998, 1881–1883. [Google Scholar] [CrossRef]
- Barbaro, G. Cardiovascular manifestations of HIV infection. Circulation 2002, 106, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Raulin, J. Human immunodeficiency virus and host cell lipids. Interesting pathways in research for a new HIV therapy. Prog. Lipid Res. 2002, 41, 27–65. [Google Scholar] [CrossRef]
- Ben-Romano, R.; Rudich, A.; Tirosh, A.; Potashnik, R.; Sasaoka, T.; Riesenberg, K.; Schlaeffer, F.; Bashan, N. Nelfinavir-induced insulin resistance is associated with impaired plasma membrane recruitment of the PI 3-kinase effectors Akt/PKB and PKC-zeta. Diabetologia 2004, 47, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Klein, D.; Hurley, L.B.; Quesenberry, C.P., Jr.; Sidney, S. Do protease inhibitors increase the risk for coronary heart disease in patients with HIV-1 infection? J. Acquir. Immune Defic. Syndr. 2002, 30, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Charakida, M.; Donald, A.E.; Green, H.; Storry, C.; Clapson, M.; Caslake, M.; Dunn, D.T.; Halcox, J.P.; Gibb, D.M.; Klein, N.J.; et al. Early structural and functional changes of the vasculature in HIV-infected children: Impact of disease and antiretroviral therapy. Circulation 2005, 112, 103–109. [Google Scholar] [CrossRef] [PubMed]
- El-Sadr, W.M.; Mullin, C.M.; Carr, A.; Gibert, C.; Rappoport, C.; Visnegarwala, F.; Grunfeld, C.; Raghavan, S.S. Effects of HIV disease on lipid, glucose and insulin levels: Results from a large antiretroviral-naive cohort. HIV Med. 2005, 6, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Umpleby, A.M.; Das, S.; Stolinski, M.; Shojaee-Moradie, F.; Jackson, N.C.; Jefferson, W.; Crabtree, N.; Nightingale, P.; Shahmanesh, M. Low density lipoprotein apolipoprotein B metabolism in treatment-naive HIV patients and patients on antiretroviral therapy. Antivir. Ther. 2005, 10, 663–670. [Google Scholar] [PubMed]
- Barbaro, G. Visceral fat as target of highly active antiretroviral therapy associated metabolic syndrome. Curr. Pharm. Des. 2007, 13, 2208–2213. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Stephan, C.; Harmjanz, A.; Staszewski, S.; Buehler, A.; Bickel, M.; von Kegler, S.; Ruhkamp, D.; Steinmetz, H.; Sitzer, M. Both long-term HIV infection and highly active antiretroviral therapy are independent risk factors for early carotid atherosclerosis. Atherosclerosis 2007, 196, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.T.; Gagnon, A.; Angel, J.B.; Sorisky, A. Ritonavir increases the level of active ADD-1/SREBP-1 protein during adipogenesis. AIDS 2000, 14, 2467–2473. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.S.; Distler, O.; Cooper, D.A.; Jamil, H.; Deckelbaum, R.J.; Ginsberg, H.N.; Sturley, S.L. HIV protease inhibitors protect apolipoprotein B from degradation by the proteasome: A potential mechanism for protease inhibitor-induced hyperlipidemia. Nat. Med. 2001, 7, 1327–1331. [Google Scholar] [CrossRef] [PubMed]
- Dressman, J.; Kincer, J.; Matveev, S.V.; Guo, L.; Greenberg, R.N. HIV protease inhibitors promote atherosclerotic lesion formation independent of dyslipidemia by increasing CD36-dependent cholesteryl ester accumulation in macrophages. J. Clin. Investig. 2003, 111, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Mu, H.; Chai, H.; Liao, D.; Yao, Q.; Chen, C. Human immunodeficiency virus protease inhibitor ritonavir inhibits cholesterol efflux from human macrophage-derived foam cells. Am. J. Pathol. 2007, 171, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Mergia, A. Nelfinavir also reduces Cav-1 expression in macrophages. University of Florida: Gainesville Florida, 2015; unpublished results. [Google Scholar]
- Hsue, P.Y.; Lo, J.C.; Franklin, A.; Bolger, A.F.; Martin, J.N.; Deeks, S.G.; Waters, D.D. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation 2004, 109, 1603–1608. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Zona, S.; Orlando, G.; Carli, F.; Ligabue, G.; Fiocchi, F.; Menozzi, M.; Rossi, R.; Modena, M.G.; Raggi, P. Human immunodeficiency virus infection is associated with accelerated atherosclerosis. J. Antimicrob. Chemother. 2011, 66, 1857–1860. [Google Scholar] [CrossRef] [PubMed]
- Coll, B.; Parra, S.; Aloonso-Villaverde, C.; de Groot, E.; Aragones, G.; Montero, M.; Tous, M.; Camps, J.; Joven, J.; Masana, L. HIV infected patients with lipodystrophy have higher rates of carotid atherosclerosis: The role of monocyte chemoattractant protein-1. Cytokine 2006, 34, 51–55. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A model for bidirectional interplay between human immunodeficiency virus (HIV) infection and Caveolin 1 (Cav-1) in establishing persistent infection in macrophages by three mechanisms. HIV infection up-regulates the expression of Cav-1 and the enhanced level of Cav-1 subsequently represses virus replication by suppressing the activity of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), countering viral negative factor (Nef) and promoting apolipoprotein A-I (apoA-I) mediated cholesterol efflux, subsequently reducing available cholesterol within the cell, and blocking the fusion steps of virus infectivity. Env: envelope; Tat: transactivator.
Figure 1.
A model for bidirectional interplay between human immunodeficiency virus (HIV) infection and Caveolin 1 (Cav-1) in establishing persistent infection in macrophages by three mechanisms. HIV infection up-regulates the expression of Cav-1 and the enhanced level of Cav-1 subsequently represses virus replication by suppressing the activity of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), countering viral negative factor (Nef) and promoting apolipoprotein A-I (apoA-I) mediated cholesterol efflux, subsequently reducing available cholesterol within the cell, and blocking the fusion steps of virus infectivity. Env: envelope; Tat: transactivator.
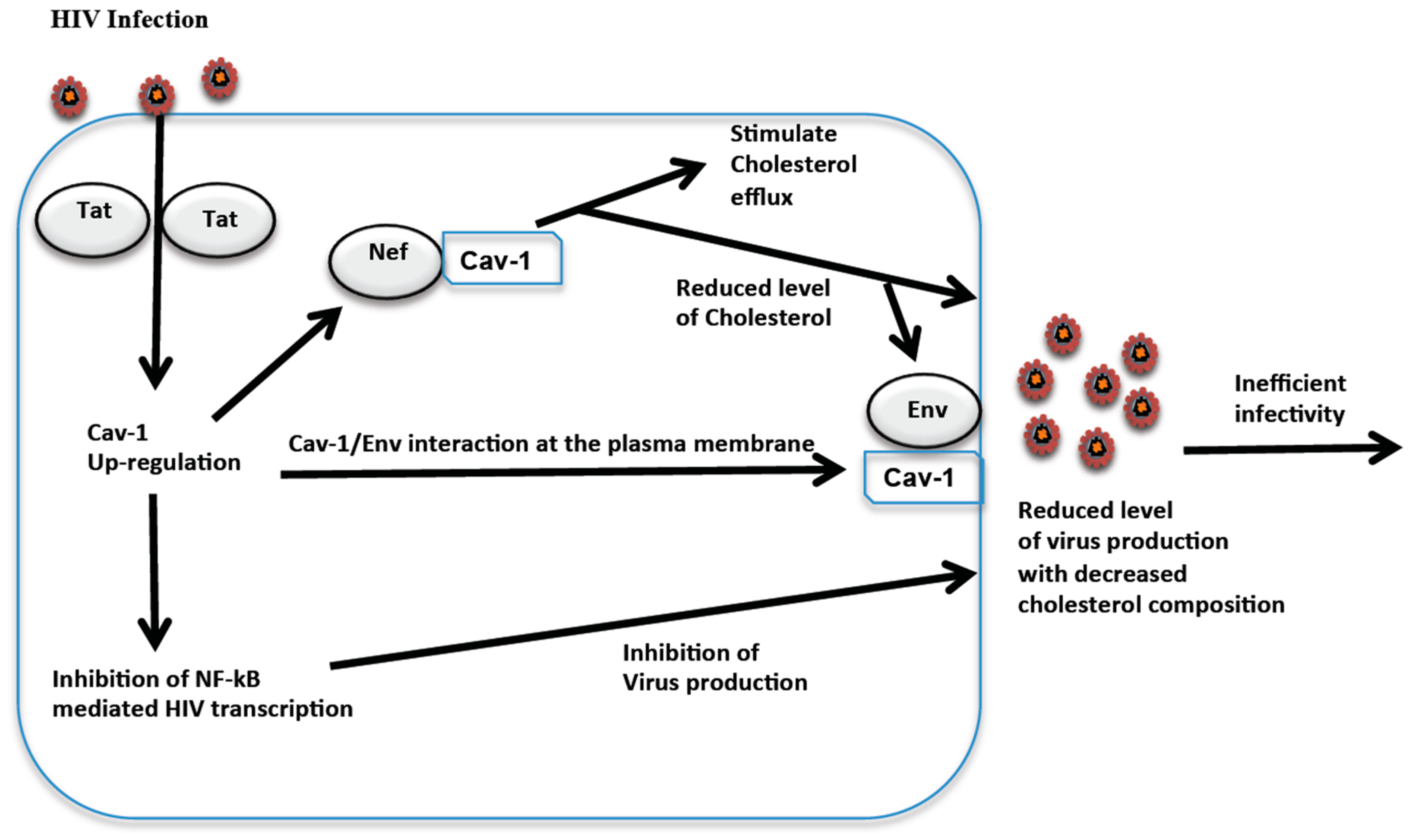
Figure 2.
HIV influence on aortic endothelial cell Cav-1 functions and potential link to pathogenesis. Viral proteins released from infected cells in combination with the induction of cellular factors such as cytokines and chemokines in the microenvironment can promote changes in Cav-1 cell distribution that impairs high-density lipoprotein (HDL) mediated cholesterol efflux and endothelial nitric oxide synthase (eNOS) regulation. There is also a reduction in eNOS, which could be related to Cav-1 redistribution. The mechanosensing function of Cav-1 may be an alternative or additional mechanism that leads to Cav-1 redistribution. These HIV induced endothelial cell dysfunctions through Cav-1 can be contributing factors to vascular diseases in HIV infected individuals.
Figure 2.
HIV influence on aortic endothelial cell Cav-1 functions and potential link to pathogenesis. Viral proteins released from infected cells in combination with the induction of cellular factors such as cytokines and chemokines in the microenvironment can promote changes in Cav-1 cell distribution that impairs high-density lipoprotein (HDL) mediated cholesterol efflux and endothelial nitric oxide synthase (eNOS) regulation. There is also a reduction in eNOS, which could be related to Cav-1 redistribution. The mechanosensing function of Cav-1 may be an alternative or additional mechanism that leads to Cav-1 redistribution. These HIV induced endothelial cell dysfunctions through Cav-1 can be contributing factors to vascular diseases in HIV infected individuals.
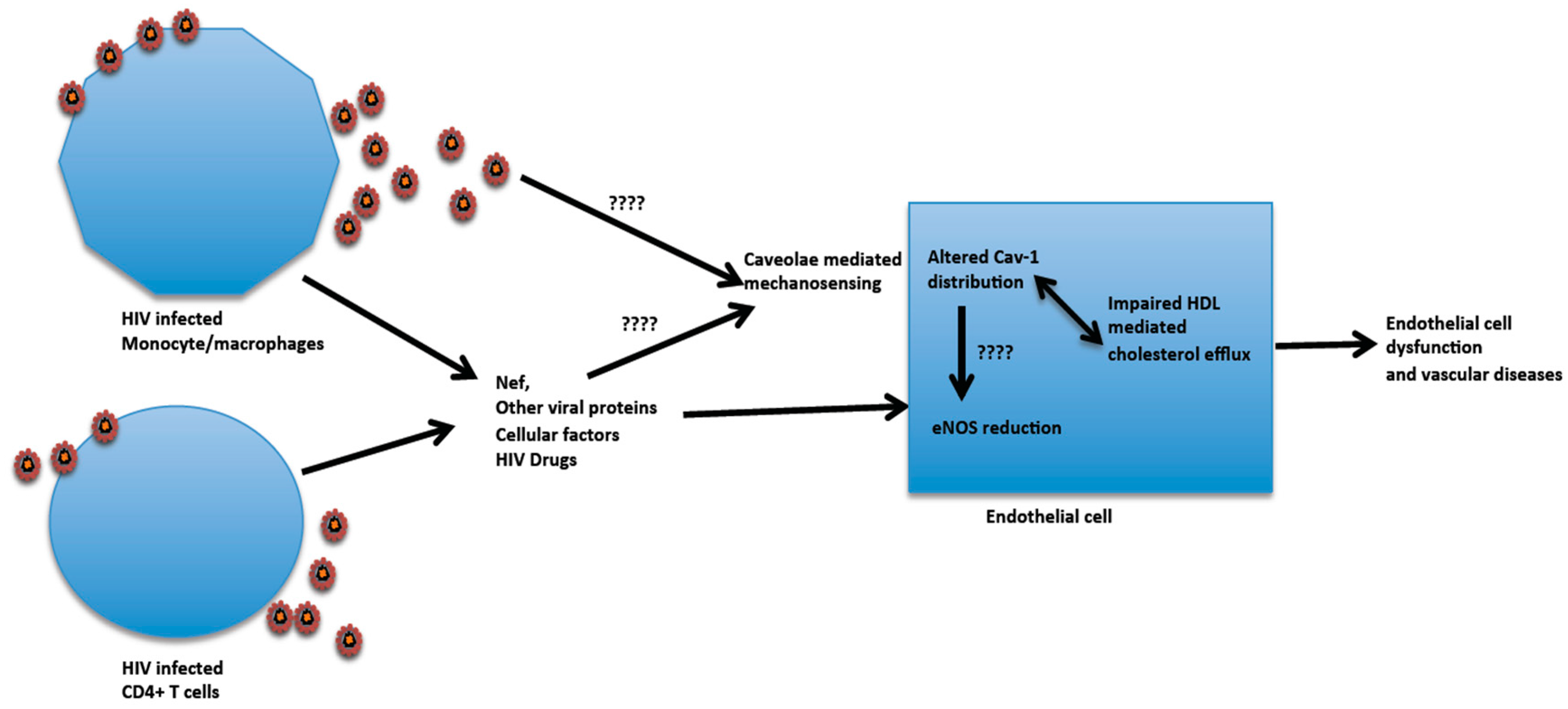

{kind=link}
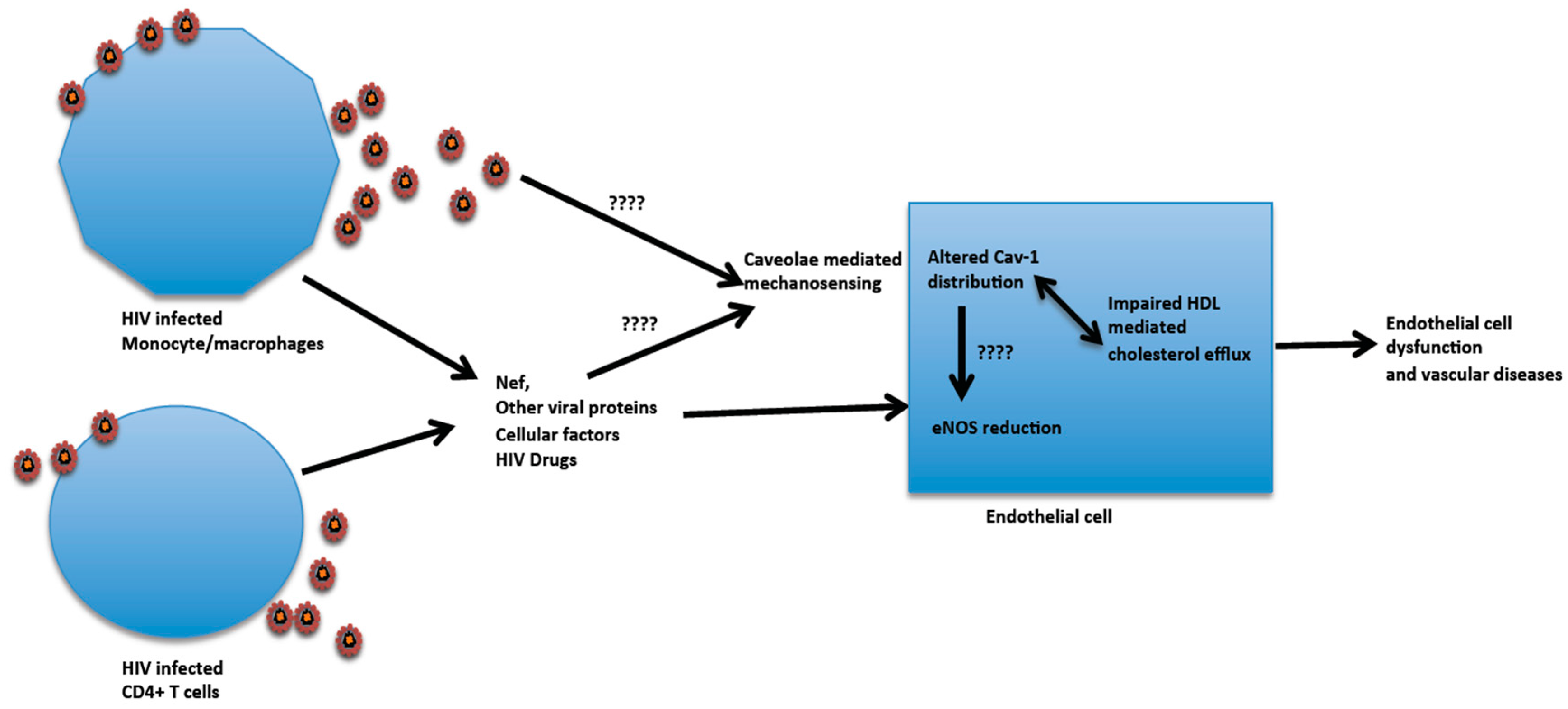{kind=link}
Table 1.
Caveolin 1/Caveolae functions *.
| Functions | Activities |
|---|---|
| Mechanosensing | Protection of cells from mechanical stress damage and other distress signals. |
| Lipid Homeostasis | Regulation of membrane lipid composition, cholesterol transport, and efflux. |
| Endocytosis | Proposed endocytosed cargos include glycosylphosphatidyl inositol (GPI)-anchored proteins, the insulin receptor, shiga and cholera toxins, cholesterol, albumin, and simian virus 40 (SV40). The specificity of caveolae and mechanisms for these cargos are still in question. |
| Transcytosis | Caveolae transport proteins and lipids such as low density lipoproteins (LDLs) albumin, and insulin from the blood across the interior of the endothelial cells to the opposite face and vice versa. |
| Signal transduction | Signaling platforms to diverse signaling molecules such as the insulin receptor, endothelial nitric oxide synthase( eNOS,) the epidermal growth factor receptor, and mitogen-activated protein kinase. |
| Inflammation | Cav-1 modulation of eNOS regulates inflammatory signaling through local control of NO production. |
| Ca2+ regulation and signaling can also be involved in inflammatory responses. | |
| Cav-1 serves as a protective protein against cellular stress and inflammation. | |
| Cancer | Serves as a tumor suppresser and at times as an oncogenic factor. Loss of Cav-1 in the stroma is linked to the clinical outcome of breast cancer. |
| Apoptosis | Involved in supporting multiple anti-apoptotic and survival pathways. |
| Angiogenesis | Involved in cancer angiogenesis. The Caveolin 1 pathway is also involved in the regulation of vascular endothelial growth factor (VEGF) in association with induced angiogenesis in brain ischemic. |
| Cellular senescence | Caveolin 1 plays a major role in controlling cellular senescence through its up-regulation by oxidative stress. |
| Cell cycle regulation | Caveolin 1 is important in the regulation of cyclin D1. |
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mergia, A. The Role of Caveolin 1 in HIV Infection and Pathogenesis. Viruses 2017, 9, 129. https://doi.org/10.3390/v9060129
AMA Style
Mergia A. The Role of Caveolin 1 in HIV Infection and Pathogenesis. Viruses. 2017; 9(6):129. https://doi.org/10.3390/v9060129
Chicago/Turabian StyleMergia, Ayalew. 2017. "The Role of Caveolin 1 in HIV Infection and Pathogenesis" Viruses 9, no. 6: 129. https://doi.org/10.3390/v9060129
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.