
Transmission of Hepatitis E Virus in Developing Countries


1
Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Kashmir 190001, India
2
Digestive Diseases Centre, Dr. Khuroo’s Medical Clinic, Srinagar, Kashmir 190010, India
3
Department of Pathology, Government Medical College, Srinagar, Kashmir 190001, India
*
Author to whom correspondence should be addressed.
Viruses 2016, 8(9), 253; https://doi.org/10.3390/v8090253
Submission received: 21 July 2016
/
Revised: 8 September 2016
/
Accepted: 8 September 2016
/
Published: 20 September 2016
(This article belongs to the Special Issue Recent Progress in Hepatitis E Virus Research)
Abstract
:Hepatitis E virus (HEV), an RNA virus of the Hepeviridae family, has marked heterogeneity. While all five HEV genotypes can cause human infections, genotypes HEV-1 and -2 infect humans alone, genotypes HEV-3 and -4 primarily infect pigs, boars and deer, and genotype HEV-7 primarily infects dromedaries. The global distribution of HEV has distinct epidemiological patterns based on ecology and socioeconomic factors. In resource-poor countries, disease presents as large-scale waterborne epidemics, and few epidemics have spread through person-to-person contact; however, endemic diseases within these countries can potentially spread through person-to-person contact or fecally contaminated water and foods. Vertical transmission of HEV from infected mother to fetus causes high fetal and perinatal mortality. Other means of transmission, such as zoonotic transmission, can fluctuate depending upon the region and strain of the virus. For instance, zoonotic transmission can sometimes play an insignificant role in human infections, such as in India, where human and pig HEV infections are unrelated. However, recently China and Southeast Asia have experienced a zoonotic spread of HEV-4 from pigs to humans and this has become the dominant mode of transmission of hepatitis E in eastern China. Zoonotic HEV infections in humans occur by eating undercooked pig flesh, raw liver, and sausages; through vocational contact; or via pig slurry, which leads to environmental contamination of agricultural products and seafood. Lastly, blood transfusion-associated HEV infections occur in many countries and screening of donors for HEV RNA is currently under serious consideration. To summarize, HEV genotypes 1 and 2 cause epidemic and endemic diseases in resource poor countries, primarily spreading through contaminated drinking water. HEV genotypes 3 and 4 on the other hand, cause autochthonous infections in developed, and many developing countries, by means of a unique zoonotic food-borne transmission.
1. Introduction
Hepatitis E is an enterically transmitted, self-limiting, acute, viral hepatitis [1]. The disease is ecologically dependent and is a major public health concern, especially in resource-poor countries [2]. The disease causes large-scale, water-borne epidemics of viral hepatitis and is the most common cause of acute sporadic hepatitis and fulminant hepatic failure in such countries [3]. The disease has unique and as yet unexplained epidemiological characteristics, including repeated waves of large-scale epidemics, occurrence of disease in adult population and high incidence and severity of disease in pregnant women [4]. The infection is prevalent in a wide range of animal species and human zoonotic hepatitis E is encountered in many developing countries and in all industrialized countries [5,6]. This paper shall focus its review on the mode of transmission of hepatitis E virus in developing countries [7].
Hepatitis E was discovered when a massive waterborne outbreak of jaundice was discovered, which had hit Gulmarg region, Kashmir, India in November 1978, and was classified as an “epidemic non-A, non-B hepatitis” [8]. The region had very hard weather conditions, inadequate primary healthcare, and poor access to tertiary care. Investigating this epidemic has been a remarkable human interest story [9], which unraveled unprecedented clinical and epidemiological data and led to postulating the existence of another human hepatitis virus [4,10,11,12,13,14]. Simultaneously, a disease with similar clinical features causing around one-half of endemic hepatitis was identified [15,16,17,18,19]. The virus-like particles (VLP) were identified using immune electron microscopy (IEM) from stool samples collected on days 28, 43, 44, and 45 from a volunteer who self-ingested extracts of nine fecal samples from patients with an epidemic of non-A, non-B hepatitis, affecting Soviet military personal in Afghanistan [20]. Over the next seven years, animal transmission studies and extensive physicochemical properties of the putative agent were performed [21]. Finally, cloning and partial sequencing of the virus recovered from the bile of the macaque was reported [22]. Soon afterwards, full length sequencing of the virus (7.2 kb) [23] and serological tests for diagnosis were readily available [24].
2. Overview of Hepatitis E Virus (HEV)
Hepatitis E virus (HEV) is one of the five major hepatotropic viruses, which primarily affect the liver [25]. HEV infection in humans causes acute hepatitic illness, designated as hepatitis E [4]. HEV is an RNA virus, spherically shaped, non-enveloped, and icosahedral in symmetry, with surface spikes and indentations [26]. The diameter of the virion is 27 to 32 nm on IEM, 32 to 34 nm after sucrose gradient centrifugation, and 38.5 to 42 nm on cryo-electron microscopy (cryo-EM) analysis. HEV has marked heterogeneity and hepatitis E-like viruses have been isolated and sequenced from a number of animals, including domestic pig, wild boar, Sicca deer, moose, rabbit, dromedary, chicken, bats, ferret, mink, rats, mongoose, and cutthroat trout [5,6,27]. All hepatitis-like viruses have been classified as members of Hepeviridae family [28] and divided into two genera, namely Orthohepevirus and Piscihepevirus. Orthohepevirus has four species: A (all mammalian isolates, such as human, pig, wild boar, deer, mongoose, rabbit, and camel); B (all 3 avian isolates, such as avian HEV-1, avian HEV-2, and avian HEV-3); C (isolates from rats, greater bandicoot, Asian musk shrew, and ferrets) and D (isolates from bats). Piscihepevirus includes a single isolate from cutthroat trout. Mammalian HEVs include several genotypes that can infect specific animals differently—for instance, genotypes HEV-1 and HEV-2 only infect humans, while genotypes HEV-3 and HEV-4 infect domestic pigs, wild boar, deer, mongoose, and humans (rabbit HEV is a distant member of genotype HEV-3 [29,30]). Lastly, genotype HEV-7, designated as DcHEV, primarily infects dromedaries. However, it has recently been found to have zoonotic potential when an infected liver transplant patient from the Middle East was discovered to have obtained HEV after consuming camel flesh and drinking camel milk [31,32]. Several animals, including the rhesus macaque, the cynomolgus monkey, horses, goat, sheep, cattle, and dogs show serological evidence of HEV infection; however, HEV strains from such animals need further characterization [33].
3. Hepatitis E in Developing Countries
Hepatitis E in developing countries has several disease patterns, determined by the geographical distribution of HEV genotypes, socioeconomic conditions, level of sanitation, access to potable water, and regional occurrence of zoonotic HEV infections in the animals [34,35,36].
3.1. HEV-1 and HEV-2
HEV-1 and HEV-2 exclusively infect humans and lack any zoonotic origin [27]. Global disease load of HEV was calculated from nine of the 21 Global Burden of Disease (GBD) regions, amounting to around two-thirds of the world population. HEV-1 and HEV-2 resulted in around 20 million incident infections, with 3.4 million clinical cases causing 70,000 deaths and 3000 stillbirths [37]; however, several factors should be considered when evaluating these numbers Hepatitis E epidemics often occur on repeated occasions over several decades, within the same geographical region [3], with a disease frequency in these regions of approximately 6% [1]. Additionally, IgG anti-HEV antibodies show a dynamic response, with a sizeable proportion of the population showing a loss of antibodies over a period of 14 years [38]. Recently, HEV reinfections with altered immune response have been reported in a small number of patients [13,39,40]. Thus, these calculated numbers may grossly underestimate the disease load in such countries.
Diseases caused by HEV-1 and HEV-2 are self-limiting and chronic hepatitis and cirrhosis have not been reported [11,12]. Hepatitis E presents as a hyperendemic disease in low-resource countries with poor sanitation through fecal contamination of food and water supplies [2,3,41]. The epidemics occur at regular intervals within these communities, causing massive epidemics of jaundice and significant morbidity and mortality [4]. Regions with hyperendemic disease include most countries of southern Asia (India, Pakistan, Nepal, Bhutan, Sri Lanka, Nepal, and Bangladesh), southeast Asia (Indonesia, Cambodia, Thailand, Vietnam, Laos, and Burma), central Asia (Tajikistan, Kazakhstan, and Uzbekistan), north Africa (Sudan, Algeria, Tunisia, and Morocco), east Africa (Uganda, Kenya, and Burundi) and west Africa (Nigeria, Ivory Coast, Liberia, and Mali) [1]. Hyperendemic zones also include many countries in Latin America (Uruguay, Venezuela, Cuba, and Mexico) [42] and northwest China (Xinjiang Uyghur) [43]. Hepatitis E accounts for over half of acute hepatitis in these countries [15]. Disease is most often seen in young adults, and has high incidence and severity in pregnant women, oftentimes causing high maternal and perinatal mortality rates [8,10,16]. HEV superinfection in otherwise compensated cirrhotic patients commonly occurs and leads to hepatic decompensation and high mortality [44,45].
Hepatitis E presents as an endemic disease in developing countries with recent improvement in socioeconomic status and access to better sanitation and water supplies [46,47,48,49,50]. Hepatitis E in endemic zones causes around one-fourth of acute hepatitis and has all the clinical features of disease seen in hyperendemic zones except for epidemics of jaundice, yet it is only caused by the HEV-1 genotype. Hepatitis E is endemic in many countries of the Middle East (Turkey, Saudi Arabia, Yemen, Libya, Oman, Bahrain, Iran, Kuwait, and the United Arab Emeritus) and some regions of southeast Asia (Singapore).
HEV-1 is also the predominant cause of hepatitis in Egypt, which has a distinctive epidemiology of hepatitis E, resembling that of hepatitis A virus (HAV), with distinct subtypes not seen in the Asian population [51,52,53]. HEV exposure occurs in the community at a young age and most young adults have IgG antibodies to HEV. Notably, the increased incidence and severity of HEV infection in pregnant women is not seen in this community. In fact, HEV in pregnant women in Egypt is either asymptomatic or presents as mild disease.
3.2. HEV-3 and HEV-4
HEV-3 and HEV-4 infect humans and a number of other animal species, and are the main cause of zoonotic autochthonous sporadic infections [5,6,54]. Most autochthonous HEV diseases occur in older individuals. Such patients have a more severe liver disease, with higher hepatic or non-hepatic complications (15%) and acute liver failure (8%–11%), except for pregnant women, in which autochthonous HEV infections do not cause a severe disease. HEV superinfection in chronic alcoholics and alcoholic chronic liver disease has been reported, culminating in hepatic decompensation, progression of liver disease and an approximately 70% death rate. HEV-3 infections are known to cause chronic viremia, chronic hepatitis and cirrhosis in patients with solid organ transplants, HIV infections, and hematological neoplasms on chemotherapy, while HEV-4 is a self-limiting disease and does not cause chronic hepatitis and cirrhosis [55,56].
Autochthonous HEV-3 infection has global distribution. Apart from industrialized countries, it has been widely reported in several developing countries of Latin America (Argentina, Brazil, Bolivia, Cuba, Venezuela, Mexico, Uruguay, Chile, and Costa Rica), Russia, and northeast China. Autochthonous HEV-4 infections are the predominant infections encountered in China and several countries in Southeast Asia (Indonesia, Cambodia, Thailand, Vietnam, Laos, and Burma), with the exception of Japan.
4. Modes of Transmission
4.1. Waterborne Transmission
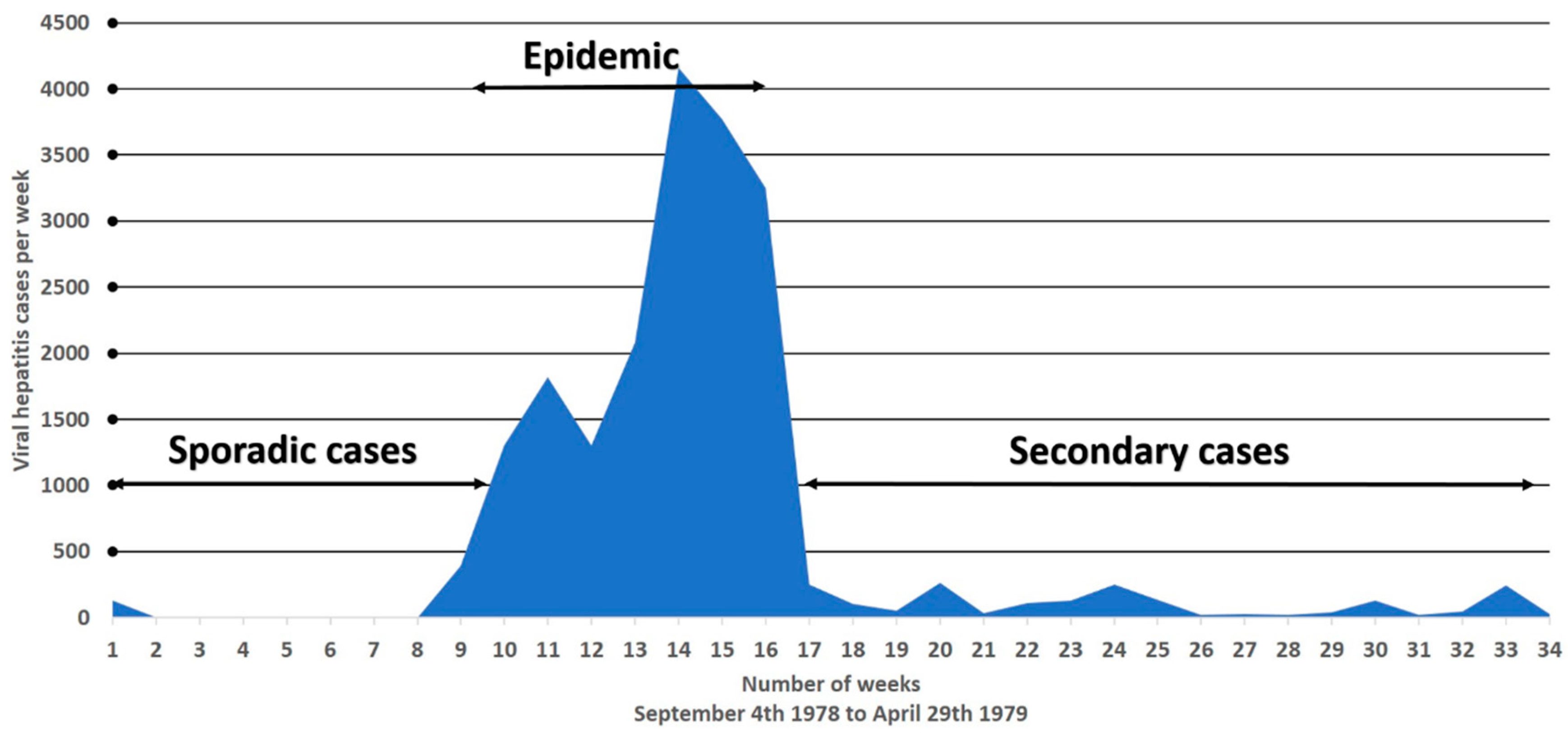
Hepatitis E is primarily transmitted through the fecal–oral route [3]. Gross fecal contamination of the community water supplies has been associated with several outbreaks in developing countries [8,57,58,59]. Epidemics are of common source origin as the epidemic curve is highly compressed, lasting for a duration of approximately six to eight weeks (Figure 1). Testing of water supplies at source and delivery points shows high E. coli counts, suggesting fecal contamination [8]. In several epidemics, there is a definite relationship between time of contamination and onset of disease, determined by the incubation period [57,58]. It has been shown that communities that use alternative water sources for drinking purposes (especially protected well water), prior to and during outbreaks, do not develop the disease [8]. Furthermore, raw sewage and water supplies have also been shown to contain HEV isolates closely related to human and animal infection [60,61,62,63].
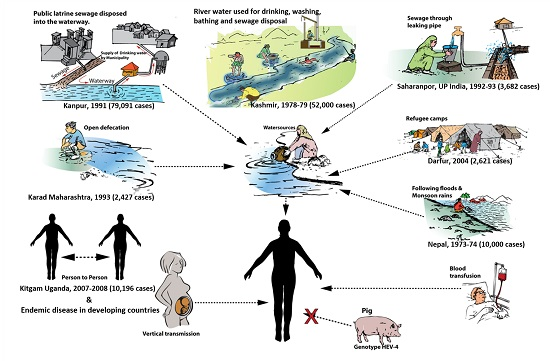
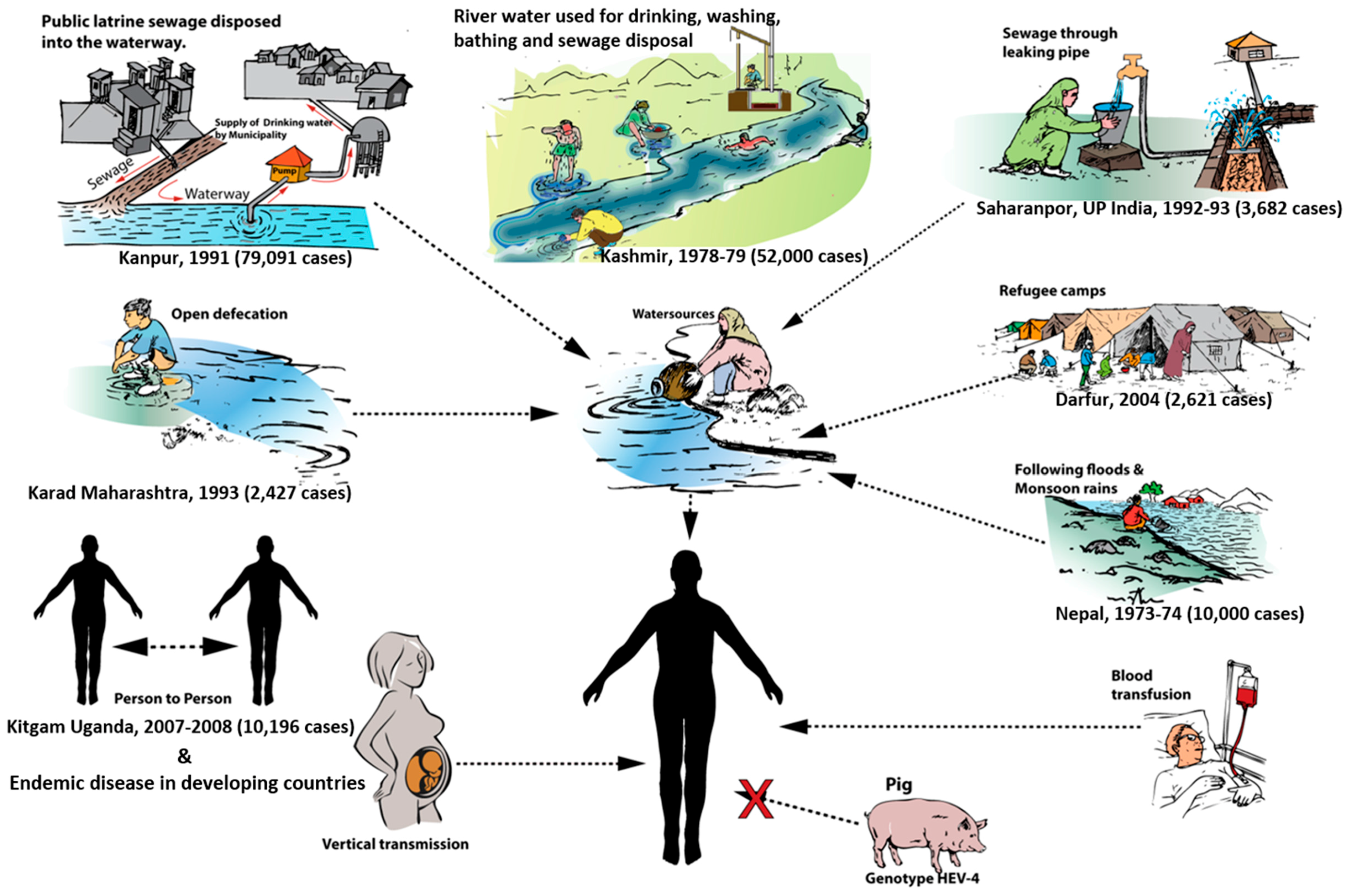
The mechanism of water contamination differs from one region to another; however, it typically follows a uniform pattern in repeated outbreaks within the same region, which is vital to understand, in order for public health officials to control any current and future epidemics [3]. Several different types of environmental settings have documented water contamination (Figure 2). Epidemics can result from contamination of river water used for drinking, washing, bathing, and sewage disposal (Figure 3) [4,39,64]. Outbreaks in such settings usually occur during winter months when the water level falls, thereby increasing the level of water contamination due to an increase in contaminant concentration [3]. Groundwater, crops, and waterways can all become contaminated. Open defecation in backyards and open fields can be another source of fecal contamination of groundwater, crops, and waterways [65]. In India for example, open defecation is rampant and over 300 million people use this practice for sanitary disposal, leading to widespread contamination of open drinking water sources, such as rivers, streams, and unprotected wells with raw sewage [2].
In fact, India accounts for 60% of individuals across the world, without access to toilets. It has been estimated that around 1.1 million liters of human feces are delivered to the Ganges River every minute. Flooding and monsoon rains wash fecally contaminated catchment areas like backyards, open fields, and ground water into open waterways, with a resultant eruption of waterborne diseases, including epidemics of hepatitis E [66].
Unfortunately, even piped water can become contaminated in certain situations. Quite often, piped drinking water is supplied to towns and cities in India, with the common practice of laying the pipes along with the sewage drains, or even crossing the sewage channels. Worn-out pipes become cracked and can start forming holes; during intermittent water supply schedules, the sewage enters the pipe lumen, causing fecal contamination of piped water. Several epidemics of hepatitis E in India have reportedly been caused by this phenomenon [67,68,69,70]. Even more dangerous is when the city sewage drains change their course due to heavy rains and flooding and enter the water source for the same city, thus supplying the city sewage water for drinking. Epidemics of massive proportion involving hundreds and thousands of cases have been reported due to sewage drain contamination of city water supplies alone [57,58].
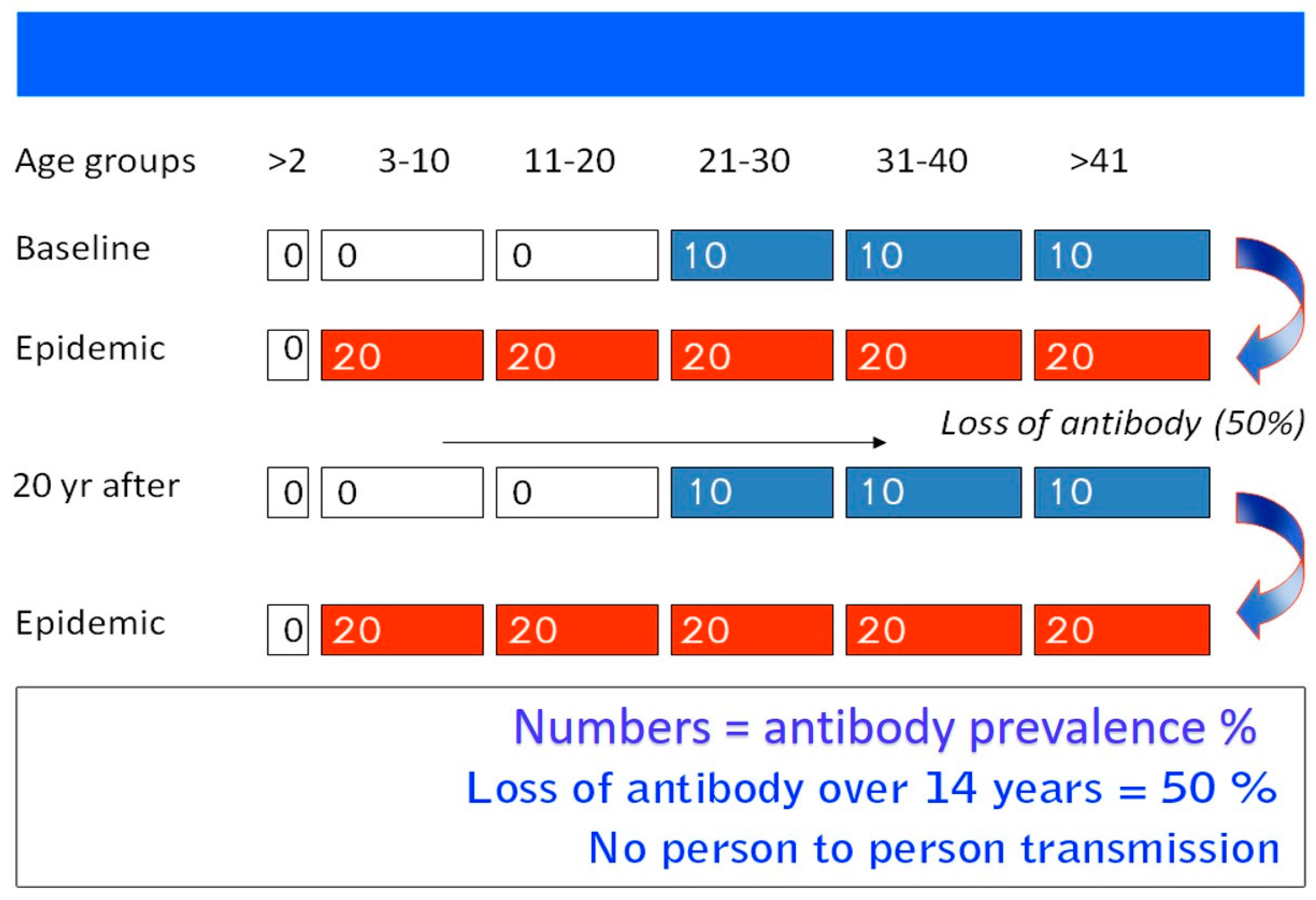
One of the puzzling epidemiological features of hepatitis E is the fact that epidemics occur only periodically within the same geographical region, in spite of constant fecal contamination of water supplies (Table 1). For example, Kashmir, India has been under surveillance since the first epidemic of viral hepatitis was recorded and studied in 1978–1979. The first reported epidemic spread over 200 villages with 600,000 inhabitants; it amounted to 20,083 individuals with jaundice and 600 fatalities in a seven-week period (Figure 1). Initially, six epidemics occurred in adjacent regions on a yearly basis (1978 to 1984), all in the late autumn and early winter months when the fecal pollution of the waterways becomes concentrated, affecting a population of 1,937,000 individuals, and causing 53,307 cases of jaundice and 1752 deaths. Following this outbreak, a decade went by with no epidemics occurring within the population. However, in November of 2007, a second wave of epidemics was then recorded by Khuroo, et al. [39], who looked at the sero-epidemiology of this outbreak, comparing it to the first epidemic from 1978–1979. In 1993, 45 hepatitis E subjects infected in 1978–1979 were studied to determine the status of long-term IgG. Around half of the subjects with HEV infection had lost the antibodies over 14 years’ follow-up [38]. After a natural infection, IgG anti-HEV titers rise for four weeks, followed by a decline. Around 28%–67% of subjects have undetectable antibodies over a two-year follow-up [64,71]. Therefore, it is thought that periodic epidemics within a population is due to a cohort effect. During an epidemic, around one-fourth of the population becomes infected and show the presence of serum IgG anti-HEV. Following this, there is a gradual loss of antibodies over time and little exposure to HEV infection in the inter-epidemic period in a new cohort of the population. Once the herd immunity falls to a critical level, the next epidemic hits the community (Figure 4).
4.2. Person-to-Person Transmission
4.2.1. Epidemic Disease
Transmission of HEV infection through person-to-person contact, causing epidemics, has long been a matter of controversy [72,73,74]. The epidemics are not followed by secondary waves of hepatitis cases [8,57] (Figure 1) and show poor intrafamilial spread [75]. These have been proposed as strong pieces of evidence that person-to-person transmission of HEV infections does not typically occur. Rather, as mentioned above, epidemics of hepatitis occur almost entirely due to gross fecal contamination of water, infecting all susceptible individuals, while secondary cases/intrafamilial spread are not expected to occur in this scenario due to a lack of susceptible individuals. Exceptionally, a large epidemic of hepatitis E that occurred in northern Uganda was related to person-to-person transmission [76,77]. This epidemic caused 10,196 icteric cases with 160 deaths; the epidemic curve was protracted, as new cases occurred from October 2007 through June 2008. There was a high attack rate in households, and 25% of cases occurring more than eight weeks after the onset of disease in the index case. Attending funerals, close contact with a jaundiced patient, and washing hands in a common family basin prior to having meals were all high risk factors for contracting the disease. These observations, along with an inability to define a common source of infection, suggest that the epidemic spread through person-to-person contact. Several outbreaks recorded a more protracted epidemic curve, and/or multiple epidemic peaks, which suggest alternative routes for the spread of infection. However, a detailed epidemiological assessment as to the mode of the spread of disease was not conducted [4,58]. Therefore, it is possible that family sharing of utensils for hand washing and drinking and eating, a common practice in resource-poor countries, along with poor hand hygiene, may allow cross-contamination of water and eatables, leading to person-to-person transfer of the virus during an outbreak.
4.2.2. Sporadic Disease
The mode of transmission of sporadic disease caused by HEV-1 and HEV-2 is also under scrutiny [72]. In the first reported series on sporadic hepatitis E, it was found [15] that 51 (33%) of the 155 cases had had recent contact with another case of jaundice, suggesting that person-to-person contact could play an important role in the transmission of sporadic hepatitis E. Khuroo, et al. [74] studied 62 household contacts of 13 index patients and showed that 18 (29%) had developed evidence of HEV infection at 31 ± 4.5 days after the onset of disease in the index patient. This suggested that the disease was spread via household contact from the index patient, rather than simultaneous infection of the index patient and household contact. However, Somani, et al. [78] reported that intrafamilial spread of sporadic HEV infection occurred infrequently. It is possible that sporadic HEV infections may occur in the setting of environmental contamination of agricultural products and water resources, and spread of infections through infected food and water. Raw sewage has been found to contain infectious HEV strains in developing countries, which closely relates to human HEV-1 and HEV-2 [61,79,80].
4.3. Zoonotic Transmission
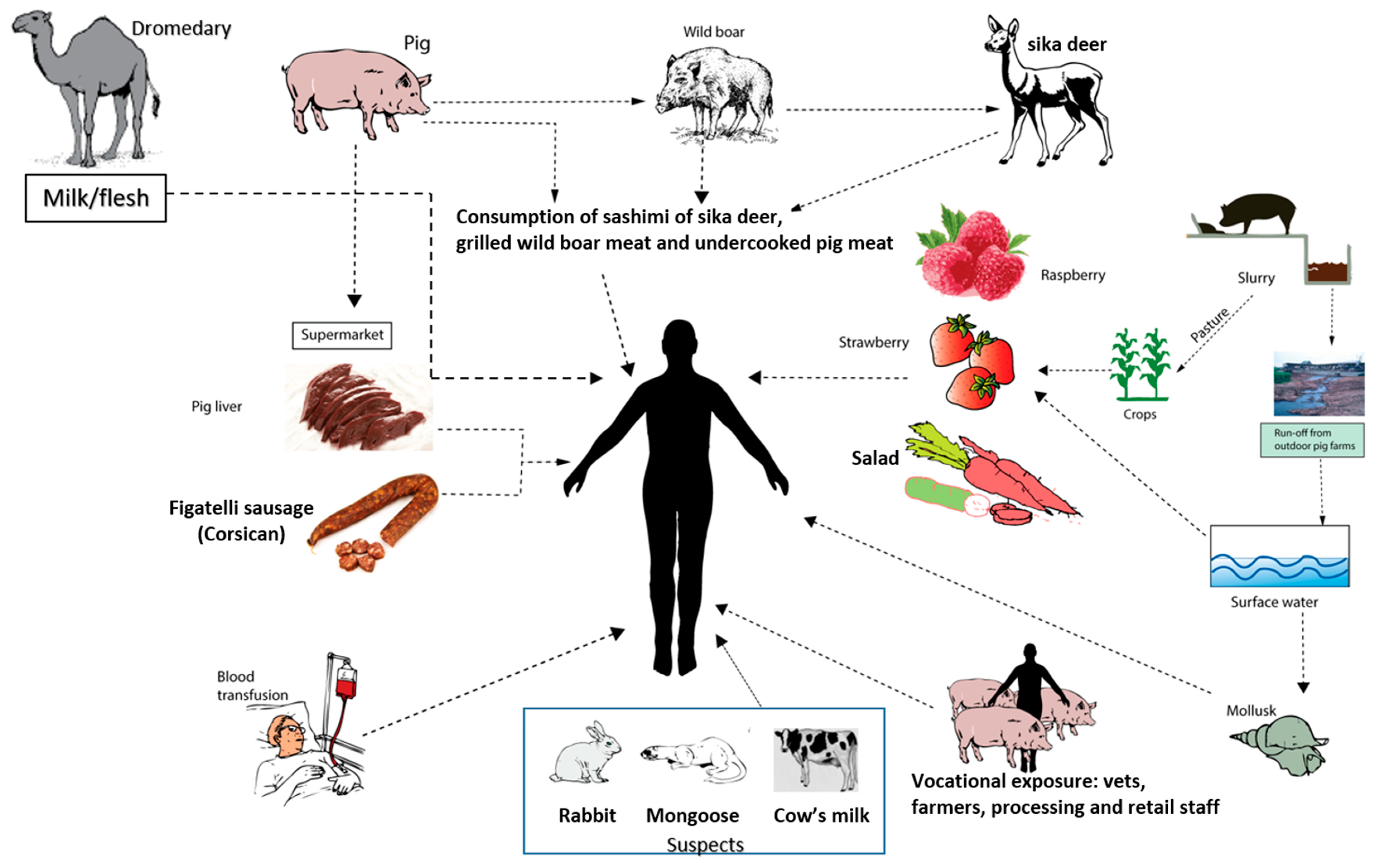
Hepatitis E is a zoonotic disease, and domestic pigs, wild boar, and sika deer are reservoirs for genotypes HEV-3 and HEV-4 [81]. Human infections occur through three methods, namely, zoonotic foodborne consumption, direct contact with infected animals, and environmental contamination by animal manure run-off (Figure 5) [82]. Food-borne zoonotic transmission of HEV-3 and HEV-4 has been well studied [56,82]. Wild boar, sika deer, and domestic pigs cross transmit HEV [83], and eating the parboiled flesh or liver (a delicacy in many countries) could be responsible for the autochthonous cases and outbreaks of hepatitis E [84]. A more common method of the spread of HEV is through consumption of raw livers from supermarkets or eating Corsican figatelli sausage in Europe [85,86,87]. Such livers and sausages are often infected with live HEV. Vocational exposure to domestic pig farms, manure, and sewage is also a significant risk factor in HEV infections in many countries [88,89,90]. Swine veterinarians as well as workers, were found to be 2 to 5 times more likely to be positive for IgG anti-HEV than non-swine veterinarians and the general population in many European countries [91,92,93,94]. Additionally, pig slurry can cause environmental contamination through several ways. Use of pig slurry as pasture can infect agricultural products like raspberries, strawberries, and many vegetables used in salad [95,96]. Run-off from outdoor pig farms causes contamination of surface water as well as produce receiving surface water [97,98].
Run-off from outdoor pig farms can also contaminate coastal waters and seafood, such as fish and shellfish [99]. HEV has been identified in commercially available mussels from several European countries [100,101], Korea [102], and Japan [103]. Consumption of shellfish has been identified as a risk factor for hepatitis E in several case reports [104,105,106] and in an outbreak of hepatitis E aboard a cruise ship [107].
HEV infections in animals in India have been the focus of a number of studies. HEV infection is ubiquitous in several animal species, including domestic pigs, sheep, goats, and buffalo [108]. Arankalle, et al. [109] studied 284 domestic pigs from Maharashtra, India were studied, where 122 (42.6%) and 13 (4.6%) animals were reactive for IgG antibodies to HEV and HEV RNA, respectively. All isolates from domestic pigs were of genotype HEV-4. Therefore, since human HEV infections are caused uniformly by genotype HEV-1 in India, both epidemic and sporadic, it is believed that human and pig HEV infections are unrelated, and zoonotic transmission plays an insignificant role in human infections in India [109].
While studying HEV in dromedaries in Dubai, U.A.E., Woo et al. [31] used fecal samples to isolate from three camels a previously unrecognized HEV genotype, designated as HEV-7. Subsequently, a liver transplant patient from the Middle East was found to be infected with HEV-7 and had developed chronic hepatitis, requiring antiviral therapy. He regularly consumed camel flesh and drank camel milk [30]. Recently 2438 dromedary samples from Sudan, Somalia, Egypt, Kenya, Pakistan, and the United Arab Emirates were screened for HEV-7. Ninety-six (45.7%) of the 210 animals were seropositive for IgG anti-HEV, while HEV RNA was isolated from 12 (0.5%) of the 2171 serum samples and five (1.9%) of the 267 fecal samples [110]. Further studies need to be done to evaluate the potential of camelid HEV-7 to cause the human disease.
Hepatitis E in China has a complex and changing epidemiology. Initially, China was a hyperendemic zone for HEV-1, and contained multiple epidemics of hepatitis E [111]. In fact, China witnessed the largest ever (119,280 cases) epidemic of hepatitis E from 1986 to 1988 [112]. However, HEV-4 has now become the dominant genotype infecting the Chinese population. This is especially true for northeast China and is possibly related to the introduction of infection via animal reservoirs, especially domestic pigs [113].
4.4. Parenteral Transmission
In a case control study, Khuroo, et al. [114] documented transfusion-transmitted hepatitis E. Thirteen HEV infections (IgM anti-HEV & HEV RNA) of 145 multiply transfused subjects were detected, as opposed to two infections of 250 subjects not transfused. 25 susceptible (IgG anti-HEV negative) patients were prospectively studied following multiple transfusion, and three post-transfusion infections were detected. These infections were traced to four of the 107 donors. These donors were positive for HEV RNA at the time of blood donation. All four donors were asymptomatic and all transfusion-associated infections in Kashmir were caused by genotype HEV-1. Subsequent to this report, a Japanese patient was found to have developed transfusion-associated HEV infection and the authors reported a complete donor–patient sequence homology, confirming observations on transfusion-transmitted hepatitis E [115]. Several cases and case series of transfusion-associated HEV infections were reported from multiple countries [116,117]. In a recent study by Hewitt, et al. [118], 18 (42%) of 42 HEV-positive transfusion recipients were found to have contracted HEV-3 infections. Of these, three had short-lasting viremia, while 10 developed prolonged and persistent infections.
HEV RNA has been detected in healthy populations from many countries (Table 2) [119,120,121]. Viremia varied from 1 out of 672 donations (Germany) to 1 out of 8416 donations (Austria). The duration of viremia extends up to 45 days and the infectious dose of HEV is as low as its detection by RT-PCR [122,123,124,125]. Based on these data, it was estimated that around 80,000–100,000 transfusion-associated HEV infections had occurred in England in 2013. Of the 7.4 million blood products administered in Germany per year, 1600 to 5900 transfusion-associated HEV infections had occurred. Blood or blood products are often required for several clinical conditions in which hepatitis E runs a more severe course or leads to chronic hepatitis and cirrhosis. These include pregnancy, liver disease, solid organ transplant (SOT), HIV positive status, and hematological neoplasm. In view of the above data, there is a need to conduct screening of blood donors in countries with high HEV prevalence.
4.5. Vertical Transmission
HEV can be transmitted vertically to the fetus and infant from infected mothers. We studied eight mothers who had HEV infection for evidence of vertical transmission. Six babies had contracted vertically transmitted HEV infection [14]. In another study, 26 pregnant women with HEV infection were studied for a pattern of vertically-transmitted HEV infection. [130]. Five mothers had died prior to delivery, two aborted the fetuses, four delivered premature babies, and 15 had completed pregnancy with normal deliveries. Out of the 19 babies evaluated, 12 were reactive for IgM anti-HEV and 10 showed viremia. In all, 15 (78.9%) had evidence of intrauterine HEV infection. HEV infection in babies presented as icteric hepatitis in seven, anicteric hepatitis in five, and jaundice alone in three. Six newborns died from liver failure and one neonate died from premature birth and low birthweight. Nine HEV infected babies who survived had short-lasting viremia and none showed evidence of chronic hepatitis or cirrhosis. Subsequent to these reports, a number of reports have documented intrauterine transmission of HEV infection with high maternal and fetal mortality (Table 3) [50,131]. Recently, HEV replication was found to occur within the placenta and was correlated with fetal and maternal mortality from acute liver failure [132]. In a study by Khuroo, et al. [133], the outcome of 36 pregnant women with hepatitis E was evaluated, assessing the occurrence and severity of vertically transmitted HEV infection in fetuses/neonates, and a relationship between the severity of disease in the fetus with the severity and outcome of disease in the mother was found. This lead to the postulation that acute liver failure in pregnant women may be an example of mirror syndrome, akin to acute fatty liver of pregnancy.
4.6. Nosocomial Transmission
Nosocomial transmission of HEV infections is unusual and most healthcare workers and inpatient populations are not at a high risk for contracting the virus. However, several reports have focused on the transmission of HEV infection in hemodialysis units [137,138,139,140] and a few have reported outbreaks of hepatitis E in hospital patients and healthcare workers [141,142,143].
4.7. Sexual Transmission
4.8. HEV and Milk
Chibber, et al. [135] studied 93 HEV infected mothers for HEV RNA in colostrum and the role of breast feeding to transmit infection to neonates. Anti-HEV antibody and HEV RNA were uniformly detected in colostral samples of HEV-infected mothers. However, the levels of antibodies and HEV RNA were significantly lower than those in maternal blood samples, and therefore breastfeeding was considered to be an unlikely route of transmission for neonatal HEV infection [135]. Recently however, HEV RNA was isolated from breast milk from a mother with acute HEV [149]. Subsequently, additional studies need to be performed to test breast milk for HEV RNA and advise whether neonates should be breastfeeding from infected mothers.
As mentioned above, transmission of camelid HEV (genotype 7) from a dromedary to a liver transplant patient was reported in Dubai [3,4]. This patient had regularly consumed camel flesh and camel milk [30]. As HEV infections are common in dromedaries from many countries, the role of camel milk in the spread of HEV in such communities needs further scrutiny [110]. Recently, Huang, et al. [150] studied 140 cows from Dali, Yunnan, China, from September to December 2015. In this community, mixed farming of domestic animals is a common practice. Active HEV infection was found in 52 cows, as determined by viral RNA positivity in fecal samples. All 52 infected animals were excreting HEV-RNA in milk samples in high titers. HEV-RNA recovered from raw and pasteurized milk samples have also been shown to transmit the disease to rhesus monkeys. However, a short period of boiling, even without pasteurization, has the potential to completely inactivate HEV. Phylogenetic analysis revealed that all HEV isolates from cow-milk belong to genotype 4 and subtype 4h. These findings need to be confirmed, and the role of infectious HEV-contaminated cow’s milk in the spread of HEV infections in endemic regions must be further defined.
5. Conclusions
In conclusion, epidemics of hepatitis E caused by HEV-1 and 2 in resource-poor countries are spread through water that has been contaminated by sewage, of which, several environmental settings contribute to fecal contamination of water supplies to such communities. Person-to-person spread of HEV infection has been implicated in epidemics with a protracted course and also in the endemic disease. Food-borne zoonotic transmission is the dominant route of spread for HEV-3 and -4 and occurs through the consumption of parboiled meat or liver of HEV-infected domestic pig, wild boar, sika Deer or Corsican figatelli sausage. The waste water of domestic pig dung in such countries may pollute waterways and infect those who visit sea beaches or ingest infected mollusks. HEV infection in pregnant women is uniformly spread through vertical transmission to the fetus, which can cause significant morbidity and mortality in fetuses and newborn babies. Transfusion-transmitted HEV is now being recognized as an important route of transmission in many countries and poses a potential risk to organ transplant patients. Lastly, recent data on the spread of HEV-7 through camel flesh/milk and detection of HEV-4 in high titers in cow’s milk in mixed animal farms from China, opens up a new vista for exploring the transmission routes of HEV infection.
Acknowledgments
This work was supported by Dr. Khuroo’s Medical Trust, a nonprofit organization that supports academic activities, disseminates medical education, and helps poor patients obtain medical treatment.
Author Contributions
All three authors contributed equally. Mehnaaz S. Khuroo and Naira S. Khuroo conducted the literature search, while Mohammad S. Khuroo wrote the paper. All authors proofed the paper to make necessary corrections.
Conflicts of Interest
The authors report no conflict of interest.
References
- Khuroo, M.S.; Khuroo, M.S. Hepatitis E: An emerging global disease—From discovery towards control and cure. J. Viral Hepat. 2016, 23, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Khuroo, M.S. Sanitation and sewage disposal in India. JK-Practitioner 2015, 20, 43–46. [Google Scholar]
- Khuroo, M.S. Hepatitis E: The enterically transmitted non-a, non-b hepatitis. Indian J. Gastroenterol. 1991, 10, 96–100. [Google Scholar] [PubMed]
- Khuroo, M.S. Discovery of hepatitis E: The epidemic non-a, non-b hepatitis 30 years down the memory lane. Virus Res. 2011, 161, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Pavio, N.; Meng, X.J.; Renou, C. Zoonotic hepatitis E: Animal reservoirs and emerging risks. Vet. Res. 2010, 41, 46. [Google Scholar] [CrossRef] [PubMed]
- Thiry, D.; Mauroy, A.; Pavio, N.; Purdy, M.A.; Rose, N.; Thiry, E.; de Oliveira-Filho, E.F. Hepatitis E virus and related viruses in animals. Transbound. Emerg. Dis. 2015. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. List of Developing Countries. In Proceedings of the 26th General Assembly International Union Geodesy and Geophysics, Prague, Czech Republic, 22 June–2 July 2015; Available online: www.iugg2015prague.com (accessed on 30 June 2016).
- Khuroo, M.S. Study of an epidemic of non-a, non-b hepatitis. Possibility of another human hepatitis virus distinct from post-transfusion non-a, non-b type. Am. J. Med. 1980, 68, 818–824. [Google Scholar] [CrossRef]
- Khuroo, M.S. Discovery of Hepatitis E: The Untold Story. 1 September 2011. Available online: https://youtu.be/idoeaMbcbk0 (accessed on 30 June 2016).
- Khuroo, M.S.; Teli, M.R.; Skidmore, S.; Sofi, M.A.; Khuroo, M.I. Incidence and severity of viral hepatitis in pregnancy. Am. J. Med. 1981, 70, 252–255. [Google Scholar] [CrossRef]
- Khuroo, M.S.; Saleem, M.; Teli, M.R.; Sofi, M.A. Failure to detect chronic liver disease after epidemic non-A, non-B hepatitis. Lancet 1980, 2, 97–98. [Google Scholar] [CrossRef]
- Khuroo, M.S. Chronic liver disease after non-A, non-B hepatitis. Lancet 1980, 2, 860–861. [Google Scholar] [PubMed]
- Jameel, S.; Durgapal, H.; Habibullah, C.M.; Khuroo, M.S.; Panda, S.K. Enteric non-A, non-B hepatitis: Epidemics, animal transmission, and hepatitis E virus detection by the polymerase chain reaction. J. Med. Virol. 1992, 37, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Kamili, S.; Jameel, S. Vertical transmission of hepatitis E virus. Lancet 1995, 345, 1025–1026. [Google Scholar]
- Khuroo, M.S.; Duermeyer, W.; Zargar, S.A.; Ahanger, M.A.; Shah, M.A. Acute sporadic non-A, non-B hepatitis in India. Am. J. Epidemiol. 1983, 118, 360–364. [Google Scholar] [PubMed]
- Khuroo, M.S.; Kamili, S. Aetiology, clinical course and outcome of sporadic acute viral hepatitis in pregnancy. J. Viral Hepat. 2003, 10, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Rustgi, V.K.; Dawson, G.J.; Mushahwar, I.K.; Yattoo, G.N.; Kamili, S.; Khan, B.A. Spectrum of hepatitis E virus infection in India. J. Med. Virol. 1994, 43, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Kamili, S. Aetiology and prognostic factors in acute liver failure in India. J. Viral Hepat. 2003, 10, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S. Acute liver failure in india. Hepatology 1997, 26, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Balayan, M.S.; Andjaparidze, A.G.; Savinskaya, S.S.; Ketiladze, E.S.; Braginsky, D.M.; Savinov, A.P.; Poleschuk, V.F. Evidence for a virus in non-A, non-B hepatitis transmitted via the fecal-oral route. Intervirology 1983, 20, 23–31. [Google Scholar] [PubMed]
- Bradley, D.W.; Purdy, M.A.; Reyes, G.R. Hepatitis E virus genome. Molecular features, expression of immunoreactive proteins and sequence divergence. J. Hepatol. 1991, 13 (Suppl. S4), S152–S154. [Google Scholar] [CrossRef]
- Reyes, G.R.; Purdy, M.A.; Kim, J.P.; Luk, K.C.; Young, L.M.; Fry, K.E.; Bradley, D.W. Isolation of a cDNA from the virus responsible for enterically transmitted non-A, non-B hepatitis. Science 1990, 247, 1335–1339. [Google Scholar] [CrossRef] [PubMed]
- Tam, A.W.; Smith, M.M.; Guerra, M.E.; Huang, C.C.; Bradley, D.W.; Fry, K.E.; Reyes, G.R. Hepatitis E virus (HEV): Molecular cloning and sequencing of the full-length viral genome. Virology 1991, 185, 120–131. [Google Scholar] [CrossRef]
- Yarbough, P.O.; Tam, A.W.; Fry, K.E.; Krawczynski, K.; McCaustland, K.A.; Bradley, D.W.; Reyes, G.R. Hepatitis E virus: Identification of type-common epitopes. J. Virol. 1991, 65, 5790–5797. [Google Scholar] [PubMed]
- Khuroo, M.S. Hepatitis E virus: Another addition to the existing alphabet of human hepatitis viruses. Ann. Saudi Med. 1996, 16, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Holla, R.P.; Ahmad, I.; Ahmad, Z.; Jameel, S. Molecular virology of hepatitis E virus. Semin. Liver Dis. 2013, 33, 3–14. [Google Scholar] [PubMed]
- Meng, X.J. From barnyard to food table: The omnipresence of hepatitis E virus and risk for zoonotic infection and food safety. Virus Res. 2011, 161, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.B.; Simmonds, P.; Jameel, S.; Emerson, S.U.; Harrison, T.J.; Meng, X.J.; Okamoto, H.; Van der Poel, W.H.; Purdy, M.A.; International Committee on the Taxonomy of Viruses Hepeviridae Study Group. Consensus proposals for classification of the family hepeviridae. J. Gen. Virol. 2014, 95, 2223–2232. [Google Scholar] [CrossRef] [PubMed]
- Cossaboom, C.M.; Cordoba, L.; Dryman, B.A.; Meng, X.J. Hepatitis E virus in rabbits, Virginia, USA. Emerg. Infect. Dis. 2011, 17, 2047–2049. [Google Scholar] [CrossRef] [PubMed]
- Izopet, J.; Dubois, M.; Bertagnoli, S.; Lhomme, S.; Marchandeau, S.; Boucher, S.; Kamar, N.; Abravanel, F.; Guerin, J.L. Hepatitis E virus strains in rabbits and evidence of a closely related strain in humans, France. Emerg. Infect. Dis 2012, 18, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.C.; Lau, S.K.; Teng, J.L.; Tsang, A.K.; Joseph, M.; Wong, E.Y.; Tang, Y.; Sivakumar, S.; Xie, J.; Bai, R.; et al. New hepatitis E virus genotype in camels, the Middle East. Emerg. Infect. Dis. 2014, 20, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.H.; Tan, B.H.; Chi-Yuan Teo, E.; Lim, S.G.; Dan, Y.Y.; Wee, A.; Kim Aw, P.P.; Zhu, Y.; Hibberd, M.L.; Tan, C.K.; et al. Chronic infection with camelid hepatitis E virus in a liver transplant recipient who regularly consumes camel meat and milk. Gastroenterology 2016, 150, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Yugo, D.M.; Cossaboom, C.M.; Meng, X.J. Naturally occurring animal models of human hepatitis E virus infection. ILAR J. 2014, 55, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Teshale, E.H.; Hu, D.J.; Holmberg, S.D. The two faces of hepatitis E virus. Clin. Infect. Dis. 2010, 51, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Pischke, S.; Wedemeyer, H. Hepatitis E virus infection: Multiple faces of an underestimated problem. J. Hepatol. 2013, 58, 1045–1046. [Google Scholar] [CrossRef] [PubMed]
- Riveiro-Barciela, M.; Rodriguez-Frias, F.; Buti, M. Hepatitis E virus: New faces of an old infection. Ann. Hepatol. 2013, 12, 861–870. [Google Scholar] [PubMed]
- Rein, D.B.; Stevens, G.A.; Theaker, J.; Wittenborn, J.S.; Wiersma, S.T. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology 2012, 55, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Kamili, S.; Dar, M.Y.; Moecklii, R.; Jameel, S. Hepatitis E and long-term antibody status. Lancet 1993, 341, 1355. [Google Scholar] [PubMed]
- Khuroo, M.S.; Khuroo, M.S. Seroepidemiology of a second epidemic of hepatitis E in a population that had recorded first epidemic 30 years before and has been under surveillance since then. Hepatol. Int. 2010, 4, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Labrique, A.B.; Zaman, K.; Hossain, Z.; Saha, P.; Yunus, M.; Hossain, A.; Ticehurst, J.R.; Nelson, K.E. Epidemiology and risk factors of incident hepatitis E virus infections in rural Bangladesh. Am. J. Epidemiol. 2010, 172, 952–961. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.K.; Thakral, D.; Rehman, S. Hepatitis E virus. Rev. Med. Virol. 2007, 17, 151–180. [Google Scholar] [CrossRef] [PubMed]
- Fierro, N.A.; Realpe, M.; Meraz-Medina, T.; Roman, S.; Panduro, A. Hepatitis E virus: An ancient hidden enemy in Latin America. World J. Gastroenterol. 2016, 22, 2271–2283. [Google Scholar] [PubMed]
- Huang, R.T.; Li, D.R.; Wei, J.; Huang, X.R.; Yuan, X.T.; Tian, X. Isolation and identification of hepatitis E virus in Xinjiang, China. J. Gen. Virol. 1992, 73, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Hamid, S.S.; Atiq, M.; Shehzad, F.; Yasmeen, A.; Nissa, T.; Salam, A.; Siddiqui, A.; Jafri, W. Hepatitis E virus superinfection in patients with chronic liver disease. Hepatology 2002, 36, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Aggarwal, R.; Naik, S.R.; Saraswat, V.; Ghoshal, U.C.; Naik, S. Hepatitis E virus is responsible for decompensation of chronic liver disease in an endemic region. Indian J. Gastroenterol. 2004, 23, 59–62. [Google Scholar] [PubMed]
- Arif, M. Enterically transmitted hepatitis in Saudi Arabia: An epidemiological study. Ann. Trop. Med. Parasitol. 1996, 90, 197–201. [Google Scholar] [PubMed]
- Saffar, M.J.; Farhadi, R.; Ajami, A.; Khalilian, A.R.; Babamahmodi, F.; Saffar, H. Seroepidemiology of hepatitis E virus infection in 2–25-year-olds in Sari district, Islamic Republic of Iran. East. Mediterr. Health J. 2009, 15, 136–142. [Google Scholar] [PubMed]
- Coursaget, P.; Depril, N.; Yenen, O.S.; Cavuslu, S.; Badur, S. Hepatitis E virus infection in Turkey. Lancet 1993, 342, 810–811. [Google Scholar] [CrossRef]
- Chow, W.C.; Lee, A.S.; Lim, G.K.; Cheong, W.K.; Chong, R.; Tan, C.K.; Yap, C.K.; Oon, C.J.; Ng, H.S. Acute viral hepatitis E: Clinical and serologic studies in Singapore. J. Clin. Gastroenterol. 1997, 24, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.M.; Uduman, S.; Rana, S.; Kochiyil, J.K.; Usmani, A.; Thomas, L. Sero-prevalence and mother-to-infant transmission of hepatitis E virus among pregnant women in the United Arab Emirates. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 100, 9–15. [Google Scholar] [CrossRef]
- Blackard, J.T.; Rouster, S.D.; Nady, S.; Galal, G.; Marzuuk, N.; Rafaat, M.M.; Daef, E.; El Din, S.S.; Purcell, R.H.; Emerson, S.U.; et al. Genotypic characterization of symptomatic hepatitis E virus (HEV) infections in Egypt. J. Clin. Virol. 2009, 46, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Aboulata, A.A.; Ahmad, M.S.; Shaban, M.M.; Zayd, K.M.; Abd El-Moktader, A.M. Prevalence of hepatitis E virus in Egyptian children presented with minor hepatic disorders. Egypt J. Immunol. 2005, 12, 71–76. [Google Scholar] [PubMed]
- Abdel, H.S.; El-Din, M.S.; El-Din, M.E. A high hepatitis E virus (HEV) seroprevalence among unpaid blood donors and haemodialysis patients in Egypt. J. Egypt Public Health Assoc. 1998, 73, 165–179. [Google Scholar]
- Meng, X.J. Zoonotic and foodborne transmission of hepatitis E virus. Semin. Liver Dis. 2013, 33, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Selves, J.; Mansuy, J.M.; Ouezzani, L.; Peron, J.M.; Guitard, J.; Cointault, O.; Esposito, L.; Abravanel, F.; Danjoux, M.; et al. Hepatitis E virus and chronic hepatitis in organ-transplant recipients. N. Engl. J. Med. 2008, 358, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Izopet, J.; Kamar, N. Hepatitis E: From zoonotic transmission to chronic infection in immunosuppressed patients. Med. Sci. 2008, 24, 1023–1025. [Google Scholar]
- Vishwanathan, R. Infectious hepatitis in Delhi (1955–1956). A critical study: Epidemiology. Indian J. Med. Res. 1957, 45, 49–58. [Google Scholar]
- Naik, S.R.; Aggarwal, R.; Salunke, P.N.; Mehrotra, N.N. A large waterborne viral hepatitis E epidemic in Kanpur, India. Bull. World Health Organ. 1992, 70, 597–604. [Google Scholar] [PubMed]
- Kane, M.A.; Bradley, D.W.; Shrestha, S.M.; Maynard, J.E.; Cook, E.H.; Mishra, R.P.; Joshi, D.D. Epidemic non-A, non-B hepatitis in Nepal. Recovery of a possible etiologic agent and transmission studies in marmosets. JAMA 1984, 252, 3140–3145. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, S.R.; Tilekar, B.N.; Walimbe, A.M.; Arankalle, V.A. Increased risk of hepatitis E in sewage workers from India. J. Occup. Environ. Med. 2003, 45, 1167–1170. [Google Scholar] [CrossRef] [PubMed]
- Ippagunta, S.K.; Naik, S.; Sharma, B.; Aggarwal, R. Presence of hepatitis E virus in sewage in Northern India: Frequency and seasonal pattern. J. Med. Virol. 2007, 79, 1827–1831. [Google Scholar] [CrossRef] [PubMed]
- Ishida, S.; Yoshizumi, S.; Ikeda, T.; Miyoshi, M.; Goto, A.; Matsubayashi, K.; Ikeda, H. Detection and molecular characterization of hepatitis E virus in clinical, environmental and putative animal sources. Arch. Virol. 2012, 157, 2363–2368. [Google Scholar] [CrossRef] [PubMed]
- Masclaux, F.G.; Hotz, P.; Friedli, D.; Savova-Bianchi, D.; Oppliger, A. High occurrence of hepatitis E virus in samples from wastewater treatment plants in Switzerland and comparison with other enteric viruses. Water Res. 2013, 47, 5101–5109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corwin, A.; Jarot, K.; Lubis, I.; Nasution, K.; Suparmawo, S.; Sumardiati, A.; Widodo, S.; Nazir, S.; Orndorff, G.; Choi, Y.; et al. Two years’ investigation of epidemic hepatitis E virus transmission in West Kalimantan (Borneo), Indonesia. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 262–265. [Google Scholar] [CrossRef]
- Gurav, Y.K.; Kakade, S.V.; Kakade, R.V.; Kadam, Y.R.; Durgawale, P.M. A study of hepatitis E outbreak in rural area of Western Maharashtra. Indian J. Community Med. 2007, 32, 182–184. [Google Scholar] [CrossRef]
- Clayson, E.T.; Vaughn, D.W.; Innis, B.L.; Shrestha, M.P.; Pandey, R.; Malla, D.B. Association of hepatitis E virus with an outbreak of hepatitis at a military training camp in Nepal. J. Med. Virol. 1998, 54, 178–182. [Google Scholar] [CrossRef]
- Singh, V.; Singh, V.; Raje, M.; Nain, C.K.; Singh, K. Routes of transmission in the hepatitis E epidemic of Saharanpur. Trop. Gastroenterol. 1998, 19, 107–109. [Google Scholar] [PubMed]
- Sailaja, B.; Murhekar, M.V.; Hutin, Y.J.; Kuruva, S.; Murthy, S.P.; Reddy, K.S.; Rao, G.M.; Gupte, M.D. Outbreak of waterborne hepatitis E in Hyderabad, India, 2005. Epidemiol. Infect. 2009, 137, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, N.T.; Prajapati, P.; Trivedi, A.V.; Bhagyalaxmi, A. Epidemic investigation of the jaundice outbreak in Girdharnagar, Ahmedabad, Gujarat, India, 2008. Indian J. Community Med. 2010, 35, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Bali, S.; Kar, S.S.; Kumar, S.; Ratho, R.K.; Dhiman, R.K.; Kumar, R. Hepatitis E epidemic with bimodal peak in a town of North India. Indian J. Public Health 2008, 52, 189–193, 199. [Google Scholar] [PubMed]
- Goldsmith, R.; Yarbough, P.O.; Reyes, G.R.; Fry, K.E.; Gabor, K.A.; Kamel, M.; Zakaria, S.; Amer, S.; Gaffar, Y. Enzyme-linked immunosorbent assay for diagnosis of acute sporadic hepatitis E in Egyptian children. Lancet 1992, 339, 328–331. [Google Scholar] [CrossRef]
- Aggarwal, R. Hepatitis E virus and person-to-person transmission. Clin. Infect. Dis. 2010, 51, 477–478; author reply 478–479. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Naik, S.R. Hepatitis E: Does person-to-person spread occur? Indian J. Gastroenterol. 1992, 11, 109–112. [Google Scholar] [PubMed]
- Khuroo, M.S.; Dar, M.Y. Hepatitis E: Evidence for person-to-person transmission and inability of low dose immune serum globulin from an Indian source to prevent it. Indian J. Gastroenterol. 1992, 11, 113–116. [Google Scholar] [PubMed]
- Arankalle, V.A.; Chadha, M.S.; Mehendale, S.M.; Tungatkar, S.P. Epidemic hepatitis E: Serological evidence for lack of intrafamilial spread. Indian J. Gastroenterol. 2000, 19, 24–28. [Google Scholar] [PubMed]
- Teshale, E.H.; Grytdal, S.P.; Howard, C.; Barry, V.; Kamili, S.; Drobeniuc, J.; Hill, V.R.; Okware, S.; Hu, D.J.; Holmberg, S.D. Evidence of person-to-person transmission of hepatitis E virus during a large outbreak in Northern Uganda. Clin. Infect. Dis. 2010, 50, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- Teshale, E.H.; Howard, C.M.; Grytdal, S.P.; Handzel, T.R.; Barry, V.; Kamili, S.; Drobeniuc, J.; Okware, S.; Downing, R.; Tappero, J.W.; et al. Hepatitis E epidemic, Uganda. Emerg. Infect. Dis. 2010, 16, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Somani, S.K.; Aggarwal, R.; Naik, S.R.; Srivastava, S.; Naik, S. A serological study of intrafamilial spread from patients with sporadic hepatitis E virus infection. J. Viral Hepat. 2003, 10, 446–449. [Google Scholar] [CrossRef] [PubMed]
- Jothikumar, N.; Aparna, K.; Kamatchiammal, S.; Paulmurugan, R.; Saravanadevi, S.; Khanna, P. Detection of hepatitis E virus in raw and treated wastewater with the polymerase chain reaction. Appl. Environ. Microbiol. 1993, 59, 2558–2562. [Google Scholar] [PubMed]
- Vaidya, S.R.; Chitambar, S.D.; Arankalle, V.A. Polymerase chain reaction-based prevalence of hepatitis A, hepatitis E and TT viruses in sewage from an endemic area. J. Hepatol. 2002, 37, 131–136. [Google Scholar] [CrossRef]
- Pavio, N.; Meng, X.J.; Doceul, V. Zoonotic origin of hepatitis E. Curr. Opin. Virol. 2015, 10, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Yugo, D.M.; Meng, X.J. Hepatitis E virus: Foodborne, waterborne and zoonotic transmission. Int. J. Environ. Res. Public Health 2013, 10, 4507–4533. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Khuroo, M.S. Hepatitis E virus. Curr. Opin. Infect. Dis. 2008, 21, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, K.; Kang, J.H.; Saga, A.; Takahashi, K.; Shimamura, T.; Yasumoto, A.; Fukushima, H.; Sogabe, S.; Konishi, K.; Uchida, T.; et al. Three cases of acute or fulminant hepatitis E caused by ingestion of pork meat and entrails in Hokkaido, Japan: Zoonotic food-borne transmission of hepatitis E virus and public health concerns. Hepatol. Res. 2012, 42, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Borentain, P.; Queyriaux, B.; Kaba, M.; Moal, V.; Gallian, P.; Heyries, L.; Raoult, D.; Gerolami, R. Pig liver sausage as a source of hepatitis E virus transmission to humans. J. Infect. Dis. 2010, 202, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Garbuglia, A.R.; Alessandrini, A.I.; Pavio, N.; Tesse, S.; Grignolo, S.; Viscoli, C.; Lapa, D.; Capobianchi, M.R. Male patient with acute hepatitis E in Genoa, Italy: Figatelli (pork liver sausage) as probable source of the infection. Clin. Microbiol. Infect. 2015, 21, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, H.; Okada, K.; Takahashi, K.; Mishiro, S. Severe hepatitis E virus infection after ingestion of uncooked liver from a wild boar. J. Infect. Dis. 2003, 188, 944. [Google Scholar] [CrossRef] [PubMed]
- Bouwknegt, M.; Frankena, K.; Rutjes, S.A.; Wellenberg, G.J.; de Roda Husman, A.M.; van der Poel, W.H.; de Jong, M.C. Estimation of hepatitis E virus transmission among pigs due to contact-exposure. Vet. Res. 2008, 39, 40. [Google Scholar] [CrossRef] [PubMed]
- Rutjes, S.A.; Lodder, W.J.; Lodder-Verschoor, F.; van den Berg, H.H.; Vennema, H.; Duizer, E.; Koopmans, M.; de Roda Husman, A.M. Sources of hepatitis E virus genotype 3 in The Netherlands. Emerg. Infect. Dis. 2009, 15, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Perez-Gracia, M.T.; Mateos, M.L.; Galiana, C.; Fernandez-Barredo, S.; Garcia, A.; Gomez, M.T.; Moreira, V. Autochthonous hepatitis E infection in a slaughterhouse worker. Am. J. Trop. Med. Hyg. 2007, 77, 893–896. [Google Scholar] [PubMed]
- Galiana, C.; Fernandez-Barredo, S.; Garcia, A.; Gomez, M.T.; Perez-Gracia, M.T. Occupational exposure to hepatitis E virus (HEV) in swine workers. Am. J. Trop. Med. Hyg. 2008, 78, 1012–1015. [Google Scholar] [PubMed]
- Bouwknegt, M.; Engel, B.; Herremans, M.M.; Widdowson, M.A.; Worm, H.C.; Koopmans, M.P.; Frankena, K.; de Roda Husman, A.M.; De Jong, M.C.; Van Der Poel, W.H. Bayesian estimation of hepatitis E virus seroprevalence for populations with different exposure levels to swine in The Netherlands. Epidemiol. Infect. 2008, 136, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Vulcano, A.; Angelucci, M.; Candelori, E.; Martini, V.; Patti, A.M.; Mancini, C.; Santi, A.L.; Calvani, A.; Casagni, L.; Lamberti, A. prevalence in the general population and among workers at zoonotic risk in Latium region. Ann. Ig. 2007, 19, 181–186. [Google Scholar] [PubMed]
- Olsen, B.; Axelsson-Olsson, D.; Thelin, A.; Weiland, O. Unexpected high prevalence of igg-antibodies to hepatitis E virus in swedish pig farmers and controls. Scand. J. Infect. Dis. 2006, 38, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Ward, P.; Muller, P.; Letellier, A.; Quessy, S.; Simard, C.; Trottier, Y.L.; Houde, A.; Brassard, J. Molecular characterization of hepatitis E virus detected in swine farms in the province of Quebec. Can. J. Vet. Res. 2008, 72, 27–31. [Google Scholar] [PubMed]
- Brassard, J.; Gagne, M.J.; Genreux, M.; Cote, C. Detection of huamn food-borne and zoonotic viruses on irrigated, field-grown strwberries. Appl. Environ. Microbiol. 2012, 78, 3763–3766. [Google Scholar] [CrossRef] [PubMed]
- Steyer, A.; Naglic, T.; Mocilnik, T.; Poljsak-Prijatelj, M.; Poljak, M. Hepatitis E virus in domestic pigs and surface waters in Slovenia: Prevalence and molecular characterization of a novel genotype 3 lineage. Infect. Genet. Evol. 2011, 11, 1732–1737. [Google Scholar] [CrossRef] [PubMed]
- Tyrrel, S.F.; Quinton, J.N. Overland flow transport of pathogens from agricultural land receiving faecal wastes. J. Appl. Microbiol. 2003, 94, 87S–93S. [Google Scholar] [CrossRef] [PubMed]
- Namsai, A.; Louisirirotchanakul, S.; Wongchinda, N.; Siripanyaphinyo, U.; Virulhakul, P.; Puthavathana, P.; Myint, K.S.; Gannarong, M.; Ittapong, R. Surveillance of hepatitis A and E viruses contamination in shellfish in Thailand. Lett. Appl. Microbiol. 2011, 53, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Diez-Valcarce, M.; Kokkinos, P.; Soderberg, K.; Bouwknegt, M.; Willems, K.; de Roda-Husman, A.M.; Von Bonsdorff, C.H.; Bellou, M.; Hernandez, M.; Maunula, L. Occurrence of human enteric viruses in commercial mussels at retail level in three European countries. Food Environ. Virol. 2012, 4, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Crossan, C.; Baker, P.J.; Craft, J.; Takeuchi, Y.; Dalton, H.R.; Scobie, L. Hepatitis E virus genotype 3 in shellfish, United Kingdom. Emerg. Infect. Dis. 2012, 18, 2085–2087. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.J.; Jeong, H.J.; Kim, Y.J.; Lee, S.W.; Lee, J.B.; Park, S.Y.; Song, C.S.; Park, H.M.; Choi, I.S. Analysis of complete genome sequences of swine hepatitis E virus and possible risk factors for transmission of to humans in Korea. J. Med. Virol. 2010, 82, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Li, T.C.; Miyamura, T.; Takeda, N. Detection of hepatitis E virus RNA from the bivalve Yamato-Shijimi (Corbicula japonica) in Japan. Am. J. Trop. Med. Hyg. 2007, 76, 170–172. [Google Scholar] [PubMed]
- Ijaz, S.; Arnold, E.; Banks, M.; Bendall, R.P.; Cramp, M.E.; Cunningham, R.; Dalton, H.R.; Harrison, T.J.; Hill, S.F.; Macfarlane, L.; et al. Non-travel-associated hepatitis E in England and Wales: Demographic, clinical, and molecular epidemiological characteristics. J. Infect. Dis. 2005, 192, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Cacopardo, B.; Russo, R.; Preiser, W.; Benanti, F.; Brancati, G.; Nunnari, A. Acute hepatitis E in Catania (Eastern Sicily) 1980–1994. The role of hepatitis E virus. Infection 1997, 25, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Renou, C.; Moreau, X.; Pariente, A.; Cadranel, J.F.; Maringe, E.; Morin, T.; Causse, X.; Payen, J.L.; Izopet, J.; Nicand, E.; et al. A national survey of acute hepatitis E in France. Aliment. Pharmacol. Ther. 2008, 27, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Said, B.; Ijaz, S.; Kafatos, G.; Booth, L.; Thomas, H.L.; Walsh, A.; Ramsay, M.; Morgan, D.; Hepatitis, E.I.I.T. Hepatitis E outbreak on cruise ship. Emerg. Infect. Dis. 2009, 15, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Shukla, P.; Chauhan, U.K.; Naik, S.; Anderson, D.; Aggarwal, R. Hepatitis E virus infection among animals in Northern India: An unlikely source of human disease. J. Viral Hepat. 2007, 14, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Arankalle, V.A.; Chobe, L.P.; Joshi, M.V.; Chadha, M.S.; Kundu, B.; Walimbe, A.M. Human and swine hepatitis E viruses from Western India belong to different genotypes. J. Hepatol. 2002, 36, 417–425. [Google Scholar] [CrossRef]
- Rasche, A.; Saqib, M.; Liljander, A.M.; Bornstein, S.; Zohaib, A.; Renneker, S.; Steinhagen, K.; Wernery, R.; Younan, M.; Gluecks, I.; et al. Hepatitis E virus infection in dromedaries, North and East Africa, United Arab Emirates, and Pakistan, 1983–2015. Emerg. Infect. Dis. 2016, 22, 1249–1252. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.; Cao, X.Y.; Liu, C.B.; Wang, G.M. Epidemiology of hepatitis E in China. Gastroenterol. Jpn. 1991, 26 (Suppl. S3), 135–138. [Google Scholar] [PubMed]
- Aye, T.T.; Uchida, T.; Ma, X.Z.; Iida, F.; Shikata, T.; Zhuang, H.; Win, K.M. Complete nucleotide sequence of a hepatitis E virus isolated from the Xinjiang Epidemic (1986–1988) of China. Nucleic Acids Res. 1992, 20, 3512. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Dong, C.; Zhou, Z.; Liang, J.; Dong, M.; Yang, Y.; Fu, J.; Tian, H.; Wang, S.; Fan, J.; et al. Hepatitis E virus genotype 4, Nanjing, China, 2001–2011. Emerg. Infect. Dis. 2013, 19, 1528–1530. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Kamili, S.; Yattoo, G.N. Hepatitis E virus infection may be transmitted through blood transfusions in an endemic area. J. Gastroenterol. Hepatol. 2004, 19, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Matsubayashi, K.; Nagaoka, Y.; Sakata, H.; Sato, S.; Fukai, K.; Kato, T.; Takahashi, K.; Mishiro, S.; Imai, M.; Takeda, N.; et al. Transfusion-transmitted hepatitis E caused by apparently indigenous hepatitis E virus strain in Hokkaido, Japan. Transfusion 2004, 44, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Suzuki, H.; Toyota, T.; Takahashi, M.; Okamoto, H. Three male patients with sporadic acute hepatitis E in Sendai, Japan, who were domestically infected with hepatitis E virus of genotype iii or iv. J. Gastroenterol. 2004, 39, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Matsubayashi, K.; Kang, J.H.; Sakata, H.; Takahashi, K.; Shindo, M.; Kato, M.; Sato, S.; Kato, T.; Nishimori, H.; Tsuji, K.; et al. A case of transfusion-transmitted hepatitis E caused by blood from a donor infected with hepatitis E virus via zoonotic food-borne route. Transfusion 2008, 48, 1368–1375. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, P.E.; Ijaz, S.; Brailsford, S.R.; Brett, R.; Dicks, S.; Haywood, B.; Kennedy, I.T.; Kitchen, A.; Patel, P.; Poh, J.; et al. Hepatitis E virus in blood components: A prevalence and transmission study in Southeast England. Lancet 2014, 384, 1766–1773. [Google Scholar] [CrossRef]
- Aggarwal, R. Hepatitis E: Is it a blood-borne pathogen? J. Gastroenterol. Hepatol. 2004, 19, 729–731. [Google Scholar] [CrossRef] [PubMed]
- Arankalle, V.A.; Chobe, L.P. Retrospective analysis of blood transfusion recipients: Evidence for post-transfusion hepatitis E. Vox Sang. 2000, 79, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Arankalle, V.A.; Chobe, L.P. Hepatitis E virus: Can it be transmitted parenterally? J. Viral Hepat. 1999, 6, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, S.; Sunaga, J.; Saito, N.; Fujimura, K.; Itoh, Y.; Sasaki, M.; Tsuda, F.; Takahashi, M.; Nishizawa, T.; Okamoto, H. Prevalence of antibodies to hepatitis E virus among Japanese blood donors: Identification of three blood donors infected with a genotype 3 hepatitis E virus. J. Med. Virol. 2004, 73, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, T.; Diekmann, J.; Johne, R.; Eberhardt, M.; Knabbe, C.; Dreier, J. Novel approach for detection of hepatitis E virus infection in German blood donors. J. Clin. Microbiol. 2012, 50, 2708–2713. [Google Scholar] [CrossRef] [PubMed]
- Holm, D.K.; Moessner, B.K.; Engle, R.E.; Zaaijer, H.L.; Georgsen, J.; Purcell, R.H.; Christensen, P.B. Declining prevalence of hepatitis E antibodies among Danish blood donors. Transfusion 2015, 55, 1662–1667. [Google Scholar] [CrossRef] [PubMed]
- Juhl, D.; Baylis, S.A.; Blumel, J.; Gorg, S.; Hennig, H. Seroprevalence and incidence of hepatitis E virus infection in German blood donors. Transfusion 2014, 54, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Gotanda, Y.; Iwata, A.; Ohnuma, H.; Yoshikawa, A.; Mizoguchi, H.; Endo, K.; Takahashi, M.; Okamoto, H. Ongoing subclinical infection of hepatitis E virus among blood donors with an elevated alanine aminotransferase level in Japan. J. Med. Virol. 2007, 79, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.; Li, J.; Yuan, Z.A.; Hu, J.Y.; Yu, Y.; Lu, Y.H. The development of a combined mathematical model to forecast the incidence of hepatitis E in Shanghai, China. BMC Infect. Dis. 2013, 13, 421. [Google Scholar] [CrossRef] [PubMed]
- Hogema, B.M.; Molier, M.; Slot, E.; Zaaijer, H.L. Past and present of hepatitis E in The Netherlands. Transfusion 2014, 54, 3092–3096. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.; Hofmann, M.; Danzer, M.; Hofer, K.; Kaar, J.; Gabriel, C. Seroprevalence and incidence of hepatitis E in blood donors in upper Austria. PLoS ONE 2015, 10, e0119576. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Kamili, S.; Khuroo, M.S. Clinical course and duration of viremia in vertically transmitted hepatitis E virus (HEV) infection in babies born to HEV-infected mothers. J. Viral Hepat. 2009, 16, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Mohanty, A.; Joshi, Y.K.; Deka, D.; Mohanty, S.; Panda, S.K. Mother-to-child transmission of hepatitis E virus infection. Indian J. Pediatr. 2003, 70, 37–39. [Google Scholar] [CrossRef] [PubMed]
- Bose, P.D.; Das, B.C.; Hazam, R.K.; Kumar, A.; Medhi, S.; Kar, P. Evidence of extrahepatic replication of hepatitis E virus in human placenta. J. Gen. Virol. 2014, 95, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S. Association of severity of hepatitis E virus infection in the mother and vertically transmitted infection in the fetus. JK-Practitioner 2006, 13, 70–74. [Google Scholar]
- Kumar, A.; Beniwal, M.; Kar, P.; Sharma, J.B.; Murthy, N.S. Hepatitis E in pregnancy. Int. J. Gynaecol. Obstet. 2004, 85, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Chibber, R.M.; Usmani, M.A.; Al-Sibai, M.H. Should HEV infected mothers breast feed? Arch. Gynecol. Obstet. 2004, 270, 15–20. [Google Scholar] [CrossRef] [PubMed]
- El Sayed Zaki, M.; El Aal, A.A.; Badawy, A.; El-Deeb, D.R.; El-Kheir, N.Y. Clinicolaboratory study of mother-to-neonate transmission of hepatitis E virus in Egypt. Am. J. Clin. Pathol. 2013, 140, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Ayoola, E.A.; Want, M.A.; Gadour, M.O.; Al-Hazmi, M.H.; Hamza, M.K. Hepatitis E virus infection in haemodialysis patients: A case-control study in Saudi Arabia. J. Med. Virol. 2002, 66, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Hosseini-Moghaddam, S.M.; Zarei, A.; Alavian, S.M.; Mansouri, M. Hepatitis E virus infection: A general review with a focus on hemodialysis and kidney transplant patients. Am. J. Nephrol. 2010, 31, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Sylvan, S.P.; Jacobson, S.H.; Christenson, B. Prevalence of antibodies to hepatitis E virus among hemodialysis patients in Sweden. J. Med. Virol. 1998, 54, 38–43. [Google Scholar] [CrossRef]
- Ucar, E.; Cetin, M.; Kuvandik, C.; Helvaci, M.R.; Gullu, M.; Huzmeli, C. Hepatitis E virus seropositivity in hemodialysis patients in Hatay Province, Turkey. Mikrobiyoloji Bulteni 2009, 43, 299–302. [Google Scholar] [PubMed]
- Siddiqui, A.R.; Jooma, R.A.; Smego, R.A., Jr. Nosocomial outbreak of hepatitis E infection in Pakistan with possible parenteral transmission. Clin. Infect. Dis. 2005, 40, 908–909. [Google Scholar] [CrossRef] [PubMed]
- Ola, S.O.; Odaibo, G.N.; Olaleye, O.D.; Ayoola, E.A. Hepatitis B and E viral infections among Nigerian healthcare workers. Afr. J. Med. Med. Sci. 2012, 41, 387–391. [Google Scholar] [PubMed]
- Robson, S.C.; Adams, S.; Brink, N.; Woodruff, B.; Bradley, D. Hospital outbreak of hepatitis E. Lancet 1992, 339, 1424–1425. [Google Scholar] [CrossRef]
- Balayan, M.S.; Fedorova, O.E.; Mikhailov, M.I.; Rytick, P.G.; Eremin, V.F.; Danilova, T.I.; Shevelev, B.I.; Gorbacheva, E.C.; Pankova, G.Y. Antibody to hepatitis E virus in HIV-infected individuals and aids patients. J. Viral Hepat. 1997, 4, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Christensen, P.B.; Engle, R.E.; Jacobsen, S.E.; Krarup, H.B.; Georgsen, J.; Purcell, R.H. High prevalence of hepatitis E antibodies among Danish prisoners and drug users. J. Med. Virol. 2002, 66, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Keane, F.; Gompels, M.; Bendall, R.; Drayton, R.; Jennings, L.; Black, J.; Baragwanath, G.; Lin, N.; Henley, W.; Ngui, S.L.; et al. Hepatitis E virus coinfection in patients with HIV infection. HIV Med. 2012, 13, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Pawlotsky, J.M.; Belec, L.; Gresenguet, G.; Deforges, L.; Bouvier, M.; Duval, J.; Dhumeaux, D. High prevalence of hepatitis B, C, and E markers in young sexually active adults from the Central African Republic. J. Med. Virol. 1995, 46, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Montella, F.; Rezza, G.; Di Sora, F.; Pezzotti, P.; Recchia, O. Association between hepatitis E virus and HIV infection in homosexual men. Lancet 1994, 344, 1433. [Google Scholar] [CrossRef]
- Rivero-Juarez, A.; Frias, M.; Rodriguez-Cano, D.; Cuenca-Lopez, F.; Rivero, A.I. Isolation of hepatitis E virus from breast milk during acute infection. Clin. Infect. Dis. 2016, 62, 1464. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Li, Y.; Yu, W.; Jing, S.; Wang, J.; Long, F.; He, Z.; Yang, C.; Bi, Y.; Cao, W.; et al. Excretion of infectious hepatitis E virus into milk in cows imposes high risks of zoonosis. Hepatology 2016, 64, 350–359. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Gulmarg Kashmir Epidemic, 1978–1979. Weekly occurrence of 20,083 hepatitis E cases reported from 200 villages (n = 600,000) from 4 September 1978 to 29 April 1979 (34 weeks). Epidemic curve lasted from the 8th to the 17th week (nine weeks). Prior to and following the epidemic, only isolated cases of hepatitis E were recorded, suggesting that person-to-person transmission was not of major consequence to the development of the epidemic.
Figure 1.
Gulmarg Kashmir Epidemic, 1978–1979. Weekly occurrence of 20,083 hepatitis E cases reported from 200 villages (n = 600,000) from 4 September 1978 to 29 April 1979 (34 weeks). Epidemic curve lasted from the 8th to the 17th week (nine weeks). Prior to and following the epidemic, only isolated cases of hepatitis E were recorded, suggesting that person-to-person transmission was not of major consequence to the development of the epidemic.

Figure 2.
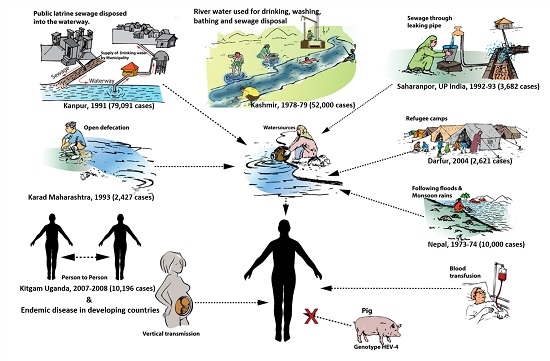
Modes of transmission of hepatitis E in developing countries. The settings for contamination of drinking water have been drawn in sketches, with epidemics reported in each case.
Figure 2.
Modes of transmission of hepatitis E in developing countries. The settings for contamination of drinking water have been drawn in sketches, with epidemics reported in each case.
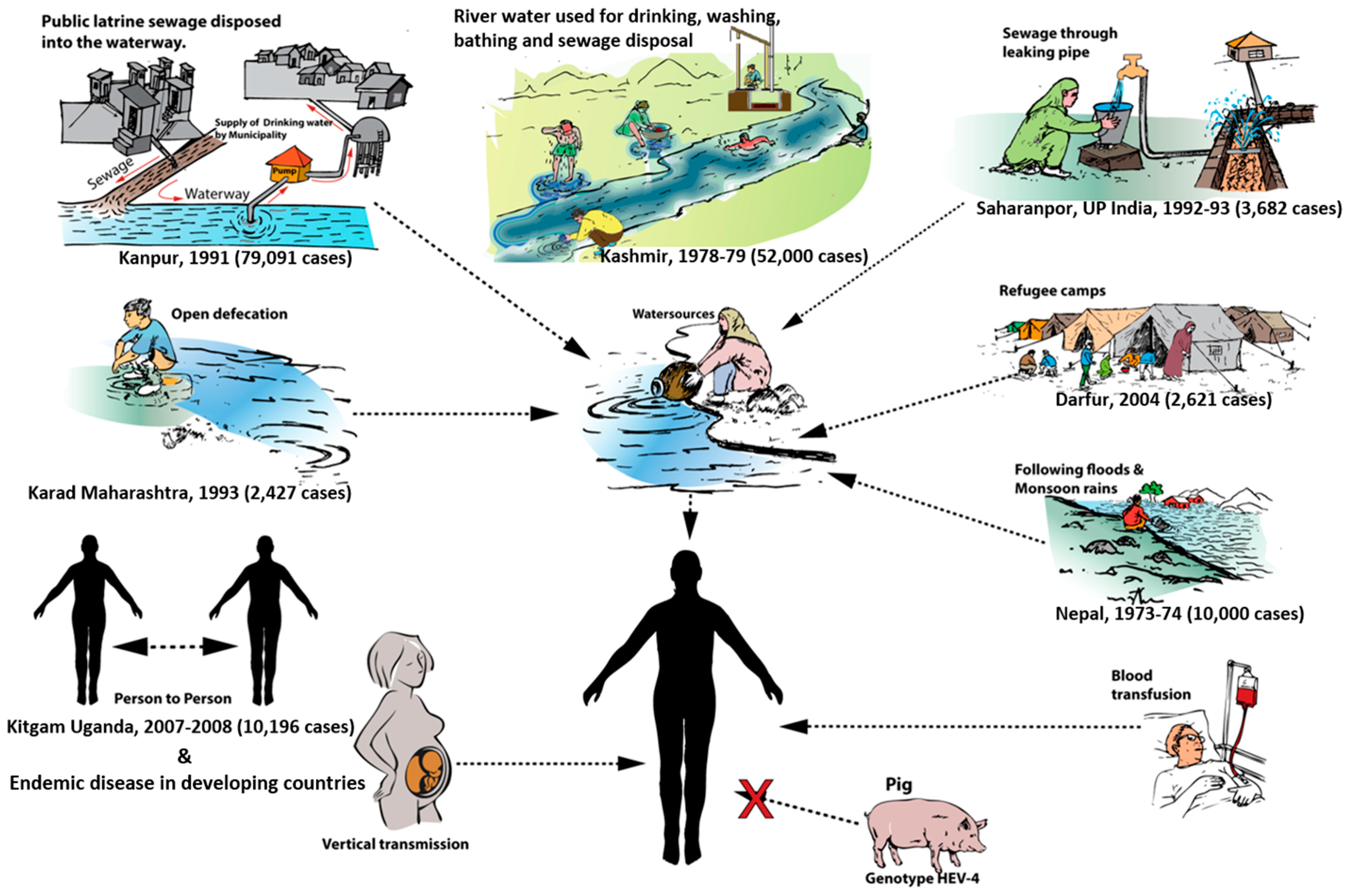
Figure 3.
Epidemic region: Kashmir, 1978. Drinking water is collected from a canal in which public latrine sewage flows, garbage of the whole locality is dumped, utensils and linen are washed, children swim, and locals buy fish (Adapted from Khuroo, et al. [4]).
Figure 3.
Epidemic region: Kashmir, 1978. Drinking water is collected from a canal in which public latrine sewage flows, garbage of the whole locality is dumped, utensils and linen are washed, children swim, and locals buy fish (Adapted from Khuroo, et al. [4]).

Figure 4.
Suggested model of repeated hepatitis E epidemics in hyperendemic areas. IgG anti-Hepatitis E virus (anti-HEV) positivity in the general population is around 4%. Following the epidemic, around 20% are sero-positive. There is a general decline in sero-positivity of IgG anti-HEV and poor exposure to HEV infections during the inter-epidemic period. Repeat outbreaks occur when sero-positivity is around 4% and there is gross fecal contamination of drinking water sources (Adapted from Khuroo, et al. [4]).
Figure 4.
Suggested model of repeated hepatitis E epidemics in hyperendemic areas. IgG anti-Hepatitis E virus (anti-HEV) positivity in the general population is around 4%. Following the epidemic, around 20% are sero-positive. There is a general decline in sero-positivity of IgG anti-HEV and poor exposure to HEV infections during the inter-epidemic period. Repeat outbreaks occur when sero-positivity is around 4% and there is gross fecal contamination of drinking water sources (Adapted from Khuroo, et al. [4]).
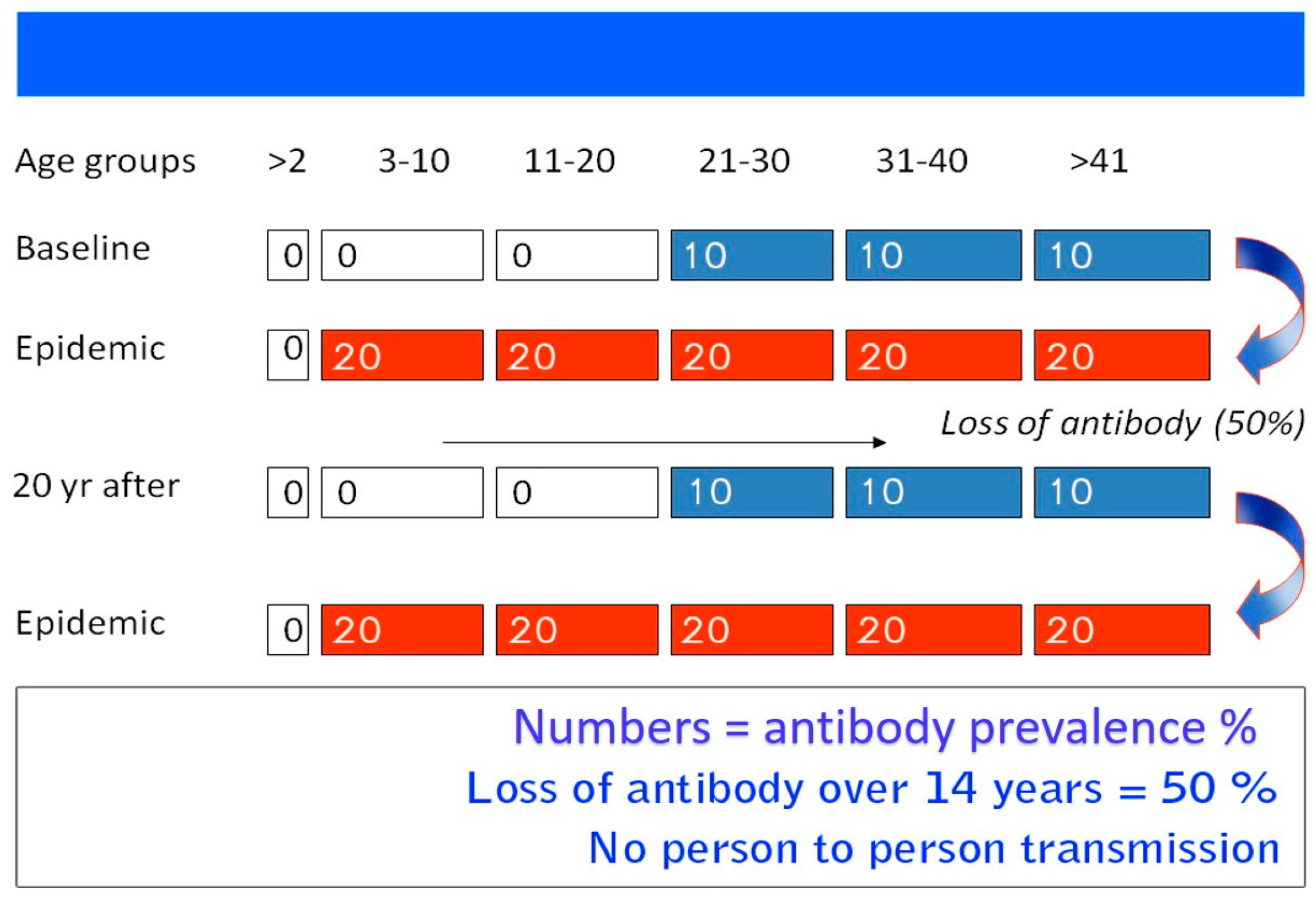
Figure 5.
Zoonotic transmission of hepatitis E in developed and many developing countries.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Place | Year | Population Exposed | Icteric Cases | Deaths |
|---|---|---|---|---|
| Gulmarg | 1978–1979 | 600,000 | 20,083 | 600 |
| Sopore | 1979–1980 | 200,000 | 6000 | 200 |
| Handwara | 1980–1981 | 400,000 | 11,500 | 400 |
| Jammu Army Camp | 1981–1982 | 845 | 206 | 0 |
| Kupwara | 1981–1982 | 500,000 | 15,000 | 550 |
| Jammu | 1983–1984 | 176,833 | 518 | 2 |
| Pinglina | 1993–1994 | 10,000 | 156 | 2 |
| Shopian | 1994–1995 | 60,000 | 1500 | 17 |
| Maharajpora, Sopore | 2007–2008 | 720 | 21 | 2 |
| Pattan, Gulmarg | 2012–2013 | 20,000 | 600 | 2 |
| Total | 1978–2013 | 1,968,398 | 55,563 | 1775 |
| Reference | Region | HEV RNA (%) | HEV Infected Transfusion vs. Total Donations |
|---|---|---|---|
| Arankalle et al., 2000 [120] | Pune India | 3/200 (1.5%) | 1:67 |
| Khuroo et al., 2004 [114] | Kashmir India | 4/107 (3.7%) | 1:27 |
| Gotanda et al., 2007 [126] | Japan | 9/6700 (0.13%) | 1:745 |
| Ren et al., 2013 [127] | China | 6/10,741 (0.06%) | 1:1790 |
| Juhl et al., 2014 [125] | Germany | 35/23,500 (0.14%) | 1:671 |
| Hewitt et al., 2014 [118] | England | 79/225,000 (0.04%) | 1:2848 |
| Hogema et al., 2014 [128] | Netherlands | 20/35,220 (0.06%) | 1:1761 |
| Fischer et al., 2015 [129] | Austria | 7/58,915 (0.01%) | 1:8416 |
Infectious dose required for HEV infection seems to be low. Duration of viremia in asymptomatic donors does not exceed 45 days (Adopted from Khuroo, et al. [1]).
| Reference | Region | Mothers | Vertical Transmission (%) | Deaths |
|---|---|---|---|---|
| Khuroo, et al., 1995 [14] | Kashmir, India | 8 | 6 (75%) | 3 (50%) |
| Kumar, et al., 2001 [50] | Al-Khobar, KSA | 26 | 26 (100%) | 2 (7.7%) |
| Kumar, et al., 2004 [134] | New Delhi, India | 18 | 6 (33.3%) | - |
| Singh, et al., 2003 [131] | New Delhi, India | 6 | 3 (50%) | - |
| Chibber, et al., 2004 * [135] | Al-Khobar, KSA | 6 | 4 (66.6%) | - |
| Khuroo, et al., 2009 [130] | Kashmir, India | 19 | 15 (78.9%) | - |
| Zaki, et al., 2013 [136] | Mansoura, Egypt | 9 | 6 (66.6%) | - |
* All 57 HEV-infected mothers had low levels of HEV RNA in the colostrum.
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Khuroo, M.S.; Khuroo, M.S.; Khuroo, N.S. Transmission of Hepatitis E Virus in Developing Countries. Viruses 2016, 8, 253. https://doi.org/10.3390/v8090253
AMA Style
Khuroo MS, Khuroo MS, Khuroo NS. Transmission of Hepatitis E Virus in Developing Countries. Viruses. 2016; 8(9):253. https://doi.org/10.3390/v8090253
Chicago/Turabian StyleKhuroo, Mohammad S., Mehnaaz S. Khuroo, and Naira S. Khuroo. 2016. "Transmission of Hepatitis E Virus in Developing Countries" Viruses 8, no. 9: 253. https://doi.org/10.3390/v8090253
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.