
A Parallel-Arm Randomized Controlled Trial to Assess the Effects of a Far-Infrared-Emitting Collar on Neck Disorder

Abstract
:1. Introduction
2. Results and Discussion
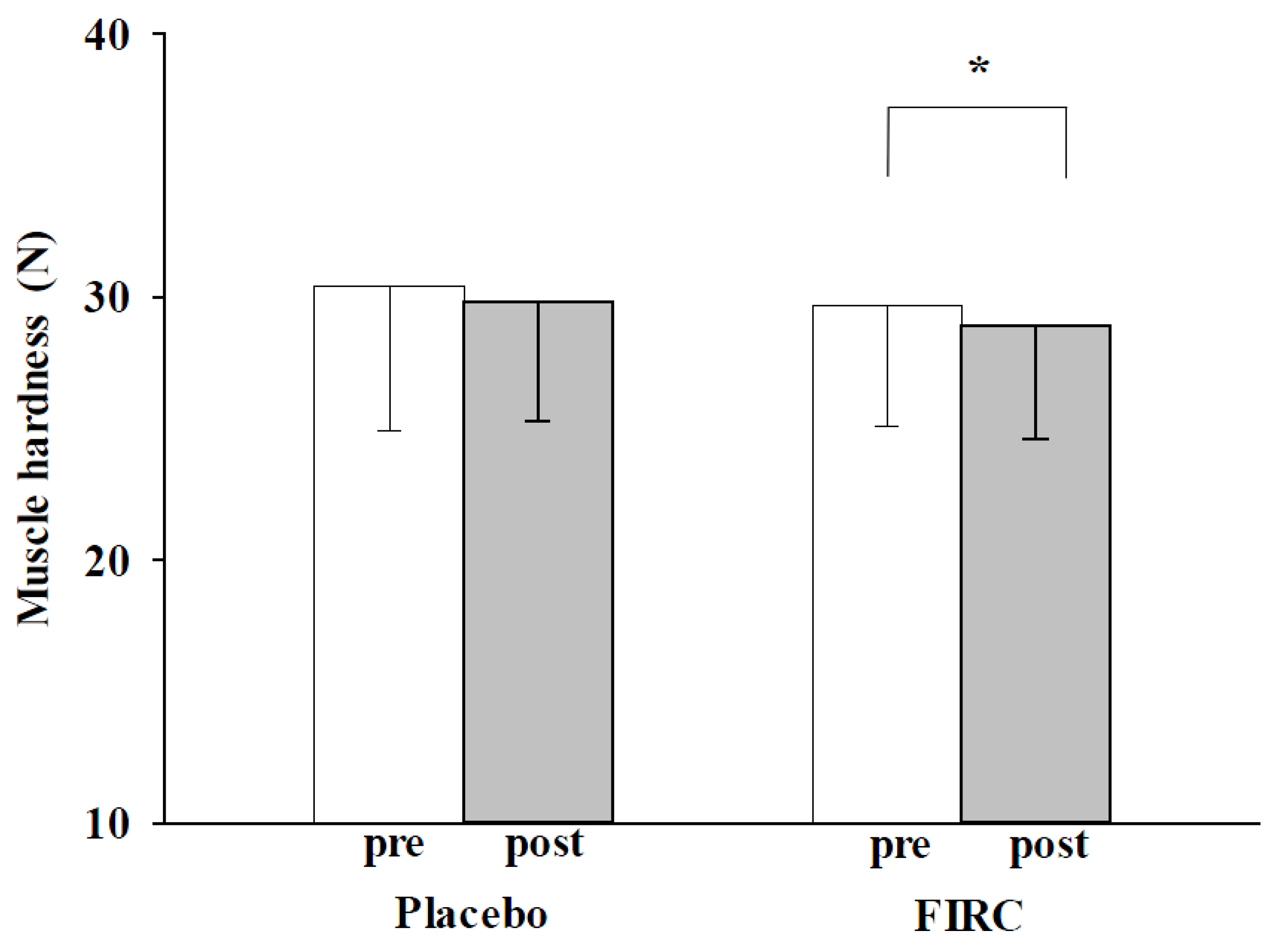
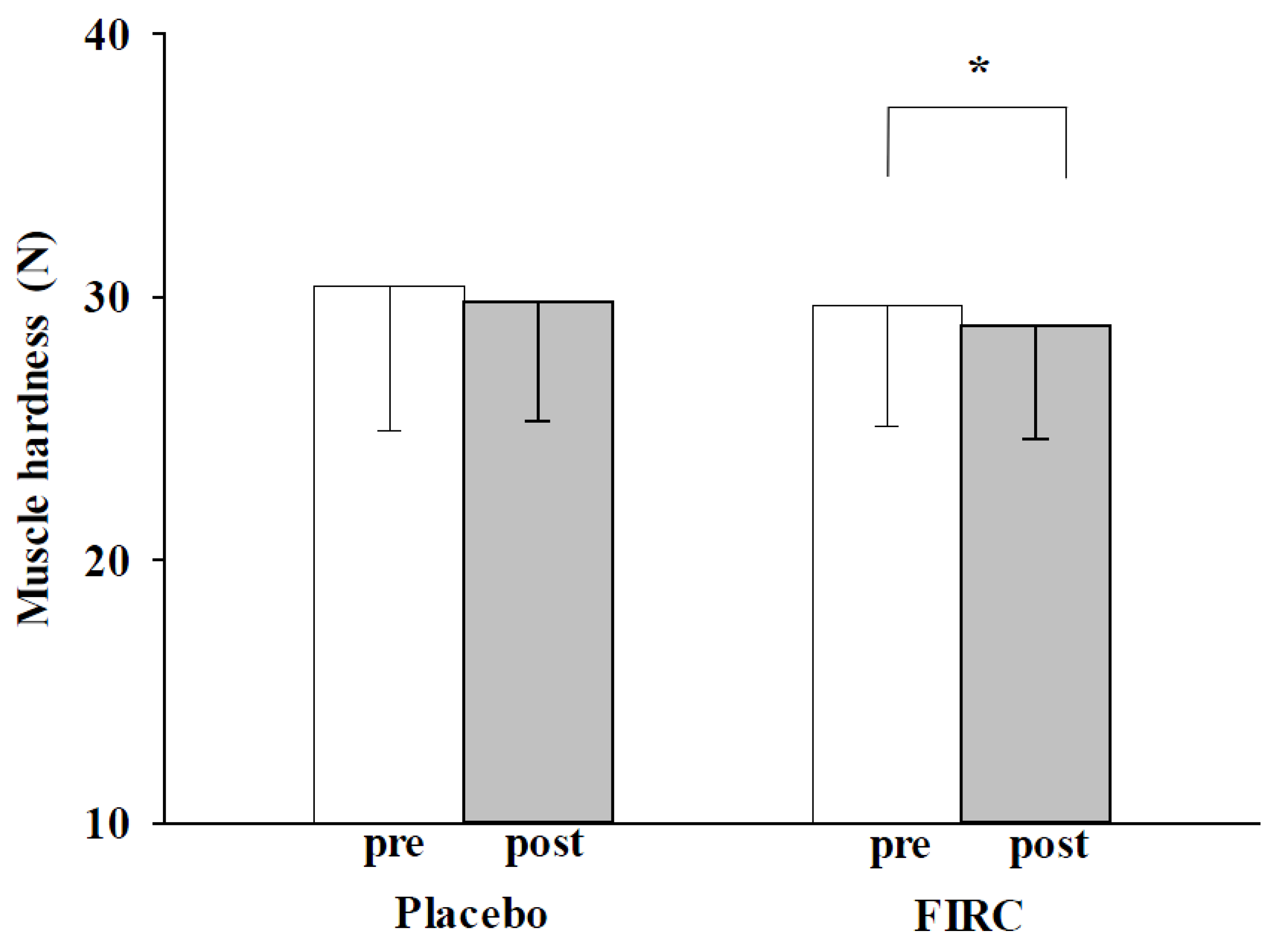
2.1. Muscle Hardness

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Placebo Group | FIR group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Measurement | Pre | Post | Difference (ΔP) | P Value (pre vs. post) | Pre | Post | Difference (ΔF) | P Value (pre vs. post) | P Value (ΔP vs. ΔF) | |
| Muscle hardness (N) | 30.43 ± 5.5 | 29.7 ± 4.6 | −0.7 ± 3.7 | 0.190 | 29.8 ± 4.5 | 28.9 ± 4.3 | −1.2 ± 2.8 | 0.026 * | 0.412 | |
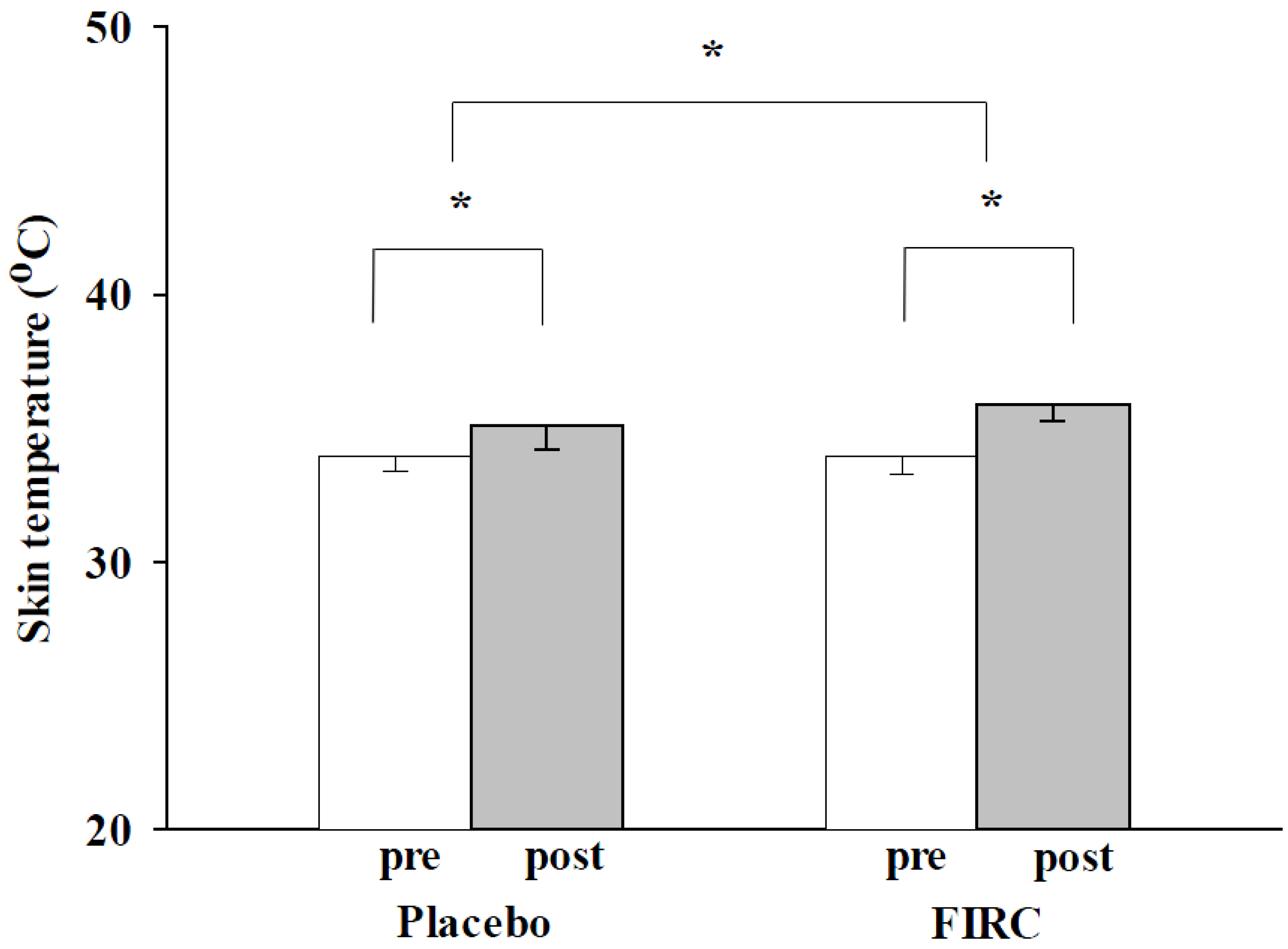
| Skin temperature (°C) | 34.0 ± 0.6 | 35.1 ± 0.9 | 1.1 ± 0.9 | 0.001 * | 34.0 ± 0.7 | 35.9 ± 0.6 | 1.8 ± 0.9 | 0.001 * | 0.003 * | |
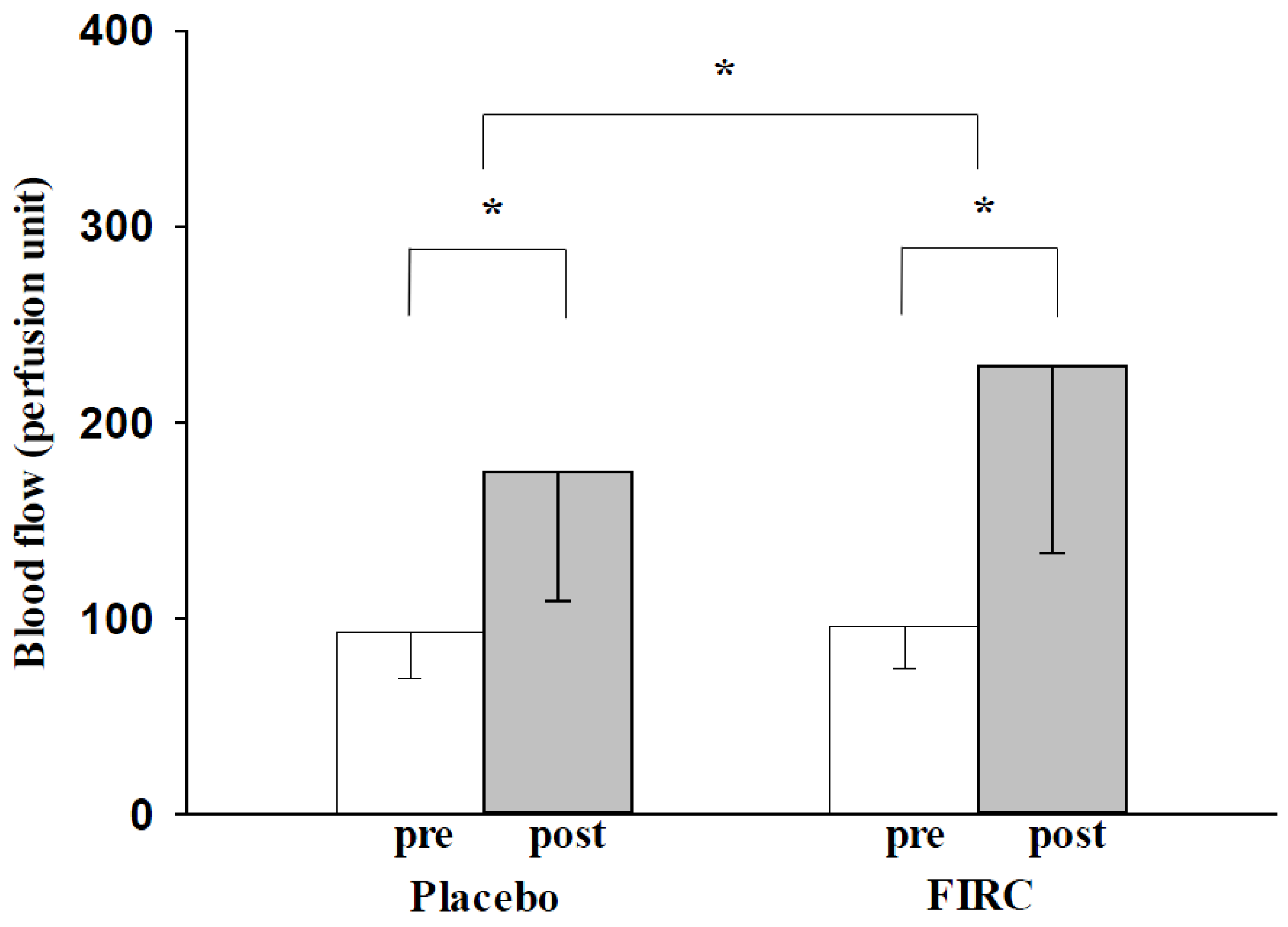
| Blood flow (PU) | 93.5 ± 23.8 | 174.4 ± 65.7 | 80.9 ± 63.0 | 0.001 * | 96.2 ± 21.3 | 228.9 ± 95.8 | 132.6 ± 96.8 | 0.001 * | 0.020 * | |
| Visual analogue scale | Pain | 3.6 ± 2.3 | 2.1 ± 1.8 | −1.5 ± 1.3 | 0.001 * | 3.8 ± 2.2 | 2.0 ± 1.9 | −1.7 ± 1.5 | 0.001 * | 0.433 |
| Anxiety | 2.8 ± 2.3 | 1.7 ± 2.1 | −1.1 ± 1.9 | 0.004 * | 3.5 ± 2.3 | 2.0 ± 1.8 | −1.8 ± 1.7 | 0.001 * | 0.077 | |
| Depression | 2.2 ± 2.2 | 1.3 ± 1.8 | −0.9 ± 1.4 | 0.002 * | 3.2 ± 2.3 | 1.7 ± 1.7 | −1.4 ± 1.6 | 0.001 * | 0.122 | |
| Fatigue | 4.6 ± 2.5 | 2.5 ± 2.1 | −2.1 ± 2.2 | 0.001 * | 5.2 ± 2.6 | 2.9 ± 2.2 | −2.4 ± 2.1 | 0.001 * | 0.615 | |
2.2. Temperature
2.3. Blood Flow

2.4. Pain, Anxiety, Depression, and Fatigue

3. Experimental Section
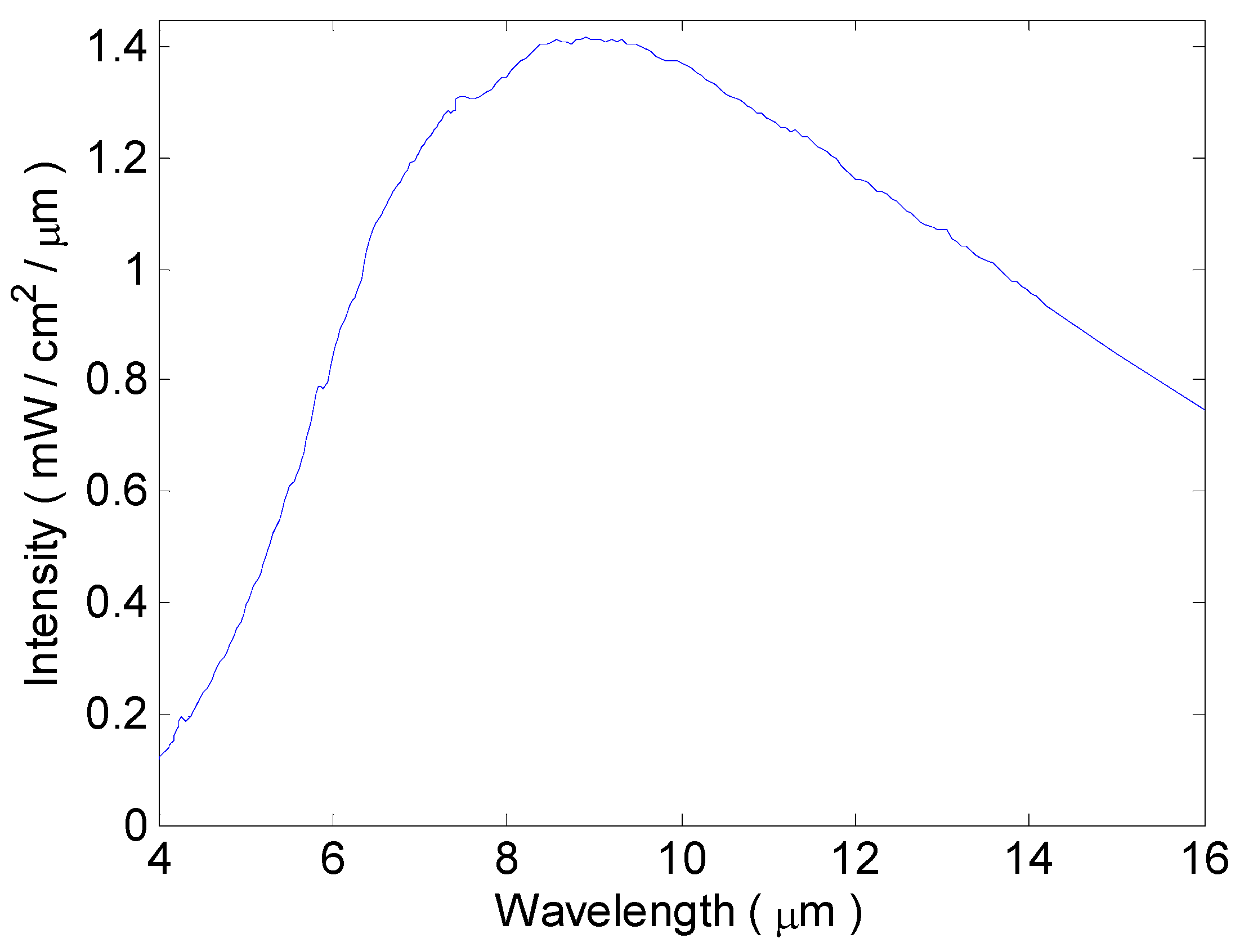
3.1. Collars of the FIRC Group and Placebo Group

3.2. Participants
3.3. Procedures
3.4. Physical Monitoring
3.5. Participant-Recorded Outcome Measures
3.6. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Yu, S.Y.; Chiu, J.H.; Yang, S.D.; Hsu, Y.C.; Lui, W.Y.; Wu, C.W. Biological effect of far infrared therapy on increasing skin microcirculation in rats. Photodermatol. Photoimmunol. Photomed. 2006, 22, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.H.; Chen, Y.C.; Chen, T.H.; Sue, Y.M.; Cheng, T.H.; Chen, J.R.; Chen, C.H. Far-infrared therapy induces the nuclear translocation of PLZF which inhibits VEGF-induced proliferation in human umbilical vein endothelial cells. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Beever, R. Far-infrared saunas for treatment of cardiovascular risk factors: Summary of published evidence. Can. Fam. Physician 2009, 55, 691–696. [Google Scholar] [PubMed]
- Ishibashi, J.; Yamashita, K.; Ishikawa, T.; Hosokawa, H.; Sumida, K.; Nagayama, M.; Kitamura, S. The effects inhibiting the proliferation of cancer cells by far-infrared radiation (FIR) are controlled by the basal expression level of heat shock protein (HSP) 70A. Med. Oncol. 2008, 25, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.F.; Hsiao, S.; Wang, S.Y. Infrared irradiation has potential antidepressant effect. Prog. Neuro-Psychoph. 2007, 31, 1397–1400. [Google Scholar] [CrossRef] [PubMed]
- Hamada, Y.; Teraoka, F.; Matsumoto, T.; Madachi, A.; Toki, F.; Uda, E.; Hase, R.; Takahashi, J.; Matsuura, N. Effects of far infrared ray on Hela cells and WI-38 cells. Int. Congr. S. 2003, 1255, 339–341. [Google Scholar] [CrossRef]
- Toyokawa, H.; Matsui, Y.; Uhara, J.; Tsuchiya, H.; Teshima, S.; Nakanishi, H.; Kwon, A.H.; Azuma, Y.; Nagaoka, T.; Ogawa, T.; et al. Promotive effects of far-infrared ray on full-thickness skin wound healing in rats. Exp. Biol. Med. 2003, 228, 724–729. [Google Scholar]
- Lee, C.H.; Roh, J.W.; Lim, C.Y.; Hong, J.H.; Lee, J.K.; Min, E.G. A multicenter, randomized, double-blind, placebo-controlled trial evaluating the efficacy and safety of a far infrared-emitting sericite belt in patients with primary dysmenorrheal. Complement. Ther. Med. 2011, 19, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Masuda, A.; Koga, Y.; Hattanmaru, M.; Minagoe, S.; Tei, C. The effects of repeated thermal therapy for patients with chronic pain. Psychother. Psychosom. 2005, 74, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Masuda, A.; Kihara, T.; Fukudome, T.; Shinsato, T.; Minagoe, S.; Tei, C. The effects of repeated thermal therapy for two patients with chronic fatigue syndrome. J. Psychosom. Res. 2005, 58, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Shimodozono, M.; Etoh, S.; Miyata, R.; Kawahira, K. Effects of thermal therapy combining sauna therapy and underwater exercise in patients with fibromyalgia. Complem. Ther. Clin. Pract. 2011, 17, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Yatsuzuka, M.; Wada, S.; Hara, Y.; Matsui, A.; Komai, N.; Yasuda, T.; Yoshii, M.; Tazawa, K. Psychological characteristics after far-infrared hyperthermia evaluated using the orofile of mood state (POMS). Jpn. J. Hyperthermic Oncol. 2005, 21, 231–236. [Google Scholar]
- Beever, R. The effects of repeated thermal therapy on quality of life in patients with type II diabetes mellitus. J. Altern. Complem. Med. 2010, 16, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Masuda, A.; Nakazato, M.; Kihara, T.; Minagoe, S.; Tei, C. Repeated thermal therapy diminishes appetite loss and subjective complaints in mildly depressed patients. Psychosom. Med. 2005, 67, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Croft, P.R.; Lewis, M.; Papageorgiou, A.C.; Thomas, E.; Jayson, M.I.; Macfarlane, G.J.; Silman, A.J. Risk factors for neck pain: A longitudinal study in the general population. Pain 2001, 93, 317–325. [Google Scholar] [CrossRef]
- Gustavsson, C.; Denison, E.; Koch, L.V. Self-management of persistent neck pain: A randomized controlled trial of a multi-component group intervention in primary health care. Eur. J. Pain 2010, 14. [Google Scholar] [CrossRef] [PubMed]
- Stahl, M.; Kautiainen, H.; El-Metwally, A.; Hakkinen, A.; Ylinen, J.; Salminen, J.J.; Mikkelsson, M. Non-specific neck pain in schoolchildren: Prognosis and risk factors for occurrence and persistence. A 4-year follow-up study. Pain 2008, 137, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Stahl, M.; Mikkelsson, M.; Kautiainen, H.; Hakkinen, A.; Ylinen, J.; Salminen, J.J. Neck pain in adolescence. A 4-year follow-up of pain-free preadolescents. Pain 2004, 110, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Von Trott, P.; Wiedemann, A.M.; Ludtke, R.; Reishauer, A.; Willich, S.N.; Witt, C.M. Qigong and exercise therapy for elderly patients with chronic neck pain (QIBANE): A randomized controlled study. Pain 2009, 10, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Misailidou, V.; Malliou, P.; Beneka, A.; Karagiannidis, A.; Godolias, G. Assessment of patients with neck pain: A review of definitions, selection criteria, and measurement tools. J. Chiropr. Med. 2010, 9, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Matsui, T.; Fujimoto, T. Treatment for depression with chronic neck pain completely cured in 94.2% of patients following neck muscle treatment. Neurosci. Med. 2011, 2, 71–77. [Google Scholar] [CrossRef]
- Rasotto, C.; Bergamin, M.; Sieverdes, J.C.; Gobbo, S.; Alberton, C.L.; Neunhaeuserer, D.; Maso, S.; Zaccaria, M.; Ermolao, A. A tailored workplace exercise program for women at risk for neck and upper limb musculoskeletal disorders: a randomized controlled trial. J. Occup. Environ. Med. 2015, 57, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Rasotto, C.; Bergamin, M.; Simonetti, A.; Maso, S.; Bartolucci, G.B.; Ermolao, A.; Zaccaria, M. Tailored exercise program reduces symptoms of upper limb work-related musculoskeletal disorders in a group of metalworkers: A randomized controlled trial. Man. Ther. 2015, 20, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Kogo, H.; Kurosawa, K. Seeking the cause of myofascial pain syndrome by identifying which manual therapy is effective against muscle tenderness and stiffness. J. Phys. Ther. Sci. 2010, 22, 173–176. [Google Scholar] [CrossRef]
- Yasui, H.; Takamoto, K.; Hori, E.; Urakawa, S.; Nagashima, Y.; Yada, Y.; Ono, T.; Nishijo, H. Significant correlation between autonomic nervous activity and cerebral hemodynamics during thermotherapy on the neck. Auton. Neurosci. 2010, 156, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Wahlstrom, J.; Hagberg, M.; Toomingas, A.; Wigaeus Tornqvist, E. Perceived muscular tension, job strain, physical exposure, and associations with neck pain among VDU users; a prospective cohort study. Occup. Environ. Med. 2004, 61, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Lauche, R.; Cramer, H.; Hohmann, C.; Choi, K.E.; Rampp, T.; Saha, F.J.; Musial, F.; Langhorst, J.; Dobos, G. The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: a randomized controlled pilot study. Evid. Based Compl. Alt. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Vas, J.; Perea-Milla, E.; Mendez, C.; Sanchez Navarro, C.; Leon Rubio, J.M.; Brioso, M.; Garcia Obrero, I. Efficacy and safety of acupuncture for chronic uncomplicated neck pain: A randomized controlled study. Pain 2006, 126, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Edmondston, S.; Bjornsdottir, G.; Palsson, T.; Solgard, H.; Ussing, K.; Allison, G. Endurance and fatigue characteristics of the neck flexor and extensor muscles during isometric tests in patients with postural neck pain. Manual Ther. 2011, 16, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Mantyselka, P.; Lupsakko, T.; Kautiainen, H.; Vanhala, M. Neck-shoulder pain and depressive symptoms: A cohort study with a 7-year follow-up. Eur. J. Pain 2010, 14, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Nagashima, Y.; Igaki, M.; Suzuki, A.; Tsuchiya, S.; Yamazaki, Y.; Hishinuma, M.; Oh-Ishi, S.; Majima, M. Application of a heat- and steam-generating sheet increases peripheral blood flow and induces parasympathetic predominance. Evid. Based Compl. Alt. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Petrofsky, J.; Paluso, D.; Anderson, D.; Swan, K.; Yim, J.E.; Murugesan, V.; Chindam, T.; Goraksh, N.; Alshammari, F.; Lee, H.; et al. The contribution of skin blood flow in warming the skin after the application of local heat; the duality of the Pennes heat equation. Med. Eng. Phys. 2011, 33, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Park, B.N.R.; Kim, S.H. The effects of heat and massage application on autonomic nervous system. Yonsei Med. J. 2011, 52, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Liau, B.Y.; Leung, T.K.; Ou, M.C.; Ho, C.K.; Yang, A.; Lin, Y.S. Inhibitory effects of far-infrared ray emitting belts on primary dysmenorrheal. Int. J. Photoener. 2012, 2012. [Google Scholar] [CrossRef]
- Hassett, A.L.; Radvanski, D.C.; Vaschillo, E.G.; Vaschillo, B.; Sigal, L.H.; Karavidas, M.K.; Buyske, S.; Lehrer, P.M. A pilot study of the efficacy of heart rate variability (HRV) biofeedback in patients with fibromyalgia. Appl. Psychophysiol. Biofeedback 2007, 32, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Yazdi, F.; Tsertsvadze, A.; Gross, A.; Van Tulder, M.; Santaguida, L.; Doucette, S. A systematic review and meta-analysis of efficacy, cost-effectiveness, and safety of selected complementary and alternative medicine for neck and low-back pain. Evid-Based Compl. Alt. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.K.; Lee, C.M.; Lin, M.Y.; Ho, Y.S.; Chen, C.S.; Wu, C.H.; Lin, Y.S. Far infrared ray irradiation induces intracellular generation of nitric oxide in breast cancer cells. J. Med. Biol. Eng. 2009, 29, 15–18. [Google Scholar]
- Leung, T.K.; Lin, Y.S.; Chen, Y.C.; Shang, H.F.; Lee, Y.H.; Su, C.H. Immunomodulatory effects of far infrared ray irradiation via increasing calmodulin and nitric oxide production in RAW 264.7 macrophages. Biomed. Eng. Appl. Basis Commun. 2009, 21, 317–323. [Google Scholar] [CrossRef]
- Leung, T.K.; Shang, H.F.; Chen, D.C.; Chen, J.Y.; Chang, T.M.; Hsiao, S.Y.; Ho, C.K.; Lin, Y.S. Effects of far infrared rays on hydrogen peroxide-scavenging capacity. Biomed. Eng. Appl. Basis Commun. 2011, 23, 99–105. [Google Scholar] [CrossRef]
- Leung, T.K.; Lin, Y.S.; Lee, C.M.; Chen, Y.C.; Shang, H.F.; Hsiao, S.Y.; Chang, H.T.; Chao, J.S. Direct and indirect effects of ceramic far infrared radiation on the hydrogen peroxide-scavenging capacity and on murine macrophages under oxidative stress. J. Med. Biol. Eng. 2011, 31, 345–351. [Google Scholar] [CrossRef]
- Ke, Y.M.; Ou, M.C.; Ho, C.K.; Lin, Y.S.; Liu, H.Y.; Chang, W.A. Effects of somatothermal far-infrared ray on primary dysmenorrhea: A pilot study. Evid. Based Compl. Alt. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.K.; Chan, C.F.; Lai, P.S.; Yang, C.H.; Hsu, C.Y.; Lin, Y.S. Inhibitory effects of far-infrared irradiation generated by ceramic material on murine melanoma cell growth. Int. J. Photoenergy 2012, 2012. [Google Scholar] [CrossRef]
- Johnston, V.; Souvlis, T.; Jimmieson, N.L.; Jull, G. Associations between individual and workplace risk factors for self-reported neck pain and disability among female office workers. Appl. Ergon. 2008, 39, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Howell, E.R. The association between neck pain, the Neck Disability Index and cervical ranges of motion: A narrative review. J. Can. Chiropr. Assoc. 2011, 55, 211–221. [Google Scholar] [PubMed]
- MacDermid, J.C.; Walton, D.M.; Avery, S.; Blanchard, A.; Etruw, E.; McAlpine, C.; Goldsmith, C.H. Measurement properties of the neck disability index: A systematic review. J. Orthop. Sport. Phys. 2009, 39, 400–417. [Google Scholar] [CrossRef] [PubMed]
- Yonezu, T.; Kogure, S. The effect of low-level laser irradiation on muscle tension and hardness compared among three wavelengths. Laser Ther. 2013, 22, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Damijan, Z.; Uhrynski, A. The influence of driver’s working environment on thermical changes of their organism. Acta Phys. Pol. A 2010, 118, 35–40. [Google Scholar]
- Jia, L.Y.; Yao, A.H.; Kuang, F.; Zhang, Y.K.; Shen, X.F.; Ju, G. Beneficial effect of the traditional chinese drug Shu-Xue-Tong on recovery of spinal cord injury in the rat. Evid. Based Compl. Alt. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the visual analog scale for measurement of acute pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, T.; Balsa, A.; Sainz, D.M.; Zamorano, E.; Gonzales, I.; Martin-Mola, E. Spanish version of the Northwick Park neck pain questionnaire: Reliability and validity. Clin. Exp. Rheumatol. 2001, 19, 41–46. [Google Scholar] [PubMed]
- Wainner, R.S.; Fritz, J.M.; Boninger, M.; Irrgang, J.J.; Delitto, T.; Allison, S.C. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine 2003, 28, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Bicer, A.; Yazici, A.; Camdeviren, H.; Erdogan, C. Assessment of pain and disability in patients with chronic neck pain: Reliability and construct validity of the Turkish version of the neck pain and disability scale. Disabil. Rehabil. 2004, 26, 959–962. [Google Scholar] [CrossRef] [PubMed]
- Wlodyka-Demaille, S.; Poiraudeau, S.; Catanzariti, J.F.; Rannou, F.; Fermanian, J.; Revel, M. The ability to change of three questionnaires for neck pain. Spine 2004, 71, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Nordin, M.; Carragee, E.; Hogg-Johnson, S.; Weiner, S.S.; Hurwitz, E.L.; Peloso, P.M.; Guzman, J.; van der Velde, G.; Carroll, L.J.; Holm, L.W.; et al. Assessment of neck pain and its associated disorders: Results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. Spine 2008, 33, S101–S122. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.L.; Bershadsky, B.; Rockwood, T.; Saleh, K.; Islam, N.C. Visual Analog Scale pain reporting was standardized. J. Clin. Epidemiol. 2005, 58, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Ou, M.C.; Lee, Y.F.; Li, C.C.; Wu, S.K. The effectiveness of essential oils for patients with neck pain: A randomized controlled study. J. Altern. Complem. Med. 2014, 20, 771–779. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-S.; Hung, K.-S.; Liau, B.-Y.; Yang, C.-H.; Yang, A.; Huang, K.-S. A Parallel-Arm Randomized Controlled Trial to Assess the Effects of a Far-Infrared-Emitting Collar on Neck Disorder. Materials 2015, 8, 5862-5876. https://doi.org/10.3390/ma8095279
Lin Y-S, Hung K-S, Liau B-Y, Yang C-H, Yang A, Huang K-S. A Parallel-Arm Randomized Controlled Trial to Assess the Effects of a Far-Infrared-Emitting Collar on Neck Disorder. Materials. 2015; 8(9):5862-5876. https://doi.org/10.3390/ma8095279
Chicago/Turabian StyleLin, Yung-Sheng, Kuo-Sheng Hung, Ben-Yi Liau, Chih-Hui Yang, Aiga Yang, and Keng-Shiang Huang. 2015. "A Parallel-Arm Randomized Controlled Trial to Assess the Effects of a Far-Infrared-Emitting Collar on Neck Disorder" Materials 8, no. 9: 5862-5876. https://doi.org/10.3390/ma8095279