Differential Exposure to Hazardous Air Pollution in the United States: A Multilevel Analysis of Urbanization and Neighborhood Socioeconomic Deprivation

Abstract
:1. Introduction
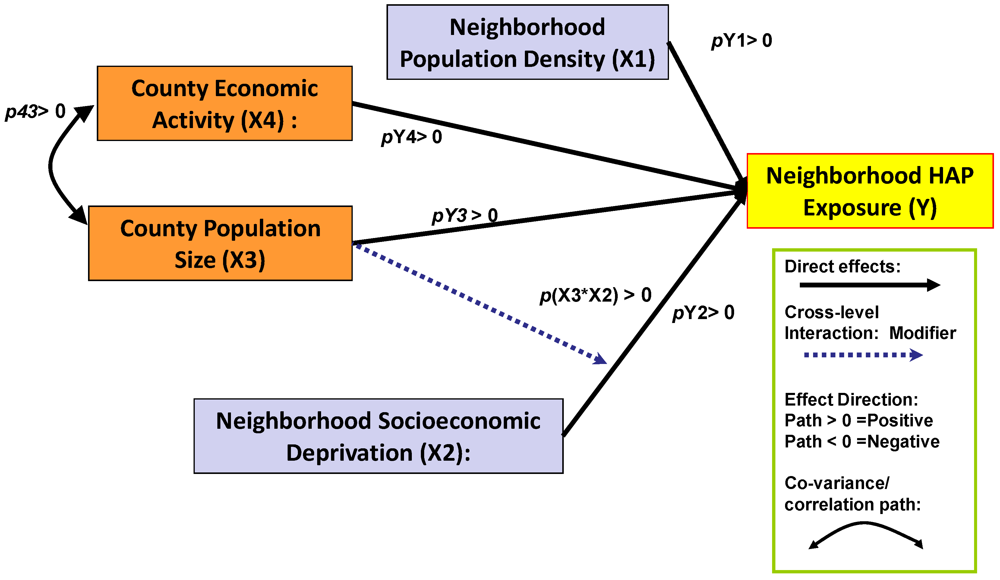
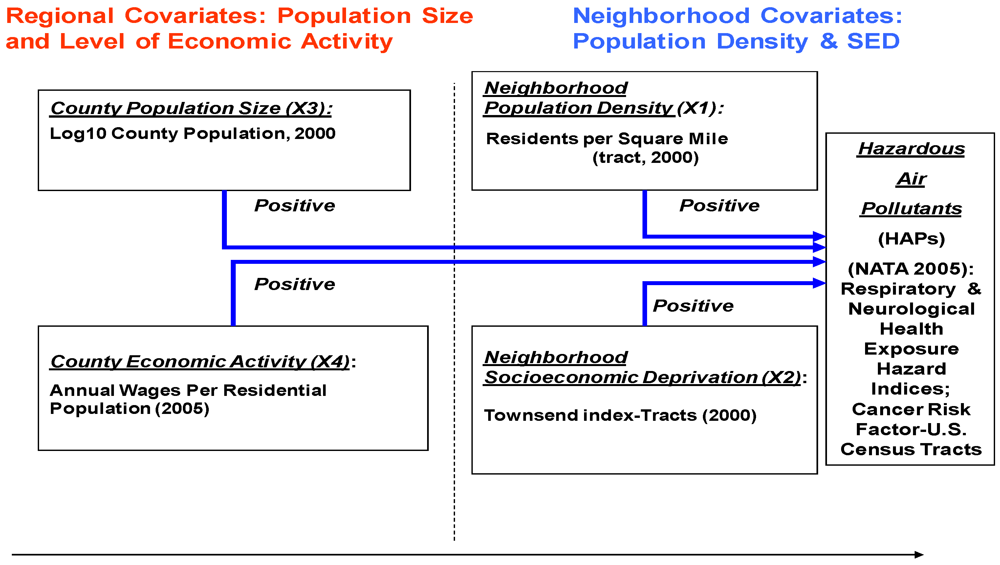
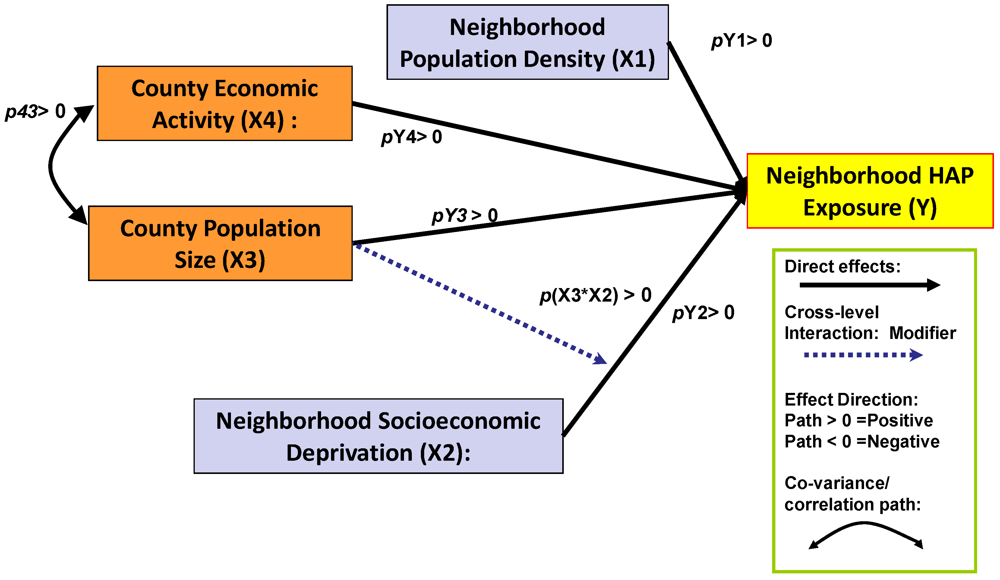
- Hypothesis 1: The greater the population size and level of regional economic activity, the higher the level of HAP exposure hazard in the region.
- Hypothesis 2: The greater the population size and level of regional economic activity, the higher the level of socioeconomic deprivation among the local neighborhoods.
- Hypothesis 3: The higher the level of neighborhood socioeconomic deprivation, the higher the level of HAP exposure, after adjustment for population size and level of economic activity.
2. Research Design and Methods

2.1. Assessment of HAP Exposure
2.2. Measurement of Socioeconomic Deprivation
- Unemployment as a percentage of those aged 16 and over who are economically active.
- Households without access to a car (car lease or ownership), as a percentage of all households.
- Residential household renting, as a percentage of all households.
- Percentage of households with “crowded housing,” i.e., the number of residents exceeds the number of rooms within the household.
2.3. Measures of Urbanization and Economic Activity
2.4. Multilevel Statistical Modeling
3. Results
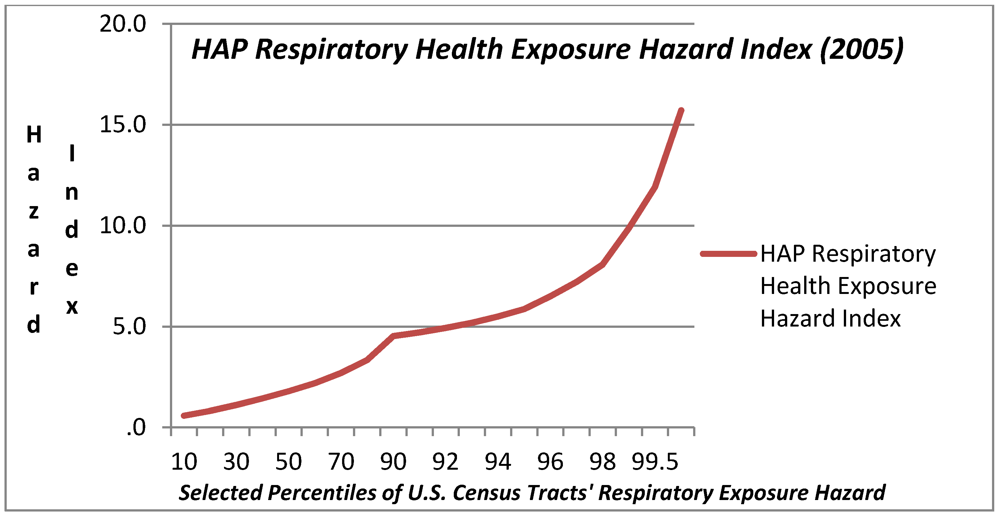
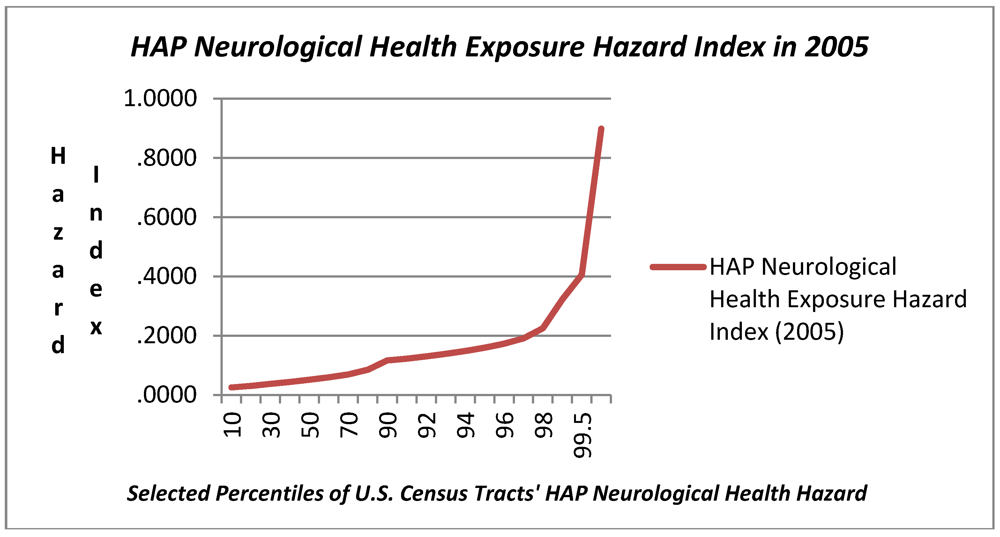
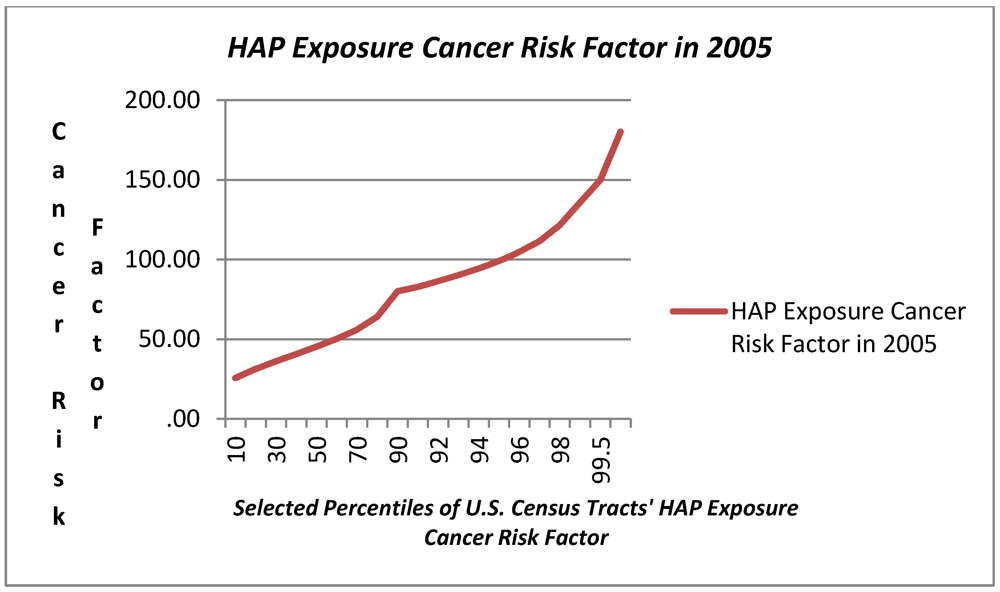
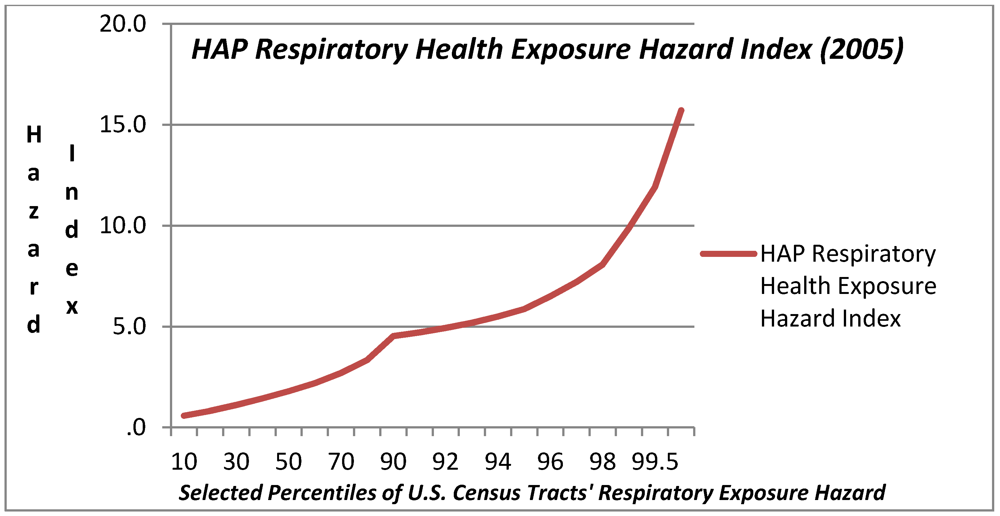
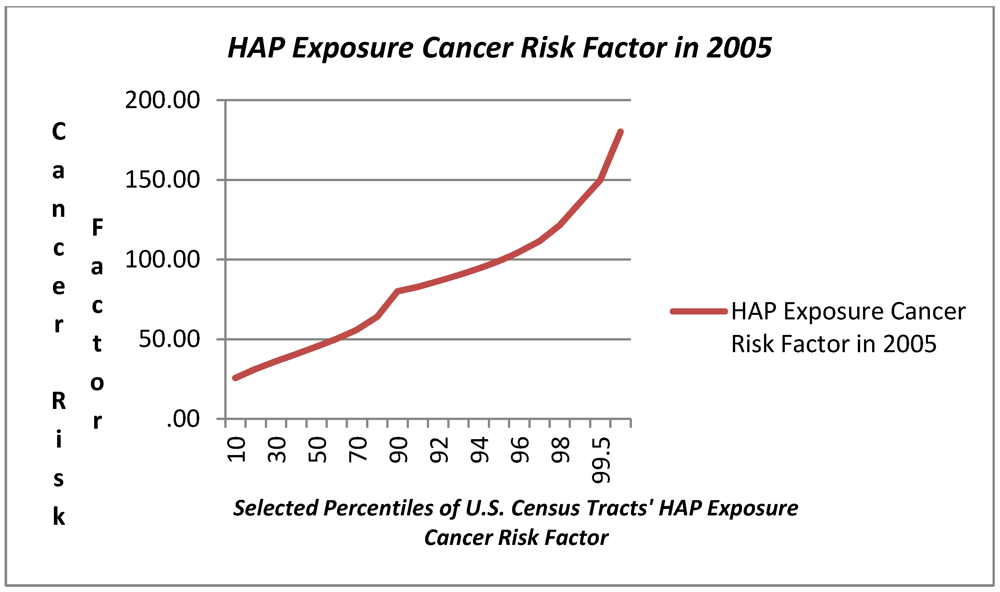
3.1. Variation in HAP Exposure Risk

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tract-Level Descriptive Statistics (N = 64,524) | Mean | Std. Dev. | Percentiles | ||||
|---|---|---|---|---|---|---|---|
| 5th | 25th | 50th | 75th | 99th | |||
| Population Size of Tracts’ Host County [000s] | 1,049.71 | 1,906.97 | 16.87 | 95.79 | 401.61 | 1,003.16 | 9,937.74 |
| Density per Sq Mile Census Tract | 5,215.51 | 11,997.51 | 17.04 | 234.18 | 1,981.92 | 5,204.29 | 61,564.29 |
| Townsend Index-Tract | (0.00) | 3.08 | (3.06) | (2.11) | (0.99) | 1.14 | 10.90 |
| Number Employed in County, 2005 [000s] | 436.19 | 763.05 | 3.78 | 32.03 | 163.77 | 473.59 | 3,805.77 |
| Aggregate Wage Payroll (2005) [$000] | 19,016 | 34,796 | 97 | 955 | 5,861 | 18,893 | 162,202 |
| Avg. Wages per Employee in County 2005 [$000] | 36.05 | 9.42 | 23.51 | 29.26 | 34.97 | 40.81 | 66.37 |
| County-Level Descriptive Statistics (N = 3,138) | Mean | Std. Dev. | 5th | 25th | 50th | 75th | 99th |
| Population Size of Tracts’ Host County [000s] | 934.99 | 3,047.51 | 29.95 | 112.28 | 251.11 | 636.22 | 11,745.13 |
| Number Employed in County, 2005 [000s] | 364.03 | 1,330.98 | 4.77 | 21.69 | 65.36 | 195.73 | 5,507.85 |
| Aggregate Wage Payroll (2005) [$000] | 14,063 | 64,340 | 104 | 524 | 1,728 | 5,784 | 233,483 |
| Avg. Wages per Employee in County, 2005 [$000] | 27.71 | 6.90 | 19.26 | 23.44 | 26.64 | 30.63 | 50.26 |
| Tract-Level Outcomes: | Mean | Std. Dev. | 5th | 25th | 50th | 75th | 99th |
| Respiratory Health Hazard (2005) | 2.30 | 1.96 | 0.44 | 0.96 | 1.80 | 2.99 | 9.87 |
| Neurological Health Hazard (2005) | 0.07 | 0.10 | 0.02 | 0.03 | 0.05 | 0.08 | 0.32 |
| Cancer Risks per MM Population (2005) | 50.11 | 24.38 | 21.32 | 33.89 | 45.39 | 59.56 | 135.79 |

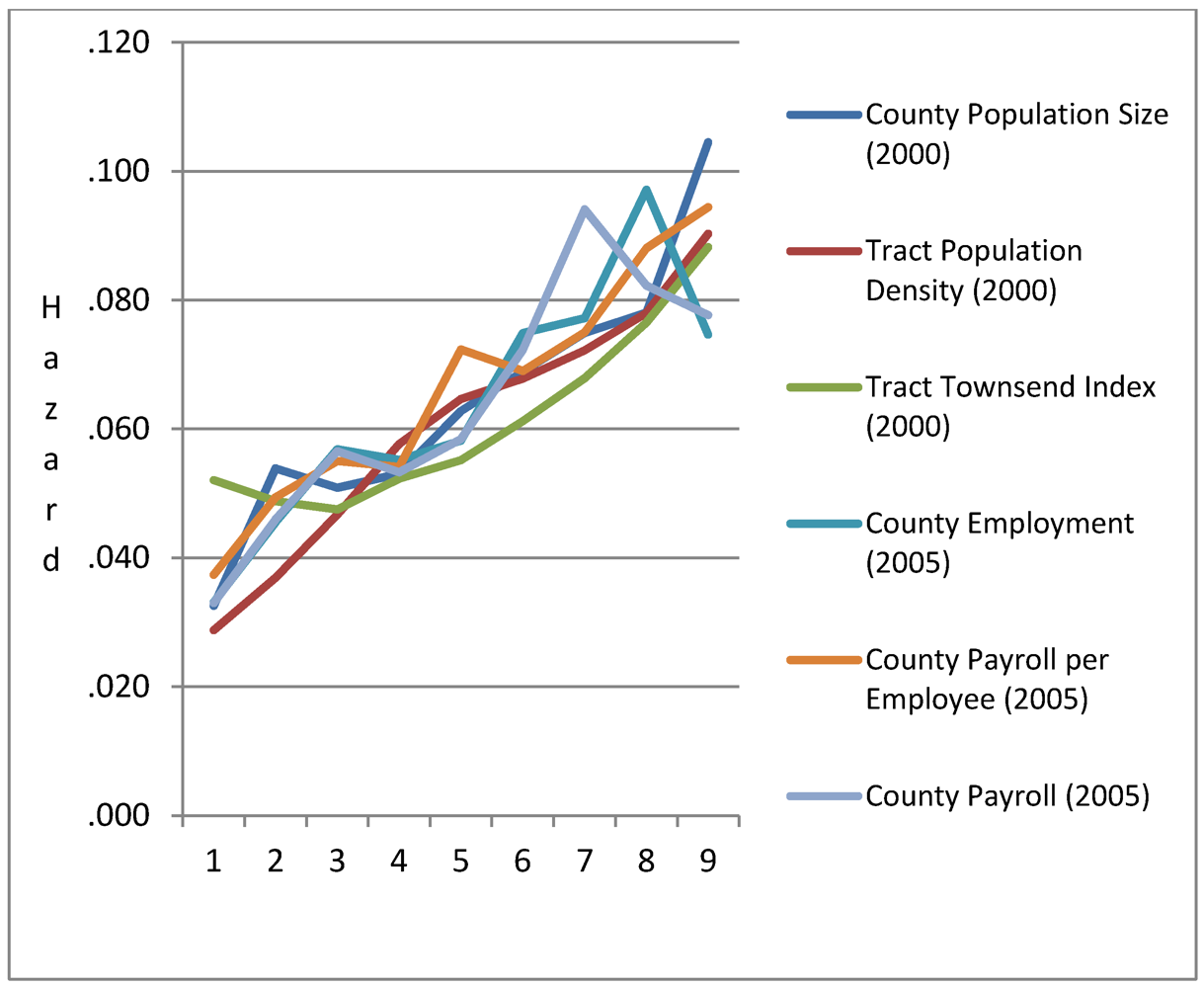
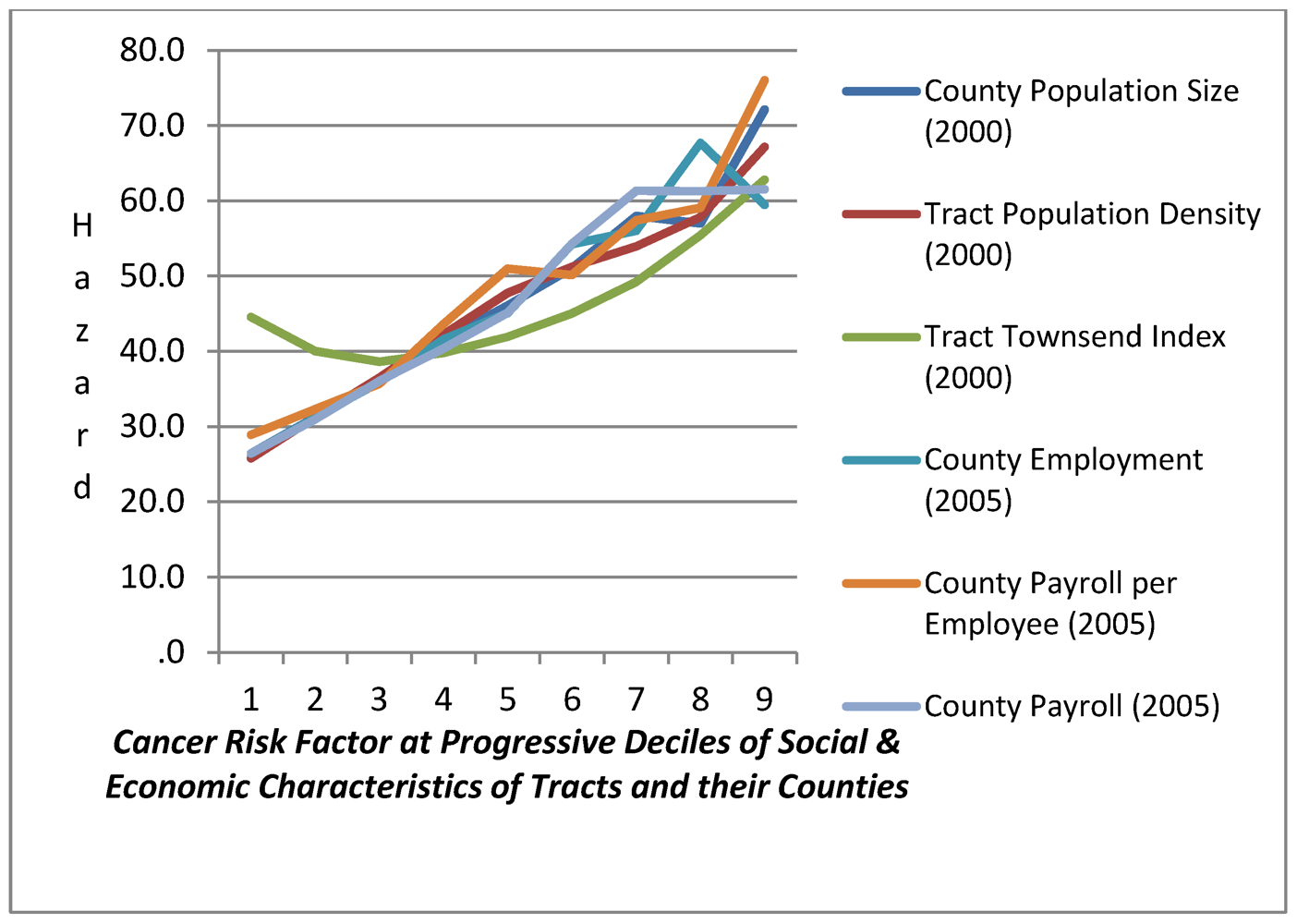
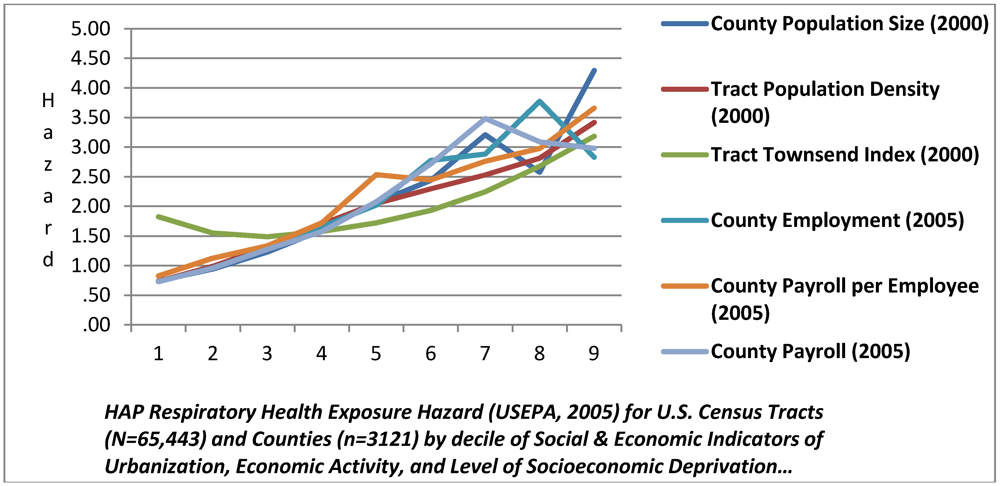
3.2. HAP Chemical Exposure Hazard by Urbanization and Economic Activity
| HAP Health Hazard Metrics | Ratio of HAP Exposure Risk at Selected Percentiles to Risk at 20th Percentile | County Population Size (2000) | Tract Population Density (2000) | Tract Townsend Index | County Employment (2005) | County Payroll per Employee (2005) |
|---|---|---|---|---|---|---|
| Respiratory Health Exposure Hazard | Ratio 80/20 | 2.73 | 2.85 | 1.73 | 3.93 | 2.65 |
| Ratio 95/20 | 2.81 | 4.51 | 2.94 | 4.39 | 3.23 | |
| Ratio 97/20 | 5.63 | 6.3 | 3.56 | 5.52 | 3.64 | |
| Neurological Health Exposure Hazard | Ratio 80/20 | 1.45 | 2.11 | 1.57 | 2.13 | 1.78 |
| Ratio 95/20 | 2.18 | 3.29 | 2.59 | 3.25 | 1.84 | |
| Ratio 97/20 | 1.91 | 4.21 | 2.82 | 2.26 | 1.76 | |
| Cancer Risk Factor | Ratio 80/20 | 1.82 | 1.85 | 1.38 | 2.17 | 1.83 |
| Ratio 95/20 | 1.99 | 2.63 | 2.01 | 2.48 | 2.11 | |
| Ratio 97/20 | 3.48 | 3.08 | 2.32 | 3.49 | 2.11 |
3.3. Differential HAP Exposure Related to Neighborhood SED: Multilevel Model Estimates
| HAP Exposure Hazards | Respiratory | Neurological | Cancer |
|---|---|---|---|
| Tract Population Density (Log 10 Density/Sq M) | 0.385 *** | 0.0121 *** | 5.797 *** |
| −0.00538 | −0.00057 | −0.0687 | |
| Townsend Index-Tract | 0.0905 *** | 0.00312 *** | 1.185 *** |
| −0.00138 | −0.000146 | −0.0176 | |
| County Population (2000) Log 10 | 0.247 *** | 0.00353 | 5.947 *** |
| −0.031 | −0.00334 | −0.297 | |
| Annual Wage per Employee in Tract’s County ’05 | 0.0170 *** | 0.000331 | 0.308 *** |
| −0.0026 | −0.00028 | −0.0247 | |
| Cross-level Tract SED & County Population Size | 0.0138 *** | −2.94 × 10−6 | 0.510 *** |
| −0.00079 | −8.41 × 10−5 | −0.0102 | |
| New England Region | 0.357 *** | −0.00992 | 1.792 * |
| −0.11 | −0.0118 | −0.983 | |
| Mid-Atlantic Region | −0.0684 | 0.00163 | 3.617 *** |
| −0.0823 | −0.00887 | −0.746 | |
| East North Central | −0.207 *** | 0.0132 * | 3.057 *** |
| −0.0633 | −0.00682 | −0.59 | |
| West North Central | −0.0189 | 0.000438 | 4.110 *** |
| −0.0609 | −0.00655 | −0.58 | |
| South Atlantic | 0.567 *** | −0.00275 | 10.68 *** |
| −0.0607 | −0.00653 | −0.57 | |
| East South Central | 0.166 ** | 0.0217 *** | 12.37 *** |
| −0.0657 | −0.00707 | −0.618 | |
| West South Central | −0.0179 | −0.00828 | 8.470 *** |
| −0.063 | −0.00678 | −0.595 | |
| Pacific Region | 0.854 *** | −0.00184 | 4.812 *** |
| −0.0812 | −0.00874 | −0.749 | |
| Constant | −1.372 *** | −0.00616 | −21.31 *** |
| West Region-Intercept | −0.127 | −0.0136 | −1.21 |
| Model Fit Statistics: | |||
| ll_0 | −85,224 | 67,237 | −252,964 |
| ll | −76,808 | 68,045 | −240,725 |
| df_m | 13 | 13 | 13 |
| Number Counties | 3,119 | 3,119 | 3,119 |
| rho | 0.485 | 0.494 | 0.294 |
| sigma_e | 0.755 | 0.08 | 9.706 |
| sigma_u | 0.733 | 0.0791 | 6.27 |
| chi2_c | 67,085 | 21,898 | 42,053 |
| ll_c | −110,351 | 57,096 | −261,752 |
| chi2 | 16,831 | 1,616 | 24,477 |
| Tract SED | Predicted HAP Exposure at 20th Percentile County Population Size | Predicted HAP Exposure at 80th Percentile County Population Size | Predicted HAP Exposure at 95th Percentile County Population Size | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Percentiles: | Resp | Neuro | Cancer | Resp | Neuro | Cancer | Resp | Neuro | Cancer |
| 20th | 1.43 | 0.06 | 38.80 | 1.73 | 0.06 | 45.75 | 1.73 | 0.06 | 44.01 |
| 80th | 1.77 | 0.07 | 42.65 | 2.11 | 0.07 | 51.04 | 2.38 | 0.08 | 58.91 |
| 95th | 2.16 | 0.08 | 46.91 | 2.54 | 0.09 | 56.89 | 3.09 | 0.09 | 75.36 |
| 99th | 2.53 | 0.10 | 50.97 | 2.95 | 0.10 | 62.46 | 3.77 | 0.11 | 91.04 |
| Ratio 80/20 | 1.25 | 1.23 | 1.10 | 1.23 | 1.21 | 1.12 | 1.37 | 1.20 | 1.34 |
| Ratio 95/20 | 1.52 | 1.48 | 1.21 | 1.47 | 1.45 | 1.24 | 1.79 | 1.43 | 1.71 |
| Ratio 99/20 | 1.77 | 1.73 | 1.31 | 1.709 | 1.671 | 1.365 | 2.18 | 1.65 | 2.07 |
| Progressive excess risk associated with increased SED, for census tracts at the 95th and 80th percentile of County population size: | Case Contrast Assumptions: Mid Atlantic Region; Median Tract Population Density & County Economic Activity; and varying levels of County Population Size and Tract SED | ||||||||
| Resp | Neuro | Cancer | |||||||
| Ratio 80/20 | 1.122 | 0.993 | 1.200 | ||||||
| Ratio 95/20 | 1.214 | 0.988 | 1.377 | ||||||
| Ratio 99/20 | 1.276 | 0.985 | 1.515 | ||||||
4. Discussion
Acknowledgments
Conflict of Interest
References
- Abbey, D.; Nishino, N.; McDonnell, W.; Burchette, R.; Knutsen, S.; Beeson, L.; Yang, J. Long-term inhalable particles and other air pollutants related to mortality in non-smokers. Am. J. Respir. Crit. Care Med. 1992, 159, 373–382. [Google Scholar]
- Anderson, H.R.; Atkinson, R.W.; Bremner, S.A.; Marston, L. Particulate air pollution and hospital admissions for cardiorespiratory diseases: Are the elderly at greater risk? Eur. Pespir. J. 2003, 21, 39–46. [Google Scholar] [CrossRef]
- Bell, M.L.; Dominici, F.; Samet, J.M. A meta-analysis of time-series studies of ozone and mortality with comparison to the national morbidity, mortality, and air pollution study. Epidemiology 2005, 16, 436–445. [Google Scholar] [CrossRef]
- Bell, M.L.; Ebisu, K.; Peng, R.D.; Samet, J.M.; Dominici, F. Hospital admissions and chemical composition of fine particle air pollution. Am. J. Respir. Crit. Care Med. 2009, 179, 1115–1120. [Google Scholar] [CrossRef]
- Bell, M.L.; Ebisu, K.; Peng, R.D.; Walker, J.; Samet, J.M.; Zeger, S.L.; Dominici, F. Seasonal and regional short-term effects of fine particles on hospital admissions in 202 U.S. counties, 1999-2005. Am. J. Epidemiol. 2008, 168, 1301–1310. [Google Scholar] [CrossRef]
- Bell, M.L.; Peng, R.D.; Dominici, F.; Samet, J.M. Emergency hospital admissions for cardiovascular diseases and ambient levels of carbon monoxide: Results for 126 United States urban counties, 1999-2005. Circulation 2009, 120, 949–955. [Google Scholar] [CrossRef]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. J. Am. Med. Assoc. 2006, 295, 1127–1134. [Google Scholar]
- Dominici, F. Revised Analysis of the National Morbidity Mortality Air Pollution Study: Part II; The Health Effects Institute: Cambridge, MA, USA, 2003. [Google Scholar]
- Dominici, F.; McDermott, A.; Daniels, M.; Zeger, S.L.; Samet, J.M. Revised analyses of the national morbidity, mortality, and air pollution study: Mortality among residents of 90 cities. J. Toxicol. Environ. Health Part A 2005, 68, 1071–1092. [Google Scholar] [CrossRef]
- Dominici, F.; McDermott, A.; Zeger, S.L.; Samet, J.M. National maps of the effects of particulate matter on mortality: Exploring geographical variation. Environ. Health Perspect. 2003, 111, 39–44. [Google Scholar]
- Eftim, S.E.; Samet, J.M.; Janes, H.; McDermott, A.; Dominici, F. Fine particulate matter and mortality: A comparison of the six cities and American Cancer Society cohorts with a Medicare cohort. Epidemiology 2008, 19, 209–216. [Google Scholar] [CrossRef]
- Peng, R.D.; Chang, H.H.; Bell, M.L.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Coarse particulate matter air pollution and hospital admissions for cardiovascular and respiratory diseases among Medicare patients. J. Am. Med. Assoc. 2008, 299, 2172–2179. [Google Scholar]
- Samet, J.M.; Dominici, F.; Curriero, F.; Coursac, I.; Zeger, S.L. Fine particulate air pollution and mortality in 20 U.S. cities: 1987-1994. N. Engl. J. Med. 2000, 343, 1742–1757. [Google Scholar] [CrossRef]
- Samoli, E.; Peng, R.; Ramsay, T.; Pipikou, M.; Touloumi, G.; Dominici, F.; Burnett, R.; Cohen, A.; Krewski, D.; Samet, J.; Katsouyanni, K. Acute effects of ambient particulate matter on mortality in Europe and North America: Results. Environ. Health Perspect. 2008, 116, 1480–1486. [Google Scholar]
- Zeger, S.L.; Dominici, F.; McDermott, A.; Samet, J.M. Mortality in the Medicare population and chronic exposure to fine particulate air pollution in urban centers (2000-2005). Environ. Health Perspect. 2008, 116, 1614–1619. [Google Scholar] [CrossRef]
- Gauderman, J.A.; Vora, H.; McConnell, R.; Berhane, K.; Gwelliland, F.; Thomas, D.; Lurmann, F.; Avol, E.; Kunzli, N.; Jerrett, M.; Peters, J. Effect of exposure to traffic on lung development from 10 to 18 years of age: A cohort study. Lancet 2007, 369, 571–577. [Google Scholar]
- Dockery, D.; Pope, C.A.; Xu, X.; Spengler, J.; Ware, J.; Fay, M.; Ferris, B.; Speizer, F. An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar]
- Pope, C.A.; Burnett, R.T.; Thruston, G.D.; Calle, E.; Thun, M.J.; Krewski, D.; Goldeski, J. Cardiovascular mortality and long-term exposure to particulate air pollution: Epidemiological evidence of general pathophysiological pathways of disease. Circulation 2003, 6, 71–77. [Google Scholar]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thruston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. J. Am. Med. Assoc. 2002, 287, 1132–1141. [Google Scholar]
- Pope, C.A.; Dockery, D.; Schwartz, J. Review of epidemiological evidence of health effects of particulate air pollution. Inhal. Toxicol. J. 1995, 47, 1–18. [Google Scholar]
- Pope, C.A.; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef]
- Pope, C.A., III; Muhlestein, J.B.; May, H.T.; Rehlund, D.G.; Anderson, J.L.; Horne, B.D. Ischemic heart disease events triggered by short-term exposure to fine particulate air pollution. Circulation 2006, 114, 2443–2448. [Google Scholar] [CrossRef]
- Pope, C.A., III.; Thun, M.J.; Namboodiri, M.M. Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar]
- Schwartz, J. Air pollution and daily mortality: A review and meta-analysis. Environ. Res. 1994, 64, 36–52. [Google Scholar] [CrossRef]
- Schwartz, J. Assessing confounding, effect modification, and thresholds in the association between ambient particles and daily deaths. Environ. Health Perspect. 2000, 108, 563–568. [Google Scholar] [CrossRef]
- Schwartz, J. Is there harvesting association of airborne particles with daily deaths and hospital admissions? Epidemiology 2001, 12, 55–61. [Google Scholar] [CrossRef]
- Schwartz, J. Lung function and chronic exposure to air pollution: A cross-sectional analysis of NHANES II. Environ. Res. 1989, 50, 309–321. [Google Scholar] [CrossRef]
- Wellenius, G.A.; Schwartz, J.; Mittleman, M. Particulate air pollution and hospital admissions for congestive heart failure in seven U.S. cities. Am. J. Cardiol. 2006, 97, 404–408. [Google Scholar] [CrossRef]
- Zanobetti, A.; Schwartz, J. Cardiovascular damage by air borne particles: Are diabetics more susceptible? Epidemiology 2002, 13, 588–592. [Google Scholar]
- Zanobetti, A.; Schwartz, J. The effect of fine and coarse particulate air pollution on mortality: A national analysis. Environ. Health Perspect. 2009, 117, 898–903. [Google Scholar] [CrossRef]
- Zanobetti, A.; Schwartz, J.; Dockery, D.W. Airborne particles are a risk factor for hospital admissions for heart and lung disease. Environ. Health Perspect. 2000, 108, 1071–1077. [Google Scholar] [CrossRef]
- Zanobetti, A.; Schwartz, J.; Gold, D. Are there sensitive subgroups for the effects of airborne particles? Environ. Health Perspect. 2000, 108, 841–845. [Google Scholar]
- Greenbaum, D.; Bachmann, J.; Krewski, D.; Samet, J.; White, R.; Wyzga, R. Particulate air pollution standards and morbidity and mortality: Case study. Am. J. Epidemiol. 2001, 154, 78–90. [Google Scholar] [CrossRef]
- Wyzga, R. Commentary on the HEI Reanalysis of the two cohort studies of particulate air pollution and mortality. J. Toxicol. Environ. Health Part A 2003, 66, 1701–1704. [Google Scholar] [CrossRef]
- U.S. EPA, Concepts, Methods, and Data Sources for Cummulative Health Risk Assesment of Multiple Chemicals, Exposures and Effects: A Resource Document (Final Report); U.S. Environmental Protection Agency: Washington, DC, USA, 2007.
- Laden, F.; Schwartz, J.; Speizer, F.E.; Dockery, D.W. Reduction in fine particulate air pollution and mortality. Extended follow-up of Harvard Six Cities Study. Am. J. Respir. Crit. Care Med. 2006, 173, 667–672. [Google Scholar]
- Fox, M.; Groopman, J.D.; Burke, T.A. Evaluating cumulative risk assessment for environmental justice: A community case-study. Environ. Health Perspect. 2002, 110, 203–209. [Google Scholar]
- Fox, M.; Tran, N.L.; Groopman, J.D.; Burke, T.A. Toxicological resources for cumulative risk: An example with hazardous air pollutants. Regul. Toxicol. Pharmacol 2004, 40, 305–311. [Google Scholar] [CrossRef]
- National Research Council, Science and Decisions: Advancing Risk Assessment; National Academies Press: Washington, DC, USA, 2008.
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and the North; Croom Helm: London, UK, 1988. [Google Scholar]
- Brown, P. Race, class and environmental health: A review and systemisation of the literature. Environ. Res. 1995, 69, 15–30. [Google Scholar] [CrossRef]
- Anderson, R.T.; Sorlie, P.; Backlund, J.N.; Kaplan, G.A. Mortality effects of community socioeconomic status. Epidemiology 1997, 8, 42–47. [Google Scholar] [CrossRef]
- Walker, G.; Mitchell, G.; Fairburn, J.; Smith, G. Industrial pollution and social deprivation: evidence and complexity in evaluating and responding to environmental inequality. Local Environ. 2005, 10, 361–377. [Google Scholar] [CrossRef] [Green Version]
- U.S. Environmental Protection Agency. 2005 National-Scale Air Toxics Assessment. March 2011. Available online: http://www.epa.gov/ttn/atw/nata2005 (accessed on 18 March 2012).
- StataCorp, Stata Statistical Software, Release 11, StataCorp LP: College Station, TX, USA, 2009.
- Bowen, W. An analytical review of environmental justice research: What do I really know? Environ. Manag. 2002, 29, 3–15. [Google Scholar] [CrossRef]
- Bard, D. Exploring the joint effect of atmospheric pollution and socioeconomic status on selected health outcomes: An overview of the PAISARC project. Environ. Res. Lett. 2007, 2. [Google Scholar]
- Gwynn, R.; Thurston, G.D. The burden of air pollution: Impacts among racial minorities environmental health perspectives. Inhaled Irrit. Allerg. 2001, 109, 501–506. [Google Scholar]
- Bellinger, D.C.; Leviton, A.; Waternaux, C.; Needleman, H.; Rabinowitz, M. Low-level lead exposure, social class, and infant development. Neurotoxicol. Teratol. 1988, 10, 497–503. [Google Scholar] [CrossRef]
- Weiss, B.; Bellinger, D.C. Social ecology of children’s vulnerability to environmental pollutants. Environ. Health Perspect. 2006, 114, 1479–1485. [Google Scholar] [CrossRef]
- Clougherty, J.E.; Levy, J.I.; Kubzansky, L.D.; Ryan, P.B.; Suglia, S.F.; Canner, M.J.; Wright, R.J. Synergistic effects of traffic-related air pollution and exposure to violence on urban asthma etiology. Environ. Health Perspect. 2007, 115, 1140–1146. [Google Scholar]
- American Lung Association. Urban air pollution and health inequities: A workshop report. Environ. Health Perspect. 2001, 109, 357–373. [CrossRef]
- Wheeler, B. Health-related environmental indices and environmental equity in England and Wales. Environ. Plan. A 2004, 36, 803–822. [Google Scholar] [CrossRef]
- Zimmerman, R. Issues of classification in environmental equity: How we manage is how we measure. Fordham Urban Law Journal 1994, 21, 633–669. [Google Scholar]
- U.S. EPA, Ensuring Risk Reduction in Communities with Multiple Stressors: Environmental Justice and Cummulative Risks/Impacts; U.S. EPA: Washington, DC, USA, 2004.
- Gee, G.C.; Payne-Sturges, D.C. Environmental health disparities: A framework integrating psychosocial and environmental concepts. Environ. Health Perspect. 2004, 112, 1645–1653. [Google Scholar]
- Diez Roux, A. The Examination of Neighborhood Effects on Health: Conceptual and Methodological Issues Related to the Presence of Multiple Levels of Organization; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Macintyre, S.; Ellaway, A. Ecological Approaches: Rediscovering the Role of Physical and Social Enviornment; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- O’Neil, M.S.; Jarret, M.; Kawachi, I.; Levy, J.I.; Cohen, A.J. Health, wealth, and air pollution: Advancing theory and methods. Environ. Health Perspect. 2003, 111, 1861–1870. [Google Scholar]
- Drukker, M.; van Os, J. Mediators of neighborhood socioeconomic deprivation and quality of life. Soc. Psychiatry Epidemiol. 2003, 38, 698–706. [Google Scholar] [CrossRef]
- Augustin, T.; Glass, T.A.; James, B.; Schwartz, B.S. Neighborhood psychosocial hazards and cardiovascular disease: The Baltimore Memory Study. Am. J. Public Health 2008, 98, 1664–1670. [Google Scholar] [CrossRef]
- Eberhardt, M.S.; Pamuk, E.R. The importance of place of residence: Examining health in rural and nonrural areas. Am. J. Public Health 2004, 94, 1682–1686. [Google Scholar] [CrossRef]
- Elreedy, S.; Krieger, N.; Ryan, P.; Sparrow, D.; Weiss, S. Relations between individual and neighborhood-based measures of socioeconomic position and bone lead concentrations among community-exposed men: The Normative Aging Study. Am. J. Epidemiol. 1999, 150, 129–141. [Google Scholar] [CrossRef]
- Geronimus, A.T. Race, Ethnicity, and Health: A Public Health Reader; Josey-Bass: San Francisco, CA, USA, 2002. [Google Scholar]
- Glass, T.A. Neighborhoods and obesity in older adults: The Baltimore Memory Study. Am. J. Prev. Med. 2006, 31, 455–463. [Google Scholar] [CrossRef]
- Glass, T.A.; Bandeen-Roche, K.; McAtee, M.; Bolla, K.; Todd, A.C.; Schwartz, B.S. The association of environmental lead exposure with cognitive function is modified by neighborhood psychosocial hazards. Am. J. Epidemiol. 2009, 169, 683–692. [Google Scholar] [CrossRef]
- Schwartz, B.S.; Glass, T.A.; Bolla, K.I.; Stewart, W.F.; Glass, G.; Rasmussen, M.; Bressler, J.; Shi, W.; Bandeen-Roche, K. Disparities in cognitive functioning by race/ethnicity in the Baltimore Memory Study. Environ. Health Perspect. 2004, 112, 314–320. [Google Scholar]
- Katsouyanni, K.; Toulomi, G.; Samoli, E.; Gryparis, A.; LeTertre, A.; Monopolis, Y.; Rossi, G.; Zmirou, D.; Ballester, F.; Boumghar, A.; Anderson, H.R. Confounding and effect modification in the short-term effects of ambient particles on total mortality: results from 29 European cities within the APHEA2 project. Epidemiology 2001, 12, 521–531. [Google Scholar] [CrossRef]
- Katsouyanni, K.; Touloumi, G.; Spix, C.; Balducci, F.; Medina, S.; Rossi, G.; Wojtyniak, B.; Sunyer, J.; Bacharova, L.; Schouten, J.; Ponka, A.; Anderson, H.R. Short term effects of ambient sulfur dioxide and particulate matter on mortality in 12 European cities: Results from time series data from the APHEA project. Br. Med. J. 1997, 314, 1658–1663. [Google Scholar]
- Janes, H.; Dominici, F.; Zeger, S.L. Trends in air pollution and mortality: An approach to the assessment of unmeasured confounding. Epidemiology 2007, 18, 416–423. [Google Scholar] [CrossRef]
- Hernan, M.A. Causal knowledge as a prerequisite for confounding evaluation: An application to birth defects epidemiology. Am. J. Epidemiol. 2002, 155, 176–184. [Google Scholar] [CrossRef]
- U.S. EPA, Supplementary Guidance for Conducting Health Risk Assesment of Chemical Mixtures; U.S. Environmental Protection Agency: Washington, DC, USA, 2000.
- U.S. EPA, Guidance on Cummulative Risk Assesment of Pesticide Chemicals That Have a Common Mechanism of Toxicity; U.S. Environmental Protection Agency: Washington, DC, USA, 2002.
- U.S. EPA, Framework for Cumulative Risk Assessment; EPA/630/P-02/001F; Risk Assessment Forum: Washington, DC, USA, 2003.
- U.S. EPA, Guidelines for Exposure Assessment; U.S. Environmental Protection Agency: Washington, DC, USA, 1992.
Appendix
| Census Division: | Counties (Pct) | Population (Pct) | Tracts (Pct) | |||
|---|---|---|---|---|---|---|
| New England | 67 | 2.1 | 14,238,888 | 4.8 | 3,203 | 4.9 |
| Middle Atlantic | 150 | 4.8 | 40,332,259 | 13.7 | 9,918 | 15.2 |
| East North Central | 437 | 13.9 | 46,031,860 | 15.7 | 11,328 | 17.4 |
| West North Central | 618 | 19.7 | 19,697,992 | 6.7 | 5,090 | 7.8 |
| South Atlantic | 589 | 18.8 | 55,182,959 | 18.8 | 10,781 | 16.5 |
| East South Central | 364 | 11.6 | 17,480,032 | 6.0 | 3,938 | 6.0 |
| West South Central | 470 | 15.0 | 33,281,974 | 11.3 | 7,104 | 10.9 |
| Mountain | 281 | 8.9 | 19,823,587 | 6.8 | 4,255 | 6.5 |
| Pacific | 165 | 5.3 | 47,610,448 | 16.2 | 9,549 | 14.7 |
| Total | 3,141 | 100.0 | 293,679,999 | 100.0 | 65,166 | 100.0 |


© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Young, G.S.; Fox, M.A.; Trush, M.; Kanarek, N.; Glass, T.A.; Curriero, F.C. Differential Exposure to Hazardous Air Pollution in the United States: A Multilevel Analysis of Urbanization and Neighborhood Socioeconomic Deprivation. Int. J. Environ. Res. Public Health 2012, 9, 2204-2225. https://doi.org/10.3390/ijerph9062204
Young GS, Fox MA, Trush M, Kanarek N, Glass TA, Curriero FC. Differential Exposure to Hazardous Air Pollution in the United States: A Multilevel Analysis of Urbanization and Neighborhood Socioeconomic Deprivation. International Journal of Environmental Research and Public Health. 2012; 9(6):2204-2225. https://doi.org/10.3390/ijerph9062204
Chicago/Turabian StyleYoung, Gary S., Mary A. Fox, Michael Trush, Norma Kanarek, Thomas A. Glass, and Frank C. Curriero. 2012. "Differential Exposure to Hazardous Air Pollution in the United States: A Multilevel Analysis of Urbanization and Neighborhood Socioeconomic Deprivation" International Journal of Environmental Research and Public Health 9, no. 6: 2204-2225. https://doi.org/10.3390/ijerph9062204