Suicide Mortality in Comparison to Traffic Accidents and Homicides as Causes of Unnatural Death. An Analysis of 14,441 Cases in Germany in the Year 2010

Abstract
:
1. Introduction
2. Material and Methods
3. Results
3.1. Overall Event Rates and Proportions

{kind=link}
{kind=link}
{kind=link}
| Men | Women | |
|---|---|---|
| Suicide rate | 18.6 | 6.1 |
| Traffic accidents rate | 7.2 | 2.5 |
| Homicide rate | 0.6 | 0.6 |
| Suicide proportion | 1.8 | 0.6 |
| Traffic accidents proportion | 0.7 | 0.2 |
| Homicide proportion | 0.06 | 0.05 |
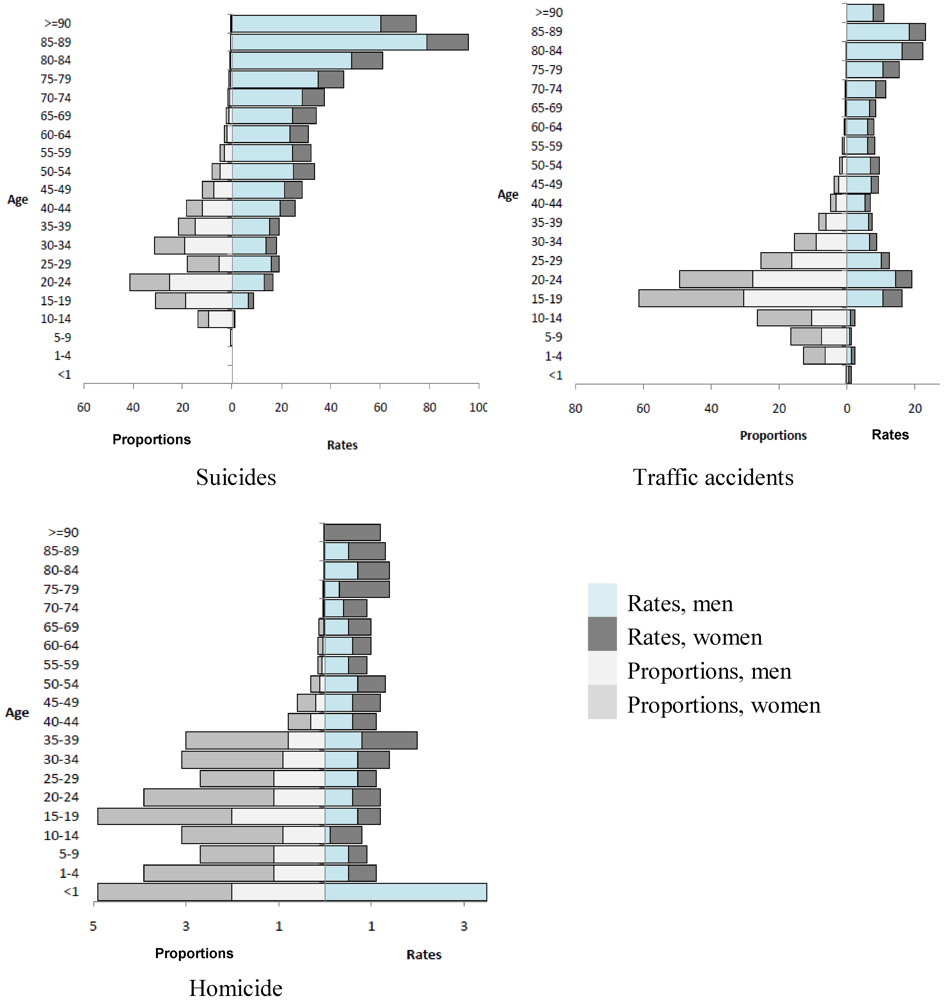
3.2. Age-Specific Event Rates and Proportions
| Age | SR | SP | TR | TP | HR | HP | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| m | w | m | w | m | w | m | w | m | w | m | w | |
| <1 | - | - | - | - | 0.6 | 0.6 | 0.2 | 0.2 | 3.5 | 1.8 | 0.9 | 0.6 |
| 1–4 | - | - | - | - | 1.2 | 0.7 | 6.5 | 6.3 | 0.5 | 0.3 | 2.7 | 1.4 |
| 5–9 | 0.1 | - | 0.6 | - | 0.7 | 1.7 | 7.5 | 9.1 | 0.5 | 0.3 | 5.2 | 3.5 |
| 10–14 | 1.0 | 0.3 | 9.5 | 4.2 | 1.1 | 1.2 | 10.4 | 16.0 | 0.1 | 0.1 | 1.4 | 1.4 |
| 15–19 | 6.6 | 2.2 | 18.8 | 12.2 | 10.7 | 5.5 | 30.5 | 30.8 | 0.7 | 0.5 | 2.0 | 2.9 |
| 20–24 | 13.1 | 3.5 | 25.3 | 16.1 | 14.3 | 4.8 | 27.8 | 21.6 | 0.6 | 0.6 | 1.1 | 2.8 |
| 25–29 | 15.8 | 3.3 | 25.1 | 13.0 | 10.2 | 2.2 | 16.2 | 9.0 | 0.7 | 0.4 | 1.1 | 1.6 |
| 30–34 | 13.9 | 4.1 | 19.0 | 12.1 | 6.7 | 2.1 | 9.2 | 6.2 | 0.7 | 0.7 | 0.9 | 2.2 |
| 35–39 | 15.3 | 3.7 | 14.8 | 7.0 | 6.3 | 1.1 | 6.1 | 2.1 | 0.8 | 1.2 | 0.8 | 2.2 |
| 40–44 | 19.6 | 5.9 | 12.1 | 6.3 | 5.4 | 1.4 | 3.3 | 1.5 | 0.6 | 0.5 | 0.3 | 0.5 |
| 45–49 | 21.1 | 7.2 | 7.4 | 4.5 | 7.2 | 2.0 | 2.5 | 1.2 | 0.6 | 0.6 | 0.2 | 0.4 |
| 50–54 | 24.8 | 8.8 | 4.9 | 3.2 | 6.9 | 2.5 | 1.4 | 0.9 | 0.7 | 0.6 | 0.1 | 0.2 |
| 55–59 | 24.5 | 7.6 | 3.0 | 2.0 | 6.1 | 2.0 | 0.8 | 0.5 | 0.5 | 0.4 | 0.06 | 0.1 |
| 60–64 | 23.6 | 7.3 | 2.0 | 1.2 | 6.1 | 1.8 | 0.5 | 0.3 | 0.6 | 0.4 | 0.05 | 0.1 |
| 65–69 | 24.4 | 9.9 | 1.3 | 1.1 | 6.6 | 1.9 | 0.4 | 0.2 | 0.5 | 0.5 | 0.03 | 0.1 |
| 70–74 | 28.3 | 9.1 | 1.0 | 0.6 | 8.4 | 2.9 | 0.3 | 0.2 | 0.4 | 0.5 | 0.02 | 0.03 |
| 75–79 | 35.0 | 10.1 | 0.7 | 0.4 | 10.5 | 4.8 | 0.2 | 0.2 | 0.3 | 1.1 | 0.01 | 0.04 |
| 80–84 | 48.5 | 12.4 | 0.6 | 0.2 | 16.2 | 6.2 | 0.2 | 0.00 | 0.7 | 0.7 | 0.01 | 0.01 |
| 85–89 | 78.9 | 16.7 | 0.6 | 0.1 | 18.2 | 4.9 | 0.1 | 0.04 | 0.5 | 0.8 | 0.00 | 0.01 |
| >=90 | 60.3 | 14.1 | 0.3 | 0.06 | 7.6 | 3.3 | 0.04 | 0.02 | - | 1.2 | - | 0.01 |
3.3. Years of Life Lost
| Suicide | Traffic accidents | Homicide | |
|---|---|---|---|
| men | 314 | 188 | 19 |
| women | 90 | 67 | 15 |
4. Discussion
5. Conclusions
Conflict of Interest
References
- Grabauskas, V.; Gaizauskiene, A.; Sauliune, S.; Miseikyte, R. Trends in avoidable mortality in Lithuania during 2001-2008 and their impact on life expectancy. Medicina (Kaunas.) 2011, 47, 504–511. [Google Scholar]
- Nolte, E.; McKee, M. Does Health Care Cave Lives? Avoidable Mortality Revisited; The Nuffield Trust: London, UK, 2004. [Google Scholar]
- Pfeiffer, C.; Windzio, M.; Kleinmann, M. Die Medien, das Böse und wir. Zu den Auswirkungen von Mediennutzung auf Kriminalitätswahrnehmung (in German). Monatsschrift für Kriminologie und Strafrechtsreform 2004, 6, 415–435. [Google Scholar]
- 4. Federal Statistical Office of Germany Home Page. Available online: http://www.gbe-bund.de (accessed on 13 March 2012).
- Aragon, T.J.; Lichtensztajn, D.Y.; Katcher, B.S.; Reiter, R.; Katz, M.H. Calculating expected years of life lost for assessing local ethnic disparities in causes of premature death. BMC Public Health 2008, 8, 116. [Google Scholar]
- Marshall, R.J. Standard expected years of life lost as a measure of mortality: Norms and reference to New Zealand data. Aust. N. Z. J. Public Health 2004, 28, 452–457. [Google Scholar]
- Lopez, A.D.; Mathers, C.; Ezzati, M.; Jamison, D.T.; Murray, C.J.L. Global Burden of Disease and Risk Factors; Oxford University Press: New York, USA, 2006. [Google Scholar]
- Statistical Analysis System SAS, version 9.2, SAS Institute Inc., 2009.
- Arato, M. The Hungarian suicide enigma. Encephale 1996, 22 Spec No 4, 25–27. [Google Scholar]
- Organisation for Economic Co-operation and Development (OECD). Health at a Glance: Europe 2010; OECD Publishing: Paris, France, 2010.
- Kivela, S.L. Relationship between suicide, homicide and accidental deaths among the aged in Finland in 1951-1979. Acta Psychiatr. Scand. 1985, 72, 155–160. [Google Scholar]
- Waller, P.F. Challenges in motor vehicle safety. Annu. Rev. Public Health 2002, 23, 93–113. [Google Scholar]
- Wintemute, G.J. From research to public policy: The prevention of motor vehicle injuries, childhood drownings, and firearm violence. Am. J. Health Promot. 1992, 6, 451–464. [Google Scholar]
- Althaus, D.; Hegerl, U. Causes, diagnosis and treatment of suicidality. Nervenarzt 2004, 75, 1123–1134. [Google Scholar]
- Baumert, J.; Erazo, N.; Ruf, E.; Ladwig, K.H. Time trends in suicide mortality vary in choice of methods: An analysis of 145,865 fatal suicide cases in Germany 1991-2002. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 913–919. [Google Scholar]
- Baumert, J.; Erazo, N.; Ladwig, K.H. Sex- and age-specific trends in mortality from suicide and undetermined death in Germany 1991-2002. BMC Public Health 2005, 5, 61. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lukaschek, K.; Erazo, N.; Baumert, J.; Ladwig, K.-H. Suicide Mortality in Comparison to Traffic Accidents and Homicides as Causes of Unnatural Death. An Analysis of 14,441 Cases in Germany in the Year 2010. Int. J. Environ. Res. Public Health 2012, 9, 924-931. https://doi.org/10.3390/ijerph9030924
Lukaschek K, Erazo N, Baumert J, Ladwig K-H. Suicide Mortality in Comparison to Traffic Accidents and Homicides as Causes of Unnatural Death. An Analysis of 14,441 Cases in Germany in the Year 2010. International Journal of Environmental Research and Public Health. 2012; 9(3):924-931. https://doi.org/10.3390/ijerph9030924
Chicago/Turabian StyleLukaschek, Karoline, Natalia Erazo, Jens Baumert, and Karl-Heinz Ladwig. 2012. "Suicide Mortality in Comparison to Traffic Accidents and Homicides as Causes of Unnatural Death. An Analysis of 14,441 Cases in Germany in the Year 2010" International Journal of Environmental Research and Public Health 9, no. 3: 924-931. https://doi.org/10.3390/ijerph9030924