Dental Caries Risk Studies Revisited: Causal Approaches Needed for Future Inquiries

Abstract
:1. Common Approaches in Caries Risk Studies
2. Literature Search for Caries Risk Studies
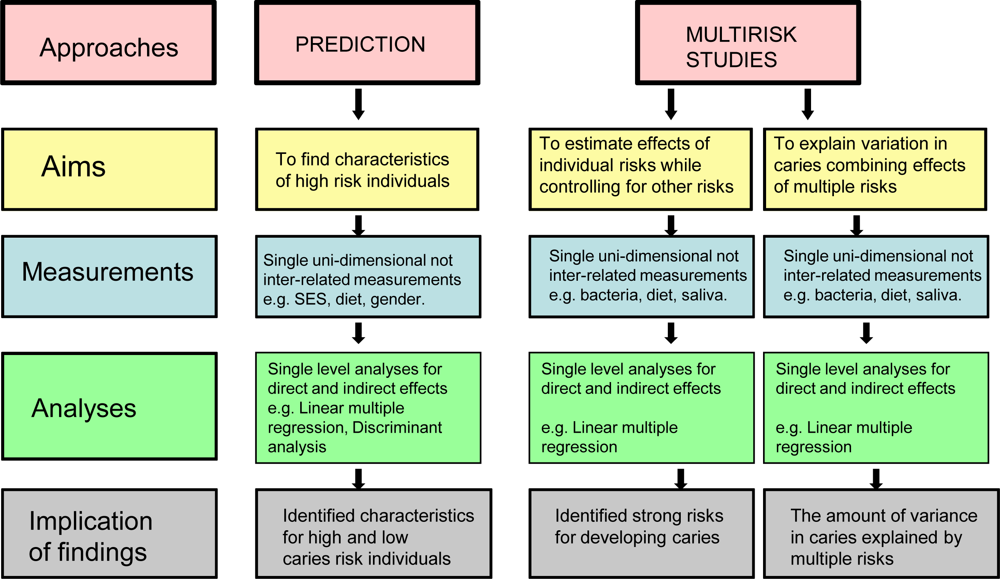
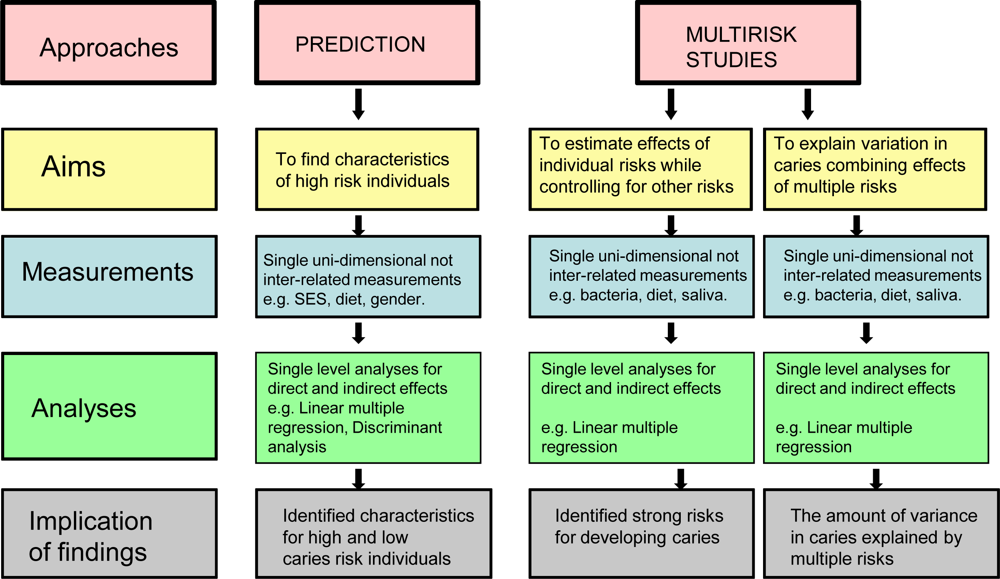
3. Prediction Studies
4. Multi-Risk Studies
5. Differences and Commonalities between Prediction and Multi-Risk Approaches
6. Limitations of Current Approaches
- Lack of success to predict high-risk individuals.
- Lack of success to explain variations in caries among individuals, population subgroups or between populations.
- Evidence for dental health promotion is insufficient; individual-based caries risk studies are plenty, while population-based risk studies are scarce.
- Current approaches cannot efficiently support population-based dental health preventive programs.
Lack of success to predict high-risk individuals
Lack of success to explain variations in caries among individuals, population subgroups or between populations
Evidence for dental health promotion is insufficient: individual-based caries risk studies are plenty, while population-based risk studies are scarce
Current approaches cannot efficiently support population-based dental health preventive programs
7. Towards Further Understanding of the Development of Dental Caries in Populations: A Causal Approach as an Alternative to Prediction and Multi-Risk Assessment
8. Causal Studies—Focus on Measurements and Analyses
Re: Selection of measurements
Are prediction analyses suitable for causal inquiries?
Causal analyses are necessary for causal inquiries
Different treatment of ‘confounder’ variables in prediction and causal analyses
9. Empirical Examples of Causal Studies
A medical example of a causal study
Causal studies in dentistry
10. Conclusions
Acknowledgments
- Conflict of Interest StatementNone declared.
References
- Rose, G. Sick individuals and sick populations. Int. J. Epidemiol 1985, 14, 32–38. [Google Scholar]
- Wolfson, MC. Social proprioception: measurement, data, and information from a population health perspective. In Why Some People Are Healthy and Others Are Not? The Determinants of Health in Populations; Evans, RG, Barer, ML, Marmor, TR, Eds.; Aldine De Gruyter: New York, NY, USA, 1994; pp. 287–316. [Google Scholar]
- Vanobbergen, J; Martens, L; Lesaffre, E; Bogaerts, K; Declerck, D. Assessing risk indicators for dental caries in the primary dentition. Community Dent. Oral Epidemiol 2001, 29, 424–434. [Google Scholar]
- Steiner, M; Helfenstein, U; Marthaler, TM. Dental predictors of high caries increment in children. J. Dent. Res 1992, 71, 1926–1933. [Google Scholar]
- van Palenstein Helderman, WH; van’T Hof, MA; van, LC. Prognosis of caries increment with past caries experience variables. Caries Res 2001, 35, 186–192. [Google Scholar]
- Helderman, WH; Mulder, J; van’T Hof, MA; Truin, GJ. Validation of a Swiss method of caries prediction in Dutch children. Community Dent. Oral Epidemiol 2001, 29, 341–345. [Google Scholar]
- Abernathy, JR; Graves, RC; Bohannan, HM; Stamm, JW; Greenberg, BG; Disney, JA. Development and application of a prediction model for dental caries. Community Dent. Oral Epidemiol 1987, 15, 24–28. [Google Scholar]
- Petti, S; Hausen, HW. Caries prediction by multiple salivary mutans streptococcal counts in caries-free children with different levels of fluoride exposure, oral hygiene and sucrose intake. Caries Res 2000, 34, 380–387. [Google Scholar]
- Raitio, M; Pienihakkinen, K; Scheinin, A. Multifactorial modeling for prediction of caries increment in adolescents. Acta Odontol. Scand 1996, 54, 118–121. [Google Scholar]
- Stamm, JW; Disney, JA; Graves, RC; Bohannan, HM; Abernathy, JR. The University of North Carolina Caries Risk Assessment Study. I: Rationale and content. J. Public Health Dent 1988, 48, 225–232. [Google Scholar]
- Stewart, PW; Stamm, JW. Classification tree prediction models for dental caries from clinical, microbiological, and interview data. J. Dent. Res 1991, 70, 1239–1251. [Google Scholar]
- Vanobbergen, J; Martens, L; Lesaffre, E; Bogaerts, K; Declerck, D. The value of a baseline caries risk assessment model in the primary dentition for the prediction of caries incidence in the permanent dentition. Caries Res 2001, 35, 442–450. [Google Scholar]
- Benn, DK; Dankel, DD; Kostewicz, SH. Can low accuracy disease risk predictor models improve health care using decision support systems. Proc AMIA Symp 1998, 577–581. [Google Scholar]
- Disney, JA; Graves, RC; Stamm, JW; Bohannan, HM; Abernathy, JR; Zack, DD. The University of North Carolina Caries Risk Assessment study: further developments in caries risk prediction. Community Dent. Oral Epidemiol 1992, 20, 64–75. [Google Scholar]
- Messer, LB. Assessing caries risk in children. Aust. Dent. J 2000, 45, 10–16. [Google Scholar]
- Graves, RC; Disney, JA; Stamm, JW; Abernathy, JR; Bohannen, HM. Physical and environmental risk factors in dental caries. Bader, JD, Ed.; University of North Carolina: Chapel Hill, NC, USA, 1990; pp. 37–47. [Google Scholar]
- Honkala, E; Nyyssonen, V; Kolmakow, S; Lammi, S. Factors predicting caries risk in children. Scand. J. Dent. Res 1984, 92, 134–140. [Google Scholar]
- Hausen, H. Caries prediction—state of the art. Community Dent. Oral Epidemiol 1997, 25, 87–96. [Google Scholar]
- Beck, JD; Disney, JA; Graves, RC; Stamm, JW; Kaste, LM; Bohannan, HM. University of North Carolina caries risk assessment study. Comparisons of high-risk prediction, any risk prediction, and any risk etiologic models. Community Dent. Oral Epidemol 1992, 20, 313–321. [Google Scholar]
- Mattila, ML; Rautava, P; Paunio, P; Ojanlatva, A; Hyssala, L; Helenius, H; Sillanpaa, M. Caries experience and caries increments at 10 years of age. Caries Res 2001, 35, 435–441. [Google Scholar]
- Broadbent, JM; Ayers, KM; Thomson, WM. Is attention-deficit hyperactivity disorder a risk factor for dental caries? A case-control study. Caries Res 2004, 38, 29–33. [Google Scholar]
- Agrawal, D. Inappropriate interpretation of the odds ratio: oddly not that uncommon. Pediatrics 2005, 116, 1612–1613. [Google Scholar]
- Turunen, S; Nyyssonen, V; Vesala, H. Perspectives on poor dental health and its determinants. Community Dent. Health 1992, 10, 49–55. [Google Scholar]
- Baerum, P; Holst, DRJ. Dental Health in Trondelag 1983. Changes from 1973 to 1983; Directorate of Health: Oslo, Norway, 1985. [Google Scholar]
- Unell, L; Soderfeldt, B; Halling, A; Birkhed, D. Explanatory models for clinically determined and symptom reported caries indicators in an adult population. Acta Odontol. Scand 1999, 57, 132–143. [Google Scholar]
- Berset, GP; Eriksen, HM; Bjertness, E; Hansen, BF. Caries experience of 35-year-old Oslo residents and changes over a 20-year period. Community Dent. Health 1996, 13, 238–244. [Google Scholar]
- Gilbert, GH; Foerster, U; Dolan, TA; Duncan, RP; Ringelberg, ML. Twenty-four month coronal caries incidence: the role of dental care and race. Caries Res 2000, 34, 367–79. [Google Scholar]
- Schwartz, S; Susser, E; Susser, M. A future for epidemiology? Annu. Rev. Public Health 1999, 20, 15–33. [Google Scholar]
- Polit, DF; Hungler, BP. Nursing Research Principles and Methods; J.B. Lippincott Company: Philadelphia, NY, USA, 1995. [Google Scholar]
- Drake, CW; Hunt, RJ; Beck, JD; Koch, GG. Eighteen-month coronal caries incidence in North Carolina older adults. J. Public Health Dent 1994, 54, 24–30. [Google Scholar]
- Eriksen, HM; Marques, MD; Bjertness, E; Moe, B. Dental caries determinants in an adult Portuguese population and a comparison with Norwegian adults. Acta Odontol. Scand 1996, 54, 49–54. [Google Scholar]
- Hallett, KB; O’Rourke, PK. Social and behavioural determinants of early childhood caries. Aust. Dent. J 2003, 48, 27–33. [Google Scholar]
- Lawrence, HP; Hunt, RJ; Beck, JD. Three-year root caries incidence and risk modeling in older adults in North Carolina. J. Public Health Dent 1995, 55, 69–78. [Google Scholar]
- Li, Y; Wang, W. Predicting caries in permanent teeth from caries in primary teeth: an eight-year cohort study. J. Dent. Res 2002, 81, 561–566. [Google Scholar]
- Campus, G; Solinas, G; Strohmenger, L; Cagetti, MG; Senna, A; Minelli, L; Majori, S; Montagna, MT; Reali, D; Castiglia, P. The Collaborating Study Group. National pathfinder survey on children’s oral health in Italy: pattern and severity of caries disease in 4-year-olds. Caries Res 2009, 43, 155–162. [Google Scholar]
- Hansel, PG; Twetman, S; Bratthall, D. Evaluation of a computer program for caries risk assessment in schoolchildren. Caries Res 2002, 36, 327–340. [Google Scholar]
- Seow, WK; Clifford, H; Battistutta, D; Morawska, A; Holcombe, T. Case-control study of early childhood caries in Australia. Caries Res 2009, 43, 25–35. [Google Scholar]
- Tu, YKKM; Clerehugh, V; Gilthorpe, MS. Problems of correlations between explanatory variables in multiple regression analyses in the dental literature. Br. Dent. J 2005, 199, 457–461. [Google Scholar]
- Victora, CG; Huttly, SR; Fuchs, SC; Olinto, MT. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. Int. J. Epidemiol 1997, 26, 224–227. [Google Scholar]
- Hunt, R. Behavioral and sociodemographic risk factors for caries. In Risk Assessment in Dentistry; Bader, JD, Ed.; University of North Carolina: Chapel Hill, NC, USA, 1990; pp. 29–34. [Google Scholar]
- Batchelor, P; Sheiham, A. The limitations of a ‘high-risk’ approach for the prevention of dental caries. Community Dent. Oral Epidemiol 2002, 30, 302–312. [Google Scholar]
- Johnson, NW. Introduction: the nature of the caries process and the need for markers of risk. In Dental Caries; Johnson, NW, Ed.; Cambridge University Press: Cambridge, UK, 1991; pp. 1–12. [Google Scholar]
- Risk Assessment in Dentistry; Bader, JD (Ed.) University of North Carolina: Chapel Hill, NC, USA, 1990.
- Beck, JD; Kohout, FJ; Hunt, RJ; Heckert, DA. Root caries: physical, medical and psychosocial correlates in an elderly population. Gerodontics 1986, 32, 42–47. [Google Scholar]
- Locker, D; Leake, JL. Coronal and root decay experience in older adults in Ontario, Canada. J. Public Health Dent 1993, 53, 158–164. [Google Scholar]
- Stamm, JW; Disney, JA; Beck, JD; Weintraub, JA. The University of North Carolina Caries Risk Assessment Study: final results and some alternative modelling approaches. In Cariology for the Nineties; Bowen, HW, Tabak, LA, Eds.; University of Rochester Press: Rochester, NY, USA, 1993; pp. 209–233. [Google Scholar]
- Tubert-Jeannin, S; lardon, JP; Pham, E; Martin, JL. Factors affecting caries experience in French adolescents. Community Dent. Oral Epidemiol 1994, 22, 30–35. [Google Scholar]
- Perera, I; Ekanayake, L. Factors influencing perception of oral health among adolescents in Sri Lanka. Int. Dent. J 2008, 58, 349–355. [Google Scholar]
- Greenland, S; Gago-Dominguez, CJE. The value of risk-factor (“black box”) epidemiology. Epidemiology 2004, 15, 529–535. [Google Scholar]
- Karhausen, LR. Causation: the elusive grail of epidemiology. Med. Health Care Philos 2000, 3, 59–67. [Google Scholar]
- Kay-Tee, K. Rose’s Strategy of Preventive Medicine; updated ed; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- Porta, M. A Dictionary of Epidemiology, 5th ed; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Doyle, YG; Furey, A; Flowers, J. Sick Individuals and Sick Populations: 20 Years Later; Eastern Region Public Health Observatory, Institute of Public Health: Cambridge, UK, 2005. [Google Scholar]
- Weed, DL. Environmental epidemiology: basics and proof of cause-effect. Toxicology 2002, 181, 399–403. [Google Scholar]
- Weed, DL. Theory and practice in epidemiology. Ann. NY Acad. Sci 2001, 954, 52–62. [Google Scholar]
- Weed, DL. Precaution, Prevention, and Public Health Ethics. J. Med. Philos 2004, 29, 313–332. [Google Scholar]
- Donaldson, AN; Everitt, B; Newton, T; Steele, J; Sherriff, M; Bower, E. The effects of social class and dental attendance on oral health. J. Dent. Res 2008, 87, 60–64. [Google Scholar]
- Vanobbergen, J; Martens, L; Lesaffre, E; Bogaerts, K; Declerck, D. Assessing risk indicators for dental caries in the primary dentition. Community Dent. Oral Epidemiol 2001, 29, 424–434. [Google Scholar]
- Rockhill, B. Theorizing about causes at the individual level while estimating effects at the population level: implications for prevention. Epidemiology 2005, 16, 124–129. [Google Scholar]
- Susser, E; Schwartz, S. Are social causes so different from all other causes? A comment on Sander Greenland. Emerg. Themes Epidemiol 2005, 24, 2–4. [Google Scholar]
- Susser, M; Susser, E. Choosing a future for epidemiology: from black box to Chinese boxes and eco-epidemiology. Am. J. Public Health 1996, 86, 674–677. [Google Scholar]
- Parascandola, M; Weed, DL. Causation in epidemiology. J. Epidemiol. Community Health 2001, 55, 905–912. [Google Scholar]
- Mann, CJ. Observational research methods. Research design. II: cohort, cross sectional, and case-control studies. Emerg. Med. J 2003, 20, 54–60. [Google Scholar]
- Barreto, ML. Epidemiologists and causation in an intricate world. Emerg. Themes Epidemiol 2005, 24, 2–3. [Google Scholar]
- Rose, G. The Strategy of Preventive Medicine; Oxford University Press: Oxford, UK, 1993. [Google Scholar]
- Maldonado, GGS. The causal-contrast study design. Am. J. Epidemiol 2000, 151, S39. [Google Scholar]
- Earp, JA; Ennett, ST. Conceptual models for health education research and practice. Health Educ. Res 1991, 6, 163–171. [Google Scholar]
- Phillips, LR. Causal modeling as a relevant approach to gerontological nursing. J. Gerontol. Nurs 1990, 16, 20–24. [Google Scholar]
- Kar, SB; Berkanovic, E. Indicators of behaviour conducive to health promotion. In Measurement in Health Promotion and Protection; Abelin, T, Brzezinski, ZJ, Carstairs, VDL, Eds.; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 1987; pp. 267–293. [Google Scholar]
- McHorney, CA. Health status assessment methods for adults: past accomplishments and future challenges. Annu. Rev. Public Health 1999, 20, 309–335. [Google Scholar]
- Greenland, S. Interpretation and choice of effect measures in epidemiologic analysis. Am. J. Epidemiol 1987, 125, 761–768. [Google Scholar]
- Evans, RG; Barer, ML; Marmor, TR. Why Are Some People Healthy and Others Not? The Determinants of Health of Populations; Aldine De Gruyter: New York, NY, USA, 1994. [Google Scholar]
- Altman, DG. Statistics in medical journals: some recent trends. Statist. Med 2000, 19, 3275–3289. [Google Scholar]
- Cohen, JT. The cost of dichotomization. Applied Psychological Measurement 1983, 7, 249–253. [Google Scholar]
- Jacobsen, BS. Organising and displaying data. In Statistical Methods for Health Care Research; Munro, BH, Ed.; Lippincot: Philadelphia, NY, USA, 1997; pp. 3–29. [Google Scholar]
- Aleksejuniene, J; Holst, D; Eriksen, HM. Patterns of dental caries and treatment experience in elderly Lithuanians. Gerodontology 2000, 17, 77–86. [Google Scholar]
- Foxman, B. Challenges of epidemiology in the 21st century: comments from the leaders of several epidemiology associations. Ann. Epidemiol 2005, 15, 1–4. [Google Scholar]
- Altman, DG. Practical Statistics for Medical Research; Chapman and Hall: London, UK, 1993. [Google Scholar]
- Lewis-Beck, M. Applied Regression; SAGE Publications: Beverly Hills, CA, USA, 1980. [Google Scholar]
- Koopman, JS; Lynch, JW. Individual causal models and population system models in epidemiology. Am. J. Public Health 1999, 89, 1170–1174. [Google Scholar]
- Aleksejuniene, J; Holst, D; Sandvik, L. Prediction and explanation—two approaches for studying lifestyle in relation to oral health. In Trends in Lifestyle and Health Research; Kinger, L, Ed.; Nova Science Inc: New York, NY, USA, 2005. [Google Scholar]
- Scheutz, F; Frydenberg, M; Matee, MI; Poulsen, S. The effect of choosing different units of analysis when estimating risk of presence of dental caries in the primary dentition. Community Dent. Health 2003, 20, 27–33. [Google Scholar]
- Dean, K. Integrating theory and methods in population health research. In Population Health Research: Linking Theory and Methods; Dean, K, Ed.; Sage Publications: Thousand Oaks, CA, USA, 1993; pp. 9–37. [Google Scholar]
- Bokhout, B; Hofman, FXLJ; Prahl-Andersen, BA. ‘Sufficient cause’ model for dental caries. J. Epidemiol. Biostat 2000, 5, 203–208. [Google Scholar]
- Diez-Roux, AV. Multilevel analysis in public health research. Annu. Rev. Public Health 2000, 21, 171–192. [Google Scholar]
- Greenland, S; Brumback, B. An overview of relations among causal modelling methods. Int. J. Epidemiol 2002, 31, 1030–1037. [Google Scholar]
- Byrne, BM. Structural Equation Models Structural Equation Modeling with EQS and EQS/Windows; SAGE Publications: Thousand Oaks, CA, USA, 1994; pp. 3–22. [Google Scholar]
- Bollen, K; Long, J. Testing Structural Equation Models; Sage Publications: Newbury Park, CA, USA, 1993. [Google Scholar]
- Rasbash, J; Steele, F; Browne, WG; Goldstein, H. A User’s Guide to MLwiN version 2.10; Centre for Multilevel Modelling, University of Bristol: Bristol, UK, 2009. [Google Scholar]
- Newton, JT; Bower, EJ. The social determinants of oral health: new approaches to conceptualizing and researching complex causal networks. Community Dent. Oral Epidemiol 2005, 33, 25–34. [Google Scholar]
- Greenland, S; Morgenstern, H. Confounding in health research. Annu. Rev. Public Health 2001, 22, 189–212. [Google Scholar]
- Oh, HS; Seo, WS. Development of a structural equation model for causal relationships among arteriosclerosis risk factors. Public Health Nurs 2001, 18, 409–417. [Google Scholar]
- Litt, MD; Reisine, S; Tinanoff, N. Multidimensional causal model of dental caries development in low-income preschool children. Public Health Rep 1995, 110, 607–617. [Google Scholar]
- Aleksejuniene, J; Holst, D; Eriksen, HM; Gjermo, P. Psychosocial stress, lifestyle and periodontal health. J. Clin. Periodontol 2002, 29, 326–335. [Google Scholar]
- Aleksejuniene, J; Holst, D; Grytten, JI; Eriksen, HM. Causal patterns of dental health in populations. An empirical approach. Caries Res 2002, 36, 233–240. [Google Scholar]
- Fliege, H; Rose, M; Arck, P; Walter, OB; Kocalevent, RD; Weber, C; Klapp, BF. The Perceived Stress Questionnaire (PSQ) reconsidered: validation and reference values from different clinical and healthy adult samples. Psychosom. Med 2005, 67, 78–88. [Google Scholar]
- Donaldson, AN; Everitt, B; Newton, T; Steele, J; Sherriff, M; Bower, E. The effects of social class and dental attendance on oral health. J. Dent. Res 2008, 87, 60–64. [Google Scholar]
- Bower, E; Gulliford, M; Steele, J; Newton, T. Area deprivation and oral health in Scottish adults: a multilevel study. Community Dent. Oral Epidemiol 2007, 35, 118–129. [Google Scholar]

{kind=link}
| Steps | MeSH subject heading or keyword | Number of references | Search mode |
|---|---|---|---|
| 1 | exp Epidemiologic Studies | 1,180,888 | Advanced |
| 2 | dental caries.sh. not restor*.af. not endo*.af. not perio.af. not implant*.af. | 26,910 | Advanced |
| 3 | 1 and 2 | 2,269 | Advanced |
| 4 | predict*.mp. [mp = title, original title, abstract, name of substance word, subject heading word] | 618,379 | Advanced |
| 5 | expla*.mp. [mp = title, original title, abstract, name of substance word, subject heading word] | 348,896 | Advanced |
| 6 | caus*.mp. [mp = title, original title, abstract, name of substance word, subject heading word] | 1,286,475 | Advanced |
| 7 | risk*.mp. [mp = title, original title, abstract, name of substance word, subject heading word] | 1,075,803 | Advanced |
| 8 | 6 or 4 or 7 or 5 | 2,901,862 | Advanced |
| 9 | 8 and 3 | 768 | Advanced |
| 10 | The titles and abstracts of references from step 9 overviewed | 222 | Manual |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Aleksejūnienė, J.; Holst, D.; Brukienė, V. Dental Caries Risk Studies Revisited: Causal Approaches Needed for Future Inquiries. Int. J. Environ. Res. Public Health 2009, 6, 2992-3009. https://doi.org/10.3390/ijerph6122992
Aleksejūnienė J, Holst D, Brukienė V. Dental Caries Risk Studies Revisited: Causal Approaches Needed for Future Inquiries. International Journal of Environmental Research and Public Health. 2009; 6(12):2992-3009. https://doi.org/10.3390/ijerph6122992
Chicago/Turabian StyleAleksejūnienė, Jolanta, Dorthe Holst, and Vilma Brukienė. 2009. "Dental Caries Risk Studies Revisited: Causal Approaches Needed for Future Inquiries" International Journal of Environmental Research and Public Health 6, no. 12: 2992-3009. https://doi.org/10.3390/ijerph6122992