How Older People Experience the Age-Friendliness of Their City: Development of the Age-Friendly Cities and Communities Questionnaire


Abstract
:1. Introduction
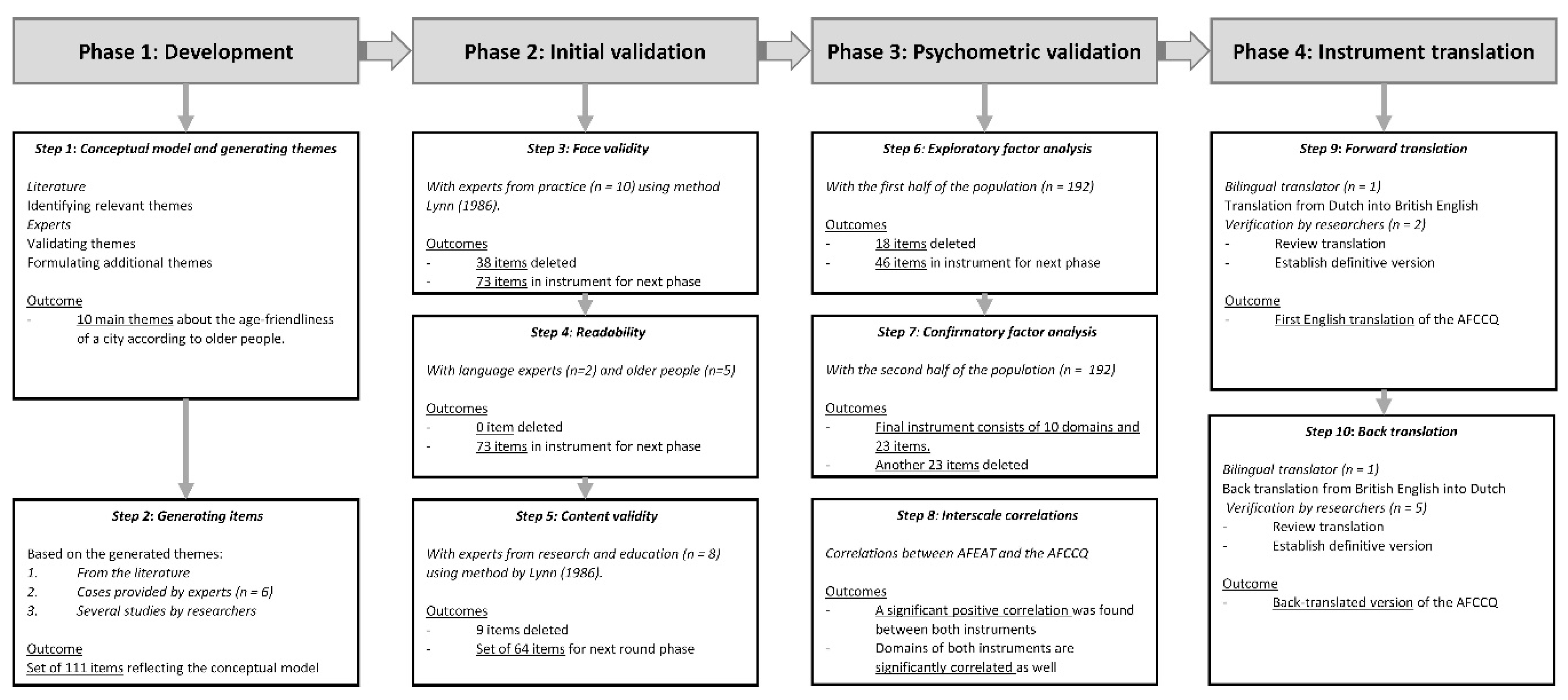
2. Materials and Methods
2.1. Phase 1: Development of the Conceptual Model, Themes and Questions of the AFCCQ (steps 1 and 2)
2.2. Phase 2: Initial (Qualitative) Validation (Steps 3 to 5)
2.2.1. Step 3: Face Validity—Participants and Measurement
2.2.2. Step 4: Readability—Participants and Measurement
2.2.3. Step 5: Content Validity—Participants and Measurement
2.2.4. Statistical Analyses in Phase 2
2.3. Phase 3: Psychometric Validation (Steps 6 to 8)
2.3.1. Data Collection and Participants in Phase 2
2.3.2. Step 6: Exploratory Factor Analysis
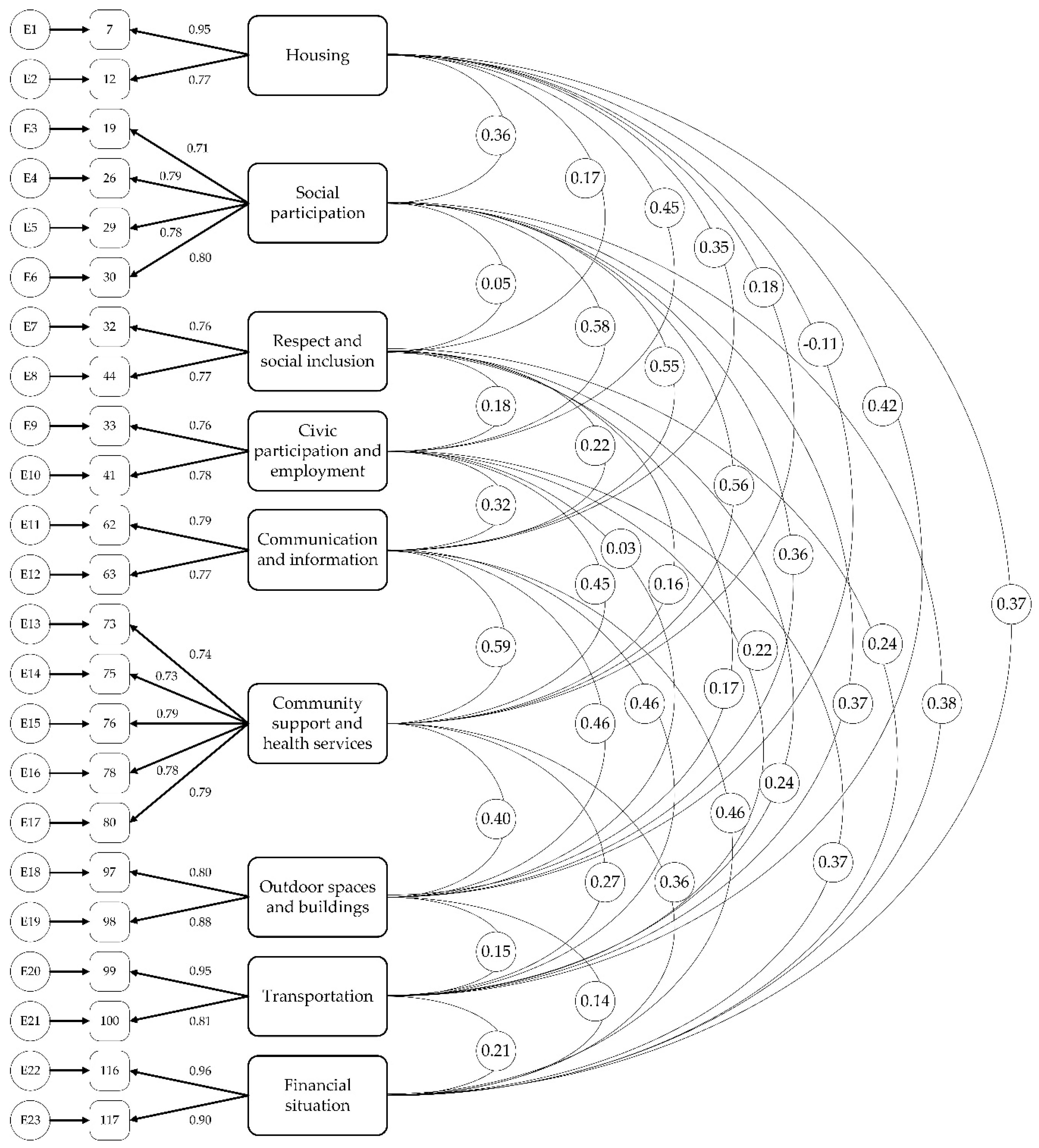
2.3.3. Step 7: Confirmatory Factor Analysis
2.3.4. Step 8: Interscale Correlation
2.4. Phase 4: Instrument Translation (Steps 9 and 10)
3. Results
3.1. Phase 1: Development of the Conceptual Model, Themes and Questions of the AFCCQ (Steps 1 and 2)
3.2. Phase 2: Initial (Qualitative) Validation
3.2.1. Step 3: Face Validity
3.2.2. Step 4: Readability
3.2.3. Step 5: Content Validity
3.3. Phase 3: Psychometric Validation
3.3.1. Step 6: Exploratory Factor Analysis
3.3.2. Step 7: Confirmatory Factor Analysis
3.4. Phase 4: Instrument Translation (Steps 9 and 10)
3.5. Interpretation and Presentation of Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| De Age Friendly Cities and Communities Questionnaire (AFCCQ) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Alle Vragen van de AFCCQ Kunnen Beantwoord Worden op een 5-Punt Likert-Schaal van −2 (Helemaal Oneens); −1 (Oneens); 0 (Noch Mee Eens, Noch Mee Oneens); 1 (Eens); 2 (helemaal Eens). | ||||||||
| Item | Domein | |||||||
| Huisvesting | ||||||||
| Q1 | Mijn woning is toegankelijk voor mij. | |||||||
| Q2 | Mijn woning is toegankelijk voor mensen die mij willen bezoeken. | |||||||
| Sociale participatie | ||||||||
| Q3 | In mijn buurt zijn voldoende gelegenheden om mensen te ontmoeten. | |||||||
| Q4 | Activiteiten en evenementen worden georganiseerd op voor mij bereikbare plaatsen. | |||||||
| Q5 | De informatie over activiteiten en evenementen vind ik voldoende en ook geschikt voor mij. | |||||||
| Q6 | Ik vind het aanbod van evenementen en activiteiten voldoende afwisselend. | |||||||
| Sociale inclusie | ||||||||
| Q7 * | Ik krijg wel eens vervelende of negatieve opmerkingen vanwege mijn leeftijd. | |||||||
| Q8 * | Ik krijg wel eens te maken met discriminatie vanwege mijn leeftijd. | |||||||
| Burgerparticipatie en werkgelegenheid | ||||||||
| Q9 | Ik heb voldoende mogelijkheden om met jongere generaties om te gaan. | |||||||
| Q10 | Ik voel mij een gewaardeerd lid van de samenleving. | |||||||
| Communicatie en informatie | ||||||||
| Q11 | Gedrukte en digitale informatie van de gemeente en andere maatschappelijke instanties zijn goed leesbaar qua lettertype en grootte. | |||||||
| Q12 | Gedrukte en digitale informatie van de gemeente en andere maatschappelijke instanties zijn geschreven in begrijpelijke taal. | |||||||
| Sociale en gezondheidsvoorzieningen | ||||||||
| Q13 | Het aanbod van zorg en welzijn in mijn stad is voor mij voldoende. | |||||||
| Q14 | Als ik ziek ben, krijg ik de zorg en hulp die ik nodig heb. | |||||||
| Q15 | Indien nodig, kan ik zorg en welzijn telefonisch en fysiek gemakkelijk bereiken. | |||||||
| Q16 | Ik heb voldoende informatie over zorg en welzijn in mijn buurt. | |||||||
| Q17 | Zorg en welzijn werkers in mijn buurt zijn voldoende respectvol. | |||||||
| Buitenruimte en gebouwen | ||||||||
| Q18 | Mijn buurt is voldoende toegankelijk voor rollator of rolstoel. | |||||||
| Q19 | De winkels in mijn buurt zijn voldoende toegankelijk met rollator of rolstoel. | |||||||
| Transport | ||||||||
| Q20 | Ik kan gemakkelijk instappen in de bus of tram in mijn buurt. | |||||||
| Q21 | De bus- en tramhaltes in mijn buurt zijn gemakkelijk te bereiken en te gebruiken. | |||||||
| Financiën | ||||||||
| Q22 | Mijn inkomen is voldoende om zonder problemen in mijn basisbehoeften te voorzien. | |||||||
| Q23 | Ik kan goed rondkomen met mijn inkomen. | |||||||
| Interpretatie AFCCQ totaalscore en specifieke domeinen | ||||||||
| − − − − | − − − | − − | − | + | + + | + + + | + + + + | |
| AFCCQ Totaal score | ≤−35.1 | −23.1–−35.0 | −11.5–−23.0 | −11.4–0.0 | 0.1–11.4 | 11.5–23.0 | 23.1–35.0 | ≥35.1 |
| Huisvesting | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Sociale participatie | ≤−6.1 | −4.1–−6.0 | −2.1–−4.0 | −2.0–0.0 | 0.1–2.0 | 2.1–4.0 | 4.1–6.0 | ≥6.1 |
| Sociale inclusie | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Burgerparticipatie en werkgelegenheid | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Communicatie en informatie | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Sociale en geszondheids-voorzieningen | ≤−7.6 | −5.1–−7.5 | −2.6–−5.0 | −2.5–0.0 | 0.1–2.5 | 2.6–5.0 | 5.1–7.5 | ≥7.6 |
| Buitenruimte en gebouwen | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Transport | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Financiën | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| The Age Friendly Cities and Communities Questionnaire (AFCCQ) | ||||||||
|---|---|---|---|---|---|---|---|---|
| All Questions of the AFCCQ Can Be Answered on a 5-Point Likert-Scale Ranging from: −2 (Totally Disagree); −1 (Disagree); 0 (Neutral); 1 (Agree); 2 (Totally Agree). | ||||||||
| Item | Domain | |||||||
| Housing | ||||||||
| Q1 | My house is accessible to me. | |||||||
| Q2 | My house is accessible to the people who come to visit me. | |||||||
| Social participation | ||||||||
| Q3 | There are enough opportunities to meet people in my neighbourhood. | |||||||
| Q4 | Activities and events are organised in places that are accessible to me. | |||||||
| Q5 | The information about activities and events is enough for me and also suitable for me. | |||||||
| Q6 | I find the range of events and activities sufficiently varied. | |||||||
| Respect and Social inclusion | ||||||||
| Q7 * | I sometimes get annoying or negative remarks because of my age. | |||||||
| Q8 * | I sometimes face discrimination because of my age. | |||||||
| Civic participation and employment | ||||||||
| Q9 | I have enough opportunities to interact with younger generations. | |||||||
| Q10 | I feel like a valued member of society. | |||||||
| Communication and information | ||||||||
| Q11 | Printed and digital information from the municipality and other social institutions is easy to read in terms of font and size. | |||||||
| Q12 | Printed and digital information from the municipality and other social institutions is written in understandable language. | |||||||
| Community support and health services | ||||||||
| Q13 | The supply of care and welfare in my city is enough for me. | |||||||
| Q14 | When I am ill, I receive the care and help I need. | |||||||
| Q15 | If necessary, I can easily reach care and welfare services by telephone and in person. | |||||||
| Q16 | I have enough information about care and welfare services in my neighbourhood. | |||||||
| Q17 | Care and welfare workers in my neighbourhood are sufficiently respectful. | |||||||
| Outdoor spaces and buildings | ||||||||
| Q18 | My neighbourhood is sufficiently accessible for a wheeled walker or wheelchair. | |||||||
| Q19 | The shops in my neighbourhood are sufficiently accessible with a wheeled walker or wheelchair. | |||||||
| Transportation | ||||||||
| Q20 | I can easily get on the bus or tram in my neighbourhood. | |||||||
| Q21 | The bus and tram stops in my neighbourhood are easy to reach and use. | |||||||
| Financial situation | ||||||||
| Q22 | My income is sufficient to cover my basic needs without any problems. | |||||||
| Q23 | I live well on my income. | |||||||
| Interpretation AFCCQ total score and separate domains. | ||||||||
| − − − − | − − − | − − | − | + | + + | + + + | + + + + | |
| AFCCQ Total score | ≤−35.1 | −23.1–−35.0 | −11.5–−23.0 | −11.4–0.0 | 0.1–11.4 | 11.5–23.0 | 23.1–35.0 | ≥35.1 |
| Housing | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Social participation | ≤−6.1 | −4.1–−6.0 | −2.1–−4.0 | −2.0–0.0 | 0.1–2.0 | 2.1–4.0 | 4.1–6.0 | ≥6.1 |
| Respect and social inclusion | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Civic participation and employment | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Communication and information | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Community support and health services | ≤−7.6 | −5.1–−7.5 | −2.6–−5.0 | −2.5–0.0 | 0.1–2.5 | 2.6–5.0 | 5.1–7.5 | ≥7.6 |
| Outdoor spaces and buildings | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Transportation | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
| Financial situation | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 |
References
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007; ISBN 9789241547307. [Google Scholar]
- Plouffe, L.; Kalache, A. Towards global age-friendly cities: Determining urban features that promote active aging. J. Urban Health 2010, 87, 33–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buffel, T.; Phillipson, C.; Rémillard-Boilard, S. Age-friendly cities and communities: New directions for research and policy. In Encyclopedia of Gerontology and Population Aging; Gu, D., Dupre, M.E., Eds.; Springer Nature: Cham, Switzerland, 2019. [Google Scholar] [CrossRef] [Green Version]
- van Hoof, J.; Kazak, J.K.; Perek-Białas, J.M.; Peek, S.T.M. The challenges of urban ageing: Making cities age-friendly in Europe. Int. J. Environ. Res. Public Health 2018, 15, 2473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, T.-Y.S. Planning for Greying Cities. Age-Friendly City Planning and Design Research and Practice; Routledge—Taylor & Francis Group: Abingdon, UK, 2018; ISBN 978-0-367-33190-0. [Google Scholar]
- Buffel, T.; Handler, S.; Phillipson, C. (Eds.) Age-friendly Cities and Communities. A Global Perspective; Policy Press: Bristol, UK, 2019; ISBN 978-1-4473-3134-6. [Google Scholar]
- Moulaert, T.; Garon, S. (Eds.) International perspectives on aging. In Age-Friendly Cities and Communities in International Comparison—Political Lessons, Scientific Avenues, and Democratic Issues; Springer International Publishing: Cham, Switzerland, 2016; Volume 14, ISBN 978-3-319-24029-9. [Google Scholar] [CrossRef]
- Van Hoof, J.; Marston, H.R.; Brittain, K.R.; Barrie, H.R. Creating age-friendly communities: Housing and technology. Healthcare 2019, 7, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hoof, J.; Kazak, J.K. Urban Ageing. Indoor Built Env. 2018, 27, 583–586. [Google Scholar] [CrossRef]
- Greenfield, E.A.; Oberlink, M.; Scharlach, A.E.; Neal, M.B.; Stafford, P.B. Age-friendly community initiatives: Conceptual issues and key questions. Gerontologist 2015, 55, 191–198. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. About the Global Network for Age-Friendly Cities and Communities. Available online: https://extranet.who.int/agefriendlyworld/who-network/ (accessed on 30 June 2020).
- World Health Organization. The Global Network for Age-Friendly Cities and Communities: Looking Back Over the Last Decade, Looking Forward to the Next; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Buckner, S.; Mattocks, C.; Rimmer, M.; Lafortune, L. An evaluation tool for Age-Friendly and Dementia Friendly Communities. Work. Older People 2018, 22, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Buckner, S.; Pope, D.; Mattocks, C.; Lafortune, L.; Dherani, M.; Bruce, N. Developing Age-Friendly Cities: An evidence-based evaluation tool. J. Popul. Ageing 2019, 12, 203–223. [Google Scholar] [CrossRef]
- World Health Organization. Measuring the Age-Friendliness of Cities: A Guide to Using Core Indicators; World Health Organization: Geneva, Switzerland, 2015; ISBN 9789241509695. [Google Scholar]
- World Health Organization. The Checklist of Essential Features of Age-Friendly Cities; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Fulmer, T.; Patel, P.; Levy, N.; Mate, K.; Berman, A.; Peloton, L.; Beard, J.; Kalache, A.; Auerbach, J. Moving toward a global age-friendly ecosystem. J. Am. Ger. Soc. 2020, in press. [Google Scholar] [CrossRef]
- Marston, H.R.; van Hoof, J. “Who doesn’t think about technology when designing urban environments for older people?” A case study approach to a proposed extension of the WHO’s age-friendly cities model. Int. J. Environ. Res. Public Health 2019, 16, 3525. [Google Scholar] [CrossRef] [Green Version]
- van Hoof, J.; Dikken, J.; Buttiġieġ, S.C.; van den Hoven, R.F.M.; Kroon, E.; Marston, H.R. Age-friendly cities in the Netherlands: An explorative study of facilitators and hindrances in the built environment and ageism in design. Indoor Built Environ. 2020, 29, 417–437. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.W.; Chan, H.Y.; Chan, I.K.; Cheung, B.Y.; Lee, D.T. An age-friendly living environment as seen by Chinese older adults: A “Photovoice” Study. Int. J. Environ. Res. Public Health 2016, 13, 913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.C.; King, D.K.; Banchoff, A.; Solomonov, S.; Ben Natan, O.; Hua, J.; Gardiner, P.; Goldman Rosas, L.; Rodriguez Espinosa, P.; Winter, S.J.; et al. Employing participatory citizen science methods to promote age-friendly environments worldwide. Int. J. Environ. Res. Public Health 2020, 17, 1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrie, H.; Soebarto, V.; Lange, J.; Mc Corry-Breen, F.; Walker, L. Using citizen science to explore neighbourhood influences on ageing well: Pilot project. Healthcare 2019, 7, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luciano, A.; Pascale, F.; Polverino, F.; Pooley, A. Measuring age-friendly housing: A framework. Sustainability 2020, 12, 848. [Google Scholar] [CrossRef] [Green Version]
- Flores, R.; Caballer, A.; Alarcón, A. Evaluation of an age-friendly city and its effect on life satisfaction: A two-stage study. Int. J. Environ. Res. Public Health 2019, 16, 5073. [Google Scholar] [CrossRef] [Green Version]
- Zaman, A.U.; Thornton, K. Prioritization of local indicators for the development of an age-friendly city: A community perspective. Urban Sci. 2018, 2, 51. [Google Scholar] [CrossRef] [Green Version]
- Garner, I.W.; Holland, C.A. Age-friendliness of living environments from the older person’s viewpoint: Development of the Age-friendly Environment Assessment Tool. Age Ageing 2020, 49, 193–198. [Google Scholar] [CrossRef]
- COSMIN. Consensus-Based Standards for Selection of Health Measurement Instruments. Available online: https://www.cosmin.nl/cosmin-tools/ (accessed on 11 August 2020).
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.M. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [Green Version]
- de Vet, H.C.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar] [CrossRef]
- Bottenheft, C.; van Doleweerd, M.K.; van de Kraats, E.J.; Egter van Wissekerke, N.G.; Engbers, L.H. TNO-Rapport: TNO 2015 R10311. Wijkdashboard: Age-Friendly City Den Haag; TNO: The Hague, The Netherlands, 2015. (In Dutch) [Google Scholar]
- AARP Public Policy Institute. AARP Livability Index—Great Neighborhoods for All Ages. 2020. Available online: https://livabilityindex.aarp.org/livability-defined (accessed on 23 July 2020).
- Chief Secretary for Administration’s Office. Active and Healthy Ageing in Hong Kong; Hong Kong Special Administrative Region Government: Hong Kong, China, 2017. [Google Scholar]
- World Health Organization. Equity. Available online: https://www.who.int/healthsystems/topics/equity/en/ (accessed on 1 September 2020).
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–386. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; Wegener, D.T.; MacCallum, R.C.; Strahan, E.J. Evaluating the use of exploratory factor analysis in psychological research. Psychol. Methods 1999, 4, 272. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale Development: Theory and Applications; Sage: Los Angeles, CA, USA, 2016; Volume 26, ISBN 9781506341569. [Google Scholar]
- Lee, W.C.; Godwin, A. Hermunstad Nave, A.L. Development of the engineering student integration instrument: Rethinking measures of integration. J. Eng. Educ. 2018, 107, 30–55. [Google Scholar] [CrossRef]
- Lijzenga, J.; Gijsbers, V.; Poelen, J.; Tiekstra, C. Ruimte voor Wonen. De Resultaten van het WoonOnderzoek Nederland 2018; Ministry of the Interior and Kingdom Relations: The Hague, The Netherlands, 2018; Available online: https://www.woononderzoek.nl/document/Ruimte-voor-wonen--de-resultaten-van-het-WoON2018-(interactief)-/174 (accessed on 22 August 2020).
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007; Volume 5, pp. 481–498. ISBN 9780134790541. [Google Scholar]
- Matsunaga, M. How to factor-analyze your data right: Do’s, don’ts, and how-to’s. Int. J. Psychol. Res. 2010, 3, 97–110. [Google Scholar] [CrossRef]
- Schumacker, R.E.; Lomax, R.G. A Beginner's Guide to Structural Equation Modeling, 2nd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; ISBN 1-4106-1090-X. [Google Scholar]
- Shadfar, S.; Malekmohammadi, I. Application of Structural Equation Modeling (SEM) in restructuring state intervention strategies toward paddy production development. Int. J. Acad. Res. Bus. Soc. Sci. 2013, 3, 576. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Evaluating model fit. In Structural Equation Modelling: Concepts, Issues, and Applications; Hoyle, R.H., Ed.; London Sage: London, UK, 1995; pp. 76–99. ISBN 0803953186. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternations. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power analysis and determination of sample size for covariance structure modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Hair, J.; Hult, C.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage: Los Angeles, CA, USA, 2014; ISBN 1452217440. [Google Scholar]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Maneesriwongul, W.; Dixon, J.K. Instrument translation process: A methods review. J. Adv. Nurs. 2004, 48, 175–186. [Google Scholar] [CrossRef]
- Costello, A.B.; Osborne, J.W. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 1–9. [Google Scholar]
- Netemeyer, R.G.; Bearden, W.O.; Sharma, S. Scaling Procedures; Sage Publications Inc.: Thousand Oaks, CA, USA, 2003. [Google Scholar] [CrossRef]
- Van de Schoot, R.; Lugtig, P.; Hox, J. A checklist for testing measurement invariance. Eur. J. Dev. Psychol. 2012, 9, 486–492. [Google Scholar] [CrossRef]
- Dikken, J.; Hoogerduijn, J.G.; Klaassen, S.; Lagerwey, M.D.; Shortridge-Baggett, L.; Schuurmans, M.J. The knowledge-about-older-patients-quiz (KOP-Q) for nurses: Cross-cultural validation between the Netherlands and United States of America. Nurse Educ. Today 2017, 55, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Buffel, T.; Phillipson, C.; Scharf, T. Ageing in urban environments: Developing ‘age-friendly’ cities’. Crit. Soc. Policy 2012, 32, 597–617. [Google Scholar] [CrossRef] [Green Version]
- Scharf, T.; Phillipson, C.; Smith, A. Older people’s perceptions of the neighbourhood: Evidence from socially deprived urban areas. Sociol. Res. Online 2003, 8, 153–164. [Google Scholar] [CrossRef]
- Baraković, S.; Baraković Husić, J.; van Hoof, J.; Krejcar, O.; Maresova, P.; Akhtar, Z.; Melero, F.J. Quality of life framework for personalised ageing: A systematic review of ICT solutions. Int. J. Environ. Res. Public Health 2020, 17, 2940. [Google Scholar] [CrossRef]
- Verkerk, M.J.; van Hoof, J.; Aarts, S.; de Koning, S.J.M.M.; van der Plaats, J.J. A neurological and philosophical perspective on the design of environments and technology for older people with dementia. J. Enabling Technol. 2018, 12, 57–75. [Google Scholar] [CrossRef] [Green Version]
- Mundform, D.J.; Shaw, D.G.; Ke, T.L. Minimum sample size recommendations for conducting factor analyses. Int. J. Test. 2005, 5, 159–168. [Google Scholar] [CrossRef]
- Wolf, E.J.; Harrington, K.M.; Clark, S.L.; Miller, M.W. Sample size requirements for structural equation models an evaluation of power, bias, and solution propriety. Educ. Psychol. Meas. 2013, 73, 913–934. [Google Scholar] [CrossRef]
- Sideridis, G.; Simos, P.; Papanicolaou, A.; Fletcher, J. Using structural equation modeling to assess functional connectivity in the brain: Power and sample size considerations. Educ. Psychol. Meas. 2014, 74, 733–758. [Google Scholar] [CrossRef] [Green Version]


| Sex | |
| Male | n = 188 (49%) |
| Female | n = 196 (51%) |
| Age | |
| Mean (SD) | 74.4 (6.36) |
| 60–65 | n = 10 (2.6%) |
| 65–69 | n = 82 (21.4%) |
| 70–74 | n = 118 (30.7%) |
| 75+ | n = 156 (40.6%) |
| Missing values | n = 17 (4.7%) |
| Born in the European part of the Kingdom of the Netherlands (%) 1 | n = 329 (85.7%) |
| Educational level | |
| Primary education only | n= 19 (4.9%) |
| Secondary school giving entry to intermediate vocational education | n = 101 (26.4%) |
| Intermediate vocational education | n = 64 (16.7%) |
| Secondary school giving entry to university (of applied sciences) | n = 35 (9.1%) |
| University of applied sciences | n = 95 (24.7%) |
| University | n = 70 (18.2%) |
| Years living in The Hague | |
| Mean (SD) | 51.3 (22.7) |
| Type of dwelling | |
| Owner-occupant | n = 230 (59.9%) |
| Social housing | n = 110 (28.6%) |
| Private rent | n = 44 (11.5%) |
| Living together with a partner (%) | n = 216 (56.3%) |
| Receiving care (%) | n = 98 (25.5%) |
| Living with one or more chronic conditions (%) | n = 186 (48.4%) |
| Using a wheeled walker or wheelchair (%) | n = 56 (14.6%) |
| Item | Communality | Factor Loading | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Housing | Social Participation | Respect and Social Inclusion | Civic Participation and Employment | Communication and Information | Community Support and Health Services | Outdoor Spaces and Buildings | Transportation | Technology | Financial Situation | ||
| 1 | 0.702 | 0.30 | 0.67 | ||||||||
| 3 | 0.621 | 0.51 | |||||||||
| 4 | 0.677 | 0.76 | |||||||||
| 9 | 0.628 | 0.77 | |||||||||
| 10 | 0.699 | 0.41 | |||||||||
| 12 | 0.611 | 0.64 | |||||||||
| 13 | 0.611 | 0.56 | |||||||||
| 16 | 0.632 | 0.67 | |||||||||
| 19 | 0.517 | 0.62 | |||||||||
| 20 | 0.505 | 0.45 | |||||||||
| 21 | 0.690 | 0.50 | 0.38 | ||||||||
| 22 | 0.676 | 0.66 | |||||||||
| 24 | 0.572 | 0.41 | |||||||||
| 25 | 0.685 | 0.76 | |||||||||
| 26 | 0.639 | 0.77 | |||||||||
| 27 | 0.672 | 0.74 | |||||||||
| 39 | 0.632 | 0.70 | |||||||||
| 28 | 0.538 | 0.58 | |||||||||
| 36 | 0.542 | 0.51 | |||||||||
| 41 | 0.520 | 0.54 | |||||||||
| 42 | 0.495 | 0.45 | 0.32 | ||||||||
| 43 | 0.566 | 0.32 | 0.56 | ||||||||
| 47 | 0.625 | 0.36 | 0.39 | ||||||||
| 48 | 0.564 | 0.38 | 0.47 | ||||||||
| 50 | 0.506 | 0.35 | |||||||||
| 54 | 0.550 | 0.54 | |||||||||
| 55 | 0.542 | 0.51 | |||||||||
| 56 | 0.578 | 0.58 | |||||||||
| 57 | 0.565 | 0.31 | 0.51 | ||||||||
| 59 | 0.602 | 0.49 | |||||||||
| 61 | 0.596 | 0.74 | |||||||||
| 62 | 0.554 | 0.54 | |||||||||
| 64 | 0.567 | 0.58 | |||||||||
| 66 | 0.575 | 0.67 | |||||||||
| 67 | 0.637 | 0.76 | |||||||||
| 69 | 0.670 | 0.54 | |||||||||
| 71 | 0.568 | 0.62 | |||||||||
| 73 | 0.533 | ||||||||||
| 74 | 0.661 | 0.53 | |||||||||
| 75 | 0.695 | 0.52 | |||||||||
| 76 | 0.544 | 0.51 | |||||||||
| 78 | 0.522 | 0.30 | 0.36 | ||||||||
| 83 | 0.547 | 0.48 | |||||||||
| 84 | 0.562 | 0.40 | |||||||||
| 85 | 0.644 | 0.59 | |||||||||
| 86 | 0.654 | 0.52 | 0.37 | ||||||||
| 88 | 0.601 | 0.37 | |||||||||
| 89 | 0.652 | 0.40 | |||||||||
| 90 | 0.711 | 0.76 | |||||||||
| 91 | 0.718 | 0.82 | |||||||||
| 92 | 0.663 | 0.74 | |||||||||
| 93 | 0.548 | 0.40 | |||||||||
| 96 | 0.619 | 0.35 | 0.32 | 0.46 | |||||||
| 98 | 0.564 | 0.70 | |||||||||
| 106 | 0.815 | 0.87 | |||||||||
| 107 | 0.827 | 0.88 | |||||||||
| Model | Normed χ2 | Comparative Fit Index (CFI) | Tucker Lewis Index (TLI) | Root-Mean Squared Residual (SRMR) | Root-Mean Square Error of Approximation (RMSEA) |
|---|---|---|---|---|---|
| Model 1 (45 variables) | 2.068 | 0.757 | 0.736 | 0.1041 | 0.075 |
| Model 2 (35 variables) Exclusion of items with loadings below < 0.50 | 1.968 | 0.849 | 0.829 | 0.0820 | 0.071 |
| Model 3 (31 variables) Exclusion of items with loadings < 0.60 | 1.960 | 0.878 | 0.857 | 0.0796 | 0.071 |
| Model 4 (27 variables) Exclusion of items with loadings < 0.70 | 1.752 | 0.913 | 0.915 | 0.0628 | 0.063 |
| Model 5 (23 variables) | 1.619 | 0.937 | 0.923 | 0.0569 | 0.057 |
| Domain | Housing | Social Participation | Respect and Social Inclusion | Civic Participation and Employment | Communication and Information | Community Support and Health Services | Outdoor Spaces and Buildings | Transportation | Financial Situation |
|---|---|---|---|---|---|---|---|---|---|
| Composite Reliability | 0.85 | 0.85 | 0.74 | 0.74 | 0.76 | 0.88 | 0.83 | 0.88 | 0.93 |
| Scales and Domains | AFEAT | AFEAT—Housing | AFEAT—Social Participation | AFEAT—Civic Participation and Employment | AFEAT—Communication and Information | AFEAT—Transportation |
|---|---|---|---|---|---|---|
| AFCCQ total | 0.748 ** | |||||
| AFCCQ—Housing | 0.416 ** | 0.561 ** | 0.309 ** | 0.243 ** | 0.200 ** | 0.292 ** |
| AFCCQ—Social participation | 0.613 ** | 0.366 ** | 0.626 ** | 0.456 ** | 0.380 ** | 0.328 ** |
| AFCCQ—Civic participation and employment | 0.516 ** | 0.290 ** | 0.225 ** | 0.444 | 0.356 ** | 0.306 ** |
| AFCCQ—Communication and information | 0.480 ** | 0.310 ** | 0.373 ** | 0.375 ** | 0.456 ** | 0.347 ** |
| AFCCQ—transportation | 0.507 ** | 0.532 ** | 0.298 ** | 0.261 ** | 0.251 ** | 0.551 ** |
| Scale and Domains of the AFCCQ | Colour Scheme Principle | Mean | SD | Variance | Range | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| − − − − | − − − | − − | − | + | ++ | +++ | ++++ | |||||
| AFCCQ Total score | ≤−35.1 | −23.1–−35.0 | −11.5–−23.0 | −11.4–0.0 | 0.1–11.4 | 11.5–23.0 | 23.1–35.0 | ≥35.1 | 13.3 | 7.86 | 61.7 | 66 |
| Housing | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 | 2.3 | 1.4 | 1.1 | 6 |
| Social participation | ≤−6.1 | −4.1–−6.0 | −2.1–−4.0 | −2.0–0.0 | 0.1–2.0 | 2.1–4.0 | 4.1–6.0 | ≥6.1 | 2.5 | 1.0 | 5.8 | 8 |
| Respect and social inclusion | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 | 1.6 | 1.5 | 2.5 | 8 |
| Civic participation and employment | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 | 1.4 | 1.3 | 1.7 | 8 |
| Communication and information | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 | 1.4 | 1.3 | 1.6 | 8 |
| Community support and health services | ≤−7.6 | −5.1–−7.5 | −2.6–−5.0 | −2.5–0.0 | 0.1–2.5 | 2.6–5.0 | 5.1–7.5 | ≥7.6 | 2.5 | 2.9 | 8.2 | 20 |
| Outdoor spaces and buildings | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 | 0.9 | 1.4 | 1.9 | 8 |
| Transportation | ≤−3.1 | −2.1–−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 | 1.7 | 1.5 | 2.2 | 8 |
| Financial situation | ≤−3.1 | −2.1−3.0 | −1.1–−2.0 | −1.0–0.0 | 0.1–1.0 | 1.1–2.0 | 2.1–3.0 | ≥3.1 | 1.8 | 1.3 | 1.6 | 6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dikken, J.; van den Hoven, R.F.M.; van Staalduinen, W.H.; Hulsebosch-Janssen, L.M.T.; van Hoof, J. How Older People Experience the Age-Friendliness of Their City: Development of the Age-Friendly Cities and Communities Questionnaire. Int. J. Environ. Res. Public Health 2020, 17, 6867. https://doi.org/10.3390/ijerph17186867
Dikken J, van den Hoven RFM, van Staalduinen WH, Hulsebosch-Janssen LMT, van Hoof J. How Older People Experience the Age-Friendliness of Their City: Development of the Age-Friendly Cities and Communities Questionnaire. International Journal of Environmental Research and Public Health. 2020; 17(18):6867. https://doi.org/10.3390/ijerph17186867
Chicago/Turabian StyleDikken, Jeroen, Rudy F.M. van den Hoven, Willeke H. van Staalduinen, Loes M.T. Hulsebosch-Janssen, and Joost van Hoof. 2020. "How Older People Experience the Age-Friendliness of Their City: Development of the Age-Friendly Cities and Communities Questionnaire" International Journal of Environmental Research and Public Health 17, no. 18: 6867. https://doi.org/10.3390/ijerph17186867