Return to Work Interventions for Cancer Survivors: A Systematic Review and a Methodological Critique

 , , , , ,
, , , , ,
Abstract
:1. Introduction
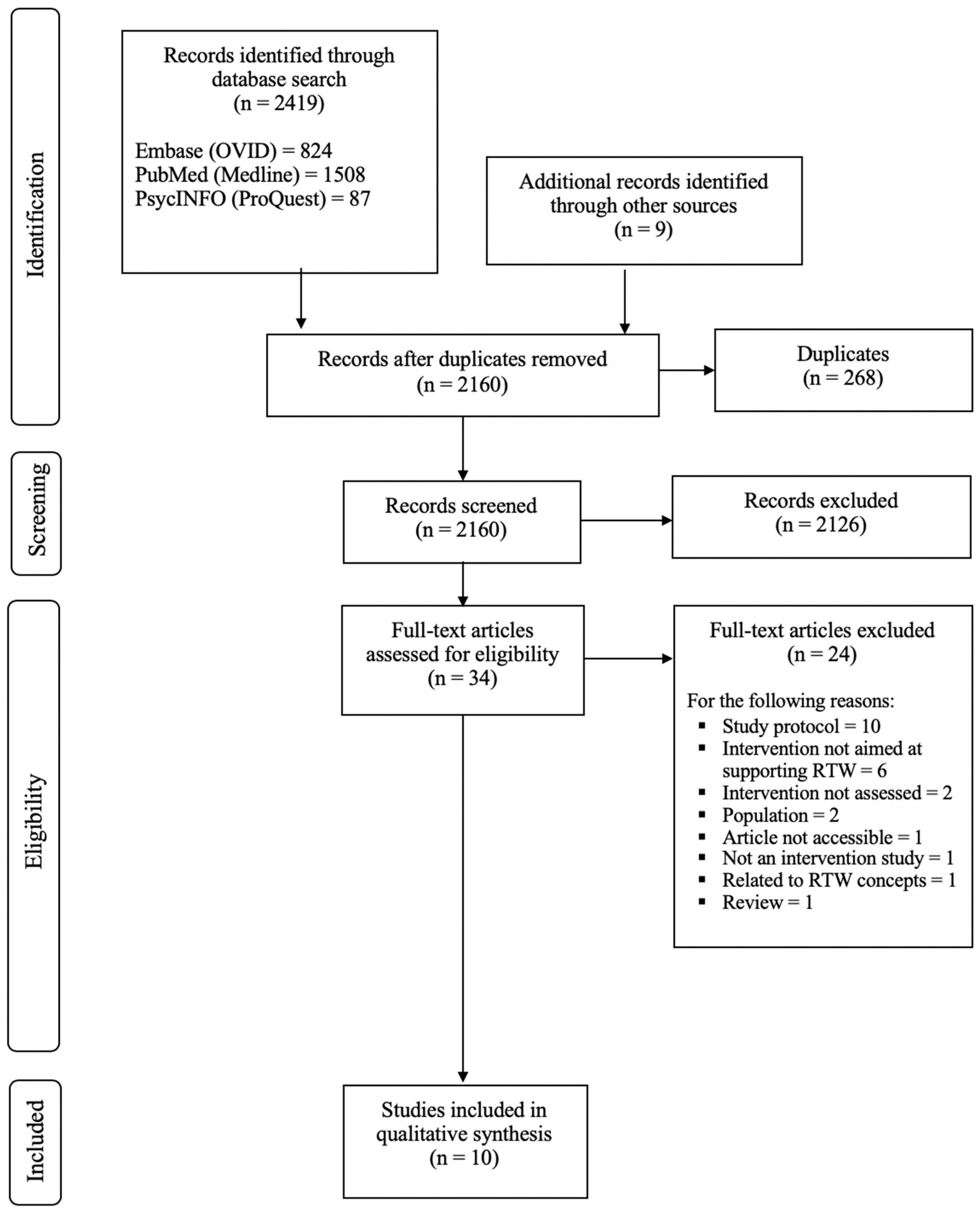
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Critical Appraisal of Study Quality
3. Results
3.1. Study Design and Participant Characteristics
3.2. Quality Assessment of the Included Studies
3.3. Intervention Theoretical Framework and Program Development
3.4. RTW Interventions
3.4.1. Hospital Rehabilitation Programs
3.4.2. Interventions Outside the Hospital
3.4.3. Combined Hospital and Outside Hospital Interventions
3.5. Intervention Effects or Results: Primary and Secondary Outcomes Measured in the Included Studies
3.5.1. Primary Outcomes: Work-Related Outcome Results
3.5.2. Secondary Outcome Results
3.5.3. Qualitative Results
4. Discussion
- 1.
- Define the concept of return to work (RTW): a systematic review on RTW and how researchers, health agencies and ministries consider or assess RTW should be realized. A work group should be created with international experts on RTW, employers and cancer survivors to define clearly what RTW means after a chronic disease.
- 2.
- Define how to assess RTW: based on the results found in the literature, the most appropriate way(s) to assess RTW should be defined. Researchers should answer the following question: RTW should be evaluated equally or with different variables from one condition to another?
- 3.
- Explore the literature and take into consideration the appropriate variables: researchers should target their intervention for a specific population and take into account several variables (e.g., age, tumor location, socioeconomic status) when designing their intervention.
- 4.
- Include appropriate people: healthcare professionals, employers, patients or survivors, and representatives of health agencies should be included when designing an intervention or in the intervention program.
- 5.
- Write an intervention program manual for professionals: A detailed manual presenting the steps followed by healthcare professionals when conducting the intervention should be provided. It will allow researchers to communicate easier on their programs and to adapt it to clinical practice.
- 6.
- Pre-test the intervention with few participants, then pilot-test the intervention before to test the efficacy of the program.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Global Cancer Observatory World Fact Sheets. 2018. Available online: http://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf (accessed on 28 December 2018).
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Cancer in Australia 2017. Available online: https://www.aihw.gov.au/getmedia/3da1f3c2-30f0-4475-8aed-1f19f8e16d48/20066-cancer-2017.pdf.aspx?inline=true (accessed on 10 September 2018).
- Maddams, J.; Utley, M.; Moller, H. Projections of cancer prevalence in the United Kingdom, 2010–2040. Br. J. Cancer 2012, 107, 1195–1202. [Google Scholar] [CrossRef]
- National Cancer Institute. Age and Cancer Risk. 2015. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/age (accessed on 10 September 2018).
- Mols, F.; Vingerhoets, A.J.; Coebergh, J.W.; van de Poll-Franse, L.V. Quality of life among long-term breast cancer survivors: A systematic review. Eur. J. Cancer 2005, 41, 2613–2619. [Google Scholar] [CrossRef]
- Tamminga, S.J.; Bültmann, U.; Husson, O.; Kuijpens, J.L.P.; Frings-Dresen, M.H.W.; De Boer, A.G.E.M. Employment and insurance outcomes and factors associated with employment among long-term thyroid cancer survivors: A population-based study from the PROFILES registry. Qual. Life Res. 2016, 25, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Stergiou-Kita, M.; Grigorovich, A.; Tseun, V.; Milosevic, E.; Hebert, D.; Phan, S.; Jones, J. Qualitative meta-synthesis of survivors’ work experiences and the development of strategies to facilitate return to work. J. Cancer Surviv. 2014, 8, 657–670. [Google Scholar] [CrossRef]
- Roelen, C.A.; Koopmans, P.C.; van Rhenen, W.; Groothoff, J.W.; van der Klink, J.J.; Bultmann, U. Trends in return to work of breast cancer survivors. Breast Cancer Res. Treat. 2011, 128, 237–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, A.G.E.M.; Taskila, T.; Ojajärvi, A.; van Dijk, F.J.H.; Verbeek, J.H.A.M. Cancer survivors and unemployment—A meta-analysis and meta-regression. JAMA 2009, 301, 753–762. [Google Scholar] [CrossRef]
- The Statistical Portal. Unemployment Rate in Member States of the European Union in June 2018 (Seasonally Adjusted). 2018. Available online: https://www.statista.com/statistics/268830/unemployment-rate-in-eu-countries/ (accessed on 10 September 2018).
- Tranding Economics. United States Unemployment Rate. 2018. Available online: https://tradingeconomics.com/united-states/unemployment-rate (accessed on 10 September 2018).
- Organisation for Economic Co-Operation and Development [OECD]. Sickness, Disability and Work. Breaking the Barriers. A Synthesis of Findings across OECD Countries. 2010. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=3&ved=2ahUKEwjq_fyLprHdAhUJx4UKHc8TA84QFjACegQICRAC&url=https%3A%2F%2Fmoodle.adaptland.it%2Fpluginfile.php%2F20577%2Fmod_data%2Fcontent%2F39060%2Fdisability_synthesis_2010_en%2520.pdf&usg=AOvVaw0-JjZ5iPm91Rt53uQ9I2Dt (accessed on 10 September 2018).
- Danish Ministry of Health. Program for Rehabilitation and Palliation in Cancer Treatment. 2018. Available online: http://www.sst.dk/~/media/B0FD5078B1654B33A9E744CCBAE89022.ashx (accessed on 10 September 2018).
- Duijts, S.F.; van Egmond, M.P.; Spelten, E.; van Muijen, P.; Anema, J.R.; van der Beek, A.J. Physical and psychosocial problems in cancer survivors beyond return to work: A systematic review. Psychooncology 2013, 23, 481–492. [Google Scholar] [CrossRef]
- Tikka, C.; Verbeek, J.; Tamminga, S.; Leensen, M.; De Boer, A. Rehabilitation and Return to Work after Cancer: Literature Review; Publications Office of the European Union: Luxembourg, 2017; Available online: https://osha.europa.eu/en/tools-and-publications/publications/rehabilitation-and-return-work-after-cancer-literature-review (accessed on 10 September 2018).
- Australian Government. What Is Return to Work? Available online: https://www.comcare.gov.au/__data/assets/pdf_file/0016/117061/What_is_Return_to_Work_concept_paper_PDF_82.9_KB.pdf (accessed on 28 December 2019).
- Nitkins, P.; Parkinson, M.; Schultz, I. Cancer and Work: A Canadian Perspective. 2011. Available online: http://www.capo.ca/pdf/CancerandWork-ACanadianPerspective.pdf (accessed on 10 September 2018).
- Carlsen, K.; Harling, H.; Pedersen, J.; Christensen, K.B.; Osler, M. The transition between work, sickness absence and pension in a cohort of Danish colorectal cancer survivors. BMJ Open 2013, 3, e002259. [Google Scholar] [CrossRef] [Green Version]
- Morrison, T.; Thomas, R. Survivors’ experiences of return to work following cancer: A photovoice study. Can. J. Occup. Ther. 2014, 81, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Tiedtke, C.; de Rijk, A.; Dierckx de Casterle, B.; Christiaens, M.-R.; Donceel, P. Experiences and concerns about ‘returning to work’ for women breast cancer survivors: A literature review. Psychooncology 2010, 19, 677–683. [Google Scholar] [CrossRef]
- Stergiou-Kita, M.; Pritlove, C.; Holness, D.L.; Kirsh, B.; van Eerd, D.; Duncan, A.; Jones, J. Am I ready to return to work? Assisting cancer survivors to determine work readiness. J. Cancer Surviv. 2016, 10, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Tamminga, S.J.; de Boer, A.G.; Verbeek, J.H.; Frings-Dresen, M.H. Breast cancer patients’ views of factors that influence the return-to-work process—A qualitative study. Scand. J. Work Environ. Health 2012, 38, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Taskila, T.; Lindbohm, M.L.; Martikainen, R.; Lehto, U.S.; Hakanen, J.; Hietanen, P. Cancer patients’ received and needed social support from their work place and the occupational health services. Support. Care Cancer 2006, 14, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Hoving, J.L.; Broekhuizenn, M.L.A.; Frings-Dresen, M.H.W. Return to work of breast cancer survivors: A systematic review of intervention studies. BMC Cancer 2009, 9, 117. [Google Scholar] [CrossRef]
- De Boer, A.G.E.M.; Taskila, T.K.; Tamminga, S.J.; Feuerstein, M.; Frings-Dresen, M.H.W.; Verbeek, J.H. Interventions to enhance return-to-work for cancer patients. Cochrane Database Syst. Rev. 2015, 16, CD007569. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Cohort Study Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Cohort-Study-Checklist.pdf (accessed on 10 September 2018).
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist.pdf (accessed on 10 September 2018).
- Critical Appraisal Skills Programme. CASP Randomised Controlled Trial Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Randomised-Controlled-Trial-Checklist.pdf (accessed on 10 September 2018).
- Bains, M.; Munir, F.; Yarker, J.; Steward, W.; Thomas, A. Return-to-work guidance and support for colorectal cancer patients: A feasibility study. Cancer Nurs. 2011, 34, E1–E12. [Google Scholar] [CrossRef]
- Hubbard, G.; Gray, N.M.; Ayansina, D.; Evans, J.M.M.; Kyle, R.G. Case management vocational rehabilitation for women with breast cancer after surgery: A feasibility study incorporating a pilot randomized controlled trial. Trials 2013, 14, 175. [Google Scholar] [CrossRef]
- Leensen, M.C.J.; Groeneveld, I.F.; van der Heide, I.; Rejda, T.; van Veldhoven, P.L.J.; van Berkel, S.; Snoek, A.; Harten, W.V.; Frings-Dressen, M.H.W.; de Boer, A.G.E.M. Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: A prospective study in the Netherlands. BMJ Open 2017, 7, e014746. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; Bos-Ransdorp, B.; Uitterhoeve, L.L.J.; Sprangers, M.A.G.; Verbeek, J.H.A.M. Enhanced provider communication and patient education regarding return to work in cancer survivors following curative treatment: A pilot study. J. Occup. Rehabil. 2006, 16, 647–657. [Google Scholar] [CrossRef]
- Oldervoll, L.M.; Thorsen, L.; Kaasa, S.; Fossa, S.D.; Dahl, A.A.; Smastuen, M.C.; Nystad, R.; Hokstad, A.; Smeland, S.; Loge, J.H. Inpatient versus outpatient rehabilitation after breast and gynecological cancers—A comparative study. Int. J. Phys. Med. Rehabil. 2014, 2, 2. [Google Scholar] [CrossRef]
- Rusbridge, S.L.; Walmsley, N.C.; Griffiths, S.B.; Wilford, P.A.; Rees, J.H. Predicting outcomes of vocational rehabilitation in patients with brain tumours. Psychooncology 2013, 22, 1907–1911. [Google Scholar] [CrossRef]
- Schumacher, L.; Armaou, M.; Rolf, P.; Sadhra, S.; Sutton, A.J.; Zarkar, A.; Grunfeld, E.A. Usefulness and engagement with a guided workbook intervention (WorkPlan) to support work related goals among cancer survivors. BMC Psychol. 2017, 5, 34. [Google Scholar] [CrossRef]
- Tamminga, S.J.; Verbeek, J.H.A.M.; Bos, M.M.E.M.; Fons, G.; Kitzen, J.J.E.M.; Plaisier, P.W.; Frings-Dressen, M.H.; de Boer, A.G.E.M. Effectiveness of a hospital-based work support intervention for female cancer patients—A multi-centre randomised controlled trial. PLoS ONE 2013, 8, e63271. [Google Scholar] [CrossRef]
- Thorsen, L.; Dahl, A.A.; Nystad, R.; Kiserud, C.E.; Geirdal, A.; Smeland, S. Baseline characteristics in female cancer patients with unimproved work status after an outpatient rehabilitation program and health changes during the intervention. SpringerPlus 2016, 5, 1009. [Google Scholar] [CrossRef]
- Van Egmond, M.P.; Duijts, S.F.A.; Jonker, M.A.; van der Beek, A.J.; Anema, J.R. Effectiveness of a tailored return to work program for cancer survivors with job loss: Results of a randomized controlled trial. Acta Oncol. 2016, 55, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Czajkowski, S.M.; Powell, L.H.; Adler, N.; Naar-King, S.; Reynolds, K.D.; Hunter, C.M.; Laraia, B.; Olster, D.H.; Perna, F.M.; Peterson, J.C.; et al. From Ideas to Efficacy: The ORBIT Model for Developing Behavioral Treatments for Chronic Diseases. Health Psychol. 2016, 34, 971–982. [Google Scholar] [CrossRef]
- Ogez, D.; Péloquin, K.; Bertout, L.; Bourque, C.-J.; Curnier, D.; Drouin, S.; Laverdière, C.; Marcil, V.; Ribeiro, R.; Callaci, M.; et al. Psychosocial intervention programs for parents of children with cancer: A systematic review and critical comparison of programs’ models and development. J. Clin. Psychol. Med. Settings 2019. forthcoming. [Google Scholar] [CrossRef]
- Wang, L.; Hong, B.Y.; Kennedy, S.A.; Chang, Y.; Hong, C.J.; Craigie, S.; Kwon, H.Y.; Romerosa, B.; Couban, R.J.; Reid, S.; et al. Predictors of Unemployment After Breast Cancer Surgery: A Systematic Review and Meta-Analysis of Observational Studies. J. Clin. Oncol. 2018, 36, 1868–1879. [Google Scholar] [CrossRef]
- Nilsson, M.I.; Petersson, L.-M.; Wennman-Larsen, A.; Olsson, M.; Vaez, M.; Alexanderson, K. Adjustment and social support at work early after breast cancer surgery and its associations with sickness absence. Psychooncology 2013, 22, 2755–2762. [Google Scholar] [CrossRef] [PubMed]
- Amir, Z.; Wynn, P.; Chan, F.; Strauser, D.; Whitaker, S.; Luker, K. Return to Work After Cancer in the UK: Attitudes and Experiences of Line Managers. J. Occup. Rehabil. 2010, 20, 435–442. [Google Scholar] [CrossRef]
- Stergiou-Kita, M.; Pritlove, C.; van Eerd, D.; Holness, L.D.; Kirsh, B.; Duncan, A.; Jones, J. The provision of workplace accommodations following cancer: Survivor, provider, and employer perspectives. J. Cancer Surviv. 2016, 10, 489–504. [Google Scholar] [CrossRef] [PubMed]
- Tiedtke, C.; Dierckx de Casterlé, B.; Donceel, P.; de Rijk, A. Workplace support after breast cancer treatment: Recognition of vulnerability. Disabil. Rehabil. 2015, 37, 1770–1776. [Google Scholar] [CrossRef] [PubMed]
- MacKay, G.; Knott, V.; Delfabbo, P. Return to work and cancer: The Australian experience. J. Occup. Rehabil. 2013, 23, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Morrison, T.; Thomas, R.; Guitard, P. Physicians’ perspectives of cancer survivors’ work integration. Can. Fam. Physician 2015, 61, e36–e42. [Google Scholar]
- Davidson, L.; White, W. The concept of recovery as an organizing principle for integrating mental health and addiction services. J. Behav. Health Serv. Res. 2007, 34, 109–120. [Google Scholar] [CrossRef]
- Jacob, K.S. Recovery model of mental illness: A complementary approach to psychiatric care. Jacob KS. Recovery model of mental illness: A complementary approach to psychiatric care. Indian J. Psychol. Med. 2015, 37, 117–119. [Google Scholar] [CrossRef]
- Tourette-Turgis, C. Recovering, self-healing and self-reconstruction: How to integrate the dynamics of the concept of recovery in cancer survivorship care? Sujet Cité 2017, 8, 223–238. [Google Scholar]
- Silvaggi, F.; Leonardi, M.; Guastafierro, E.; Quintas, R.; Toppo, C.; Foucaud, J.; Lamore, K.; Rothe, U.; Scaratti, C. Chronic diseases & employment: An overview of existing training tools for employers. Int. J. Environ. Res. Public Health 2019, 16, 718. [Google Scholar]
- Munir, F.; Kalawsky, K.; Wallis, D.J.; Donaldson-Feilder, E. Using intervention mapping to develop a work-related guidance tool for those affected by cancer. BMC Public Health 2013, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Stapelfeldt, C.M.; Labriola, M.; Jensen, A.B.; Andersen, N.T.; Momsen, A.-M.H.; Nielsen, C.V. Municipal return to work management in cancer survivors undergoing cancer treatment: A protocol on a controlled intervention study. BMC Public Health 2015, 15, 720. [Google Scholar] [CrossRef] [PubMed]
- Tamminga, S.J.; Hoving, J.L.; Frings-Dresen, M.H.W.; de Boer, A.G.E.M. Cancer@Work—A nurse-led, stepped-care, e-health intervention to enhance the return to work of patients with cancer: Study protocol for a randomized controlled trial. Trials 2016, 17, 453. [Google Scholar] [CrossRef] [PubMed]
- Wienert, J.; Schwarz, B.; Bethge, M. Effectiveness of work-related medical rehabilitation in cancer patients: Study protocol of a cluster-randomized multicenter trial. BMC Cancer 2016, 6, 544. [Google Scholar] [CrossRef] [PubMed]
- Zaman, A.-C.G.N.M.; Tytgat, K.M.A.J.; Klinkenbijl, J.H.G.; Frings-Dresen, M.H.W.; de Boer, A.G.E.M. Design of a multicentre randomized controlled trial to evaluate the effectiveness of a tailored clinical support intervention to enhance return to work for gastrointestinal cancer patients. BMC Cancer 2016, 16, 303. [Google Scholar] [CrossRef]
- Wells, M.; Williams, B.; Firnigl, D.; Lang, H.; Coyle, J.; Kroll, T.; MacGillivray, S. Supporting “work-related goals” rather than “return to work” after cancer? A systematic review and meta-synthesis of 25 qualitative studies. Psychooncology 2013, 22, 1208–1219. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Number | References |
|---|---|---|
| Country of publication | ||
| Netherlands | 4 | [35,36,40,42] |
| United-Kingdom | 4 | [33,34,38,39] |
| Norway | 2 | [37,41] |
| Intervention adapted to one cancer type | ||
| Yes | 3 | [33,34,38] |
| No | 7 | [35,36,37,39,40,41,42] |
| Studies design | ||
| Longitudinal study | 3 | [35,36,37] |
| Quasi-experimental study | 3 | [33,38,41] |
| Randomized control trial | 3 | [34,40,42] |
| Qualitative study | 1 | [39] |
| Participants | ||
| Women | 425 | - |
| Men | 74 | - |
| Total | 499 | - |
| Cohort Studies | Q1 | Q2 | ? | Q3 | Q4 | Q5a | Q5b | Q5a | Q6b | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 |
| Bains et al. (2011) [33] |  |  | | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Leesen et al. (2017) [35] | | | | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Nieuwenhuijsen et al. (2006) [36] | | | | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Oldervoll et al. (2014) [37] | | | | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Rusbridge et al. (2013) [38] | | | | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Thorsen et al. (2016) [41] | | | | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Randomized controlled trial studies | Q1 | Q2 | Q3 | ? | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | |||
| Hubbard et al. (2013) [34] | | | | | | +/− | | | | | | | |||
| Tamminga et al., (2013) [40] | | | | | | | | | | | | | |||
| Van Egmond et al. (2016) [42] | | | | | | | | | | | | | |||
| Qualitative studies | Q1 | Q2 | ? | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | ||||
| Schumacher et al. (2017) [39] | | | | | | | +/− | | | | |
= yes or strong; = no or weak; +/− = can’t tell; NA = not administered.| [Ref.] Author (year), Country | Cancer Site | Objectives of Intervention | Theoretical Framework | Intervention Methods | Structure of Intervention | Number and Discipline of Trainer or Counsellors |
|---|---|---|---|---|---|---|
| [33] Bains et al. (2011), United Kingdom | Colorectal (100%) | To provide work-related advice. | Based on RTW literature and work related guidelines offered by national cancer charitable organizations on information provided to patients. | An individual return to work (RTW) consultation and a ‘Managing Cancer and Employment’ educational leaflet were provided to the participants. The consultation included tailored advice based on the individual’s type of treatment and nature of his/her work (manual/nonmanual). The intervention leaflet was designed to offer information to patients according to whether they were employed in a manual or nonmanual job on the following aspects: managing symptoms at work, communication with employer, and work ability during and after treatment. | One-to-one RTW guidance verbally and in the form of a written educational leaflet. | A researcher provided individual RTW consultation. |
| [34] Hubbard et al. (2013), United Kingdom | Breast (100%) | To assess patients’ needs and to provide adapted support to help them RTW. | Based on the bio-psycho-social model. | First, patients had to complete a questionnaire assessing individual needs to enable RTW, then assessed by phone consultation. Based on this assessment, individuals were referred to relevant services that could support them with cancer-related and treatment side effects. Participants also received a booklet on ‘Work and Cancer’. | One phone consultation with a working health professional followed by a different combination of intervention adapted to the patient’s needs. | Working Health Services. |
| [35] Leensen et al. (2017), Netherlands | Breast (83.9%), colorectal (8.9%), non-Hodgkin’s lymphoma (5.4%) and other localization (2.2%, not specified) | To increase the likelihood of a timely and enduring RTW in cancer patients. | Based on scientific literature and interviews with care providers in the field of occupational health, oncology, sports medicine and physio-therapy. | Before the program, a sports medical assessment was realized. Then, physical training was proposed to the participants (ergometer and resistance exercises of the large muscle groups). Exercises were performed ranging from two series of eight repetitions to three series of 12 repetitions with increasing weight. Alongside the exercise program, participants received 1 to 3 individual counselling sessions on work resumption and work ability. | Twelve weeks of physical training, twice a week for a maximum of 1 hour per session. | An oncology occupational physician, a sport physician and physiotherapist. |
| [36] Nieuwenhuijsen et al. (2006), Netherlands | Breast (50%), male genitals (15%), female genitals (12%), gastro-intestinal (15%) and 12% other | To enhance the communication of information between the patient and the occupational physician on the illness and RTW. | Based upon the principles of graded activity and goal-setting. | First, the letters sent routinely to the general practitioner (on the disease and treatments) were sent to the occupational physician. Then, an educational leaflet containing 10 steps that cancer survivors can undertake to enhance their RTW was given (e.g., draw up an RTW plan). | An education leaflet was given to patients. There was no limited time in its use. | A radiation oncologist. |
| [37] Oldervoll et al. (2014), Norway | Breast (70%) and gynecological (30%) | To reduce drop-out from the work force by providing physical, psychological and social support. | No information provided. | The intervention can be proposed to inpatients and outpatients. The intervention consists in physical exercise, patient education and group discussions. Patient education themes: (1) cancer treatment and its side-effects; (2) physical activity; (3) nutrition; (4) economy and work situation including patient rights within the welfare system; (5) factors that can contribute to a permanent RTW for cancer patients; (6) partnership and sexuality; (7) psychological reactions in relation to cancer; and (8) distress management and coping strategies. These themes were then discussed in group discussions. Patients could also bring new subjects of discussion during these groups. | Inpatient program: Four weeks (three weeks stay and one more week 8 to 12 weeks later to increase patient’s motivation) Outpatient program: seven weeks (5 hours per day) Every day, patients had physical exercises to perform, patient education and group discussions. | At least one social worker, one health professional, one physiotherapist and one sport instructor. |
| [38] Rusbridge et al. (2013), United Kingdom | Brain (100%) | To support patients to overcome the barriers faced when returning to work or remaining in work. | No information provided. | Support was adapted to patients needs after an initial assessment of patients’ impairment and job demand to establish short and long-term goals. Interventions took the form of patient-based symptom management (e.g., fatigue, relaxation) and workplace intervention (e.g., scheduling, strategies to manage memory impairment). A professional contacted the employer to suggest specific workload adaptations, created RTW plan and accompany patients to adopt strategies adapted to their work. | An average of 11 hours sessions in 5 months | An occupational therapist and a neuropsychologist. |
| [39] Schumacher et al. (2017), United Kingdom | Breast (52%), urological (30%), bowel (13%) and gynecological (4%) | To support RTW. | Based on self-regulation model and goal-setting theories and scientific literature. | A work-book was given to the patients. It was composed of 4 chapters and included activities to encourage thoughts/beliefs about cancer and how it could affect work, develop goals around RTW with small achievable steps, culminating in the creation of a RTW plan. Two support phone consultations at week 2 and 4 gave participants the opportunity to discuss their progress, ask questions about items they found difficult, and seek clarification on any of the workbook content. | Four weeks (but there was no real limit time in its use). | Not specified. |
| [40] Tamminga et al., (2013), Netherlands | Breast, (64%) cervix (23%), ovarian (5%), vulva (3%) and other (5%, not specified) | To support RTW and improve quality of life. | Based on the shared care model, scientific literature and interview with both cancer survivors and professionals. | The intervention was composed of three steps: (1) delivering patient education and support at the hospital, as part of usual psycho-oncology care (4 meetings of 15 minutes); (2) improving communication between the treating physician and the occupational physician by sending at least one letter; (3) drawing-up a RTW plan in collaboration with the employer. | Maximum of 14 months | An occupational physician, an oncology nurse and a medical social worker. |
| [41] Thorsen et al. (2016), Norway | Breast (60%), gynecological (31%), lymphoma (7%) and esophagus (1%) | To improve work ability and health related quality of life. | The program was initiated by the Norwegian government. However, no information on intervention design and theoretical framework are provided. | At the start and end of the program, each patient had a consultation with a social worker focusing on individual goals for the program period. Each day, the program started with a patient education session for 2 h. These sessions covered topics related to cancer treatment, side effects, partnership and sexuality, economy and work situation, nutrition, physical exercise and coping strategies. The patient education was followed by 1-h group discussion of the topic presented. After lunch the participants performed physical activity (e.g., Nordic walking, water gymnastics, yoga) for 60–120 min. | Full day weekly for 7 weeks | A least one social worker, one physiotherapist, one nurse and one physician (a radiotherapist). |
| [42] van Egmond et al. (2016), Netherlands | Breast (39.8%), lung (1.8%), gynecological (4.1%), colon (7.6%), gastro-intestinal (5.8%), head and neck (4.7%), prostate (1.8%), hematological (13.5%), brain (4.7%) and other type of cancer (14%, not specified) | To support RTW after job loss. | Based on the attitude-social influence-efficacy theoretical model, scientific literature and focus groups with cancer survivors. | First, an introductory interview was conducted to discuss RTW plans and assess whether the patients were actively involved in looking for jobs or not involved in RTW activities. Then, patients were allocated to one of the following routes. - Route 1: If patients were involved in RTW activities, participants were placed in therapeutic or paid work with the support of two job hunting agencies. - Route 2: If patients were not involved in RTW activities, participants were helped to RTW (e.g., creation of a RTW plan) and coached on several themes (e.g., fatigue management, communication about cancer). The participants motivation to RTW was assessed after 4 session of coaching and several sessions later if the patients was not ready to RTW. If patients were ready to RTW, the intervention continued with route 1. If they were not ready to RTW after the intervention, they were referred to usual care. | Maximum of 4 months. | Job hunting agencies and re-integration agency (coaches). |
| [Ref.] Author (year), Country | Intervention Group | Control Group | Primary Outcome | Secondary Outcome | Follow-up Assessment | Main Results | ||
|---|---|---|---|---|---|---|---|---|
| N, n Female (%), n Male (%) | Socio-demographic Data (Age, Education, work Status) | N, n Female (%), n Male (%) | Socio-Demographic Data (Age, Education, Work Status) | |||||
| [33] Bains et al. (2011), United Kingdom | N = 13, female n = 5 (39%), male n = 8 (61%) | Mean age: 56.25 years (SD, 5,75) Level of education: low (23%) intermediate, (38.5%), high (38.5%) Work status: on sick leave (31%), continued to work during treatments (69%) | / | / | Current sickness leave status, return to work (RTW) intentions and perceived work ability | / | T0 (baseline) and T1 (6 months) | No significant effect of the intervention on work ability, self-efficacy, anxiety, and depressive symptoms. Nine patients found the intervention ‘useful’ or ‘very useful’. |
| [34] Hubbard et al. (2013), United Kingdom | N = 7 female | Mean age: 49.7 years (SD, 7.6) Level of education: NA Work status: full time (85.7%), part time (14.3%) | N=11 female | Mean age: 49.7 years (SD, 7.6) Level of education: NA Work status: full time (45.5%), part time (54.5%) | Self-reported sickness absence | Change in employment pattern, health related quality of life and fatigue | T1 (6 months) and T2 (12 months) | No significant differences observed on primary and secondary outcomes. |
| [35] Leensen et al. (2017), Netherlands | N = 93, female n = 84 (90.3%), male n = 9 (9.7%), | Mean age: 47.9 years (SD, 7.4) Level of education: low (14%), intermediate (33.3%) and high (52.7) Work status: on sick leave (100%) | / | / | Time to RTW between first date of sick leave and the first date of resumption | Perceptions regarding work (importance of work, work ability, self-efficacy regarding RTW and work limitations), physical factors (muscle strength, cardiorespiratory fitness, physical activity level and fatigue) and quality of life. | T0 (baseline), T1 (6 months), T2 (12 months) and T3 (18 months) | Regarding RTW: 59% of the participants RTW at T1, 86% at T2 and 83% at T3. Significant improvements (p < 0.05) were observed in the importance of work, work ability, RTW self-efficacy, fatigue and quality of life. |
| [36] Nieuwenhuijsen et al. (2006), Netherlands | N = 26, gemale n = 19 (73%), male n = 7 (27%) | Mean age: 45.8 years (SD, 6.5) Level of education: NA Work status: NA | / | / | Patients’ and occupational physicians’ satisfaction with the intervention | To examine the relation between adherence to the advice and RTW. | Not clear. RTW assessed at 6, 12 and 18 months | The leaflet was perceived as useful (score of 7 on 10). Regarding RTW: 65% of the participants RTW at 6 months, 89% at 12 months and 92% at 18 months. Level of adherence to the program is not significantly related to RTW. |
| [37] Oldervoll et al. (2014), Norway | N = 56 female | Inpatient program Mean age: 51 years Level of education: low to intermediary (44%), high (56%) Work status: full time (14%), part time (20%), sick-leave (66%) | N = 60 female | Outpatient program Mean age: 50 years Level of education: low to intermediary (55%), high (45%) Work status: full time (23%), part time (10%), sick-leave (67%) | Change in work status | Fatigue and health related quality of life | T0 (baseline), T1 (after the intervention) and T2 (6 months later) | In Inpatient group, 73% of patients on sick-leave or in part-time work improved their work status after the intervention. In Outpatient group, 76% of patients on sick-leave or in part-time work improved their work status after the intervention. There were no statistical differences between the two groups. Fatigue and health-related quality of life improved significantly between T0 and T2 in the two groups, but no statistical differences were observed between the groups. |
| [38] Rusbridge et al. (2013), United Kingdom | N = 34, female n = 15 (41%), male n = 19 (59%) | Mean age: 46 years (SD, 11) Level of education: low to intermediary (41%) and high (59%) Work status: working (32%) and not working (68%) | / | / | work status | Relations between work status after the intervention and demographic and tumor-related factors | T0 (baseline) and T1 (discharge) | More patients RTW after the intervention (p < 0.05). Furthermore, physical disability decreased the likelihood of RTW. |
| [39] Schumacher et al. (2017), United Kingdom | N = 23, female n = 16 (70%), male n = 7 (30%) | Mean age: 50 years Level of education: low to intermediary (41%) and high (59%) Work status: working (100%) | / | / | Work-related outcomes and utilization of the intervention | / | Interview four weeks after the intervention | Participants observed changes in their empowerment. The RTW plan was perceived as helpful to identify problems and solutions, but also to discuss with employers. Patients felt less anxious and uncertain about RTW. Patients thought the intervention should be conducted during the sole or final treatment. |
| [40] Tamminga et al., (2013), Netherlands | N = 56 female | N = 65 at the beginning of the intervention Mean age: 47.5 years (SD, 8.2) Level of education: low (11%), intermediary (59%) and high (30%) Work status: on sick leave (100%) | N = 59 female | N = 68 at the beginning of the study Mean age: 47.6 years (SD, 7.8) Level of education: low (16%), intermediary (51%) and high (33%) Work status: on sick leave (100%) | RTW and quality of life | Work ability, work productivity and cost | T0 (baseline), T1 (6 months) and T2 (12 months) | Regarding RTW: 79% of the participants RTW in both groups at 12 months (p < 0.05) and quality of life improved significantly over time but did not differ statistically between groups. Work ability improved significantly over time but did not differ significantly between groups. Work functioning did not improve significantly over time and did not differ significantly between groups. The costs did not differ statistically between groups. |
| [41] Thorsen et al. (2016), Norway | N = 106 female | Mean age: 48.82 years Level of education: low and intermediary (40.57%), high (59.43%) Work status: full time (9%), part time (9%), on sick-leave (76%), Work assessment allowance (5%) | / | / | To identify the proportion of female patients with unimproved work status 6 months after termination of the program | To identify demographic-, disease- and health-related characteristics at baseline associated with unimproved work status at follow-up. A third aim was to measure changes in health-related quality of life, fatigue and physical activity after completing the R-RTW program for patients with unimproved and improved work status. | T0 (baseline) and T1 (6 months after the program) | Regarding RTW: 64% of the participants had an improvement of their work status 6 months after the intervention. Participants with unimproved work status had a significantly higher proportion of paired relations and levels of fatigue compared to patients with improved work status. No significant differences were observed on other sociodemographic variables between unimproved and improved work status after the intervention. Health-related quality of life scores increased significantly after the intervention, for both women in unimproved and improved work status groups. |
| [42] van Egmond et al. (2016), Netherlands | N = 85 at inclusion, female n = 61 (71.8%), male n = 24 (28.2%) | Mean age: 47.9 years (SD, 8.5) Level of education: low (14.1%), intermediary (58.8%) and high (27.1%) Work status: unemployed (100%) | N = 86 at inclusion, female n = 57 (66.3%), male n = 829 (33.7%) | Mean age: 48.8 years (SD, 8.7) Level of education: low (20.9%), intermediary (44.2%) and high (34.9%) Work status: unemployed (100%) | Number of days between the day of inclusion and the first day of sustainable RTW | Rate of RTW per group, fatigue, quality of life and participation in society | T0 (baseline), T1 (3 months), T2 (6 months) and T3 (12 months) | No significant differences between the groups on the variables measured were observed. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamore, K.; Dubois, T.; Rothe, U.; Leonardi, M.; Girard, I.; Manuwald, U.; Nazarov, S.; Silvaggi, F.; Guastafierro, E.; Scaratti, C.; et al. Return to Work Interventions for Cancer Survivors: A Systematic Review and a Methodological Critique. Int. J. Environ. Res. Public Health 2019, 16, 1343. https://doi.org/10.3390/ijerph16081343
Lamore K, Dubois T, Rothe U, Leonardi M, Girard I, Manuwald U, Nazarov S, Silvaggi F, Guastafierro E, Scaratti C, et al. Return to Work Interventions for Cancer Survivors: A Systematic Review and a Methodological Critique. International Journal of Environmental Research and Public Health. 2019; 16(8):1343. https://doi.org/10.3390/ijerph16081343
Chicago/Turabian StyleLamore, Kristopher, Thomas Dubois, Ulrike Rothe, Matilde Leonardi, Isabelle Girard, Ulf Manuwald, Soja Nazarov, Fabiola Silvaggi, Erika Guastafierro, Chiara Scaratti, and et al. 2019. "Return to Work Interventions for Cancer Survivors: A Systematic Review and a Methodological Critique" International Journal of Environmental Research and Public Health 16, no. 8: 1343. https://doi.org/10.3390/ijerph16081343