1. Introduction
Urinary tract infection (UTI) is one of the most common infectious diseases and the main cause of community-acquired and nosocomial infections at admission [
1]. Patients with UTI usually present with acute clinical UTI or chronic uncomplicated or complicated UTI. Complicated UTI involve individuals with a condition or more resistant pathogen that increases the risk of failing treatment with functional, metabolic, or structural abnormalities [
2]. Moreover, the UTI incidence in women is much higher than that in men, but the majority are simple or uncomplicated UTI that occur in healthy or nonpregnant women [
3]. In women, the urethra is close to the vagina and rectum, which can lead to the unintentional introduction of fecal flora into the urinary tract, the most common cause of frequent occurrence of UTI. Furthermore, the risk of bacteria colonization increases in postmenopausal women because of the loss of vaginal pH physiological tuning ability [
4].
Lower UTI includes cystitis and prostatitis, and upper UTI include pyelonephritis. The Infectious Diseases Society of America observed a UTI prevalence of 1%–5% in healthy and premenopausal women and 1.9%–9.5% in pregnant women. Symptoms of lower urinary tract are common in men, and the prevalence increases with age. Up to 90% of men aged 50–80 years may suffer from troublesome lower urinary tract symptoms [
5].
Inflammation is a main factor in cancer development, but studies on the relationship between UTI and cancer risks are scant [
6]. A recent study demonstrated a relationship between UTI and genitourinary cancers (GUC) and confirmed that recurrent UTI are a risk factor for urinary bladder cancer [
7]. Moreover, the relationship between UTI and other tumors is important because UTI-caused inflammatory response is a systemic symptom. In addition, UTI can be diagnosed on the basis of a combination of symptoms and a positive urine analysis or culture [
8]. Thus, multiple antimicrobial therapies, including treatment with cephalosporin, quinolone, ampicillin, beta-lactam, amoxicillin, nitrofurantoin, sulfamethoxazole, and trimethoprim, can be prescribed [
9,
10]. Thus, using antibiotics is necessary for UTI treatment. Although evidence for the relationship between UTI and cancer risks is rare, it is reasonable to hypothesize that UTI disorders may still lead to cancers, especially GUC. Therefore, using a nationwide database, this study investigated the association between UTI and antibiotic usage influencing the risk of cancer.
2. Materials and Methods
2.1. Data Source
A national large-scale database, the Longitudinal Health Insurance Database (LHID), was used in this study. The 2010 LHID is a subset of the National Health Insurance Database, which is released by the National Health Research Institutes in Taiwan. The 2010 LHIRD, in which 1 million beneficiaries are randomly sampled from National Health Insurance (NHI) system, comprises the claims data of outpatient, admission, and prescription from 2009 to 2013. The NHI system is a single-payer social insurance system, and the coverage was approximately 98% in 2010. To protect the privacy of patients and care providers, the personnel identification numbers are scrambled for de-identification. The study was approved by the Ethical Review Board of Chung Shan Medical University Hospital (CSMU No.: 18096).
2.2. Patient Selection (Exposure of UTI Infection)
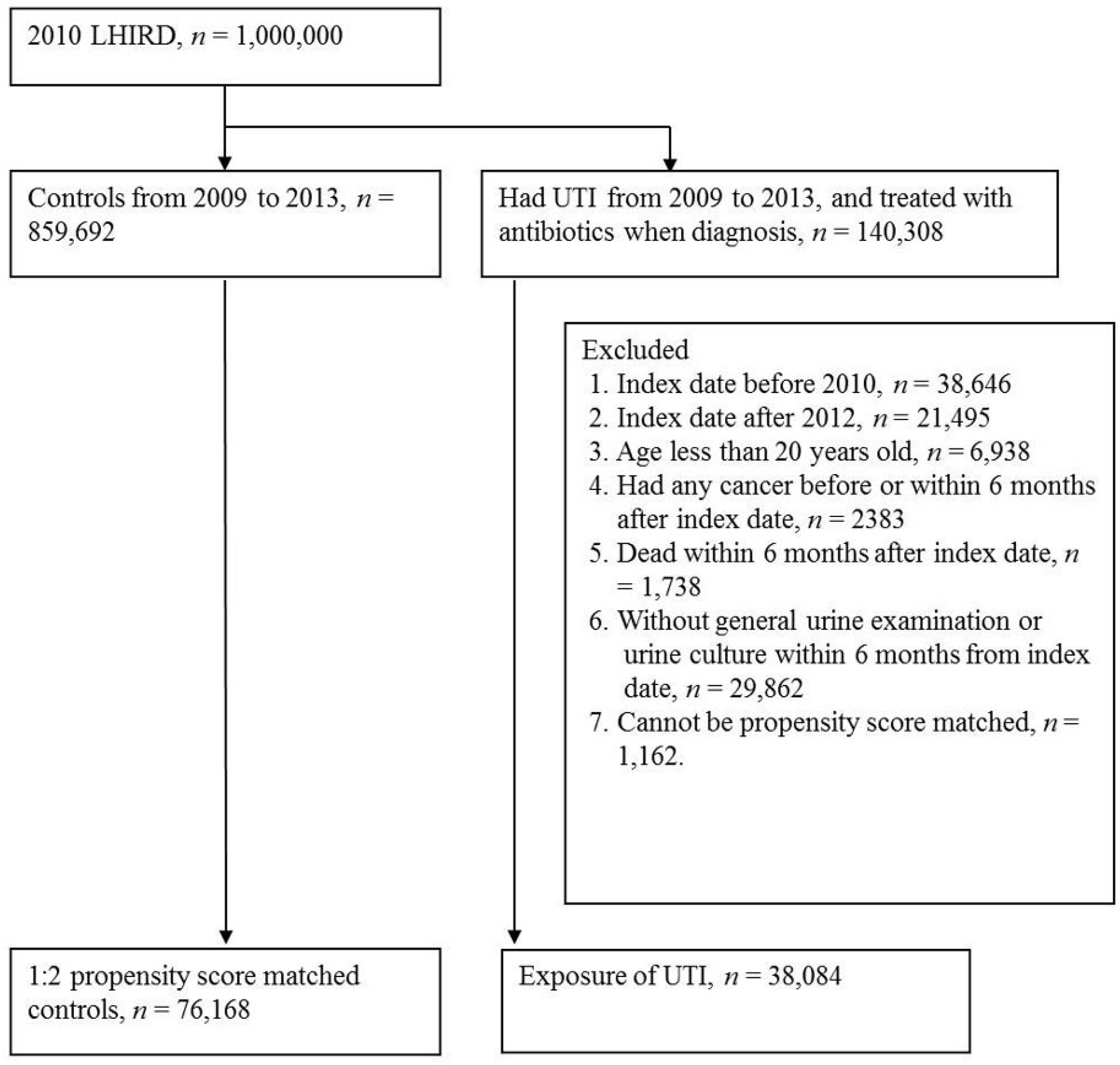
This was a retrospective cohort study. We identified patients (n = 140,308) who visited a hospital or were hospitalized for UTI (ICD-9: 599.0, 595.0, 595.9, and 590) and had antibiotic therapy (cephalosporins, quinolone antibacterial, sulfonamides and trimethoprim, ampicillin, amoxicillin, and nitrofurantoin) in the same visit during 2009–2013 as the exposure group. To ensure that only newly identified UTI was included, prevalent cases of UTI in 2009 were excluded. Furthermore, patients newly diagnosed with UTI in 2013 were excluded because they were only followed up for less than 1 year. The index date was the first date of UTI visit or admission; additional exclusion criteria included patients aged less than 20 years old, those having any cancer, those who died, and those who underwent urine examination within 6 months after the index date. A total of 38,084 patients were diagnosed with UTI in this study.
2.3. Propensity Score Matching (PSM)
A potential confounding bias exists in the observational study design. Propensity score matching (PSM) was used to diminish this bias. We used a logistic regression model to estimate the probability (propensity score) of UTI, using such predictors as age, the Charlson Comorbidity Index (CCI), and other comorbidities (hypertension (ICD-9: 401–405), diabetes (ICD-9: 250), dyslipidemia (ICD-9: 272), rheumatic diseases (ICD-9: 714, 710, 720, 696.0, and 696.1), coronary artery disease (ICD-9: 410–414), chronic obstructive pulmonary disease (COPD, ICD-9: 490–492, 493–496), and chronic kidney disease (CKD, ICD-9: 585)). The control (non-UTI exposure during 2009–2013) and study groups were 1:2 propensity-score-matched on the basis of sex because of the specific cancer sites in different genders. The greedy algorithm of PSM was applied using SAS macro [
11].
2.4. Outcome Measurement of Cancer Event
Subsequent cancer events were identified according to ICD-9: 140–208 for ≥2 outpatient visits or ≥1 admission. Major cancer sites reported in Taiwan were considered for subevent analysis, including colorectal (ICD-9: 153–154), liver (ICD-9: 155), lung (ICD-9: 162), and breast (ICD-9: 174), bladder (ICD-9: 188), kidney (ICD-9: 189), male genital organs (ICD-9: 185–187), female genital organs (ICD-9: 179–184), and prostate (ICD-9: 185) cancers. All individuals were followed up from the index date until diagnosed with any cancer, death, or end of study (31 December 2013).
2.5. Statistical Analysis
All analyses were performed after stratifying the data by sex because gender-specific cancer sites were analyzed in this study. Chi-squared test was used to analyze the homogeneity of category variables, and univariate and multivariate Cox regression models were conducted to estimate the crude and adjusted hazard ratio (aHR) (95% confidence interval (CI)). All statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA). p less than 0.05 indicated statistical significance.
3. Results
We identified 38,084 patients diagnosed with UTI from 2010 to 2012 and a total of 76,168 propensity score-matched controls to explore their sequential cancer risk after the index date (
Figure 1). The baseline characteristics among the UTI and non-UTI groups stratified by sex are listed in
Table 1. After PSM, no significant difference was observed in the distributions of age group, CCI group, and comorbidities (hypertension, diabetes hyperlipidemia, rheumatic diseases, coronary artery disease, chronic obstructive pulmonary disease (COPD), and chronic kidney disease (CKD) in both genders. More female UTI cases (the sex ratio, F:M = 31,172:6,912) were observed, especially in women aged 20–44 and 45–65 years. The median of follow-up time was 25 months (Max: 42), because the index date (start point of follow-up) was 6 months after UTI.
The age–sex stratified incidence rate (per 10,000 person-months) and adjusted hazard risks of specific-site cancer (colorectal, liver, lung, genital organs, bladder, kidney, male prostate, female breast cancer, and any cancer) in patients with UTI are presented in
Table 2. For men aged 20–64 years, significant aHRs were observed in any cancers (aHR = 1.37, 95% CI = 1.02–1.86), bladder cancer (aHR = 12.10, 95% CI = 2.70–54.19), and kidney cancer (aHR = 5.20, 95% CI = 1.01–26.82). For men aged ≥65 years, the associations were observed in any cancer (aHR = 1.29, 95% CI = 1.08–1.54), colorectal cancer (aHR = 1.59, 95% CI = 1.01–2.52), genital organ cancer (aHR = 2.37, 95% CI = 1.55–3.64), bladder cancer (aHR = 28.60, 95% CI = 6.80–120.28), kidney cancer (aHR = 3.85, 95% CI = 1.42–10.42), and prostate cancer (aHR = 2.44, 95% CI = 1.59–3.74). For women aged 20–64 years, the significant aHRs were estimated in liver cancer (aHR = 2.44, 95% CI = 1.59–3.74), bladder cancer (aHR = 30.02, 95% CI = 3.97–227.28), and kidney cancer (aHR = 2.90, 95% CI = 1.24–6.78). For women aged ≥65 years, the significantly increased aHRs were observed in any cancer (aHR = 1.30, 95% CI = 1.11–1.53), liver cancer (aHR = 1.54, 95% CI = 1.02–2.33), bladder cancer (aHR = 2.33, 95% CI = 1.01–5.42), and kidney cancer (aHR = 3.40, 95% CI = 1.34–8.64).
The significantly increased HRs of any cancer for UTI exposure in men (crude HR = 1.27, 95% CI = 1.09–1.48; aHR = 1.32, 95% CI = 1.12–1.54) and women (crude HR = 1.21, 95% CI = 1.09–1.36; aHR = 1.21, 95% CI = 1.08–1.35) are indicated in
Table 3 and
Table 4. Additionally, we also demonstrated that in individuals aged ≥65 years, a CCI score of ≥5 indicated higher risk of cancer incidence.
In
Table 5, no interaction effect between UTI and pneumonia on cancer incidence was observed. We demonstrated the dose response of antibiotic prescriptions on cancer incidence in men; the significant p for trend was observed in any cancer (
p = 0.0130) and bladder cancer (
p = 0.0066). However, no significant p trends were observed in women (
Table 6).
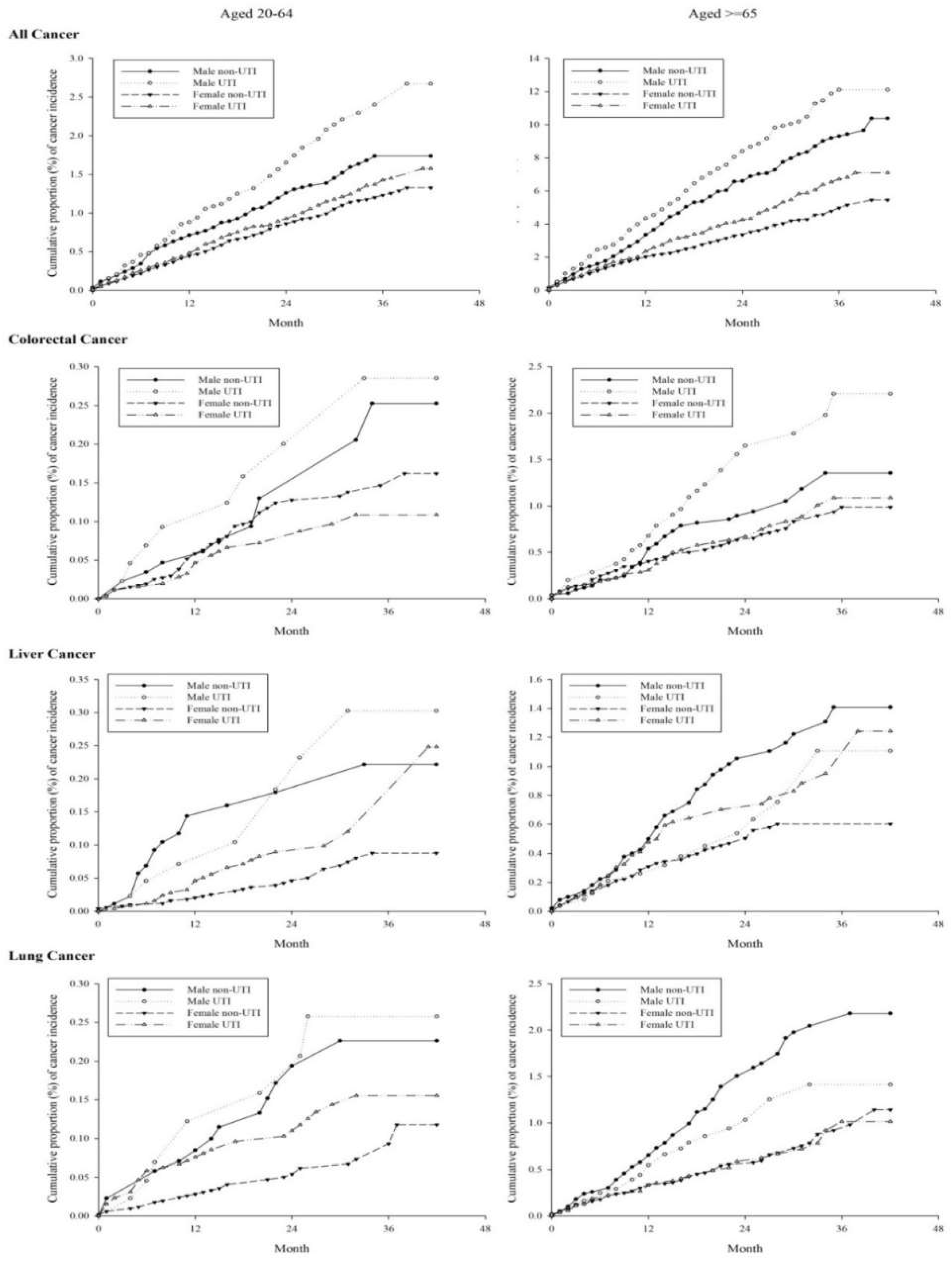
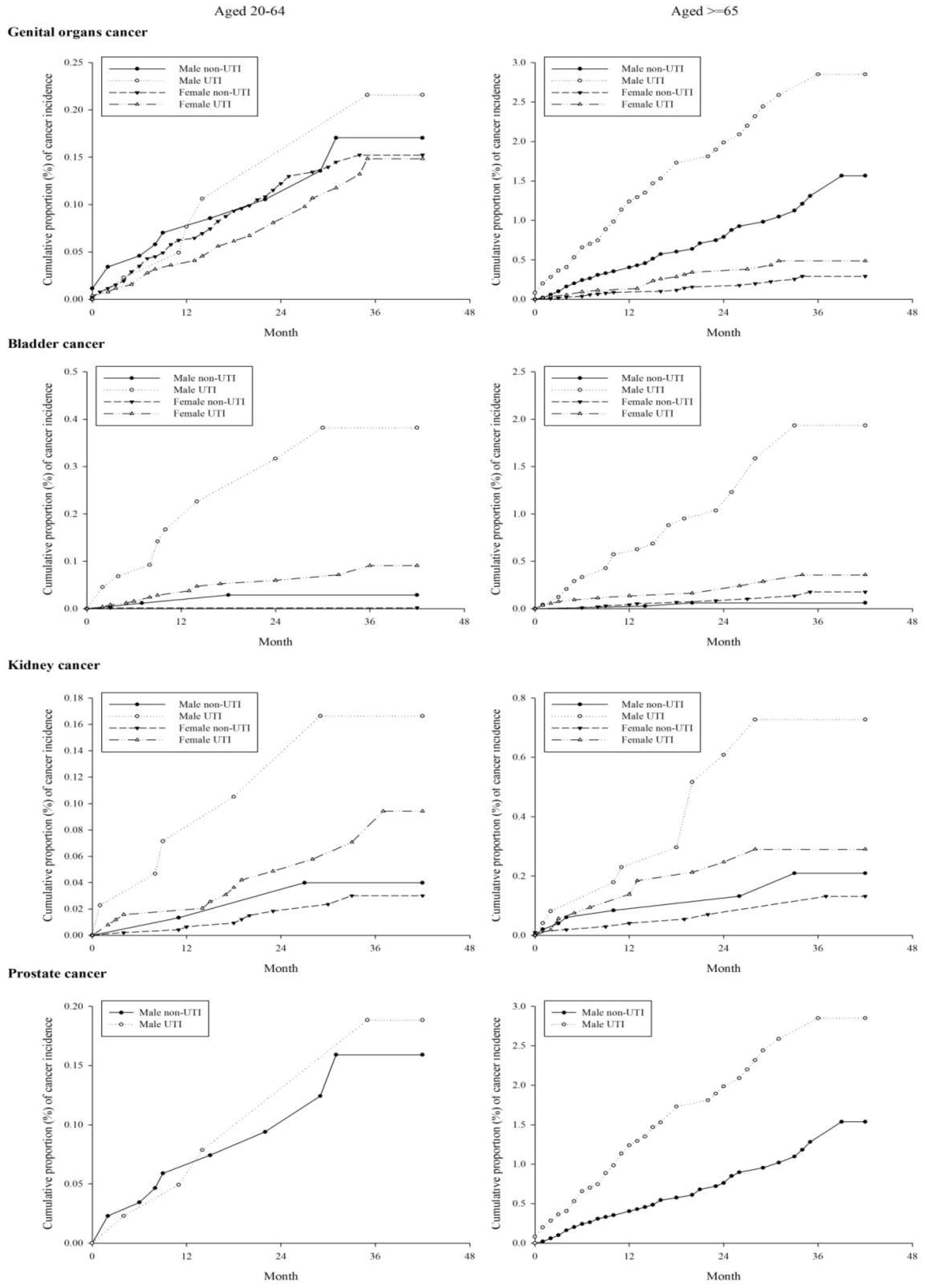
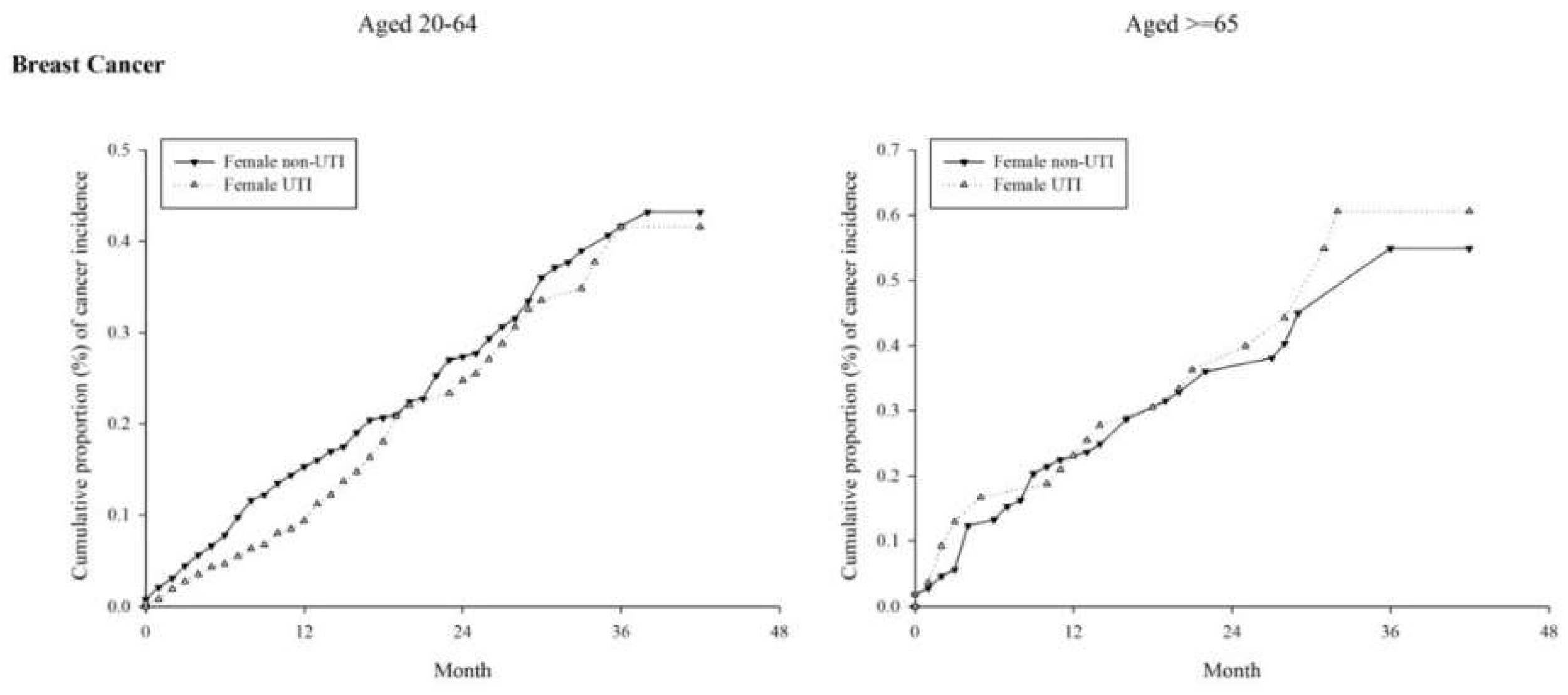
The Kaplan–Meier curve for specific cancer risk among the study groups are shown in
Appendix A Figure A1. Any cancer risk was under proportional hazard assumption; however, bladder and kidney cancer risks were modified after 24 and 18 months, respectively, in the elder (≥65 years old) population.
4. Discussion
Per the analysis results presented in
Figure A1, risk significantly increased not only in GUC but also in any-cancer development. Males older than 65 years exhibited a negative association between UTI and lung cancer risk (
Figure A1). In previous reports, cephalosporins and quinolones were associated with antitumor properties [
12,
13]. The incidence of lung cancer in middle-aged men with UTI may be reduced through antibiotic treatments, and this hypothesis requires more evidence before it can be confirmed.
UTI and pneumonia are clinically common complications, and the results of this work also showed a high correlation between UTI and pneumonia (
p < 0.001) (
Table 3). Some reports have revealed that pneumonia has a high correlation with lung cancer, and Marcus et al. provided evidence of increased lung cancer risk among history of pneumonia rather than immunodeficiency [
14]. The association between pneumonia and any cancer is rarely reported. The incidence of association between pneumonia and any cancer was low in both men and women in this study (
p > 0.05).
UTI is particularly associated with the bladder and kidney cancer in both men and women (
Table 2). The significant and large relative risk was found whether in young (20–64 y/o) or elderly (≥65 y/o) population. This evidence reinforces the study hypothesis that UTI directly increase the risk in bladder and kidney cancers, which is consistent with Anderson-Otunu’s 2016 report [
6]. Vermeulen (2015) revealed that UTI are associated with a high risk of urinary bladder cancer in postmenopausal women, especially in women who smoke or had smoked [
7]. In males, the obstructive urinary symptoms induced by benign prostatic hyperplasia include difficulty in urination and urine retention, resulting in UTI caused from urinary stasis [
15].
Similarly,
Table 6 indicates that the use of antibiotics in the course of UTI treatments increases the risk of bladder and kidney cancers. We analyzed the tumor incidence risk between UTI and pneumonia after antibiotic treatment (
Table 5). The correlation coefficient between antibiotic treatment and tumor incidence was considerably low. However, a significant increase was observed in the incidence of bladder cancer in men after antibiotic treatment for more than 7 days (
Table 6). These results are contrary to many research conclusions, and most antibiotics such as cephalosporins, quinolones, and ampicillins are considered as a kind of cancer treatment drug rather than a carcinogen [
12,
13,
16]. However, no report has clarified whether beta-lactams, amoxicillin, sulfamethoxazole, and trimethoprim are carcinogenic or have antitumor properties. Only nitrofurantoin is a possible carcinogen due to its genotoxic and carcinogenic potential structures, despite its antimicrobial property [
17,
18,
19,
20]. In Kimura’s report (2016), nitrofurantoin does not exert sufficient renal carcinogen responses even after 28 days of administration [
21]. In a recent study on the structure-related genotoxicity of nitrofurantoin, a new evidence revealed that nitrofurantoin does not increase the mutation frequency in the experimental mice. Nevertheless, nitrofurantoin presents no genotoxicity without oxidative stress [
22]. This report provided a safe basis for nitrofuran compound development. The gold standard for UTI diagnosis is isolation and quantification of pathogens in the presence of symptoms and obtaining the antibiotic sensitivity pattern to allow specific treatments. However, in this observational study, we cannot provide the evidence of carcinogen from antibiotics. The length (days) of antibiotics usage also correlated with the severity of infection, that might be the risk factor of cancer. However, the appropriate drug dosage should be based on the severity, characteristics and treatment of the infection situation. Therefore, we should consider antibiotic doses in the treatment of UTI under the premise of controlling infection and avoiding drug resistance. Thus, further research needs to clarify this issue in the future. Women after UTI have higher liver cancer risk as reported in this work, especially approximately 30 months after infection. UTI infection is positively associated with GUC, which is consistent with previous findings. Therefore, this study posits a nonpathogenic causal relationship with UTI symptoms.
Our research has some limitations. First, the database used does not contain information on patients’ clinical presentation, for example, the severity of UTI, personal behavioral information such as drinking, smoking habits, and body mass index, and microbiological culture data that might affect UTI occurrence. Second, the NHI system is limited to the population of Taiwan. Our findings reflect the situation in Taiwan, but it may not be applicable to Western populations. These confounding factors might have influenced the results.
5. Conclusions
In conclusion, UTI are highly correlated with the incidence of all tumors. Clinicians should therefore refer to tumors screening in UTI patients, especially older patients, and not just patients with GUC. In UTI treatment, especially when multiple pathogenic factors are entailed, antibiotics must be used cautiously, and the time and dose of antibiotics should be minimized. Because UTI may increase the incidence of genital organ, bladder, kidney, male colorectal, prostate, and female liver cancer, knowledge about preventing UTI such as proper drinking water, exercise, and toilet habits should be enhanced in educating the general public.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}