Predictors of Number of Healthcare Professionals Consulted by Individuals with Mental Disorders or High Psychological Distress


Abstract
:1. Introduction
2. Method
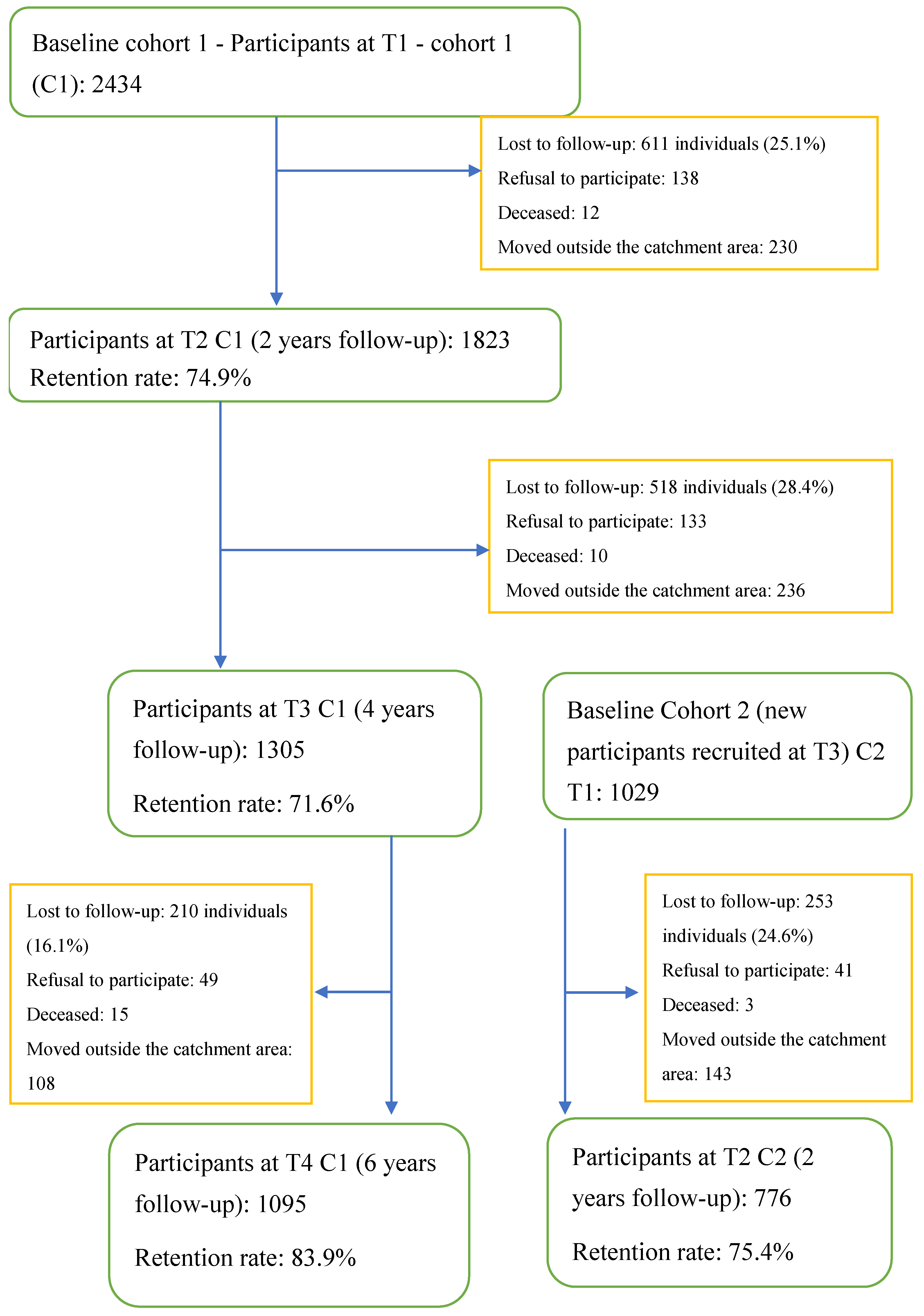
2.1. Study Design and Setting
2.2. Selection Criteria and Study Population
2.3. Conceptual Framework, Variables, and Instruments
2.4. Analyses
3. Results and Discussion
3.1. Results
3.2. Discussion
3.3. Limitations
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prince, M.; Patel, V.; Saxena, S.; Maj, M.; Maselko, J.; Phillips, M.R.; Rahman, A. No health without mental health. Lancet 2007, 370, 859–877. [Google Scholar] [CrossRef]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef]
- Andrews, G.; Slade, T.; Issakidis, C. Deconstructing current comorbidity: Data from the Australian National Survey of Mental Health and Well-Being. Br. J. Psychiatry 2002, 181, 306–314. [Google Scholar] [CrossRef]
- Patten, S.B. Recurrence risk in major depression. Depress Anxiety 2013, 30, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Fleury, M.-J.; Grenier, G.; Bamvita, J.-M.; Perreault, M.; Caron, J. Determinants of the Utilization of Diversified Types of Professionals for Mental Health Reasons in a Montreal (Canadian) Catchment Area. Glob. J. Heal. Sci. 2012, 4, 13–29. [Google Scholar] [CrossRef]
- Wang, P.S.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Borges, G.; Bromet, E.J.; Bruffaerts, R.; de Girolamo, G.; de Graaf, R.; Gureje, O.; et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet 2007, 370, 841–850. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Demler, O.; Frank, R.G.; Olfson, M.; Pincus, H.A.; Walters, E.E.; Wang, P.S.; Wells, K.B.; Zaslavsky, A.M. Prevalence and treatment of mental disorders, 1990 to 2003. N. Engl. J. Med. 2005, 352, 2515–2523. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Patten, S.B. Perceived Effectiveness of mental health care provided by primary-car physicians and mental health specialists. Psychosomatics 2007, 48, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Archer, J.; Bower, P.; Gilbody, S.; Lovell, K.; Richards, D.; Gask, L.; Dickens, C.; Coventry, P. Collaborative care for depression and anxiety problems. Cochrane Database Syst. Rev. 2012, 10, CD006525. [Google Scholar] [CrossRef]
- Bedell, J.R.; Cohen, N.L.; Sullivan, A. Case Management: The Current Best Practices and the Next Generation of Innovation. Community Ment. Heal. J. 2000, 36, 179–194. [Google Scholar] [CrossRef]
- Carter, J.J.; Zawalski, S.; Sminkey, P.V.; Christopherson, B. Assessing the whole person: Case managers take a holistic approach to physical and mental health. Prof. Case Manag. 2015, 20, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Ivbijaro, G.O.; Enum, Y.; Khan, A.A.; Lam, S.S.-K.; Gabzdyl, A. Collaborative Care: Models for Treatment of Patients with Complex Medical-Psychiatric Conditions. Curr. Psychiatry Rep. 2014, 16, 506. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S.; Duerden, D.; Shaddick, S.; Jayabarathan, A. Collaboration between primary care and psychiatric services: Does it help family physicians? Can. Fam. Physician 2006, 52, 876–877. [Google Scholar] [PubMed]
- Katon, W.J.; Lin, E.H.; Von Korff, M.; Ciechanowski, P.; Ludman, E.J.; Young, B.; Peterson, D.; Rutter, C.M.; McGregor, M.; McCulloch, D. Collaborative Care for Patients with Depression and Chronic Illnesses. N. Engl. J. Med. 2010, 363, 2611–2620. [Google Scholar] [CrossRef] [PubMed]
- Woltmann, E.; Grogan-Kaylor, A.; Perron, B.; Georges, H.; Kilbourne, A.M.; Bauer, M.S. Comparative Effectiveness of Collaborative Chronic Care Models for Mental Health Conditions Across Primary, Specialty, and Behavioral Health Care Settings: Systematic Review and Meta-Analysis. Am. J. Psychiatry 2012, 169, 790–804. [Google Scholar] [CrossRef] [PubMed]
- Huffman, J.C.; Niazi, S.K.; Rundell, J.R.; Sharpe, M.; Katon, W.J. Essential Articles on Collaborative Care Models for the Treatment of Psychiatric Disorders in Medical Settings: A Publication by the Academy of Psychosomatic Medicine Research and Evidence-Based Practice Committee. Psychosomatics 2014, 55, 109–122. [Google Scholar] [CrossRef] [PubMed]
- LeDoux, Y.; Minner, P. Occasional and frequent repeaters in a psychiatric emergency room. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 115–121. [Google Scholar] [CrossRef]
- Pasic, J.; Russo, J.; Roy-Byrne, P. High Utilizers of Psychiatric Emergency Services. Psychiatr. Serv. 2005, 56, 678–684. [Google Scholar] [CrossRef] [Green Version]
- Chaput, Y.J.A.; Lebel, M.-J. Demographic and Clinical Profiles of Patients Who Make Multiple Visits to Psychiatric Emergency Services. Psychiatr. Serv. 2007, 58, 335–341. [Google Scholar] [CrossRef]
- Wang, P.S.; Demler, O.; Olfson, M.; Pincus, H.A.; Wells, K.B.; Kessler, R.C. Changing Profiles of Service Sectors Used for Mental Health Care in the United States. Am. J. Psychiatry 2006, 163, 1187–1198. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.M. Revisiting the Behavioral Model and Access to Medical Care: Does it Matter? J. Heal. Soc. Behav. 1995, 36, 1. [Google Scholar] [CrossRef]
- Roberts, T.; Esponda, G.M.; Krupchanka, D.; Shidhaye, R.; Patel, V.; Rathod, S. Factors associated with health service utilisation for common mental disorders: A systematic review. BMC Psychiatry 2018, 18, 262. [Google Scholar] [CrossRef] [PubMed]
- Wang, J. Perceived Barriers to Mental Health Service Use among Individuals with Mental Disorders in the Canadian General Population. Med. Care 2006, 44, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Vasiliadis, H.-M.; Tempier, R.; Lesage, A.; Kates, N. General practice and mental health care: Determinants of outpatient service use. Can. J. Psychiatry 2009, 54, 468–476. [Google Scholar] [CrossRef]
- Fleury, M.-J.; Ngui, A.N.; Bamvita, J.-M.; Grenier, G.; Caron, J. Predictors of Healthcare Service Utilization for Mental Health Reasons. Int. J. Environ. Res. Public Heal. 2014, 11, 10559–10586. [Google Scholar] [CrossRef] [Green Version]
- Fleury, M.-J.; Grenier, G.; Bamvita, J.-M.; Perreault, M.; Caron, J. Variables Associated with Perceived Unmet Need for Mental Health Care in a Canadian Epidemiologic Catchment Area. Psychiatr. Serv. 2016, 67, 78–85. [Google Scholar] [CrossRef]
- Bobevski, I.; Rosen, A.; Meadows, G. Mental health service use and need for care of Australians without diagnoses of mental disorders: Findings from a large epidemiological survey. Epidemiol. Psychiatr. Sci. 2017, 26, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Burgess, P.M.; Pirkis, J.E.; Slade, T.N.; Johnston, A.K.; Meadows, G.N.; Gunn, J.M. Service Use for Mental Health Problems: Findings from the 2007 National Survey of Mental Health and Wellbeing. Aust. N. Z. J. Psychiatry 2009, 43, 615–623. [Google Scholar] [CrossRef]
- Haller, H.; Cramer, H.; Lauche, R.; Gass, F.; Dobos, G.J. The prevalence and burden of subthreshold generalized anxiety disorder: A systematic review. BMC Psychiatry 2014, 14, 128. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Smit, F.; Willemse, G. Predicting the onset of major depression in subjects with subthreshold depression in primary care: A prospective study. Acta Psychiatr. Scand. 2005, 111, 133–138. [Google Scholar] [CrossRef]
- Mirowsky, J.; Ross, C.E. Measurement for a human science. J. Health Soc. Behav. 2002, 43, 152–170. [Google Scholar] [CrossRef] [PubMed]
- Thurston-Hicks, A.; Paine, S.; Hollifield, M. Rural Psychiatry: Functional Impairment Associated with Psychological Distress and Medical Severity in Rural Primary Care Patients. Psychiatr. Serv. 1998, 49, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Mental Health Commission of Canada. Advancing the Mental Health Strategy for Canada: A Framework for Action (2017–2022). Available online: https://www.mentalhealthcommission.ca/sites/default/files/2016-08/advancing_the_mental_health_strategy_for_canada_a_framework_for_action.pdf 2016 (accessed on 23 August 2018).
- Thomas, S.; Jenkins, R.; Burch, T.; Nasir, L.C.; Fisher, B.; Giotaki, G.; Gnani, S.; Hertel, L.; Marks, M.; Mathers, N.; et al. Promoting Mental Health and Preventing Mental Illness in General Practice. Lond. J. Prim. Care 2016, 8, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Caron, J.; Fleury, M.-J.; Perreault, M.; Crocker, A.; Tremblay, J.; Tousignant, M.; Kestens, Y.; Cargo, M.; Daniel, M. Prevalence of psychological distress and mental disorders, and use of mental health services in the epidemiological catchment area of Montreal South-West. BMC Psychiatry 2012, 12, 183. [Google Scholar] [CrossRef]
- Torvik, F.A.; Rognmo, K.; Tambs, K. Alcohol use and mental distress as predictors of non-response in a general population health survey: The HUNT study. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Kosidou, K.; Dalman, C.; Lundberg, M.; Hallqvist, J.; Isacsson, G.; Magnusson, C. Socioeconomic status and risk of psychological distress and depression in the Stockholm Public Health Cohort: A population-based study. J. Affect. Disord. 2011, 134, 160–167. [Google Scholar] [CrossRef]
- Twomey, C.D.; Baldwin, D.S.; Hopfe, M.; Cieza, A. A systematic review of the predictors of health service utilisation by adults with mental disorders in the UK. BMJ Open 2015, 5, e007575. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- De Graaf, R.; ten Have, M.; van Gool, C.; van Dorsselaer, S. Prevalence of mental disorders and trends from 1996 to 2009. Results from the Netherlands Mental Health Survey and Incidence Study-2. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Canadian Community Health Survey-Mental Health and Well-Being-Cycle 1.2. 2003. Available online: http://www23.statcan.gc.ca/imdb-bmdi/document/3226_DLI_D1_T22_V2-eng.pdf (accessed on 15 September 2018).
- Cummins, R.A.; Eckersley, R.; Pallant, J.; Van Vugt, J.; Misajon, R. Developing a national index of subjective well-being: The Australian Unity Well-being Index. Soc. Indic. Res. 2003, 64, 159–190. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Mental Illness and/or Mental Health? Investigating Axioms of the Complete State Model of Health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Social well-being. Soc. Psychol. Q. 1998, 61, 121–140. [Google Scholar] [CrossRef]
- Andrews, F.M.; Withey, S.B. Social Indicators of Wellbeing: Americans’ Perceptions of Life Quality; Plenun Press: New York, NY, USA, 1976. [Google Scholar]
- Baker, F.; Intagliata, J. Quality of life in the evaluation of community support systems. Eval. Program Plan. 1982, 5, 69–79. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Mroczek, D.; Üstün, B.; Wittchen, H.-U. The World Health Organization Composite International Diagnostic Interview short-form (CIDI-SF). Int. J. Methods Psychiatr. Res. 1998, 7, 171–185. [Google Scholar] [CrossRef]
- Tousignant, M.; Bastien, M.F.; Hamel, S. Suicidal attempts and ideations among adolescents and young adults: The contribution of the father’s and mother’s care and of parental separation. Soc. Psychiatry Psychiatr. Epidemiol. 1993, 28, 256–261. [Google Scholar] [PubMed]
- Gold, L.H. DSM-5 and the assessment of functioning: The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0). J. Am. Acad. Psychiatry Law 2014, 42, 173–181. [Google Scholar] [PubMed]
- Vonkorff, M.; Simon, G.; Saunders, K.; Brandenburg, N.; Kessler, R.; Von Korff, M.; Crane, P.; Lane, M.; Miglioretti, D.L.; Stang, P. Chronic spinal pain and physical–mental comorbidity in the United States: Results from the national comorbidity survey replication. Pain 2005, 113, 331–339. [Google Scholar] [CrossRef]
- Laurin, I. Facteurs de risque de la condition des sans domicile fixe. In Comparaison d’une Cohorte de Nouveaux Sans Domicile Fixe et d’une Cohorte de Domiciliés Pauvres; Université de Montréal: Montréal, QC, Canada, 1998. [Google Scholar]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for Serious Mental Illness in the General Population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Kay, S.R.; Wolkenfeld, F.; Murrill, L.M. Profiles of Aggression among Psychiatric Patients. J. Nerv. Ment. Dis. 1988, 176, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Meadows, G.N.; Burgess, P.; Fossey, E.; Harvey, C. Perceived need for mental health care- findings from the Autralian National Survey of Mental Health and Wellbeing. Psychol. Med. 2000, 30, 645–656. [Google Scholar] [CrossRef]
- Kohn, R.; Saxena, S.; Levav, I.; Saraceno, B. The treatment gap in mental health care. Bull. World Heal. Organ. 2004, 82, 858–866. [Google Scholar]
- Sagar, R.; Pattanayak, R.D.; Chandrasekaran, R.; Chaudhury, P.K.; Deswal, B.S.; Singh, R.K.L.; Malhotra, S.; Nizamie, S.H.; Panchal, B.N.; Sudhakar, T.P.; et al. Twelve-month prevalence and treatment gap for common mental disorders: Findings from a large-scale epidemiological survey in India. Indian J. Psychiatry 2017, 59, 46–55. [Google Scholar] [CrossRef]
- Drapeau, A.; Boyer, R.; Lesage, A. The Influence of Social Anchorage on the Gender Difference in the Use of Mental Health Services. J. Behav. Heal. Serv. Res. 2009, 36, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Seekles, W.; Van Straten, A.; Beekman, A.; Van Marwijk, H.; Cuijpers, P. Stepped care treatment for depression and anxiety in primary care. A randomized controlled trial. Trials 2011, 12, 171. [Google Scholar] [CrossRef] [PubMed]
- Fleury, M.-J. Implementation of the Consultation-liaison Model in Quebec and its Impact on Primary Care Providers. Ment. Health Fam. Med. 2016, 12, 228–240. [Google Scholar] [CrossRef]
- Walters, P.; Tylee, A.; Goldberg, D. Psychiatry in Primary Care. In Essential Psychiatry, 4th ed.; Murray, R.M., Kendler, K.S., McGuffin, P., Wessely, S., Castle, D.J., Eds.; Cambridge University Press: Cambridge, UK, 2008; pp. 479–497. [Google Scholar]
- Fleury, M.J.; Grenier, G.; Bamvita, J.M.; Perreault, M.; Caron, J. Determinants associated with the utilization of primary and specialized mental health services. Psychiatr. Q. 2012, 83, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Van Ameringen, M.; Mancini, C.; Patterson, B.; Boyle, M.H. Post-Traumatic Stress Disorder in Canada. CNS Neurosci. Ther. 2008, 14, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Erbes, C.; Westermeyer, J.; Engdahl, B.; Johnsen, E. Post-traumatic stress disorder and service utilization in a sample of service members from Iraq and Afghanistan. Mil. Med. 2007, 172, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Kuramoto-Crawford, S.J.; Smith, K.E.; McKeon, R. Characteristics of U.S. Mental Health Facilities That Offer Suicide Prevention Services. Psychiatr. Serv. 2016, 67, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Mojtabai, R.; Olfson, M.; Mechanic, D. Perceived Need and Help-Seeking in Adults with Mood, Anxiety, or Substance Use Disorders. Arch. Gen. Psychiatry 2002, 59, 77. [Google Scholar] [CrossRef]
- Brook, R.; Klap, R.; Liao, D.; Wells, K.B. Mental health care for adults with suicide ideation. Gen. Hosp. Psychiatry 2006, 28, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Caron, J.; Liu, A. Factors associated with psychological distress in the Canadian population: A comparison of low-income and non low-income sub-groups. Community Ment. Health J. 2011, 47, 318–330. [Google Scholar] [CrossRef]
- Ullman, S.E.; Brecklin, L.R. Sexual Assault History and Suicidal Behavior in a National Sample of Women. Suicide Life Threat. Behav. 2002, 32, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Benjet, C.; Borges, G.; Medina-Mora, M.E. Chronic childhood adversity and onset of psychopathology during three life stages: Childhood, adolescence and adulthood. J. Psychiatr. Res. 2010, 44, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Glover, K.; Olfson, M.; Gameroff, M.J.; Neria, Y. Assault and Mental Disorders: A Cross-Sectional Study of Urban Adult Primary Care Patients. Psychiatr. Serv. 2010, 61, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Holman, E.A. Traumatic Life Events in Primary Care Patients: A Study in an Ethnically Diverse Sample. Arch. Fam. Med. 2000, 9, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huỳnh, C.; Caron, J.; Fleury, M.-J. Mental health services use among adults with or without mental disorders: Do development stages matter? Int. J. Soc. Psychiatry 2016, 62, 434–451. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F.; Christensen, H.; Medway, J.; Korten, A.E.; Jacomb, P.A.; Rodgers, B. Public belief systems about the helpfulness of interventions for depression: Associations with history of depression and professional help-seeking. Soc. Psychiatry Psychiatr. Epidemiol. 2000, 35, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Mojtabai, R.; Evans-Lacko, S.; Schomerus, G.; Thornicroft, G. Attitudes Toward Mental Health Help Seeking as Predictors of Future Help-Seeking Behavior and Use of Mental Health Treatments. Psychiatr. Serv. 2016, 67, 650–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, L.E.; Vigod, S.; Wishart, J.; Waese, M.; Spence, J.D.; Oliver, J.; Chambers, J.; Anderson, S.; Shields, R. Barriers and facilitators to primary care for people with mental health and/or substance use issues: A qualitative study. BMC Fam. Pr. 2015, 16, 135. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, G.; Foley, K.; Majeed, A. Rethinking primary care’s gatekeeper role. BMJ 2016, 354, 4803. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B.; Lemke, K.W.; Bernhardt, T.; Foldes, S.S.; Forrest, C.B.; Weiner, J.P. Comorbidity: Implications for the Importance of Primary Care in ‘Case’ Management. Ann. Fam. Med. 2003, 1, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Lebrun-Harris, L.A.; Sripipatana, A.; Ngo-Metzger, Q. Access to Mental Health Services Among Patients at Health Centers and Factors Associated with Unmet Needs. J. Heal. Care Poor Underserved 2014, 25, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, J.M.; Sacco, P. Employee Assistance Program Services for Alcohol and Other Drug Problems: Implications for Increased Identification and Engagement in Treatment. Am. J. Addict. 2012, 21, 468–475. [Google Scholar] [CrossRef]
- Paul, K.I.; Geithner, E.; Moser, K. Latent Deprivation among People who Are Employed, Unemployed, or Out of the Labor Force. J. Psychol. 2009, 143, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Buffel, V.; Van De Straat, V.; Bracke, P. Employment status and mental health care use in times of economic contraction: A repeated cross-sectional study in Europe, using a three-level model. Int. J. Equity Heal. 2015, 14, 308. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.; Yoon, H.; Chiriboga, D.A.; Molinari, V.; Powers, D.A. Bridging the Gap Between Common Mental Disorders and Service Use: The Role of Self-Rated Mental Health Among African Americans. Am. J. Geriatr. Psychiatry 2015, 23, 658–665. [Google Scholar] [CrossRef]
- Kim, G.; Jang, Y.; Chiriboga, D.A.; Ma, G.X.; Schonfeld, L. Factors associated with mental health service use in Latino and Asian immigrant elders. Aging Ment. Heal. 2010, 14, 535–542. [Google Scholar] [CrossRef]
- Whitley, R.; Wang, J.; Fleury, M.J.; Liu, A.; Caron, J. Mental Health Status, Health Care Utilisation, and Service Satisfaction among Immigrants in Montreal: An Epidemiological Comparison. Can. J. Psychiatry 2017, 62, 570–579. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Instruments, References, and Psychometric Properties | Description |
|---|---|---|
| Predisposing factors | ||
| Age | Canadian Community Health Survey of MH and Well-Being CCHS 1.2 [41] | Calculated from date of birth and confirmed by participants One item Numeric value |
| Gender | CCHS 1.2 [41] | As declared by participants Two items (male/female) |
| Civil status | CCHS 1.2 [41] | As declared by participants Two items (living as a couple; living alone) |
| Household size | CCHS 1.2 [41] | As declared by participants One item Numeric value |
| Number of children in the household | CCHS 1.2 [41] | As declared by participants One item Numeric value |
| Self-perception of physical health | CCHS 1.2 [41] | Self-perception of physical health One item Five-point Likert scale Higher = more negative |
| Self-perception of mental health (MH) | CCHS 1.2 [41] | Self-perception of mental health (MH) One item Five-point Likert scale Higher = more negative |
| Satisfaction with health services | CCHS 1.2 [41] | Measure satisfaction with health services 30 items Four-point Liker scale Higher = greater satisfaction |
| Enabling factors | ||
| Having a family physician | CCHS 1.2 [41] | As declared by participants Yes/No |
| Previous use of MH services | CCHS 1.2 [41] | As declared by participants Yes/No |
| Employment status | CCHS 1.2 [41] | As declared by participants Yes/No |
| Personal well-being | Australian Unity Well-being Index [42] Cronbach alpha: 0.85 | Measures personal satisfaction with life as a whole and in Eight sub-dimensions Nine items 10-point Likert scale Higher = more positive |
| Emotional well-being | MH Continuum—Short Form [43] | Measures the degree of emotional well-being defined in terms of positive affect/satisfaction with life; social well-being as described in Keyes [44] model of social well-being 14 items Seven-point Likert scale Range: 1–98 Higher = more negative |
| Quality of life | Satisfaction with Life Domains Scale [45]; adapted by Baker and Intagliata [46] for psychiatric patients Cronbach alpha: 0.9 | Quality of life in five domains 20 items Seven-point Likert scale Range: 0–140 Higher = better quality of life |
| Needs factors | ||
| Major depressive disorder | Composite International Diagnostic Interview (CIDI) and CIDI-SF [47] | Psychiatric diagnoses based on the definitions and criteria of ICD-10 a and DSM-IV b. Yes/No and multiple choice |
| Generalized anxiety disorder | Composite International Diagnostic Interview (CIDI) and CIDI-SF [47] | Psychiatric diagnoses based on the definitions and criteria of ICD-10 and DSM-IV. Yes/No and multiple choice |
| Post-traumatic stress disorder (PTSD) | Composite International Diagnostic Interview (CIDI) and CIDI-SF [47] | Psychiatric diagnoses based on the definitions and criteria of ICD-10 and DSM-IV. Yes/No and multiple choice |
| Drug and alcohol dependence | Composite International Diagnostic Interview (CIDI) and CIDI-SF [47] | Psychiatric diagnoses based on the definitions and criteria of ICD-10 and DSM-IV Yes/No and multiple choice |
| Suicide ideation | Tousignant et al. [48] | Suicide ideation at life in the last 12 months Yes/No |
| Functional disability | 12-item version of the World Health Organization Disability Assessment Schedule II (WHO-DAS-II) [49] | Measure functional disability 12 items Five-point Likert-scale Range: 0–60 Score of 45 or greater indicates substantial disability [50] |
| Stressful events | Lifetime Events Questionnaire [51] | Stressful events in the last 12 months related to housing, family and friends, income, love, and aggressive experiences 25 items Yes/No |
| High psychological distress | K-10 scale [52] Cronbach alpha: 0.93 | Measure frequency of distress symptoms in the past month such as nervousness, tiredness, despair, agitation, sadness, and feeling of worthlessness 10 items Five-point Likert scale (cut-off point for determining high psychological distress = 9) |
| Physical illnesses | CCHS 1.2 [41] | Number of physical illness as declared by participants Yes/No |
| Physical aggression | Modified Observed Aggression Scale [53] | Assess 4 categories of aggressive behavior: Verbal aggression, aggression to propriety, self-inflicted aggression, physical aggression 20 items Yes/No |
| Unmet need for help | Perceived Need for Care Questionnaire [54] | Five items Yes/No |
| Frequency Distributions | Bivariate Associations with Number of Healthcare Professionals Visited at T4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables at T3 | Min | Max | n/Mean | %/SD | Beta | t | p Value | ||
| Predisposing factors | Age | 15.00 | 72.00 | 43.71 | 14.04 | 0.011 | 0.289 | 0.773 | |
| Gender | Female | 460 | 61.7 | 1 | |||||
| Male | 286 | 38.3 | −0.063 | −1.725 | 0.085 | ||||
| Civil status | Living alone | 473 | 63.4 | 1 | |||||
| Living as a couple | 273 | 36.6 | −0.106 | −2.903 | 0.004 | ||||
| Household size | 0.00 | 13.00 | 2.47 | 1.47 | −0.071 | −1.950 | 0.052 | ||
| Self-perception of physical health in the past 12 months | 1.00 | 5.00 | 2.75 | 1.05 | −0.128 | −3.529 | <0.001 | ||
| Self-perception of MH | 1.00 | 5.00 | 2.89 | 0.98 | −0.287 | −8.179 | <0.001 | ||
| Satisfaction with health services | 4.00 | 90.00 | 51.68 | 13.78 | −0.136 | −3.747 | <0.001 | ||
| Enabling factors | Having a family physician | 515 | 69.0 | 0.130 | 3.568 | <0.001 | |||
| Previous use of services for MH reasons | 219 | 29.4 | 0.346 | 10.065 | <0.001 | ||||
| Private insurance coverage including visits to psychologist | 46 | 6.2 | 0.142 | 3.921 | <0.001 | ||||
| Employment status | 138 | 18.5 | 0.098 | 2.685 | 0.007 | ||||
| Quality of life (QOL) (total score) a | 45.00 | 135.00 | 100.95 | 15.50 | −0.199 | −5.533 | <0.001 | ||
| Emotional well-being b | 4.00 | 70.00 | 42.47 | 12.20 | −0.159 | −4.404 | <0.001 | ||
| Personal well-being c | 2.00 | 90.00 | 58.48 | 13.69 | −0.186 | −5.168 | <0.001 | ||
| Needs factors | Stressful events (total score) | 0.00 | 14.00 | 3.84 | 2.45 | 0.221 | 6.174 | <0.001 | |
| High psychological distress | 0.00 | 35.00 | 13.83 | 5.13 | 0.201 | 5.593 | <0.001 | ||
| Physical illnesses | 1.36 | 1.47 | 0.079 | 2.169 | 0.030 | ||||
| Unmet need for help | 110 | 14.7 | 0.151 | 4.171 | <0.001 | ||||
| Major depressive episode | 129 | 17.3 | 0.250 | 7.028 | <0.001 | ||||
| Generalized anxiety disorder | 15 | 2.0 | 0.099 | 2.707 | 0.007 | ||||
| Post-traumatic stress disorder (PTSD) | 50 | 6.7 | 0.225 | 6.286 | <0.001 | ||||
| Drug and alcohol dependence | 29 | 3.9 | 0.070 | 1.916 | 0.056 | ||||
| Number of mental disorders | 0.00 | 5.00 | 0.37 | 0.71 | 0.253 | 7.142 | <0.001 | ||
| Physical aggression | 43 | 5.8 | 0.085 | 2.332 | 0.020 | ||||
| Functional disability d | 13.00 | 49.00 | 19.33 | 6.91 | 0.186 | 5.157 | <0.001 | ||
| Suicide ideation | 69 | 9.2 | 0.213 | 5.949 | <0.001 | ||||
| Variables | Block 1 | Block 2 | Block 3 | Block 4 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beta | p | Beta | p | Beta | p | Beta | t | p | 95.0% CI for B | Collinearity Statistics | ||||
| LB a | UB b | Tolerance | VIF c | |||||||||||
| Needs 1 Factors (Clinical) | (Constant) | 0.128 | 0.278 | 0.012 | 0.761 | 0.447 | −0.205 | 0.464 | ||||||
| High psychological distress | 0.085 | 0.024 | 0.042 | 0.286 | −0.004 | 0.926 | 0.003 | 0.081 | 0.935 | −0.012 | 0.013 | 0.676 | 1.480 | |
| Major depressive disorder | 0.159 | <0.001 | 0.132 | <0.001 | 0.102 | 0.007 | 0.055 | 1.476 | 0.140 | −0.039 | 0.274 | 0.771 | 1.297 | |
| Generalized anxiety disorder (GAD) | 0.085 | 0.014 | 0.078 | 0.023 | 0.071 | 0.038 | 0.050 | 1.520 | 0.129 | −0.084 | 0.662 | 0.981 | 1.020 | |
| Post-traumatic stress disorder (PTSD) | 0.146 | <0.001 | 0.123 | 0.001 | 0.124 | 0.001 | 0.105 | 2.945 | 0.003 | 0.113 | 0.566 | 0.838 | 1.193 | |
| Suicide ideation | 0.114 | 0.002 | 0.101 | 0.005 | 0.085 | 0.017 | 0.062 | 1.776 | 0.076 | −0.018 | 0.364 | 0.879 | 1.138 | |
| Needs 2 Factors (Other-Clinical) | Stressful events | 0.126 | <0.001 | 0.098 | 0.007 | 0.098 | 2.746 | 0.006 | 0.009 | 0.056 | 0.830 | 1.205 | ||
| Functional disability | 0.085 | 0.028 | 0.080 | 0.036 | 0.050 | 1.355 | 0.176 | −0.003 | 0.014 | 0.778 | 1.285 | |||
| Predisposing | Self-perception of MH | −0.157 | <0.001 | −0.116 | −2.983 | 0.003 | −0.159 | −0.033 | 0.705 | 1.419 | ||||
| Enabling Factors | Previous use of MH services | 0.217 | 5.930 | <0.001 | 0.258 | 0.513 | 0.797 | 1.255 | ||||||
| Having a family physician | 0.112 | 3.358 | 0.001 | 0.082 | 0.311 | 0.954 | 1.048 | |||||||
| Employment status | 0.079 | 2.332 | 0.020 | 0.026 | 0.301 | 0.940 | 1.064 | |||||||
| Goodness of fit | F | 20.038 | 17.340 | 17.450 | 18.543 | |||||||||
| p | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||
| Total variance explained (Adjusted R Square) | 0.113 | 0.133 | 0.150 | 0.206 | ||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simo, B.; Caron, J.; Bamvita, J.-M.; Grenier, G.; Fleury, M.-J. Predictors of Number of Healthcare Professionals Consulted by Individuals with Mental Disorders or High Psychological Distress. Int. J. Environ. Res. Public Health 2019, 16, 3010. https://doi.org/10.3390/ijerph16173010
Simo B, Caron J, Bamvita J-M, Grenier G, Fleury M-J. Predictors of Number of Healthcare Professionals Consulted by Individuals with Mental Disorders or High Psychological Distress. International Journal of Environmental Research and Public Health. 2019; 16(17):3010. https://doi.org/10.3390/ijerph16173010
Chicago/Turabian StyleSimo, Béatrice, Jean Caron, Jean-Marie Bamvita, Guy Grenier, and Marie-Josée Fleury. 2019. "Predictors of Number of Healthcare Professionals Consulted by Individuals with Mental Disorders or High Psychological Distress" International Journal of Environmental Research and Public Health 16, no. 17: 3010. https://doi.org/10.3390/ijerph16173010