Proposal of an Adapted Physical Activity Exercise Protocol for Women with Osteoporosis-Related Vertebral Fractures: A Pilot Study to Evaluate Feasibility, Safety, and Effectiveness

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
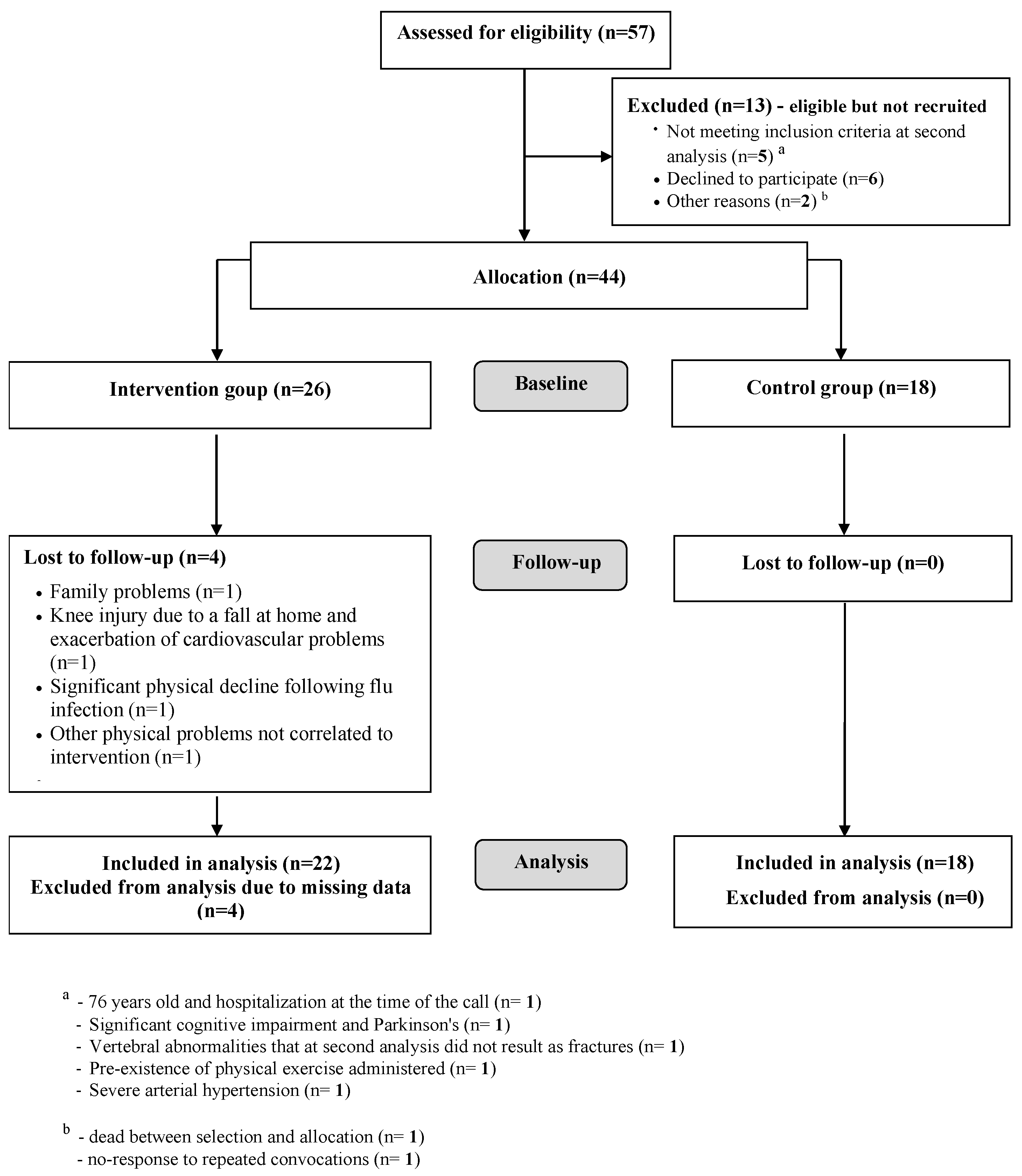
2.1. Study Design and Subjects
2.2. Intervention
2.3. Assessments at Baseline and 6-Months Follow-Up
2.3.1. Health-Related Quality of Life (HRQOL)
2.3.2. Fear of Falling
2.3.3. Lumbar Back Pain
2.3.4. Physical Performance
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. 2003. Prevention and Management of Osteoporosis. WHO Technical Report Series 921. Available online: https://apps.who.int/iris/handle/10665/42841 (accessed on 14 June 2019).
- International Osteoporosis Foundation. 2018. Broken Bones, Broken Lives: A Roadmap to Solve the Fragility Fracture Crisis in Europe. Available online: http://share.iofbonehealth.org/EU-6-Material/Reports/IOF%20Report_EU.pdf (accessed on 14 June 2019).
- Odén, A.; McCloskey, E.V.; Kanis, J.A.; Harvey, N.C.; Johansson, H. Burden of high fracture probability worldwide: Secular increases 2010–2040. Osteoporos Int. 2015, 26, 2243–2248. [Google Scholar] [CrossRef] [PubMed]
- Adachi, J.D.; Loannidis, G.; Berger, C.; Joseph, L.; Papaioannou, A.; Pickard, L.; Pickard, L.; Papadimitropoulos, E.; Hopman, W.; Poliquin, S.; et al. The influence of osteoporotic fractures on health-related quality of life in community-dwelling men and women across Canada. Osteoporos Int. 2001, 12, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Kado, D.M.; Huangm, M.; Nguyen, C.B.; Barrett-Connor, E.; Greendale, G.A. Hyperkyphotic posture and risk of injurious falls in older persons: The Rancho Bernardo Study. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Kendler, D.; Bauer, D.C.; Davison, K.; Dian, L.; Hanley, D.A.; Harris, S.; McClung, M.R.; Miller, P.; Schousboe, J.; Yuen, C. Vertebral fractures: Clinical importance and management. Am. J. Med. 2016, 129, 221.e1–221.e10. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Prieto-Merino, D.; Dale, C.; Nüesch, E.; Amuzu, A.; Bowling, A.; Ebrahim, S.; Casas, J.P. Effect of changes in moderate or vigorous physical activity on changes in health-related quality of life of elderly British women over seven years. Qual. Life Res. 2013, 22, 2011–2020. [Google Scholar] [CrossRef] [PubMed]
- Giangregorio, L.; Papaioannou, A.; Macintyre, N.; Ashe, M.; Heinonen, A.; Shipp, K.; Wark, J.; McGill, S.; Keller, H.; Jain, R. Too fit to fracture: Exercise recommendations for individuals with osteoporosis or osteoporotic vertebral fracture. Osteoporos Int. 2014, 25, 821–835. [Google Scholar] [CrossRef]
- Miyakoshi, N.; Hongo, M.; Maekawa, S.; Ishikawa, Y.; Shimada, Y.; Itoi, E. Back extensor strength and lumbar spinal mobility are predictors of quality of life in patients with postmenopausal osteoporosis. Osteoporos Int. 2007, 18, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Giangregorio, L.M.; MacIntyre, N.J.; Thabane, L.; Skidmore, C.J.; Papaioannou, A. Exercise for improving outcomes after osteoporotic vertebral fracture. Cochrane Database Syst. Rev. 2013, CD008618. [Google Scholar] [CrossRef] [PubMed]
- Varahra, A.; Rodrigues, I.; MacDermid, J.; Bryant, D.; Birmingham, T. Exercise to improve functional outcomes in persons with osteoporosis: A systematic review and meta-analysis. Osteoporos Int. 2018, 29, 265–286. [Google Scholar] [CrossRef]
- International Federation for Adapted Physical Activity. 2014. What Is APA. Available online: http://ifapa.net/what-is-apa/ (accessed on 14 June 2019).
- European Innovation Partnership on Active and Healthy Ageing. 2017. Adapted Physical Activity Programmes. Available online: https://ec.europa.eu/eip/ageing/repository/adapted-physical-activity-programmes-programmi-di-attivita-fisica-adattata_en (accessed on 14 June 2019).
- Hudon, C.; Fortin, M.; Vanasse, A. Cumulative Illness Rating Scale was a reliable and valid index in a family practice context. J. Clin. Epidemiol. 2005, 58, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Washburn, R.A.; McAuley, E.; Katula, J.; Mihalko, S.L.; Boileau, R.A. The physical activity scale for the elderly (PASE): Evidence for validity. J. Clin. Epidemiol. 1999, 52, 643–651. [Google Scholar] [CrossRef]
- Park, H. The impact of osteoporosis on health-related quality of life in elderly women. Biomed. Res. 2018, 29, 3223–3227. [Google Scholar] [CrossRef]
- Moreira, L.D.F.; Oliveira, M.L.d.; Lirani-Galvão, A.P.; Marin-Mio, R.V.; Santos, R.N.D.; Lazaretti-Castro, M. Physical exercise and osteoporosis: Effects of different types of exercises on bone and physical function of postmenopausal women. Arq. Bras. Endocrinol. Metabol. 2014, 58, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Sinaki, M.; Pfeifer, M.; Preisinger, E.; Itoi, E.; Rizzoli, R.; Boonen, S.; Geusens, P.; Minne, H.W. The role of exercise in the treatment of osteoporosis. Curr. Osteoporos. Rep. 2010, 8, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Badia, X.; Díez-Pérez, A.; Lahoz, R.; Lizán, L.; Nogués, X.; Iborra, J. The ECOS-16 questionnaire for the evaluation of health related quality of life in post-menopausal women with osteoporosis. Health Qual. Life Outcomes 2004, 2, 41. [Google Scholar] [CrossRef] [PubMed]
- Badia, X.; Prieto, L.; Roset, M.; Díez-Pérez, A.; Herdman, M. Development of a short osteoporosis quality of life questionnaire by equating items from two existing instruments. J. Clin. Epidemiol. 2002, 55, 32–40. [Google Scholar] [CrossRef]
- Salaffi, F.; Malavolta, N.; Cimmino, M.; Di Matteo, L.; Scendoni, P.; Carotti, M.; Stancati, A.; Mulé, R.; Frigato, M.; Gutierrez, M. Validity and reliability of the Italian version of the ECOS-16 questionnaire in postmenopausal women with prevalent vertebral fractures due to osteoporosis. Clin. Exp. Rheumatol. 2007, 25, 390–403. [Google Scholar]
- Rabin, R.; Charro, F.D. EQ-SD: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Dewan, N.; MacDermid, J.C. Fall efficacy scale-international (FES-I). J. Physiother. 2014, 60, 60. [Google Scholar] [CrossRef]
- Hauer, K.A.; Kempen, G.I.; Schwenk, M.; Yardley, L.; Beyer, N.; Todd, C.; Oster, P.; Zijlstra, G.R. Validity and sensitivity to change of the falls efficacy scales international to assess fear of falling in older adults with and without cognitive impairment. Gerontology 2011, 57, 462–472. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Richman, D.; Powell, L. Falls efficacy as a measure of fear of falling. J. Gerontol. 1990, 45, P239–P243. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; Huskisson, E. Graphic representation of pain. Pain 1976, 2, 175–184. [Google Scholar] [CrossRef]
- Huskisson, E.C. Measurement of pain. Lancet 1974, 304, 1127–1131. [Google Scholar] [CrossRef]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Demers, C.; McKelvie, R.S.; Negassa, A.; Yusuf, S. RESOLVD Pilot Study Investigators Reliability, validity, and responsiveness of the six-minute walk test in patients with heart failure. Am. Heart J. 2001, 142, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Macko, R.F.; Ivey, F.M.; Forrester, L.W.; Hanley, D.; Sorkin, J.D.; Katzel, L.I.; Silver, K.H.; Goldberg, A.P. Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: A randomized, controlled trial. Stroke 2005, 36, 2206–2211. [Google Scholar] [CrossRef] [PubMed]
- Enright, P.L. The six-minute walk test. Respir Care 2003, 48, 783–785. [Google Scholar]
- Shipp, K.; Purser, J.; Gold, D.; Pieper, C.; Sloane, R.; Schenkman, M.; Lyles, K. Timed loaded standing: A measure of combined trunk and arm endurance suitable for people with vertebral osteoporosis. Osteoporos. Int. 2000, 11, 914–922. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Max, J.; Noffal, G. The reliability and validity of a chair sit-and-reach test as a measure of hamstring flexibility in older adults. Res. Q Exerc. Sport. 1998, 69, 338–343. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associate: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Papaioannou, A.; Adachi, J.; Winegard, K.; Ferko, N.; Parkinson, W.; Cook, R.; Webber, C.; McCartney, N. Efficacy of home-based exercise for improving quality of life among elderly women with symptomatic osteoporosis-related vertebral fractures. Osteoporos. Int. 2003, 14, 677–682. [Google Scholar] [CrossRef]
- Rossini, M.; Adami, S.; Bertoldo, F.; Diacinti, D.; Gatti, D.; Giannini, S.; Giusti, A.; Malavolta, N.; Minisola, S.; Osella, G.; et al. Guidelines for the Diagnosis, Prevention and Treatment of Osteoporosis. Italian Society of Osteoporosis and Diseases of Mineral and Skeletal Metabolism. Available online: https://www.siommms.it/wp-content/uploads/2014/07/Linee-Guida-OSTEOPOROSI-Reumatismo-2016.pdf (accessed on 14 June 2019).
- Bergland, A.; Thorsen, H.; Kåresen, R. Effect of exercise on mobility, balance, and health-related quality of life in osteoporotic women with a history of vertebral fracture: A randomized, controlled trial. Osteoporos. Int. 2011, 22, 1863–1871. [Google Scholar] [CrossRef] [PubMed]
- Evstigneeva, L.; Lesnyak, O.; Bultink, I.; Lems, W.; Kozhemyakina, E.; Negodaeva, E.; Guselnikova, G.; Belkin, A. Effect of twelve-month physical exercise program on patients with osteoporotic vertebral fractures: A randomized, controlled trial. Osteoporos. Int. 2016, 27, 2515–2524. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.; Bergland, A. The effect of exercise and education on fear of falling in elderly women with osteoporosis and a history of vertebral fracture: Results of a randomized controlled trial. Osteoporos. Int. 2014, 25, 2017–2025. [Google Scholar] [CrossRef] [PubMed]
- Stanghelle, B.; Bentzen, H.; Giangregorio, L.; Pripp, A.H.; Bergland, A. Effect of a resistance and balance exercise programme for women with osteoporosis and vertebral fracture: Study protocol for a randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Romano Spica, V.; Macini, P.; Fara, G.M.; Giammanco, G. GSMS-Working Group on Movement Sciences for Health. Adapted Physical Activity for the promotion of health and the prevention of multifactorial chronic diseases: The Erice Charter. Ann. Ig. 2015, 27, 406–414. [Google Scholar]
- Weinrich, M.; Stuart, M.; Benvenuti, F. Community-based exercise for chronic disease management: An Italian design for the United States? Neurorehabil. Neural Repair 2014, 28, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Calugi, S.; Taricco, M.; Rucci, P.; Fugazzaro, S.; Stuart, M.; Dallolio, L.; Pillastrini, P.; Fantini, M.P. EFG/2009 investigators Effectiveness of adaptive physical activity combined with therapeutic patient education in stroke survivors at twelve months: A non-randomized parallel group study. Eur. J. Phys. Rehabil. Med. 2016, 52, 72–80. [Google Scholar]
- Regione Emilia Romagna. 2016. Indirizzi Regionali per la Promozione Dell’attività Fisica e Della Prescrizione Dell’esercizio Fisico Nelle Persone Con Patologie Croniche e Del Codice Etico Delle Palestre e Delle Associazioni Sportive Che Promuovono Salute. Delibera Della Giunta Regionale 2127/2016. Available online: http://salute.regione.emilia-romagna.it/documentazione/leggi/regionali/dgr-2127-2016/dgr-2127-2016/view (accessed on 14 June 2019).
- Taricco, M.; Dallolio, L.; Calugi, S.; Rucci, P.; Fugazzaro, S.; Stuart, M.; Pillastrini, P.; Fantini, M.P. EFG [Esercizio Fisico di Gruppo]/2009 Investigators Impact of adapted physical activity and therapeutic patient education on functioning and quality of life in patients with postacute strokes. Neurorehabil. Neural Repair 2014, 28, 719–728. [Google Scholar] [CrossRef]
- Regione Emilia Romagna. 2014. L’esercizio Fisico Come Strumento di Prevenzione e Trattamento Delle Malattie Croniche. L’esperienza Dell’emilia-Romagna Nella Prescrizione Dell’attività Fisica. Contributi n. 78/2014. Available online: http://salute.regione.emilia-romagna.it/documentazione/rapporti/contributi/Contributi%2078%20attivita%20fisica%20e%20malattie%20croniche.pdf/view (accessed on 14 June 2019).
- Sinaki, M. Exercise for patients with osteoporosis: Management of vertebral compression fractures and trunk strengthening for fall prevention. PMR 2012, 4, 882–888. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Moderate or severe respiratory failure; 2. Recent pulmonary embolism; 3. Endocarditis, myocarditis, or recent pericarditis; 4. Advanced intermittent claudication (study of Fontaine ≥3); 5. Myocardial infarction for at least three months, or unstable angina or stress angina; 6. Heart failure > III NYHA Class; 7. Severe arterial hypertension (systolic ≥180 mmHg or diastolic ≥110 mmHg); 8. Abdominal aortic aneurysm on ultrasound (transverse caliber >3.5 cm); 9. Anomalies of the rhythm that can represent a contraindication to the performance of moderate intensity physical activity; 10. Arthrosis or fractures with severe limb limitation; 11. Paralysis or important neuromotor disorders; 12. Body Mass Index ≤18 or ≥32 kg/m2; 13. Neoplastic disease or with poor prognosis; 14. Pre-existence of physical exercise administered; 15. Haemoglobin <11 g/dL; 16. Other diseases that may hinder or prevent moderate intensity physical activity. |
| Duration | Warm Up | Workout | Cool Down |
|---|---|---|---|
| 15 min | 35 min | 10 min | |
| Aim | Cardio-respiratory conditioning, increase body temperature and metabolism, joint mobilization, upper and lower limb coordination, proprioception and postural education | Bodyweight exercises for muscular reinforcement and neuromuscular activation, increasing muscle strength and balance, without weights. | Stretching, breathing education, and muscle relaxation maintaining body awareness, collecting individual feedback on the session, in order to reacquire autonomy and active self-management |
| Type of exercise | Multi-articular exercises able to safely solicit all the main muscle groups; focus directed to joint mobilization, balance, and postural control during walking | Resistance exercise affecting all the main muscle groups was performed using isometric and dynamic bodyweight exercises. | Predominantly exercises in an upright and supine static position, able to stretch the main muscles, holding a stretch position for up to 30 s. |
| Trainer’s role |
| ||
| Characteristics | APA Group (n = 26) N (%) or mean ± SD | CG (n = 18) N (%) or mean ± SD | t Test; p |
|---|---|---|---|
| Age | 67.6 ± 4.6 | 67.4 ± 4.7 | 0.124; 0.902 |
| Body mass index | 24.7 ± 3.6 | 23.9 ± 3.4 | 0.820; 0.417 |
| Classification of osteoporosis | |||
| Primary | 23 (82.1%) | 17 (94.4%) | 1.462; 0.227 |
| Secondary | 5 (17.9%) | 1 (5.6%) | |
| Number of vertebral fractures | 2.0 ± 1.2 | 1.8 ± 1.3 | 0.549; 0.586 not significant |
| Number of falls | 3 (10.7%) | 2 (11.1%) | |
| Osteoporosis of parents or siblings | 12 (42.9%) | 8 (44.4%) | 0.011; 0.916 |
| Early menopause (<45 y) | 2 (7.1%) | 0 (0%) | 1.344; 0.246 |
| Dietary deficiencies in vitamin D | 0 (0%) | 0 (0%) | - |
| Amenorrhea (>6 m) | 0 (0%) | 1 (5.6%) | 1.590; 0.207 |
| Anorexia nervosa | 1 (3.6%) | 2 (11.1%) | 1.023; 0.312 |
| Glucocorticosteroids | 2 (7.1%) | 0 (0%) | 1.344; 0.246 |
| Smokers | 5 (17.9%) | 1 (5.6%) | 1.462; 0.227 |
| Alcohol a | 0 (0%) | 0 (0%) | - |
| Physical activity (<30 min) b | 13 (46.4%) | 7 (38.9%) | 0.253; 0.615 |
| CIRS c | 27 (96,4%) | 17 (94.4%) | 0.104; 0.747 |
| Severity Index | 0.2 ± 0.1 | 0.2 ± 0.1 | −0.680; 0.500 |
| Osteoporosis medication | 28 (100%) | 18 (100%) | - |
| PASE | 102.3 ± 46.6 | 141.78 ± 70.7 | −2.286; 0.027 |
| Leisure time activity | 25.3 ± 38.4 | 58.2 ± 50.1 | −2.515; 0.016 |
| Household activity | 74.0 ± 33.7 | 80.1 ± 37.7 | −0.570; 0.572 |
| Work-related activity | 3 ± 7.5 | 3.5 ± 8.1 | −0.215; 0.831 |
| Variables | APA Group (N = 22) | Control Group (N = 18) | Between Groups a p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Change | Within Group p Value | Baseline | Follow-Up | Change | Within Group p Value | ||
| ECOS-16 | 2.49 ± 0.67 | 2.04 ± 0.57 | −0.5 ± 0.5 | 0.001 | 1.97 ± 0.61 | 1.98 ± 0.59 | 0.0 ± 0.3 | 0.329 | 0.020 |
| Pain score | 2.68 ± 0.84 | 2.22 ± 0.84 | −0.5 ± 0.7 | 0.014 | 2.23 ± 0.98 | 2.22 ± 0.80 | 0.0 ± 0.7 | 0.943 | 0.160 |
| Physical Function score | 1.95 ± 0.60 | 1.55 ± 0.49 | −0.4 ± 0.5 | 0.003 | 1.59 ± 0.50 | 1.56 ± 0.56 | 0.0 ± 0.4 | 0.630 | 0.120 |
| Psychosocial score | 2.36 ± 1.01 | 2.07 ± 0.81 | −0.4 ± 0.7 | 0.048 | 1.83 ± 0.70 | 1.89 ± 0.73 | 0.1 ± 0.4 | 0.617 | 0.200 |
| Fear of Illness score | 3.59 ± 0.91 | 2.86 ± 1.31 | −0.7 ± 1.0 | 0.005 | 2.50 ± 0.99 | 2.64 ± 1.25 | 0.1 ± 0.8 | 0.297 | 0.020 |
| PCS | 2.31 ± 0.68 | 1.89 ± 0.64 | −0.4 ± 0.5 | 0.002 | 1.91 ± 0.69 | 1.89 ± 0.64 | 0.0 ± 0.4 | 0.955 | 0.067 |
| MCS | 2.98 ± 0.79 | 2.46 ± 0.88 | −0.5 ± 0.6 | 0.002 | 2.17 ± 0.70 | 2.26 ± 0.77 | 0.1 ± 0.5 | 0.262 | 0.027 |
| EuroQoL VAS | 65.00 ± 18.00 | 70.24 ± 18.67 | 6.0 ± 16.6 | 0.126 | 71.11 ± 15.01 | 73.06 ± 18.24 | 1.9 ± 12.1 | 0.503 | 0.589 |
| FES-I | 29.09 ± 8.18 | 24.41 ± 6.71 | −4.7 ± 7.4 | 0.006 | 23.83 ± 6.60 | 24.72 ± 8.00 | 0.9 ± 2.5 | 0.181 | 0.059 |
| Lumbar back pain VAS | 4.87 ± 2.33 | 3.65 ± 2.75 | −1.2 ± 2.6 | 0.029 | 3.73 ± 2.76 | 4.03 ± 2.51 | 0.3 ± 3.3 | 0.758 | 0.719 |
| Tinetti Scale Total | 24.77 ± 5.42 | 27.59 ± 0.80 | 2.8 ± 5.2 | 0.003 | 25.83 ± 3.13 | 25.11 ± 3.71 | −0.7 ± 2.4 | 0.203 | 0.002 |
| Balance | 14.00 ± 2.96 | 15.68 ± 0.65 | 1.7 ± 2.8 | 0.005 | 14.67 ± 1.75 | 14.11 ± 1.97 | −0.6 ± 1.7 | 0.190 | 0.001 |
| Gait | 10.77 ± 2.56 | 11.91 ± 0.29 | 1.1 ± 2.5 | 0.042 | 11.17 ± 1.69 | 11.00 ± 1.85 | −0.2 ± 1.4 | 0.606 | 0.014 |
| 6-MWT | 395.62 ± 66.23 | 447.80 ± 57.31 | 52.2 ± 42.1 | <0.001 | 420.52 ± 60.65 | 411.99 ± 56.99 | −8.5 ± 45.2 | 0.420 | <0.001 |
| Borg Scale | 3.19 ± 1.75 | 1.68 ± 1.09 | −1.5 ± 1.5 | 0.001 | 2.75 ± 2.15 | 2.33 ± 1.50 | −0.3 ± 2.0 | 0.605 | 0.024 |
| Chair Sit-and-Reach right | 90.19 ± 12.32 | 96.36 ± 1.77 | 6.5 ± 8.0 | 0.002 | 94.64 ± 0.44 | 94.00 ± 10.10 | −0.6 ± 11.0 | 0.660 | 0.106 |
| Chair Sit-and-Reach left | 89.98 ± 11.22 | 97.05 ± 11.05 | 7.3 ± 7.6 | 0.001 | 94.72 ± 10.68 | 93.53 ± 8.89 | −1.2 ± 9.3 | 0.831 | 0.026 |
| Parameter | Effect Size (d) |
|---|---|
| 6-MWT | 1.390 |
| ECOS-16 | 1.204 |
| FES-I | 1.007 |
| Chair Sit-and-Reach left | 1.000 |
| Tinetti Scale Balance | 0.969 |
| Tinetti Scale Total | 0.871 |
| Chair Sit-and-Reach right | 0.739 |
| Borg Scale | 0.654 |
| Tinetti Scale Gait | 0.639 |
| Lumbar back pain VAS | 0.510 |
| EuroQoL VAS | 0.276 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marini, S.; Leoni, E.; Raggi, A.; Sanna, T.; Malavolta, N.; Angela, B.; Maietta Latessa, P.; Dallolio, L. Proposal of an Adapted Physical Activity Exercise Protocol for Women with Osteoporosis-Related Vertebral Fractures: A Pilot Study to Evaluate Feasibility, Safety, and Effectiveness. Int. J. Environ. Res. Public Health 2019, 16, 2562. https://doi.org/10.3390/ijerph16142562
Marini S, Leoni E, Raggi A, Sanna T, Malavolta N, Angela B, Maietta Latessa P, Dallolio L. Proposal of an Adapted Physical Activity Exercise Protocol for Women with Osteoporosis-Related Vertebral Fractures: A Pilot Study to Evaluate Feasibility, Safety, and Effectiveness. International Journal of Environmental Research and Public Health. 2019; 16(14):2562. https://doi.org/10.3390/ijerph16142562
Chicago/Turabian StyleMarini, Sofia, Erica Leoni, Alessandra Raggi, Tiziana Sanna, Nazzarena Malavolta, Buffa Angela, Pasqualino Maietta Latessa, and Laura Dallolio. 2019. "Proposal of an Adapted Physical Activity Exercise Protocol for Women with Osteoporosis-Related Vertebral Fractures: A Pilot Study to Evaluate Feasibility, Safety, and Effectiveness" International Journal of Environmental Research and Public Health 16, no. 14: 2562. https://doi.org/10.3390/ijerph16142562