Depression among Patients with HIV/AIDS: Research Development and Effective Interventions (GAPRESEARCH)

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Data Analysis
3. Results
3.1. Number of Published Items and Publication Trend
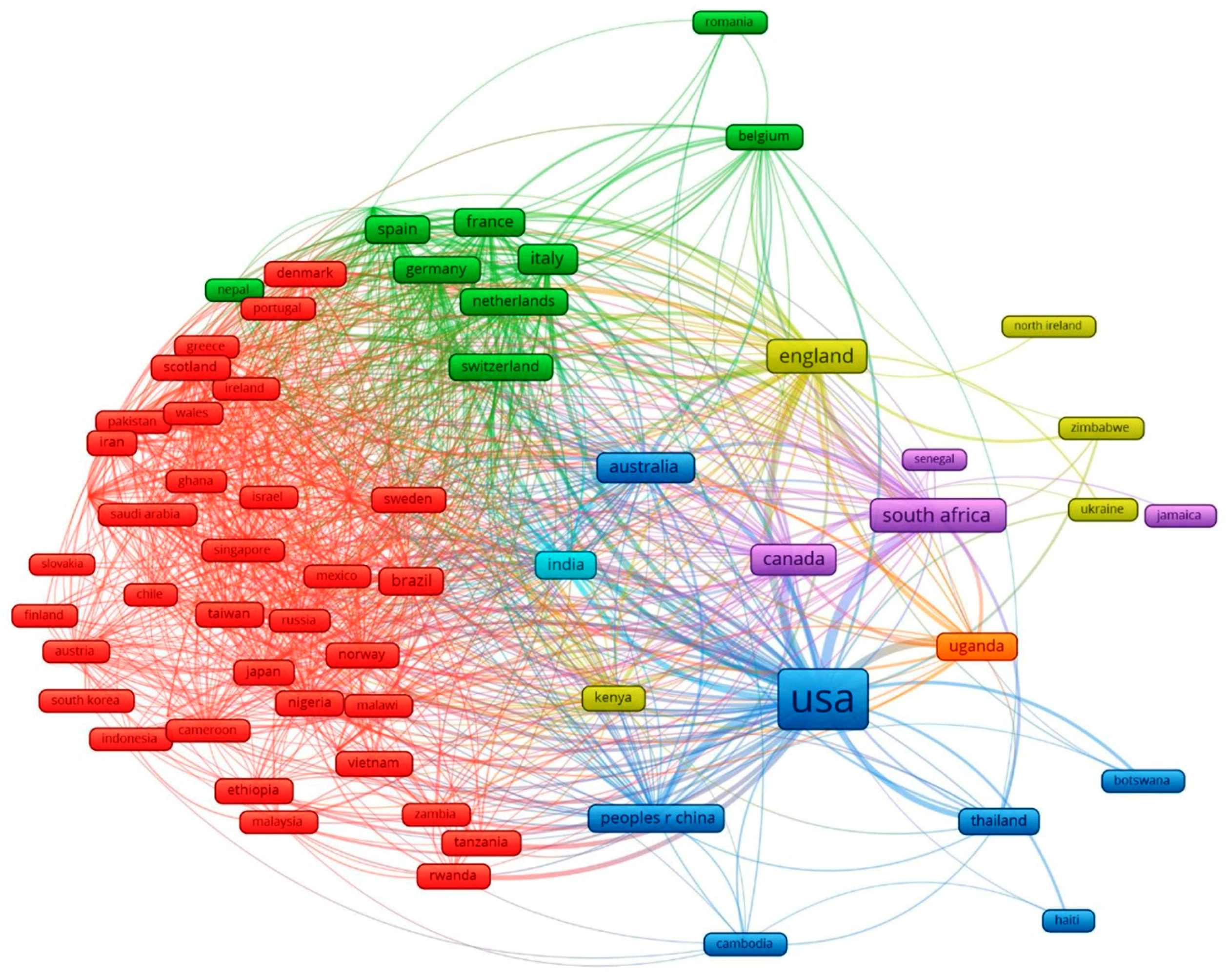
3.2. Co-Authorship Network
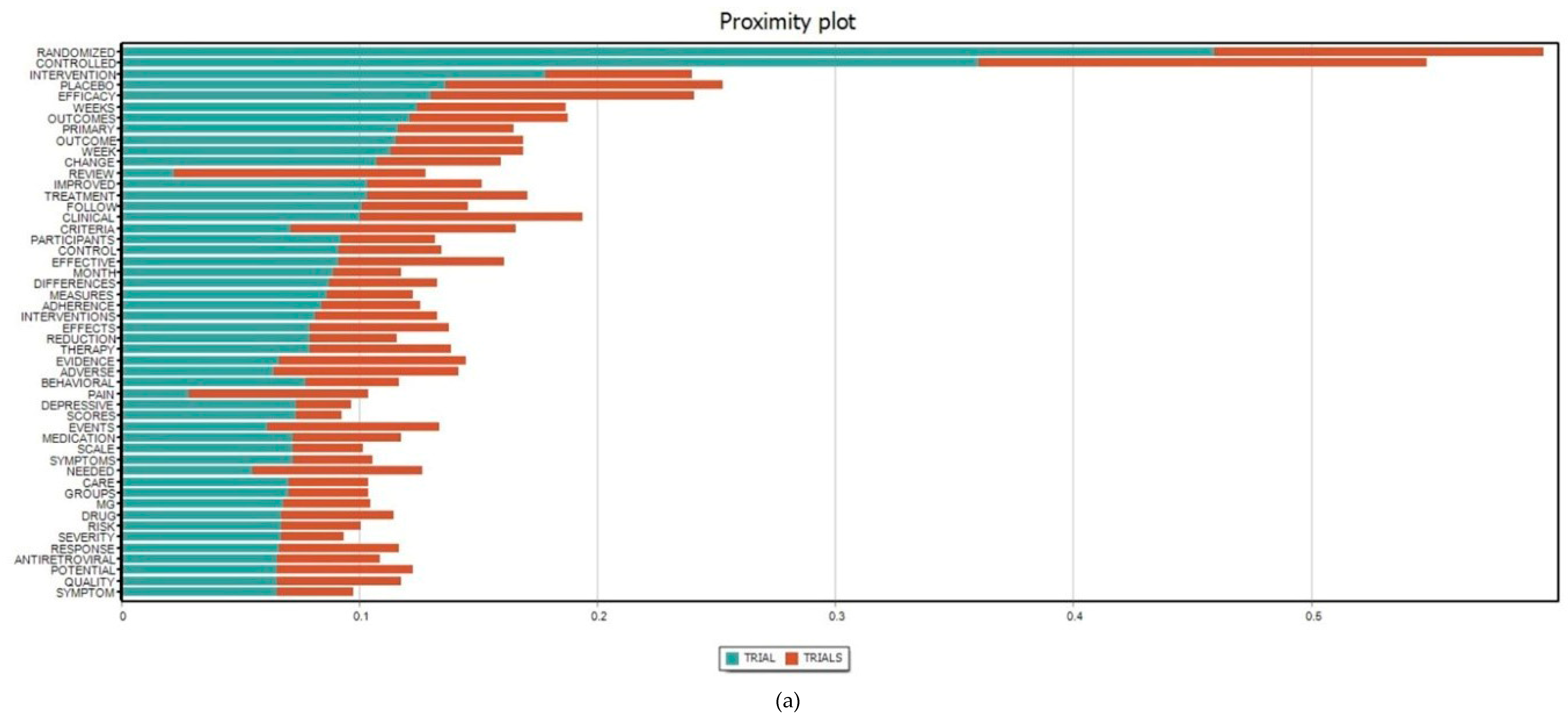
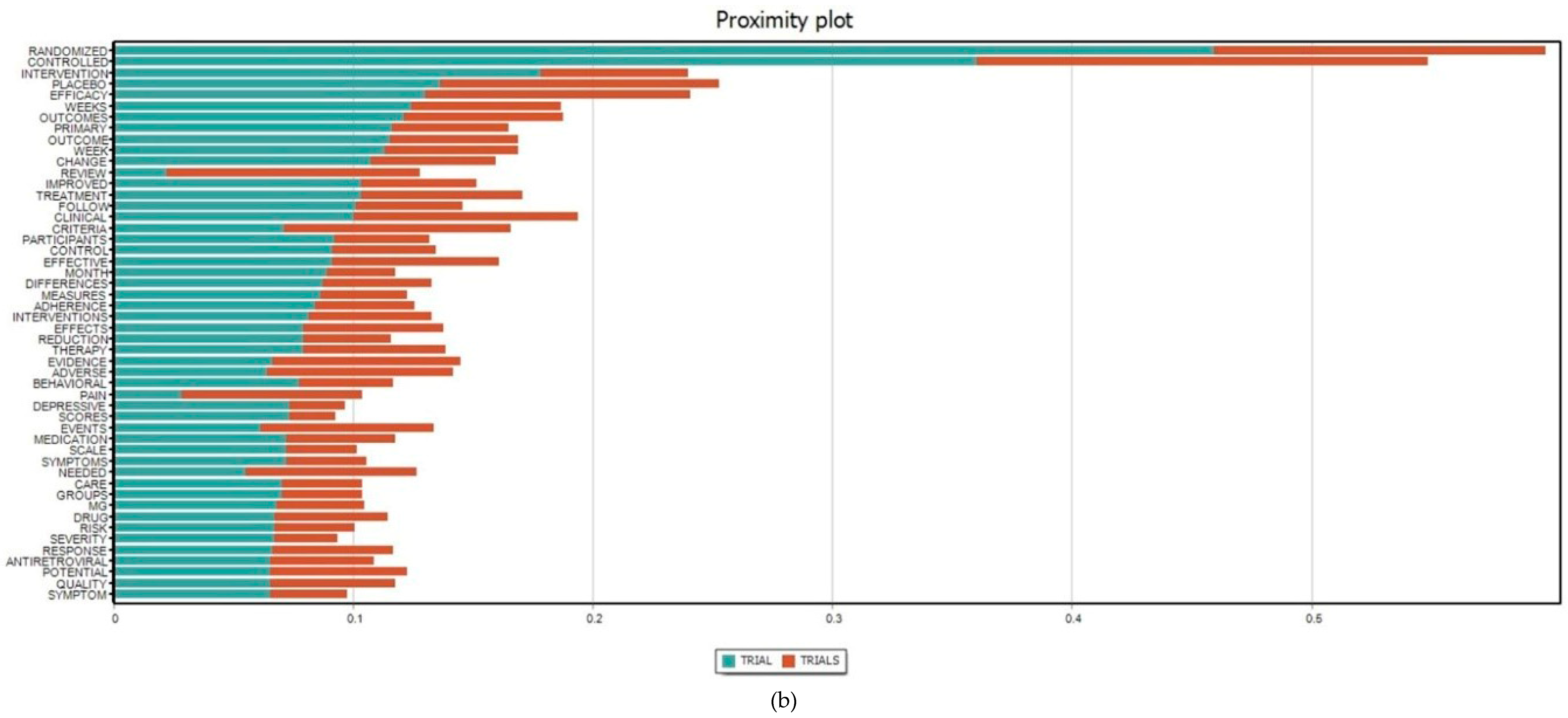
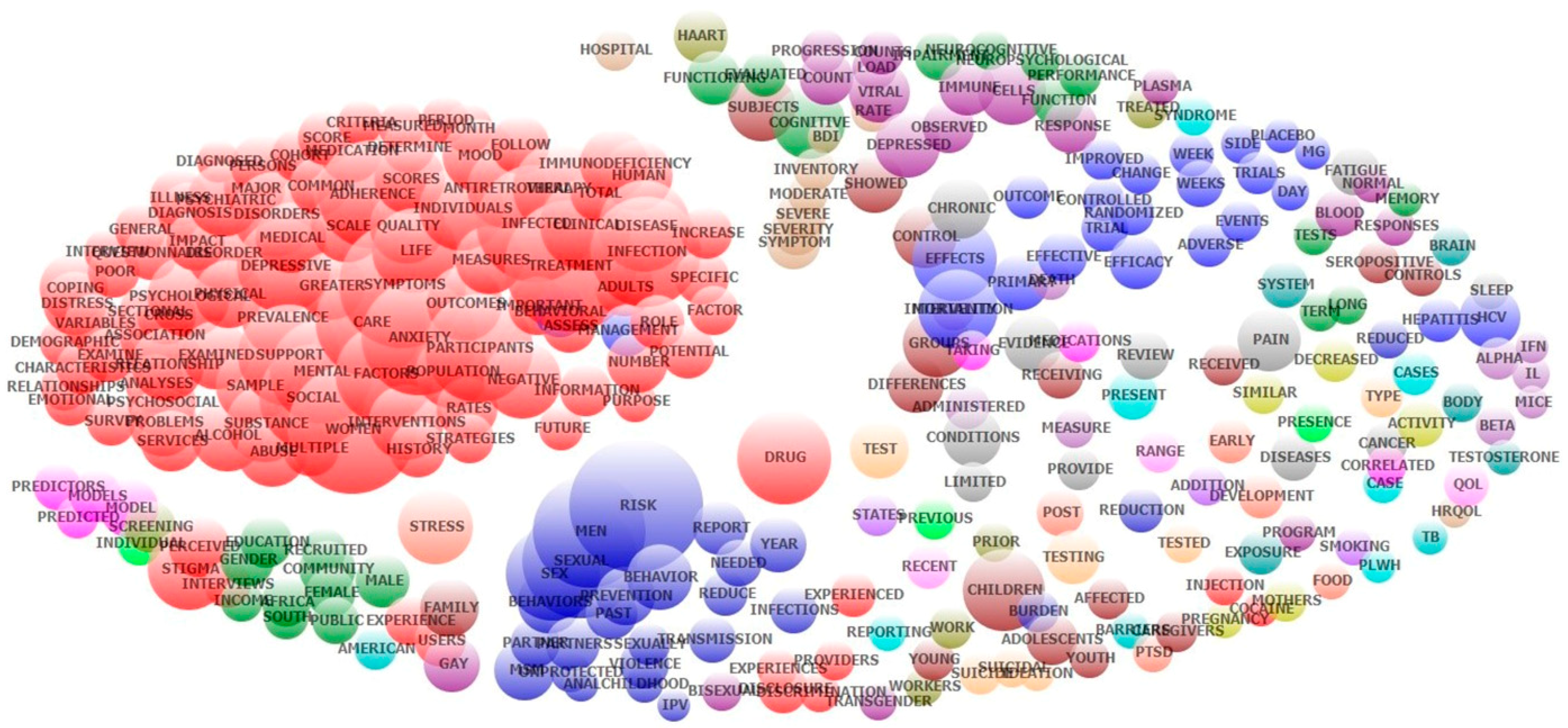
3.3. Keyword Co-Occurrence and Research Domains
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- World Health Organization. Data on the Size of the HIV/AIDS Epidemic. Available online: http://apps.who.int/gho/data/view.main.22100WHO?lang=en (accessed on 26 January 2019).
- Uthman, O.A.; Magidson, J.F.; Safren, S.A.; Nachega, J.B. Depression and adherence to antiretroviral therapy in low-, middle- and high-income countries: A systematic review and meta-analysis. Curr. HIV/AIDS Rep. 2014, 11, 291–307. [Google Scholar] [CrossRef]
- Marcus, M.; Yasamy, M.T.; Ommeren, M.v.; Chisholm, D.; Saxena, S. Depression: A Global Public Health Concern. WHO Department of Mental Health and Substance Abuse, 2017. Available online: https://www.who.int/mental_health/management/depression/who_paper_depression_wfmh_2012.pdf (accessed on 11 April 2019).
- World Health Organization (WHO). Key Facts; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Abas, M.; Ali, G.C.; Nakimuli-Mpungu, E.; Chibanda, D. Depression in people living with HIV in sub-saharan africa: Time to act. Trop. Med. Int. Health 2014, 19, 1392–1396. [Google Scholar] [CrossRef]
- Kingori, C.; Haile, Z.T.; Ngatia, P. Depression symptoms, social support and overall health among HIV-positive individuals in kenya. Int. J. STD AIDS 2015, 26, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Wroe, E.B.; Hedt-Gauthier, B.L.; Franke, M.F.; Nsanzimana, S.; Turinimana, J.B.; Drobac, P. Depression and patterns of self-reported adherence to antiretroviral therapy in rwanda. Int. J. STD AIDS 2015, 26, 257–261. [Google Scholar] [CrossRef]
- Memiah, P.; Shumba, C.; Etienne-Mesubi, M.; Agbor, S.; Hossain, M.B.; Komba, P.; Niyang, M.; Biadgilign, S. The effect of depressive symptoms and cd4 count on adherence to highly active antiretroviral therapy in sub-saharan africa. J. Int. Assoc. Provid. AIDS Care 2014, 13, 346–352. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- E Silva, A.C.O.; Reis, R.K.; Nogueira, J.A.; Gir, E. Quality of life, clinical characteristics and treatment adherence of people living with HIV/AIDS. Rev. Lat. Am. Enferm. 2014, 22, 994–1000. [Google Scholar] [CrossRef]
- Akena, D.H.; Musisi, S.; Kinyanda, E. A comparison of the clinical features of depression in HIV-positive and HIV-negative patients in uganda. Afr. J. Psychiatry 2010, 13, 43–51. [Google Scholar] [CrossRef]
- Nel, A.; Kagee, A. The relationship between depression, anxiety and medication adherence among patients receiving antiretroviral treatment in south africa. AIDS Care 2013, 25, 948–955. [Google Scholar] [CrossRef]
- Arseniou, S.; Arvaniti, A.; Samakouri, M. HIV infection and depression. Psychiatry Clin. Neurosci. 2014, 68, 96–109. [Google Scholar] [CrossRef]
- Nanni, M.G.; Caruso, R.; Mitchell, A.J.; Meggiolaro, E.; Grassi, L. Depression in HIV infected patients: A review. Curr. Psychiatry Rep. 2015, 17, 530. [Google Scholar] [CrossRef]
- Fialho, R.; Pereira, M.; Rusted, J.; Whale, R. Depression in HIV and HCV co-infected patients: A systematic review and meta-analysis. Psychol. Health Med. 2017, 22, 1089–1104. [Google Scholar] [CrossRef]
- Gong, B.; Mohammed, M.F.; Nicolaou, S.; Nasrullah, M.; Forster, B.B.; Khosa, F. Diagnostic imaging in disasters: A bibliometric analysis. Disaster Med. Public Health Prep. 2018, 12, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Araújo, C.C.S.D.; Pedron, C.D.; Picoto, W.N. What’s behind crm research? A bibliometric analysis of publications in the crm research field. J. Relatsh. Mark. 2018, 17, 29–51. [Google Scholar] [CrossRef]
- Huang, A. Similarity measures for text document clustering. In Proceedings of the Sixth New Zealand Computer Science Research Student Conference (NZCSRSC2008), Christchurch, New Zealand, 8 April 2008; pp. 9–56. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Estimated HIV Incidence and Prevalence in the United States, 2010–2016; CDC: Atlanta, GA, USA, 2019. [Google Scholar]
- UNAIDS. UNAIDS Data 2018. Available online: https://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf (accessed on 10 April 2019).
- U.S. Embassy & Consulate in Thailand. 25th Anniversary of Thai-Us Partnership on HIV Vaccine Development. Available online: https://th.usembassy.gov/25th-anniversary-of-thai-us-partnership-on-hiv-vaccine-development/ (accessed on 22 February 2019).
- U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). Pepfar 2019 Country Operational Plan Guidance for All Pepfar Countries; PEPFAR: Washington, DC, USA, 2019.
- USAID. HIV/AIDS. Available online: https://www.usaid.gov/cambodia/hivaid (accessed on 22 February 2019).
- Allinder, S.M.; Dattilo, L. The U.S.-Thai Partnership against HIV; CSIS Global Health Policy Center HIV Working Group: Washington, DC, USA, 2017. [Google Scholar]
- Roxburgh, A.; Degenhardt, L.; Copeland, J. Posttraumatic stress disorder among female street-based sex workers in the greater sydney area, australia. BMC Psychiatry 2006, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, J.A.; Grosso, A.; Decker, M.R.; Peitzmeier, S.; Papworth, E.; Diouf, D.; Drame, F.M.; Ceesay, N.; Baral, S. Sexual violence against female sex workers in the gambia: A cross-sectional examination of the associations between victimization and reproductive, sexual and mental health. BMC Public Health 2015, 15, 270. [Google Scholar] [CrossRef]
- Angst, J.; Gamma, A.; Neuenschwander, M.; Ajdacic-Gross, V.; Eich, D.; Rossler, W.; Merikangas, K.R. Prevalence of mental disorders in the zurich cohort study: A twenty year prospective study. Epidemiol. Psichiatr. Soc. 2005, 14, 68–76. [Google Scholar] [CrossRef]
- Kalemi, G.; Gkioka, S.; Tsapatsari, P.; Tzeferakos, G.; Kandri, T.; Psarra, M.L.; Konstantopoulou, F.; Douzenis, A. Stigma and self-esteem: A case of HIV-positive sex-workers. Psychiatriki 2017, 28, 67–74. [Google Scholar] [CrossRef]
- Budhwani, H.; Hearld, K.R.; Hasbun, J.; Charow, R.; Rosario, S.; Tillotson, L.; McGlaughlin, E.; Waters, J. Transgender female sex workers’ HIV knowledge, experienced stigma, and condom use in the dominican republic. PLoS ONE 2017, 12, e0186457. [Google Scholar] [CrossRef]
- Tao, J.; Wang, L.; Kipp, A.M.; Qian, H.Z.; Yin, L.; Ruan, Y.; Shao, Y.; Lu, H.; Vermund, S.H. Relationship of stigma and depression among newly HIV-diagnosed chinese men who have sex with men. AIDS Behav. 2017, 21, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Tang, E. Here are the 27 countries where same-sex marriage is officially legal. Available online: https://abcnews.go.com/culture/story/27-countries-sex-marriage-officially-legal-56041136 (accessed on 12 March 2019).
- Hopkin, M. HIV Can Never be Cured; Nature: London, UK, 2018. [Google Scholar]
- Fekete, E.M.; Williams, S.L.; Skinta, M.D. Internalised HIV-stigma, loneliness, depressive symptoms and sleep quality in people living with HIV. Psychol. Health 2018, 33, 398–415. [Google Scholar] [CrossRef]
- Dantzer, R.; Kelley, K.W. Twenty years of research on cytokine-induced sickness behavior. Brain Behav. Immun. 2007, 21, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Valcour, V.; Chalermchai, T.; Sailasuta, N.; Marovich, M.; Lerdlum, S.; Suttichom, D.; Suwanwela, N.C.; Jagodzinski, L.; Michael, N.; Spudich, S.; et al. Central nervous system viral invasion and inflammation during acute HIV infection. J. Infect. Dis. 2012, 206, 275–282. [Google Scholar] [CrossRef]
- Raedler, T.J. Inflammatory mechanisms in major depressive disorder. Curr. Opin. Psychiatry 2011, 24, 519–525. [Google Scholar] [CrossRef]
- Dantzer, R.; O’Connor, J.C.; Lawson, M.A.; Kelley, K.W. Inflammation-associated depression: From serotonin to kynurenine. Psychoneuroendocrinology 2011, 36, 426–436. [Google Scholar] [CrossRef]
- Schroecksnadel, K.; Sarcletti, M.; Winkler, C.; Mumelter, B.; Weiss, G.; Fuchs, D.; Kemmler, G.; Zangerle, R. Quality of life and immune activation in patients with HIV-infection. Brain Behav. Immun. 2008, 22, 881–889. [Google Scholar] [CrossRef]
- Peluso, M.J.; Meyerhoff, D.J.; Price, R.W.; Peterson, J.; Lee, E.; Young, A.C.; Walter, R.; Fuchs, D.; Brew, B.J.; Cinque, P.; et al. Cerebrospinal fluid and neuroimaging biomarker abnormalities suggest early neurological injury in a subset of individuals during primary HIV infection. J. Infect. Dis. 2013, 207, 1703–1712. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; Hoover, D.R.; Guccione, M.; Dew, M.A.; Wesch, J.E.; Bing, E.G.; Treisman, G.J. Changes in depressive symptoms as AIDS develops. The multicenter AIDS cohort study. Am. J. Psychiatry 1996, 153, 1430–1437. [Google Scholar]
- Penzak, S.R.; Reddy, Y.S.; Grimsley, S.R. Depression in patients with HIV infection. Am. J. Health Syst. Pharm. 2000, 57, 376–386. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year Published | Total Number of Papers | Total Citations | Mean Cite Rate per Year | Total Usage Last 6 Month | Total Usage Last 5 Years | Mean Use Rate Last 6 Month | Mean Use Rate Last 5 Year |
|---|---|---|---|---|---|---|---|
| 2017 | 428 | 565 | 1.32 | 663 | 2018 | 1.55 | 0.94 |
| 2016 | 378 | 1775 | 2.35 | 404 | 3683 | 1.07 | 1.95 |
| 2015 | 330 | 2811 | 2.84 | 272 | 3896 | 0.82 | 2.36 |
| 2014 | 329 | 3978 | 3.02 | 198 | 4083 | 0.60 | 2.48 |
| 2013 | 338 | 5078 | 3.00 | 187 | 4867 | 0.55 | 2.88 |
| 2012 | 323 | 8434 | 4.35 | 208 | 4390 | 0.64 | 2.72 |
| 2011 | 237 | 6059 | 3.65 | 123 | 2680 | 0.52 | 2.26 |
| 2010 | 248 | 6525 | 3.29 | 111 | 2141 | 0.45 | 1.73 |
| 2009 | 218 | 6315 | 3.22 | 102 | 1758 | 0.47 | 1.61 |
| 2008 | 193 | 7629 | 3.95 | 114 | 1825 | 0.59 | 1.89 |
| 2007 | 153 | 7145 | 4.25 | 107 | 1516 | 0.70 | 1.98 |
| 2006 | 181 | 10,994 | 5.06 | 130 | 2044 | 0.72 | 2.26 |
| 2005 | 147 | 7174 | 3.75 | 69 | 1135 | 0.47 | 1.54 |
| 2004 | 127 | 5453 | 3.07 | 53 | 666 | 0.42 | 1.05 |
| 2003 | 121 | 6364 | 3.51 | 64 | 945 | 0.53 | 1.56 |
| 2002 | 116 | 5739 | 3.09 | 46 | 605 | 0.40 | 1.04 |
| 2001 | 109 | 8811 | 4.75 | 49 | 968 | 0.45 | 1.78 |
| 2000 | 105 | 7415 | 3.92 | 63 | 1026 | 0.60 | 1.95 |
| 1999 | 85 | 4077 | 2.52 | 23 | 343 | 0.27 | 0.81 |
| 1998 | 109 | 3682 | 1.69 | 23 | 405 | 0.21 | 0.74 |
| 1997 | 108 | 8473 | 3.74 | 97 | 1114 | 0.90 | 2.06 |
| 1996 | 110 | 4912 | 2.03 | 24 | 288 | 0.22 | 0.52 |
| 1995 | 85 | 2706 | 1.38 | 13 | 217 | 0.15 | 0.51 |
| 1994 | 81 | 2850 | 1.47 | 9 | 128 | 0.11 | 0.32 |
| 1993 | 83 | 3940 | 1.90 | 13 | 202 | 0.16 | 0.49 |
| 1992 | 63 | 3548 | 2.17 | 12 | 149 | 0.19 | 0.47 |
| 1991 | 49 | 2302 | 1.74 | 5 | 71 | 0.10 | 0.29 |
| 1990 | 1 | 24 | 0.86 | 0 | 1 | 0.00 | 0.20 |
| # | Country Settings | Frequency | % | # | Country Settings | Frequency | % |
|---|---|---|---|---|---|---|---|
| 1 | United States | 432 | 22.7% | 31 | Haiti | 13 | 0.7% |
| 2 | South Africa | 203 | 10.7% | 32 | Iran | 13 | 0.7% |
| 3 | Uganda | 102 | 5.4% | 33 | Hong Kong | 10 | 0.5% |
| 4 | China | 89 | 4.7% | 34 | Spain | 10 | 0.5% |
| 5 | India | 73 | 3.8% | 35 | Denmark | 9 | 0.5% |
| 6 | Ireland | 73 | 3.8% | 36 | Jersey | 9 | 0.5% |
| 7 | Canada | 62 | 3.3% | 37 | Dominica | 8 | 0.4% |
| 8 | Brazil | 46 | 2.4% | 38 | Dominican Republic | 8 | 0.4% |
| 9 | Australia | 43 | 2.3% | 39 | Georgia | 8 | 0.4% |
| 10 | United Kingdom | 41 | 2.2% | 40 | Netherlands | 8 | 0.4% |
| 11 | Kenya | 35 | 1.8% | 41 | Ukraine | 8 | 0.4% |
| 12 | Viet Nam | 32 | 1.7% | 42 | Chile | 7 | 0.4% |
| 13 | Tanzania | 28 | 1.5% | 43 | Germany | 7 | 0.4% |
| 14 | Niger | 27 | 1.4% | 44 | Jamaica | 7 | 0.4% |
| 15 | Nigeria | 27 | 1.4% | 45 | Lesotho | 6 | 0.3% |
| 16 | Puerto Rico | 24 | 1.3% | 46 | Malaysia | 6 | 0.3% |
| 17 | Rwanda | 24 | 1.3% | 47 | Peru | 6 | 0.3% |
| 18 | Taiwan | 22 | 1.2% | 48 | Sweden | 6 | 0.3% |
| 19 | Ethiopia | 21 | 1.1% | 49 | Colombia | 5 | 0.3% |
| 20 | Mexico | 21 | 1.1% | 50 | Ghana | 5 | 0.3% |
| 21 | Thailand | 20 | 1.1% | 51 | Mali | 5 | 0.3% |
| 22 | Zambia | 18 | 0.9% | 52 | Namibia | 5 | 0.3% |
| 23 | Malawi | 17 | 0.9% | 53 | Norway | 5 | 0.3% |
| 24 | Zimbabwe | 17 | 0.9% | 54 | Russian Federation | 5 | 0.3% |
| 25 | Botswana | 16 | 0.8% | 55 | Cambodia | 4 | 0.2% |
| 26 | France | 16 | 0.8% | 56 | Congo | 4 | 0.2% |
| 27 | Japan | 16 | 0.8% | 57 | Congo | 4 | 0.2% |
| 28 | Nepal | 15 | 0.8% | 58 | Israel | 4 | 0.2% |
| 29 | Cameroon | 14 | 0.7% | 59 | Senegal | 4 | 0.2% |
| 30 | Italy | 14 | 0.7% | 60 | Singapore | 4 | 0.2% |
| No | Name | Keywords | Eigen Value | Freq | %cases |
|---|---|---|---|---|---|
| 1 | Sex Sexual; Unprotected | sex; unprotected; sexual; anal; partners; msm; risk; behaviors; prevention; behavior; men; partner; sexually | 3.81 | 7005 | 54.74% |
| 2 | Psychological Distress; Emotional | distress; psychological; emotional; anxiety; physical | 1.55 | 3364 | 45.28% |
| 3 | Medical Care | care; providers; medical; services; barriers; primary; interviews | 1.81 | 3455 | 43.64% |
| 4 | Depressed | depressed; anxiety | 1.30 | 2035 | 40.62% |
| 5 | Social Stigma | stigma; discrimination; social; support; disclosure; perceived; experiences | 2.39 | 3374 | 39.16% |
| 6 | Psychiatric; Disorder | psychiatric; disorder; disorders; major; interview; diagnosis | 2.89 | 3188 | 38.36% |
| 7 | Coping Strategies; Social Support | coping; strategies; support; social | 1.41 | 2705 | 35.55% |
| 8 | Scale; Hospital | scale; hospital; questionnaire; total; score | 1.31 | 2390 | 33.07% |
| 9 | Depressive | depressive; symptoms | 1.29 | 2132 | 32.22% |
| 10 | Antiretroviral | antiretroviral; therapy; haart; adherence | 2.66 | 2741 | 29.80% |
| 11 | Adherence To Medication | medication; adherence; medications; antiretroviral; taking | 1.33 | 2384 | 29.02% |
| 12 | Cancer Pain; Chronic Diseases | cancer; pain; diseases; chronic; review; conditions | 1.64 | 1930 | 28.08% |
| 13 | Mortality; Disease Progression | mortality; disease; progression; death | 1.34 | 1680 | 26.89% |
| 14 | Provide Evidence | evidence; limited; review; trials; provide | 1.39 | 1702 | 26.83% |
| 15 | Neuropsychological; Memory Performance | neuropsychological; performance; neurocognitive; impairment; memory; cognitive; tests; function; functioning | 2.76 | 2292 | 25.92% |
| 16 | Violence (IPV); Partner | ipv; violence; partner; women; pregnancy | 1.93 | 1640 | 24.63% |
| 17 | Disorder (PTSD) | ptsd; stress; post; disorder | 1.70 | 1570 | 24.20% |
| 18 | Randomized; Controlled Trial | randomized; trial; controlled; placebo; trials; intervention; efficacy | 3.30 | 2193 | 24.20% |
| 19 | Substance Abuse | abuse; substance; alcohol; childhood | 1.61 | 1800 | 23.60% |
| 20 | Month Follow | month; follow; period; year | 1.52 | 1579 | 23.19% |
| 21 | Control | controls; control; subjects; seropositive | 1.51 | 1422 | 22.95% |
| 22 | Intervention Program | program; community; intervention | 1.46 | 1266 | 22.48% |
| 23 | Examine | examine; purpose; relationships | 1.30 | 1269 | 21.82% |
| 24 | Drug Users | users; drug; injection; cocaine | 2.17 | 1457 | 20.79% |
| 25 | Viral Load; Cells Count | load; viral; count; counts; cells | 1.92 | 1703 | 20.55% |
| 26 | Test | testing; test; tested; tests | 1.42 | 1257 | 20.40% |
| 27 | Gay Men | gay; bisexual; men | 1.88 | 1400 | 20.38% |
| 28 | Life Quality | quality; life; qol; hrqol | 2.09 | 1619 | 20.32% |
| 29 | Human Immunodeficiency | immunodeficiency; human; syndrome | 2.26 | 1891 | 20.30% |
| 30 | Side Effects | effects; side | 1.43 | 1142 | 19.77% |
| 31 | Female | female; male; gender | 1.54 | 1168 | 19.03% |
| 32 | Cross-Sectional | sectional; cross; survey | 2.36 | 1703 | 18.80% |
| 33 | Symptom Severity | symptom; fatigue; sleep; severity; pain | 1.59 | 1177 | 18.27% |
| 34 | Children; Family Caregivers | children; caregivers; affected; mothers; family | 2.05 | 1241 | 18.00% |
| 35 | Response | responses; response; immune | 1.25 | 976 | 16.07% |
| 36 | Persons | persons; states | 1.28 | 756 | 14.57% |
| 37 | Infections; Sexually | infections; sexually; diseases | 1.27 | 883 | 14.43% |
| 38 | Physical | physical | 1.24 | 556 | 11.41% |
| 39 | Perceived | perceived; received | 1.26 | 600 | 11.10% |
| 40 | Brain | brain; system | 1.48 | 505 | 9.32% |
| 41 | Case | cases; case | 1.32 | 491 | 9.20% |
| 42 | History | history | 1.36 | 439 | 9.01% |
| 43 | Youth; Adolescents | youth; adolescents; young | 1.57 | 514 | 8.50% |
| 44 | Adverse Events | events; adverse | 1.39 | 488 | 8.48% |
| 45 | South Africa | africa; south | 1.68 | 584 | 8.23% |
| 46 | Work | workers; work | 1.35 | 401 | 7.45% |
| 47 | Long-Term | long; term | 2.15 | 510 | 6.69% |
| 48 | Suicidal Ideation | suicidal; ideation; suicide | 1.98 | 447 | 5.58% |
| 49 | Hepatitis C Virus (HCV) | hcv; hepatitis | 1.79 | 360 | 5.25% |
| 50 | Testosterone | testosterone; body | 1.37 | 238 | 4.52% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, B.X.; Ho, R.C.M.; Ho, C.S.H.; Latkin, C.A.; Phan, H.T.; Ha, G.H.; Vu, G.T.; Ying, J.; Zhang, M.W.B. Depression among Patients with HIV/AIDS: Research Development and Effective Interventions (GAPRESEARCH). Int. J. Environ. Res. Public Health 2019, 16, 1772. https://doi.org/10.3390/ijerph16101772
Tran BX, Ho RCM, Ho CSH, Latkin CA, Phan HT, Ha GH, Vu GT, Ying J, Zhang MWB. Depression among Patients with HIV/AIDS: Research Development and Effective Interventions (GAPRESEARCH). International Journal of Environmental Research and Public Health. 2019; 16(10):1772. https://doi.org/10.3390/ijerph16101772
Chicago/Turabian StyleTran, Bach Xuan, Roger C. M. Ho, Cyrus S. H. Ho, Carl A. Latkin, Hai Thanh Phan, Giang Hai Ha, Giang Thu Vu, Jiangbo Ying, and Melvyn W. B. Zhang. 2019. "Depression among Patients with HIV/AIDS: Research Development and Effective Interventions (GAPRESEARCH)" International Journal of Environmental Research and Public Health 16, no. 10: 1772. https://doi.org/10.3390/ijerph16101772