Elimination of Schistosoma japonicum Transmission in China: A Case of Schistosomiasis Control in the Severe Epidemic Area of Anhui Province

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
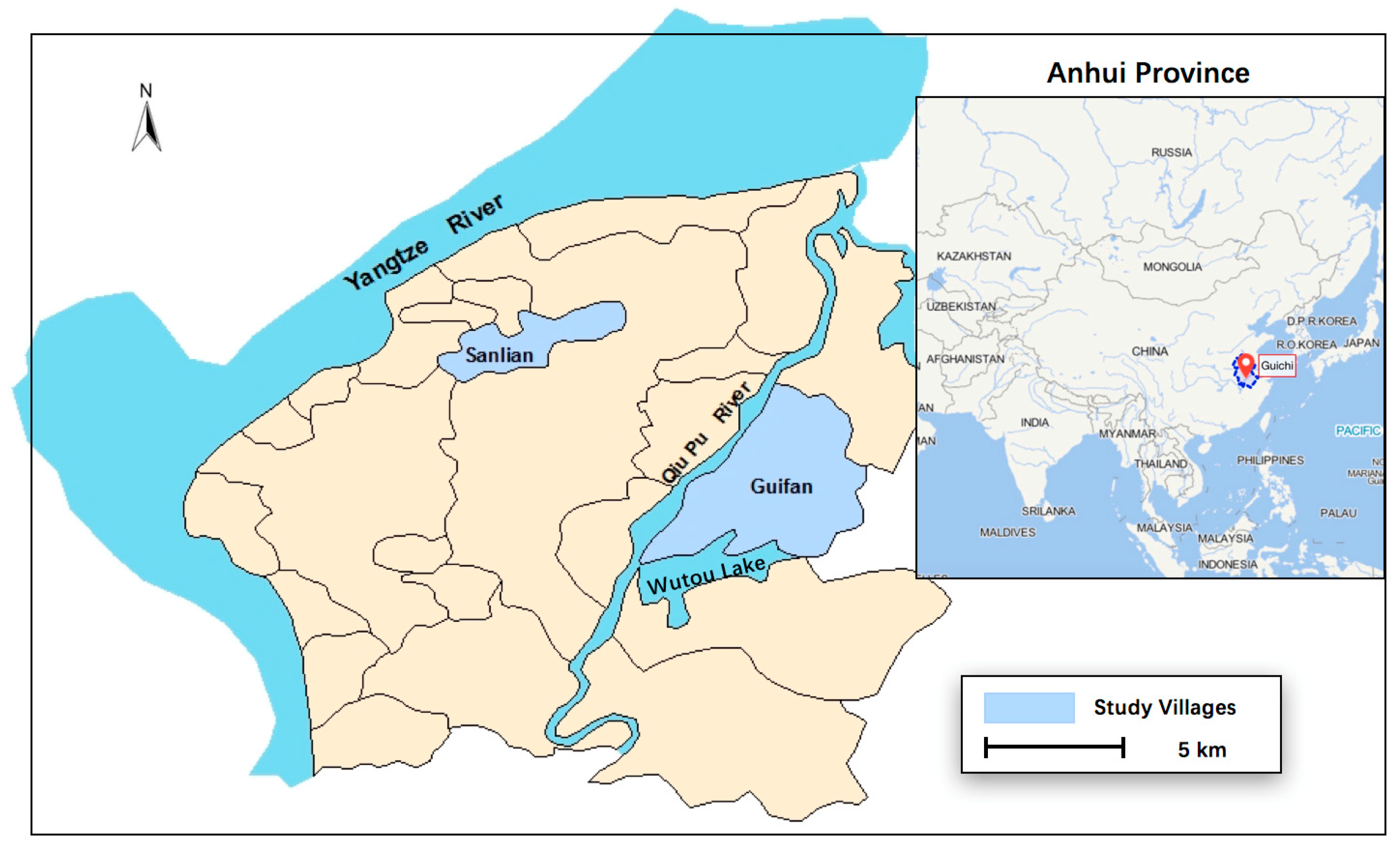
2.1. Study Area
2.2. Intervention Measures
2.3. Disease Diagnosis
2.4. Statistical Analysis
3. Results
Infection in Humans
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Logan, O.T. A case of dysentery in hunan province caused by the trematode Schistosoma japonicum. China Mission. Med. J. 1905, 19, 243–245. [Google Scholar]
- WHO. Schistosomiasis. Different Type of Schistosome. Available online: https://www.who.int/schistosomiasis/epidemiology/table3/en/ (accessed on 11 October 2018).
- King, C.H. Toward the elimination of schistosomiasis. N. Engl. J. Med. 2009, 360, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Mao, S.P.; Shao, B.R. Schistosomiasis control in the People’s Republic of China. Am. J. Trop. Med. Hyg. 1982, 31, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Utzinger, J.; Zhou, X.N. Schistosomiasis control: Experiences and lessons from China. Lancet 2008, 372, 1793–1795. [Google Scholar] [CrossRef]
- Zhou, X.N.; Wang, L.Y.; Chen, M.G.; Wu, X.H.; Jiang, Q.W.; Chen, X.Y.; Zheng, J.; Utzinger, J. The public health significance and control of schistosomiasis in China—Then and now. Acta Trop. 2005, 96, 97–105. [Google Scholar] [CrossRef]
- Warren, K.S.; Su, D.L.; Xu, Z.Y.; Yuan, H.C.; Peters, P.A.; Cook, J.A.; Mott, K.E.; Houser, H.B. Morbidity in schistosomiasis japonica in relation to intensity of infection. A study of two rural brigades in Anhui province, China. N. Engl. J. Med. 1983, 309, 1533–1539. [Google Scholar] [CrossRef]
- Qian, R.F.; Han, S.M.; Ke, Y.F. The epidemic situation of schistosomiasis in Guichi District, Chizhou City, in 2008–2012. J. Trop. Dis. Parasitol. 2014, 12, 108–110. (In Chinese) [Google Scholar]
- Katz, N.; Chaves, A.; Pellegrino, J. A simple device for quantitative stool thick-smear technique in schistosomiasis mansoni. Rev. Inst. Med. Trop. Sao Paulo 1972, 14, 397–400. [Google Scholar]
- Rogan, W.J.; Gladen, B. Estimating prevalence from the results of a screening test. Am. J. Epidemiol. 1978, 107, 71–76. [Google Scholar] [CrossRef]
- Lin, D.D.; Liu, J.X.; Liu, Y.M.; Hu, F.; Zhang, Y.Y.; Xu, J.M.; Li, J.Y.; Ji, M.J.; Bergquist, R.; Wu, G.L.; et al. Routine Kato-Katz technique underestimates the prevalence of Schistosoma japonicum: A case study in an endemic area of the People’s Republic of China. Parasitol. Int. 2008, 57, 281–286. [Google Scholar] [CrossRef]
- Bosso, L.; Lacatena, F.; Varlese, R.; Nocerino, S.; Cristinzio, G.; Russo, D. Plant pathogens but not antagonists change in soil fungal communities across a land abandonment gradient in a mediterranean landscape. Acta Oecol 2017, 78, 1–6. [Google Scholar] [CrossRef]
- Steinbaum, L.; Kwong, L.H.; Ercumen, A.; Negash, M.S.; Lovely, A.J.; Njenga, S.M.; Boehm, A.B.; Pickering, A.J.; Nelson, K.L. Detecting and enumerating soil-transmitted helminth eggs in soil: New method development and results from field testing in Kenya and Bangladesh. PLoS Negl. Trop. Dis. 2017, 11, e0005522. [Google Scholar] [CrossRef]
- Wang, L.D.; Chen, H.G.; Guo, J.G.; Zeng, X.J.; Hong, X.L.; Xiong, J.J.; Wu, X.H.; Wang, X.H.; Wang, L.Y.; Xia, G.; et al. A strategy to control transmission of Schistosoma japonicum in China. N. Engl. J. Med. 2009, 360, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Katz, N.; Rocha, R.S.; Pereira, J.P. Schistosomiasis control in Peri-Peri (Minas Gerais, Brazil) by repeated clinical treatment and molluscicide application. Rev. Inst. Med. Trop. Sao Paulo 1980, 22, 85–93, 203–211. [Google Scholar]
- McCullough, F.S.; Gayral, P.; Duncan, J.; Christie, J.D. Molluscicides in schistosomiasis control. Bull. World Health Organ. 1980, 58, 681–689. [Google Scholar] [PubMed]
- Spear, R.C.; Seto, E.; Remais, J.; Carlton, E.J.; Davis, G.; Qiu, D.; Zhou, X.; Liang, S. Fighting waterborne infectious diseases. Science 2006, 314, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- WHO. The Control of Schistosomiasis: Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1985. [Google Scholar]
- WHO. The Control of Schistosomiasis: Second Report of the WHO Committee; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Bank, T.W. Project: Infectious and Endemic Disease Control Project. Available online: http://projects.worldbank.org/P003624/infectious-endemic-disease-control-project?lang=en (accessed on 10 May 2018).
- Utzinger, J.; Bergquist, R.; Shu-Hua, X.; Singer, B.H.; Tanner, M. Sustainable schistosomiasis control—The way forward. Lancet 2003, 362, 1932–1934. [Google Scholar] [CrossRef]
- Chen, X.Y.; Wang, L.Y.; Cai, J.M.; Zhou, X.N.; Zheng, J.; Guo, J.G.; Wu, X.H.; Engels, D.; Chen, M.G. Schistosomiasis control in China: The impact of a 10-year world bank loan project (1992–2000). Bull. World Health Organ. 2005, 83, 43–48. [Google Scholar]
- Wu, X.H.; Zhang, S.Q.; Xu, X.J.; Huang, Y.X.; Steinmann, P.; Utzinger, J.; Wang, T.P.; Xu, J.; Zheng, J.; Zhou, X.N. Effect of floods on the transmission of schistosomiasis in the Yangtze River valley, People’s Republic of China. Parasitol. Int. 2008, 57, 271–276. [Google Scholar] [CrossRef]
- Yang, G.J.; Liu, L.; Zhu, H.R.; Griffiths, S.M.; Tanner, M.; Bergquist, R.; Utzinger, J.; Zhou, X.N. China’s sustained drive to eliminate neglected tropical diseases. Lancet Infect. Dis. 2014, 14, 881–892. [Google Scholar] [CrossRef]
- Zhou, Y.B.; Zhao, G.M.; Jiang, Q.W. Effects of the praziquantel-based control of schistosomiasis japonica in China. Ann. Trop. Med. Parasitol. 2007, 101, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.N.; Wang, L.Y.; Chen, M.G.; Wang, T.P.; Guo, J.G.; Wu, X.H.; Jiang, Q.W.; Zheng, J.; Chen, X.Y. An economic evaluation of the national schistosomiasis control programme in China from 1992 to 2000. Acta Trop. 2005, 96, 255–265. [Google Scholar] [CrossRef]
- Jiang, Q.W.; Wang, L.Y.; Guo, J.G.; Chen, M.G.; Zhou, X.N.; Engels, D. Morbidity control of schistosomiasis in China. Acta Trop. 2002, 82, 115–125. [Google Scholar]
- Guo, J.G.; Cao, C.L.; Hu, G.H.; Lin, H.; Li, D.; Zhu, R.; Xu, J. The role of ‘passive chemotherapy’ plus health education for schistosomiasis control in China during maintenance and consolidation phase. Acta Trop. 2005, 96, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.N.; Jiang, Q.W.; Wang, T.P.; Lin, D.D.; Wu, X.H. Status and strategy for research development of schistosomiasis control in China. Chin. J. Schistosomiasis Control 2005, 17, 1–3. [Google Scholar]
- Zhou, Y.B.; Liang, S.; Chen, G.X.; Rea, C.; He, Z.G.; Zhang, Z.J.; Wei, J.G.; Zhao, G.M.; Jiang, Q.W. An integrated strategy for transmission control of Schistosoma japonicum in a marshland area of China: Findings from a five-year longitudinal survey and mathematical modeling. Am. J. Trop. Med. Hyg. 2011, 85, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Dong, H.F.; Jiang, M.S. The new national integrated strategy emphasizing infection sources control for schistosomiasis control in China has made remarkable achievements. Parasitol. Res. 2013, 112, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhou, Y.B.; Song, X.X.; Li, S.Z.; Zhong, B.; Wang, T.P.; Bergquist, R.; Zhou, X.N.; Jiang, Q.W. Integrated control strategy of schistosomiasis in the People’s Republic of China: Projects involving agriculture, water conservancy, forestry, sanitation and environmental modification. Adv. Parasitol. 2016, 92, 237–268. [Google Scholar]
- Zhang, Z.; Zhu, R.; Ward, M.P.; Xu, W.; Zhang, L.; Guo, J.; Zhao, F.; Jiang, Q. Long-term impact of the world bank loan project for schistosomiasis control: A comparison of the spatial distribution of schistosomiasis risk in China. PLoS Negl. Trop. Dis. 2012, 6, e1620. [Google Scholar] [CrossRef]
- Zhang, S.Q.; Sun, C.S.; Wang, M.; Lin, D.D.; Zhou, X.N.; Wang, T.P. Epidemiological features and effectiveness of schistosomiasis control programme in lake and marshland region in the People’s Republic of China. Adv. Parasitol. 2016, 92, 39–71. [Google Scholar]
- Sun, L.P.; Wang, W.; Hong, Q.B.; Li, S.Z.; Liang, Y.S.; Yang, H.T.; Zhou, X.N. Approaches being used in the national schistosomiasis elimination programme in China: A review. Infect. Dis. Poverty 2017, 6, 55. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.P.; Wang, W.; Zuo, Y.P.; Zhang, Z.Q.; Hong, Q.B.; Yang, G.J.; Zhu, H.R.; Liang, Y.S.; Yang, H.T. An integrated environmental improvement of marshlands: Impact on control and elimination of schistosomiasis in marshland regions along the Yangtze River, China. Infect. Dis. Poverty 2017, 6, 72. [Google Scholar] [CrossRef]
- Wang, X.; Wang, W.; Wang, P. Long-term effectiveness of the integrated schistosomiasis control strategy with emphasis on infectious source control in China: A 10-year evaluation from 2005 to 2014. Parasitol. Res. 2017, 116, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.N.; Jiang, T.W.; Guo, J.G.; Wang, L.Y.; Jiang, Q.W. Project management model and its evolution in schistosomiasis control programme of China. Chin. J. Schistosomiasis Control 2010, 22, 1–4. [Google Scholar]
- Wang, L.D.; Guo, J.G.; Wu, X.H.; Chen, H.G.; Wang, T.P.; Zhu, S.P.; Zhang, Z.H.; Steinmann, P.; Yang, G.J.; Wang, S.P.; et al. China’s new strategy to block Schistosoma japonicum transmission: Experiences and impact beyond schistosomiasis. Trop. Med. Int. Health 2009, 14, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.B.; Wang, T.P.; Rudge, J.W.; Donnelly, C.A.; Fang, G.R.; Webster, J.P. Contrasting reservoirs for Schistosoma japonicum between marshland and hilly regions in Anhui, China—A two-year longitudinal parasitological survey. Parasitology 2010, 137, 99–110. [Google Scholar] [CrossRef]
- Colley, D.G.; Bustinduy, A.L.; Secor, W.E.; King, C.H. Human schistosomiasis. Lancet 2014, 383, 2253–2264. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.B.; Liang, S.; Jiang, Q.W. Factors impacting on progress towards elimination of transmission of schistosomiasis japonica in China. Parasit. Vectors 2012, 5, 275. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.B.; Yang, M.X.; Wang, Q.Z.; Zhao, G.M.; Wei, J.G.; Peng, W.X.; Jiang, Q.W. Field comparison of immunodiagnostic and parasitological techniques for the detection of schistosomiasis japonica in the People’s Republic of China. Am. J. Trop. Med. Hyg. 2007, 76, 1138–1143. [Google Scholar] [CrossRef]
- Wang, W.; Dai, J.R.; Liang, Y.S. Apropos: Factors impacting on progress towards elimination of transmission of schistosomiasis japonica in China. Parasit. Vectors 2014, 7, 408. [Google Scholar] [CrossRef]
- Lindholz, C.G.; Favero, V.; Verissimo, C.M.; Candido, R.R.F.; de Souza, R.P.; Dos Santos, R.R.; Morassutti, A.L.; Bittencourt, H.R.; Jones, M.K.; St Pierre, T.G.; et al. Study of diagnostic accuracy of Helmintex, Kato-Katz, and POC-CCA methods for diagnosing intestinal schistosomiasis in Candeal, a low intensity transmission area in northeastern Brazil. PLoS Negl. Trop. Dis. 2018, 12, e0006274. [Google Scholar] [CrossRef]
- Oliveira, W.J.; Magalhaes, F.D.C.; Elias, A.M.S.; de Castro, V.N.; Favero, V.; Lindholz, C.G.; Oliveira, A.A.; Barbosa, F.S.; Gil, F.; Gomes, M.A.; et al. Evaluation of diagnostic methods for the detection of intestinal schistosomiasis in endemic areas with low parasite loads: Saline gradient, Helmintex, Kato-Katz and rapid urine test. PLoS Negl. Trop. Dis. 2018, 12, e0006232. [Google Scholar] [CrossRef] [PubMed]
- Steinmann, P.; Keiser, J.; Bos, R.; Tanner, M.; Utzinger, J. Schistosomiasis and water resources development: Systematic review, meta-analysis, and estimates of people at risk. Lancet Infect. Dis. 2006, 6, 411–425. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Time | Phase | Specific Methods |
|---|---|---|
| 1981–1984 | Warren’s Study Control | Guifan Village: People with a positive stool examination result should receive drug chemotherapy. Sanlian Village: 1. People with positive result of stool examination should receive drug chemotherapy. 2. The areas where snail lived were sprayed with molluscicide every spring. |
| 1985–1991 | Local Government Control | 1. Chemotherapy for people and cattle was the basic measure. 2. Health education for people. 3. Molluscicide was directed at the susceptible areas. |
| 1992–2001 | World Bank Loan Project | Goal: Enhanced morbidity control through praziquantel to human and bovines. Details: 1. Chemotherapy was complemented by health education. 2. Snails were controlled by environmental management. 3. Molluscicide was a key way to sustain transmission control. |
| 2002–2004 | Extended Period of WBLP Control | 1. Achievements from WBLP were not reinforced. 2. The extent of chemotherapy shrinked and compliance of chemotherapy became worse. 3. Returning farmland to lake was advocated due to the molluscicide and previously reclaimed land from the lake. |
| 2005–2017 | Integrated Strategy Control | 2005: 1. Chemotherapy with praziquantel for people and cattle. 2. Snail control with molluscicides. 3. Health education programmes—residents should stay away from snail-infested areas and water Since 2006: 4. All cattle were replaced with mechanized equipment. 5. Other domestic animals were fenced in. 6. Piped water and lavatories were supplied to improve sanitation. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Zhou, Y.; Wang, T.; Zhang, S.; Chen, G.; Zhao, G.; He, N.; Zhang, Z.; Yang, D.; Yang, Y.; et al. Elimination of Schistosoma japonicum Transmission in China: A Case of Schistosomiasis Control in the Severe Epidemic Area of Anhui Province. Int. J. Environ. Res. Public Health 2019, 16, 138. https://doi.org/10.3390/ijerph16010138
Li L, Zhou Y, Wang T, Zhang S, Chen G, Zhao G, He N, Zhang Z, Yang D, Yang Y, et al. Elimination of Schistosoma japonicum Transmission in China: A Case of Schistosomiasis Control in the Severe Epidemic Area of Anhui Province. International Journal of Environmental Research and Public Health. 2019; 16(1):138. https://doi.org/10.3390/ijerph16010138
Chicago/Turabian StyleLi, Linhan, Yibiao Zhou, Tianping Wang, Shiqing Zhang, Gengxin Chen, Genming Zhao, Na He, Zhijie Zhang, Dongjian Yang, Ya Yang, and et al. 2019. "Elimination of Schistosoma japonicum Transmission in China: A Case of Schistosomiasis Control in the Severe Epidemic Area of Anhui Province" International Journal of Environmental Research and Public Health 16, no. 1: 138. https://doi.org/10.3390/ijerph16010138