Early Infant Feeding of Formula or Solid Foods and Risk of Childhood Overweight or Obesity in a Socioeconomically Disadvantaged Region of Australia: A Longitudinal Cohort Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Variables
2.3. Statistical Analysis
2.4. Demographics of Southwestern Sydney
3. Results
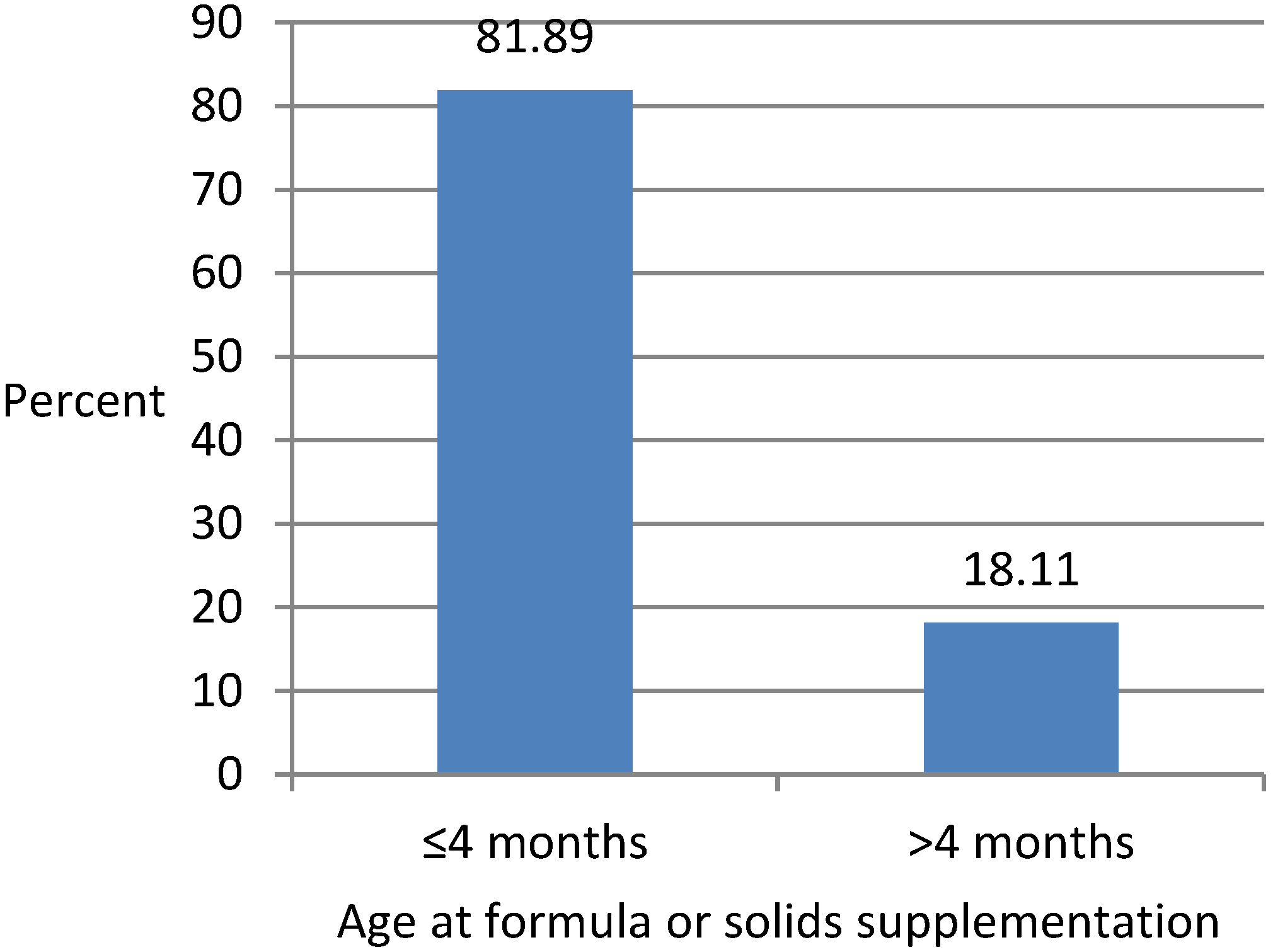
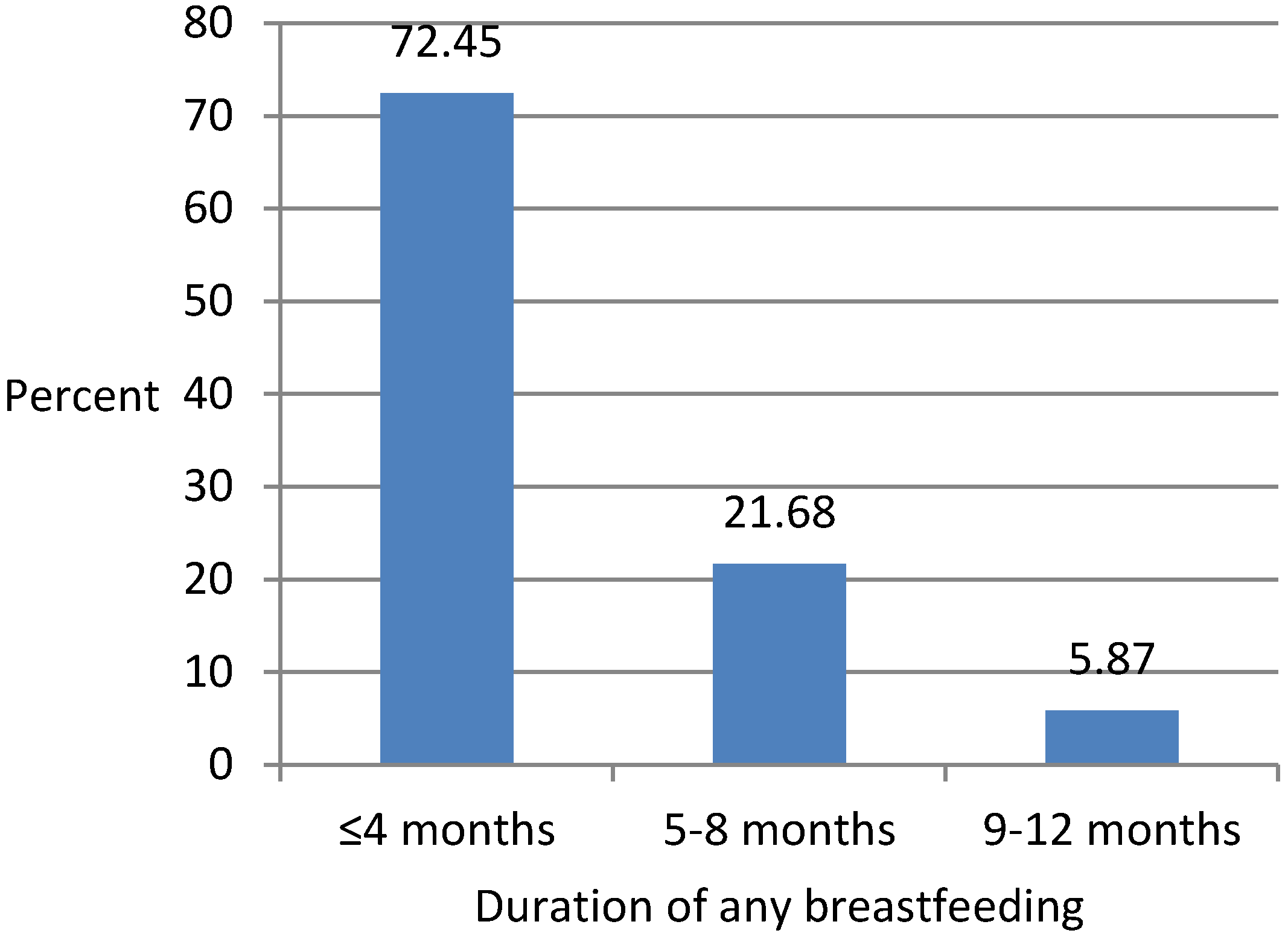
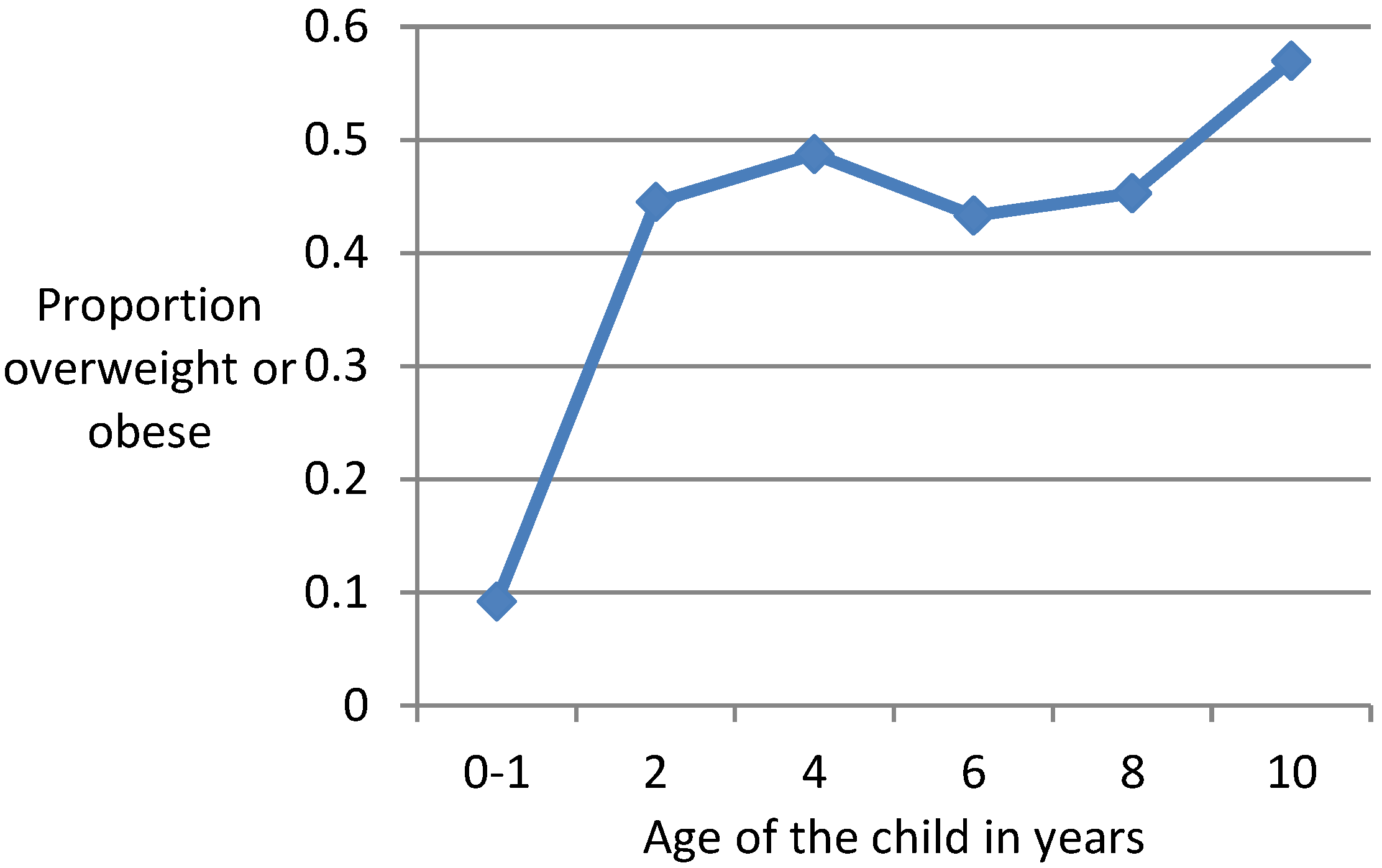
3.1. Descriptive Analysis
3.2. Multivariate Analysis
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Guo, S.S.; Huang, C.; Maynard, L.M.; Demerath, E.; Towne, B.; Chumlea, W.C.; Siervogel, R.M. Body mass index during childhood, adolescence and young adulthood in relation to adult overweight and adiposity: the Fels Longitudinal Study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1628–1635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schonfeld-Warden, N.; Warden, C.H. Pediatric obesity: an overview of etiology and treatment. Pediatr. Clin. N. Am. 1997, 44, 339–341. [Google Scholar] [CrossRef]
- Grummer-Strawn, L.M.; Mei, Z. Does breastfeeding protect against pediatric overweight? Analysis of longitudinal data from the Centers for Disease Control and Prevention Pediatric Nutrition Surveillance System. Pediatrics 2004, 113, 81–86. [Google Scholar] [CrossRef]
- Burke, V.; Beilin, L.J.; Simmer, K.; Oddy, W.H.; Blake, K.V.; Doherty, D.; Kendall, G.E.; Newnhan, J.P.; Landau, L.I.; Stanley, F.J. Breastfeeding and overweight: Longitudinal analysis in an Australian birth cohort. J. Pediatr. 2005, 147, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Harder, T.; Bergmann, R.L.; Kallischnigg, G.; Plagemann, A. Duration of breastfeeding and risk of overweight: a meta-analysis. Am. J. Epidemiol. 2005, 162, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H.; Smith, G.D.; Jacoby, P. A possible strategy for developing a model to account for attrition bias in a longitudinal cohort to investigate associations between exclusive breastfeeding and overweight and obesity at 20 years. Ann. Nutr. Metab. 2014, 65, 234–235. [Google Scholar] [CrossRef] [PubMed]
- Chivers, P.; Hands, B.; Parker, H.; Bulsara, M.; Beilin, L.J.; Kendall, G.E.; Oddy, W.H. Body mass index, adiposity rebound and early feeding in a longitudinal cohort. Int. J. Obes. 2010, 34, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Beyerlein, A.; von Kries, R. Breastfeeding and body composition in children: Will there ever be conclusive empirical evidence for a protective effect against overweight? Am. J. Clin. Nutr. 2011, 94, 1772–1775. [Google Scholar] [CrossRef] [PubMed]
- Arenz, S.; Rükerl, R.; Koletzko, B.; Von Kries, R. Breast-feeding and childhood obesity—A systematic review. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, J.; Reilly, J.J. Breastfeeding and lowering the risk of childhood obesity. Lancet 2002, 359, 2003–2004. [Google Scholar] [CrossRef]
- De Kroon, M.; Renders, C.; Buskermolen, M.; Van Wouwe, J.; van Buuren, S.; Hirasing, R. The Terneuzen Birth Cohort: longer exclusive breastfeeding duration is associated with leaner body mass and a healthier diet in young adulthood. BMC Pediatr. 2011, 11, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koletzko, B.; von Kries, R.; Monasterolo, R.C.; Subias, J.E.; Scaglioni, S.; Giovannini, M.; Beyer, J.; Demmelmair, H.; Anton, B.; Gruszfeld, D.; et al. Can infant feeding choices modulate later obesity risk? Am. J. Clin. Nutr. 2009, 89, 1502S–1508S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, J.L.; Michaelsen, K.F.; Rasmussen, K.M.; Sorensen, T. Maternal pre-pregnant body mass index, duration of breastfeeding, and timing of complementary food introduction are associated with infant weight gain. Am. J. Clin. Nutr. 2004, 80, 1579–1588. [Google Scholar] [CrossRef] [PubMed]
- Toschke, A.; Martin, R.; Kries, R.; Wells, J.; Smith, G.; Ness, A. Infant feeding method and obesity: body mass index and dual X-ray absorptiometry measurements at 9–10 years of age from the Avon Longitudinal Study of Parents and Children (ALSPAC). Am. J. Clin. Nutr. 2007, 85, 1578–1585. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, L.J.; Smeeth, L.; Hawkins, S.S.; Cole, T.J.; Dezateux, C. Effects of infant feeding practice on weight gain from birth to 3 years. Arch. Dis. Child. 2009, 94, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Huh, S.Y.; Rifas-Shiman, S.L.; Taveras, E.M.; Oken, E.; Gilman, M.W. Timing of solid food introduction and risk of obesity in preschool-aged children. Pediatrics 2011, 127, e544–e551. [Google Scholar] [CrossRef] [PubMed]
- Barrera, C.M.; Perrine, C.G.; Li, R.; Scanlon, K.S. Age at introduction to solid foods and child obesity at 6 years. Child Obes. 2016, 12, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Owen, C.G.; Martin, R.M.; Whincup, P.H.; Smith, G.D.; Cook, D.G. Effect of infant feeding on the risk of obesity across the life course: A quantitative review of published evidence. Pediatrics 2005, 115, 1367–1377. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council (NHMRC). Infant Feeding Guidelines: Summary; Australian Governement N56b; National Health and Medical Research Council: Canberra, Australia, 2013; p. 25.
- Wolfenden, L.; Hardy, L.L.; Wiggers, J.H.; Milat, A.J.; Bell, A.C.; Sutherland, R. Prevalence and socio-demographic associations of overweight and obesity among children attending child-care services in rural and regional Australia. Nutr. Diet. 2011, 68, 15–20. [Google Scholar] [CrossRef]
- Buckley, D. Southwest Sydney Has Most Obese Children: Australian Health Trackers 2017. Article published at The Telegraph. Available online: https://www.dailytelegraph.com.au/newslocal/fairfield-advance/southwest-sydney-has-most-obese-children-australian-health-trackers/news-story/30d0e9297758cf36a4806afa94a6ca22 (accessed on 9 May 2017).
- Wen, L.M.; Rissel, C.; Baur, L.A.; Hayes, A.J.; Xu, H.; Whelan, A.; Hua, M.; Shaw, M.; Phongsavan, P. A 3-Arm randomised controlled trial of Communicating Healthy Beginnings Advice by Telephone (CHAT) to mothers with infants to prevent childhood obesity. BMC Public Health 2017, 17, 79. [Google Scholar] [CrossRef] [PubMed]
- The Australian Institute of Family Studies. Longitudinal Study of Australian Children (LSAC) Rationale Documents: Growing Up in Australia Study; The Australian Institute of Family Studies: Melbourne, VIC, Australia, 2018.
- The Australian Institute of Family Studies. Longitudinal Study of Australian Children: Data user guide; The Australian Institute of Family Studies: Melbourne, VIC, Australia, 2004.
- Centers for Disease Control and Prevention. CDC Growth Charts. Available online: http.//www.cdc.gov/growthcharts/cdc_charts (accessed on 7 August 2018).
- Meng, X.L.; Rubin, D.B. Performing likelihood ratio tests with multiply-imputed data sets. Biometrika 1992, 79, 103–111. [Google Scholar] [CrossRef]
- Mistler, S.A. A SAS Macro for Computing Pooled Likelihood Ratio Tests with Multiply Imputed Data. In Proceedings of the SAS Global Forum Conference, San Francisco, CA, USA, 28 April–1 May 2013; SAS Institute Inc.: Cary, NC, USA, 2013. [Google Scholar]
- The Western Sydney Regional Organisation of Councils. 2016. Available online: http://profile.id.com.au/wsroc/about?WebID=200 (accessed on 1 June 2017).
- Western Sydney Local Health District. Available online: https://www.wslhd.health.nsw.gov.au/ (accessed on 1 June 2017).
- Oddy, W.H.; Mori, T.A.; Huang, R.-C.; Marsh, J.A.; Pennell, C.E.; Chivers, P.T.; Hands, B.P.; Jacoby, P.; Rzehak, P.; Koletzko, B.V.; et al. Early Infant Feeding and Adiposity Risk: From Infancy to Adulthood. Ann. Nutr. Metab. 2014, 64, 262–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walls, H.L.; Magliano, D.J.; Stevenson, C.; Mannan, H.; Shaw, J.; McNeil, J.J.; Peeters, A. Projected progression of the prevalence of obesity in Australia. Obesity 2012, 20, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Poole, C.; Lash, T.L. Causation and causal inference. In Modern Epidemiology, 3rd ed.; Rothman, K.J., Greenland, S., Lash, T.L., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; p. 758. [Google Scholar]
- Mayer-Davis, E.J.; Rifas-Shiman, S.L.; Zhou, L.; Hu, F.B.; Colditz, G.A.; Gillman, M.W. Breastfeeding and risk for childhood obesity. Diabetes Care 2006, 29, 2231–2237. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Yew, S.S.Y.; Devenish, G.; Ha, D.; Do, L.; Scott, J. Duration of Breastfeeding, but Not Timing of Solid Food, Reduces the Risk of Overweight and Obesity in Children Aged 24 to 36 Months: Findings from an Australian Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 599. [Google Scholar] [CrossRef] [PubMed]
- Natamba, B.K.; Sanchez, S.E.; Gelaye, B.; Williams, M.A. Concordance between self-reported pre-pregnancy body mass index (BMI) and BMI measured at the first prenatal study contact. BMC Pregnancy Childbirth 2016, 16, 187. [Google Scholar] [CrossRef] [PubMed]
- Krukowski, R.A.; West, D.S.; DiCarlo, M.; Shankar, K.; Cleves, M.A.; Saylors, M.E.; Andres, A. Are early first trimester weights valid proxies for preconception weight? BMC Pregnancy Childbirth 2016, 16, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, L.; Mallan, K.M.; Fildes, A.; Wilson, J. The timing of solid introduction in an ‘obesogenic’ environment: A narrative review of the evidence and methodological issues. Aust. N. Z. J. Public Health 2015, 39, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Konold, T.R. Statistical Significance Versus Effect Size. In International Encyclopedia of Education, 3rd ed.; Peterson, P., Baker, E., McGaw, B., Eds.; Elsevier Science: Oxford, UK, 2010; pp. 444–450. [Google Scholar]
- Trost, S.G.; Kerr, L.M.; Ward, D.S.; Pate, R.R. Physical activity and determinants of physical activity in obese and non-obese children. Int. J. Obes. Relat. Metab. Disord. 2011, 25, 822–829. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Covariate | Odds Ratio | 95% CI | t Ratio |
|---|---|---|---|
| Model 1 Age at starting formula or solids ≤4 months vs. >4 months | 2.3262 | 1.8025–2.4132 | 2.3026 a |
| Model 2 Age at starting formula or solids ≤4 months vs. >4 months | 1.9543 | 1.1010–3.4687 | 2.27 a |
| Model 3 Age at starting formula or solids * age at breastfeeding cessation ≤4 months * ≤4months vs. >4months * >4 months | 2.0856 | 1.1225–4.8205 | 1.9845 a |
| Model 4 Time*Age at starting formula or solids | |||
| Age 2/3 * ≤4 months | 0.3569 | 0.0668–1.9058 | −1.21 |
| Age 4/5 * ≤4 months | 0.8437 | 0.1547–4.6014 | −0.20 |
| Age 6/7 * ≤4 months | 0.9050 | 0.1564–5.2385 | −0.11 |
| Age 8/9 * ≤4 months | 0.4573 | 0.0810–2.5828 | −0.89 |
| Age 10/11 * ≤4 months vs. Age 0/1 * >4 months | 0.6093 | 0.1001–3.7088 | −0.54 |
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannan, H. Early Infant Feeding of Formula or Solid Foods and Risk of Childhood Overweight or Obesity in a Socioeconomically Disadvantaged Region of Australia: A Longitudinal Cohort Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1685. https://doi.org/10.3390/ijerph15081685
Mannan H. Early Infant Feeding of Formula or Solid Foods and Risk of Childhood Overweight or Obesity in a Socioeconomically Disadvantaged Region of Australia: A Longitudinal Cohort Analysis. International Journal of Environmental Research and Public Health. 2018; 15(8):1685. https://doi.org/10.3390/ijerph15081685
Chicago/Turabian StyleMannan, Haider. 2018. "Early Infant Feeding of Formula or Solid Foods and Risk of Childhood Overweight or Obesity in a Socioeconomically Disadvantaged Region of Australia: A Longitudinal Cohort Analysis" International Journal of Environmental Research and Public Health 15, no. 8: 1685. https://doi.org/10.3390/ijerph15081685