Gender Differences in Psychological Well-Being and Health Problems among European Health Professionals: Analysis of Psychological Basic Needs and Job Satisfaction



Abstract
:1. Introduction
2. Methods
2.1. Study Sample
2.2. Measurement
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics, Reliability and Correlations among the Study Variables
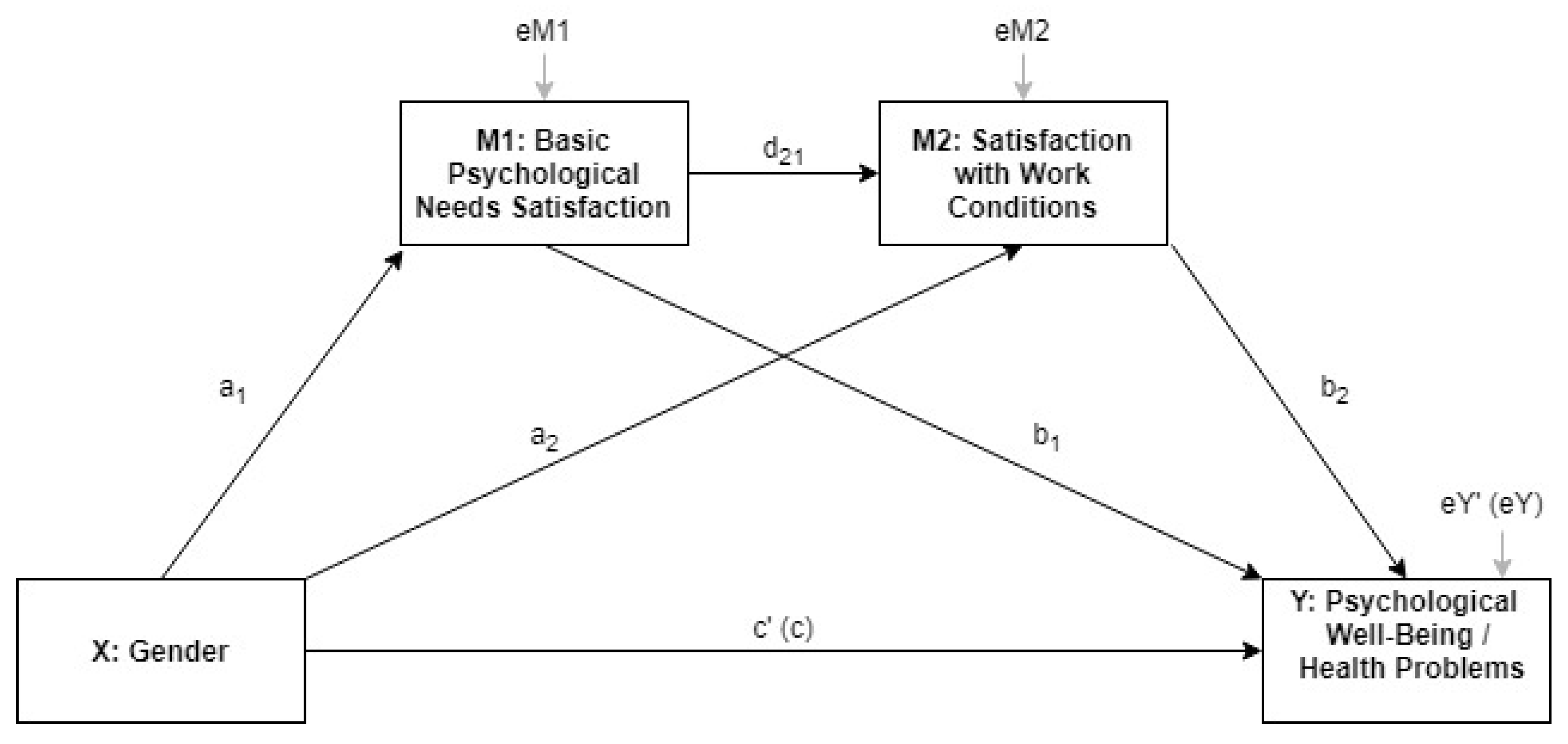
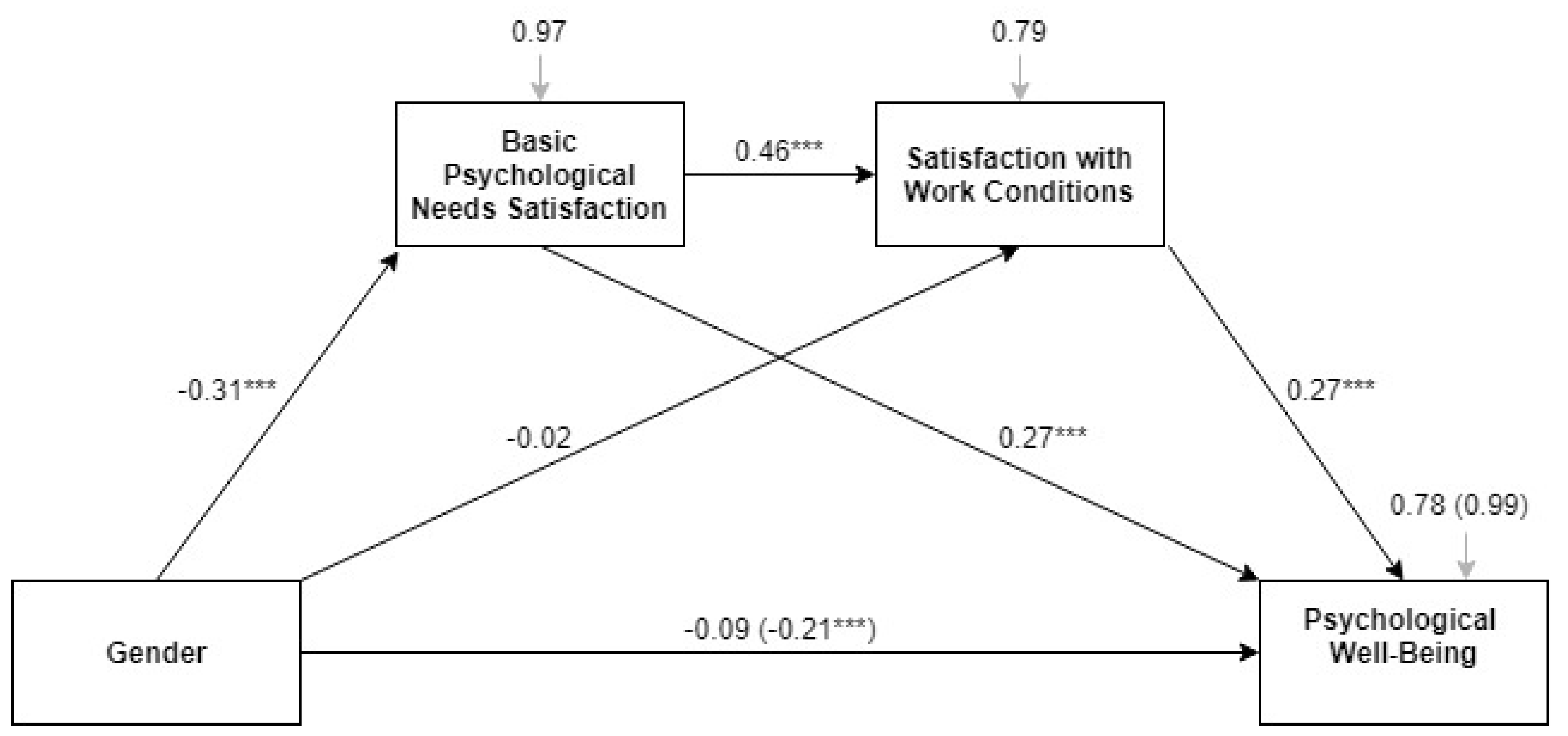
3.2. Multiple Partial Mediation of Basic Needs Satisfaction and Satisfaction with Job Conditions in the Gender Effect on Psychological Well-Being
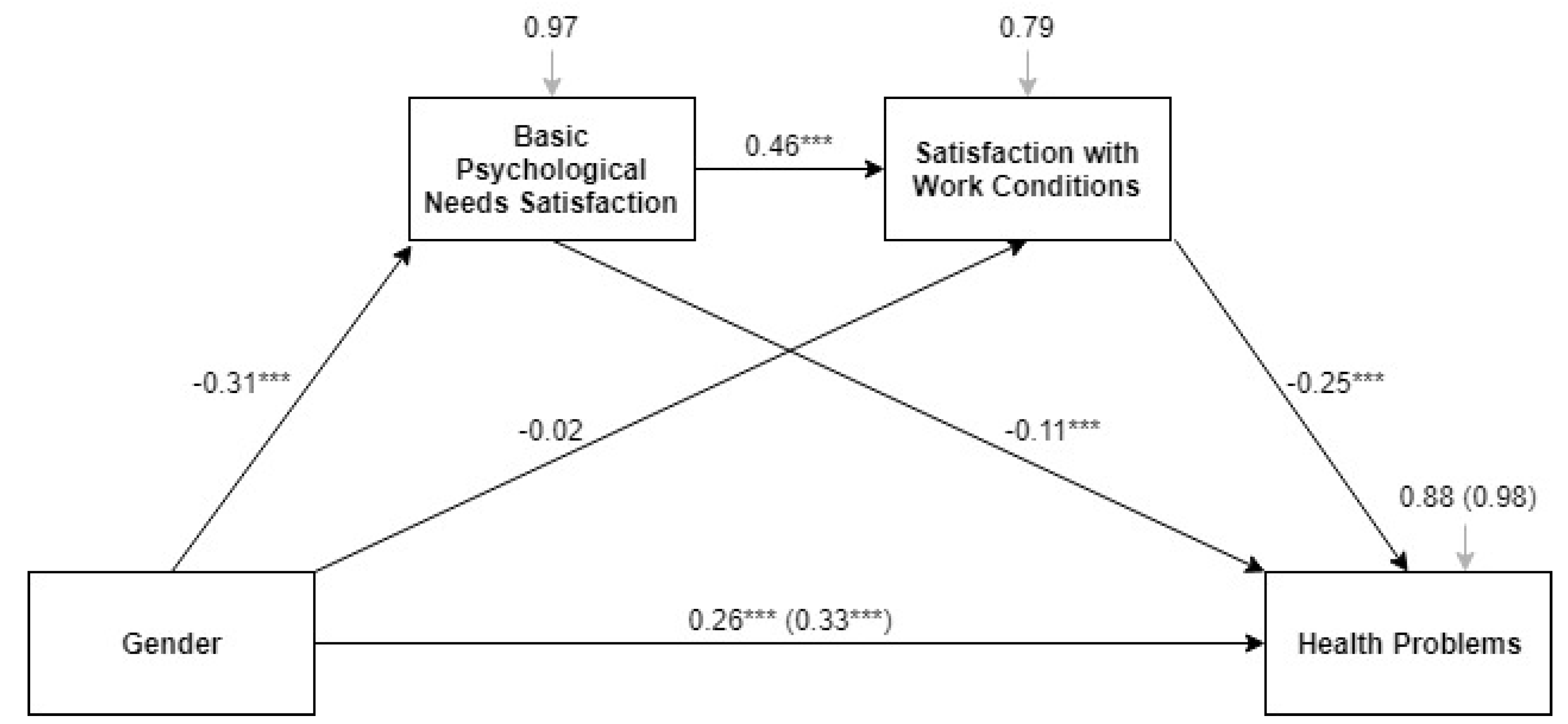
3.3. Multiple Partial Mediation of Basic Needs Satisfaction and Satisfaction with Job Conditions in the Gender Effect on Health Problems
4. Discussion
5. Conclusions
- Female health professionals in Europe reported lower psychological well-being, lower levels of basic psychological need satisfaction, and more health problems.
- Basic psychological need satisfaction is an underlying mechanism for explaining gender differences in psychological well-being.
- Basic psychological need satisfaction partly explains gender differences in health problems.
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Countries and Welfare State Regime | Code | n = 1774 | % Women | Needs Satisfaction | Satisfaction with Work Conditions | Psychological Well-Being | Health Problems | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | ||||
| Conservative | 538 | 82.7 | 3.77 | 0.54 | 3.13 | 0.68 | 4.46 | 1.00 | 2.45 | 2.11 | |
| Austria | AT | 46 | 84.8 | 3.76 | 0.48 | 3.26 | 0.77 | 4.42 | 1.06 | 2.28 | 2.27 |
| Belgium | BE | 138 | 77.5 | 3.75 | 0.55 | 3.07 | 0.71 | 4.33 | 1.18 | 2.83 | 2.20 |
| France | FR | 73 | 87.7 | 3.74 | 0.43 | 3.00 | 0.61 | 4.27 | 0.87 | 3.26 | 2.17 |
| Germany | DE | 111 | 87.4 | 3.58 | 0.60 | 3.14 | 0.68 | 4.55 | 0.91 | 1.89 | 1.85 |
| Luxembourg | LU | 43 | 74.4 | 3.88 | 0.65 | 3.02 | 0.64 | 4.29 | 1.04 | 2.49 | 2.24 |
| Netherlands | NL | 72 | 84.7 | 3.98 | 0.42 | 3.18 | 0.66 | 4.78 | 0.74 | 2.40 | 1.95 |
| Switzerland | CH | 55 | 81.8 | 3.86 | 0.51 | 3.38 | 0.62 | 4.67 | 0.92 | 1.74 | 1.74 |
| Post-Communist | 511 | 85.7 | 3.90 | 0.56 | 3.06 | 0.67 | 4.43 | 0.95 | 2.53 | 2.06 | |
| Bulgaria | BG | 23 | 73.9 | 4.10 | 0.45 | 3.26 | 0.69 | 4.30 | 0.97 | 2.57 | 1.38 |
| Croatia | HR | 37 | 81.1 | 3.72 | 0.54 | 2.97 | 0.73 | 4.23 | 0.98 | 2.76 | 2.33 |
| Czech Rep. | CZ | 39 | 84.6 | 4.09 | 0.54 | 3.44 | 0.55 | 4.73 | 0.79 | 1.62 | 1.64 |
| Estonia | EE | 34 | 97.1 | 4.01 | 0.51 | 3.18 | 0.47 | 4.48 | 1.06 | 3.50 | 1.78 |
| Hungary | HU | 43 | 83.7 | 3.92 | 0.78 | 3.00 | 0.85 | 4.75 | 0.81 | 1.16 | 1.44 |
| Latvia | LV | 24 | 95.8 | 3.84 | 0.63 | 3.13 | 0.45 | 4.29 | 0.78 | 2.96 | 1.66 |
| Lithuania | LT | 28 | 89.3 | 3.84 | 0.61 | 3.07 | 0.72 | 4.11 | 0.65 | 3.43 | 2.32 |
| Poland | PL | 32 | 90.6 | 3.84 | 0.54 | 3.06 | 0.62 | 4.46 | 0.85 | 3.45 | 2.31 |
| Romania | RO | 20 | 95.0 | 3.92 | 0.64 | 3.10 | 0.45 | 4.27 | 0.88 | 3.47 | 2.12 |
| Slovakia | SK | 32 | 90.6 | 3.64 | 0.47 | 3.06 | 0.56 | 4.31 | 1.24 | 2.19 | 2.10 |
| Slovenia | SI | 59 | 84.7 | 3.94 | 0.47 | 2.86 | 0.68 | 4.50 | 1.00 | 2.48 | 2.04 |
| Montenegro | ME | 33 | 84.8 | 3.81 | 0.55 | 3.13 | 0.66 | 4.44 | 0.88 | 2.21 | 2.03 |
| FYROM | MK | 39 | 76.9 | 4.26 | 0.49 | 3.00 | 0.61 | 4.76 | 1.02 | 2.50 | 1.94 |
| Serbia | RS | 34 | 79.4 | 3.75 | 0.53 | 2.81 | 0.82 | 4.04 | 1.07 | 3.23 | 2.15 |
| Albania | AL | 34 | 85.3 | 3.68 | 0.35 | 3.03 | 0.67 | 4.34 | 0.75 | 1.59 | 1.72 |
| Mediterranean | 323 | 74.0 | 3.82 | 0.57 | 3.16 | 0.67 | 4.57 | 0.98 | 2.58 | 2.28 | |
| Cyprus | CY | 33 | 66.7 | 3.57 | 0.41 | 2.97 | 0.68 | 4.28 | 1.09 | 3.15 | 2.02 |
| Greece | EL | 20 | 70.0 | 3.71 | 0.32 | 3.50 | 0.69 | 4.79 | 0.60 | 2.05 | 2.14 |
| Italy | IT | 57 | 75.0 | 3.66 | 0.51 | 3.14 | 0.64 | 4.30 | 0.73 | 1.93 | 2.12 |
| Malta | MT | 53 | 66.0 | 4.00 | 0.50 | 3.11 | 0.70 | 4.28 | 0.96 | 3.48 | 1.77 |
| Portugal | PT | 16 | 81.3 | 4.05 | 0.42 | 3.19 | 0.54 | 4.99 | 0.72 | 0.81 | 1.56 |
| Spain | ES | 117 | 82.1 | 3.84 | 0.64 | 3.16 | 0.69 | 4.77 | 1.10 | 2.73 | 2.53 |
| Turkey | TR | 28 | 60.7 | 3.90 | 0.69 | 3.29 | 0.60 | 4.85 | 0.84 | 2.27 | 2.24 |
| Social-Democratic | 279 | 86.7 | 3.78 | 0.47 | 3.17 | 0.73 | 4.45 | 0.94 | 2.43 | 1.83 | |
| Finland | FI | 39 | 89.7 | 3.88 | 0.46 | 3.18 | 0.76 | 4.53 | 0.89 | 2.85 | 2.23 |
| Denmark | DK | 71 | 87.3 | 3.86 | 0.45 | 3.35 | 0.70 | 4.54 | 0.76 | 2.40 | 1.64 |
| Sweden | SE | 87 | 79.3 | 3.67 | 0.50 | 3.02 | 0.75 | 4.39 | 1.00 | 2.17 | 1.79 |
| Norway | N | 82 | 92.7 | 3.77 | 0.46 | 3.16 | 0.69 | 4.39 | 1.05 | 2.51 | 1.81 |
| Liberal | 122 | 83.6 | 3.83 | 0.53 | 3.10 | 0.73 | 4.25 | 1.03 | 2.28 | 2.10 | |
| Ireland | IE | 54 | 87.0 | 3.84 | 0.53 | 3.11 | 0.66 | 4.41 | 0.86 | 1.98 | 1.81 |
| UK | UK | 68 | 80.9 | 3.82 | 0.54 | 3.09 | 0.79 | 4.12 | 1.14 | 2.51 | 2.29 |
| Countries and Welfare State Regime | Code | M1: Need Satisfaction | M2: Satisfaction with Work Conditions | Total Effect Model: Wellbeing | Total Effect Model: Health Problems | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R2 | F | a1 | R2 | F | a2 | d21 | R2 | F | c | R2 | F | c | ||
| Conservative | 0.05 | 32.84 *** | −0.58 *** | 0.25 | 61.28 *** | 0.18 | 0.50 *** | 0.01 | 9.13 ** | −0.31 ** | 0.03 | 17.49 *** | 0.43 *** | |
| Austria | AT | 0.25 | 19.94 *** | −0.31 *** | 0.18 | 2.82 | 0.46 | 0.57 * | 0.03 | 2.21 | −0.53 | 0.05 | 5.03 * | 0.64 * |
| Belgium | BE | 0.07 | 12.65 *** | −0.65 *** | 0.35 | 34.07 *** | 0.29 | 0.63 *** | 0.02 | 3.22 | −0.36 | 0.04 | 5.72 * | 0.48 * |
| France | FR | 0.04 | 4.41 * | −0.51 * | 0.23 | 10.70 *** | −0.53 * | 0.43 ** | 0.03 | 2.37 | −0.49 | 0.06 | 4.89 * | 0.75 * |
| Germany | DE | 0.05 | 9.70 ** | −0.74 ** | 0.31 | 13.95 *** | 0.11 | 0.48 *** | 0.03 | 9.81 ** | −0.48 ** | 0.05 | 9.56 ** | 0.57 ** |
| Luxembourg | LU | 0.01 | 1.01 | −0.32 | 0.16 | 5.05 * | 0.15 | 0.32 ** | 0.01 | 0.25 | −0.17 | 0.01 | 0.50 | 0.26 |
| Netherlands | NL | 0.01 | 0.04 | −0.05 | 0.27 | 9.24 *** | 0.49 | 0.61 *** | 0.02 | 0.81 | −0.27 | 0.01 | 0.34 | 0.18 |
| Switzerland | CH | 0.03 | 1.05 | −0.41 | 0.24 | 10.73 *** | 0.16 | 0.46 *** | 0.01 | 0.01 | 0.01 | 0.02 | 2.72 | 0.32 |
| Post-Communist | 0.01 | 1.46 | −0.17 | 0.10 | 27.99 *** | −0.07 | 0.31 *** | 0.01 | 2.56 | −0.17 | 0.02 | 15.14 *** | 0.44 *** | |
| Bulgaria | BG | 0.18 | 6.10 * | −0.76 * | 0.22 | 7.94 ** | −0.47 | 0.43 * | 0.02 | 0.56 | −0.28 | 0.01 | 0.03 | 0.04 |
| Croatia | HR | 0.06 | 3.21 | −0.62 | 0.12 | 2.78 | 0.67 | 0.33 * | 0.01 | 0.01 | 0.04 | 0.01 | 0.05 | 0.11 |
| Czech Rep. | CZ | 0.04 | 3.15 | −0.55 | 0.17 | 5.01 * | −0.23 | 0.31 ** | 0.01 | 0.83 | 0.24 | 0.01 | 0.33 | 0.15 |
| Estonia | EE | 0.01 | 1.71 | 0.20 | 0.20 | 67.50 *** | −0.25 *** | 0.26 * | 0.01 | 8.42 ** | −0.55 ** | 0.01 | 2.77 | −0.25 |
| Hungary | HU | 0.06 | 2.24 | 0.82 | 0.14 | 4.31 * | 0.50 | 0.30 * | 0.05 | 2.47 | 0.50 | 0.07 | 12.08 ** | 0.50 ** |
| Latvia | LV | 0.27 | 205.64 *** | 0.76 *** | 0.06 | 1.73 | −0.25 | 0.16 | 0.06 | 34.36 *** | 0.95 *** | 0.07 | 42.14 *** | −0.02 *** |
| Lithuania | LT | 0.02 | 0.41 | 0.52 | 0.36 | 13.93 *** | −0.71 *** | 0.39 ** | 0.06 | 3.03 | −0.48 | 0.07 | 3.34 | 0.95 |
| Poland | PL | 0.25 | 17.03 | −0.66 *** | 0.26 | 6.51 ** | 0.43 | 0.52 ** | 0.03 | 1.31 | −0.53 | 0.09 | 7.59 ** | 0.10 ** |
| Romania | RO | 0.02 | 6.45 * | −0.77 * | 0.23 | 87.50 *** | −0.35 *** | 0.04 | 0.01 | 0.38 | −0.12 | 0.03 | 10.26 ** | 0.72 ** |
| Slovakia | SK | 0.07 | 5.86 * | −0.74 * | 0.26 | 5.74 ** | −0.07 | 0.49 ** | 0.01 | 0.01 | −0.04 | 0.04 | 12.06 ** | 0.65 ** |
| Slovenia | SI | 0.02 | 1.25 | −0.34 | 0.28 | 9.44 *** | −0.03 | 0.61 *** | 0.01 | 0.64 | −0.28 | 0.06 | 7.72 ** | 0.68 ** |
| Montenegro | ME | 0.03 | 0.97 | 0.48 | 0.05 | 1.34 | −0.56 | 0.13 | 0.03 | 2.74 | −0.43 | 0.15 | 17.08 *** | 0.02 *** |
| FYROM | MK | 0.01 | 0.14 | −0.14 | 0.02 | 0.27 | 0.02 | 0.15 | 0.01 | 0.82 | −0.27 | 0.05 | 1.87 | 0.48 |
| Serbia | RS | 0.10 | 3.93 | 0.73 | 0.17 | 5.52 ** | 0.46 | 0.41 * | 0.02 | 0.85 | −0.39 | 0.01 | 0.06 | −0.12 |
| Albania | AL | 0.08 | 3.18 | −0.52 | 0.06 | 1.76 | −0.56 | 0.14 | 0.06 | 5.74* | −0.54* | 0.01 | 0.06 | 0.08 |
| Mediterranean | 0.01 | 2.09 | −0.18 | 0.27 | 56.81 *** | 0.01 | 0.49 *** | 0.01 | 0.11 | −0.04 | 0.01 | 3.02 | 0.23 | |
| Cyprus | CY | 0.01 | 0.15 | 0.14 | 0.19 | 6.80 ** | 0.06 | 0.50 *** | 0.01 | 0.01 | −0.01 | 0.01 | 0.05 | −0.09 |
| Greece | EL | 0.01 | 0.24 | −0.17 | 0.22 | 2.95 | −0.24 | 0.65 * | 0.02 | 0.33 | 0.18 | 0.04 | 0.59 | −0.42 |
| Italy | IT | 0.03 | 2.01 | −0.38 | 0.24 | 7.41 ** | 0.28 | 0.48 *** | 0.05 | 3.99 | −0.38 | 0.03 | 2.52 | 0.39 |
| Malta | MT | 0.04 | 2.47 | −0.40 | 0.24 | 7.10 ** | 0.35 | 0.55 *** | 0.01 | 0.01 | 0.03 | 0.14 | 9.08 ** | 0.66 ** |
| Portugal | PT | 0.01 | 0.06 | 0.08 | 0.02 | 0.18 | −0.26 | 0.01 | 0.22 | 9.63 ** | −0.86 ** | 0.01 | 0.07 | 0.09 |
| Spain | ES | 0.03 | 5.25 * | −0.48 * | 0.46 | 61.38 *** | −0.21 | 0.59 *** | 0.01 | 0.38 | −0.19 | 0.02 | 10.78 | 0.42 |
| Turkey | TR | 0.11 | 3.57 | 0.85 | 0.18 | 2.22 | 0.01 | 0.29 | 0.06 | 1.74 | 0.42 | 0.01 | 0.01 | −0.03 |
| Social-Democratic | 0.01 | 4.01 * | −0.29 * | 0.38 | 90.72 *** | −0.24 | 0.71 *** | 0.01 | 3.61 | −0.30 | 0.01 | 1.50 | 0.19 | |
| Denmark | DK | 0.01 | 0.56 | −0.20 | 0.36 | 20.13 *** | −0.20 | 0.69 *** | 0.02 | 1.55 | −0.30 | 0.01 | 0.01 | −0.01 |
| Finland | FI | 0.01 | 0.27 | −0.28 | 0.33 | 19.32 *** | −0.33 | 0.70 *** | 0.01 | 0.10 | −0.19 | 0.11 | 3.31 | −0.15 |
| Sweden | SE | 0.07 | 8.56 ** | −0.62 ** | 0.30 | 22.68 *** | −0.31 | 0.58 *** | 0.02 | 1.53 | −0.31 | 0.04 | 5.42 * | 0.41 * |
| Norway | N | 0.01 | 0.19 | 0.13 | 0.51 | 30.28 *** | −0.38 | 0.84 *** | 0.01 | 1.47 | −0.45 | 0.03 | 6.55 * | 0.61 * |
| Liberal | 0.01 | 0.27 | −0.12 | 0.28 | 24.47 *** | −0.11 | 0.58 *** | 0.01 | 0.76 | −0.20 | 0.01 | 1.37 | 0.25 | |
| Ireland | IE | 0.04 | 2.19 | 0.54 | 0.19 | 7.01 ** | −0.05 | 0.44 *** | 0.02 | 0.63 | 0.32 | 0.03 | 1.14 | −0.40 |
| UK | UK | 0.05 | 4.07 * | −0.53 * | 0.35 | 20.10 *** | −0.03 | 0.69 *** | 0.04 | 3.95 | −0.55 | 0.06 | 8.17 ** | 0.67 ** |
References
- Gomes, A.R.; Teixeira, P.M. Stress, Cognitive Appraisal and Psychological Health: Testing Instruments for Health Professionals. Stress Heal. 2016, 32, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Amoafo, E.; Hanbali, N.; Patel, A.; Singh, P. What are the significant factors associated with burnout in doctors? Occup. Med. (Lond.) 2015, 65, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Iliceto, P.; Pompili, M.; Spencer-Thomas, S.; Ferracuti, S.; Erbuto, D.; Lester, D.; Candilera, G.; Girardi, P. Occupational stress and psychopathology in health professionals: An explorative study with the Multiple Indicators Multiple Causes (MIMIC) model approach. Stress 2013, 16, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Fridner, A.; Belkic, K.; Marini, M.; Minucci, D.; Pavan, L.; Schenck-Gustafsson, K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): Cross-sectional associations with work stressors. Gend. Med. 2009, 6, 314–328. [Google Scholar] [CrossRef] [PubMed]
- Fridner, A.; Belkić, K.; Minucci, D.; Pavan, L.; Marini, M.; Pingel, B.; Putoto, G.; Simonato, P.; Løvseth, L.T.; Schenck-Gustafsson, K. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: The Health and Organization among University Hospital Physicians in Europe (HOUPE) study. Gend. Med. 2011, 8, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Rössler, W. Stress, burnout, and job dissatisfaction in mental health workers. Eur. Arch. Psychiatry Clin. Neurosci. 2012, 262, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Deriba, B.K.; Sinke, S.O.; Ereso, B.M.; Badacho, A.S. Health professionals’ job satisfaction and associated factors at public health centers in West Ethiopia. Hum. Resour. Health 2017, 15, 36. [Google Scholar] [CrossRef] [PubMed]
- Tarcan, G.Y.; Tarcan, M.; Top, M. An analysis of relationship between burnout and job satisfaction among emergency health professionals. Total Qual. Manag. Bus. Excell. 2017, 28, 1339–1356. [Google Scholar] [CrossRef]
- Noblet, A.J.; Allisey, A.F.; Nielsen, I.L.; Cotton, S.; Lamontagne, A.D.; Page, K.M. The work-based predictors of job engagement and job satisfaction experienced by community health professionals. Health Care Manag. Rev. 2017, 42, 237–246. [Google Scholar] [CrossRef] [PubMed]
- El-Jardali, F.; Makhoul, J.; Jamal, D.; Ranson, M.K.; Kronfol, N.M.; Tchaghchagian, V. Eliciting policymakers’ and stakeholders’ opinions to help shape health system research priorities in the Middle East and North Africa region. Health Policy Plan. 2010, 25, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. 2008, 49, 182–185. [Google Scholar] [CrossRef]
- Uysal, A.; Lin, H.L.; Knee, C.R.; Bush, A.L. The association between self-concealment from one’s partner and relationship well-being. Personal. Soc. Psychol. Bull. 2012, 38, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Slemp, G.R.; Vella-Brodrick, D.A. Optimising Employee Mental Health: The Relationship Between Intrinsic Need Satisfaction, Job Crafting, and Employee Well-Being. J. Happiness Stud. 2014, 15, 957–977. [Google Scholar] [CrossRef]
- Reis, H.T.; Sheldon, K.M.; Gable, S.L.; Roscoe, J.; Ryan, R.M. Daily well-being: The role of autonomy, competence, and relatedness. Personal. Soc. Psychol. Bull. 2000, 26, 419–435. [Google Scholar] [CrossRef]
- Baard, P.P.; Deci, E.L.; Ryan, R.M. Intrinsic need satisfaction: A motivational basis of performance and well-being in two work settings. J. Appl. Soc. Psychol. 2004, 34, 2045–2068. [Google Scholar] [CrossRef]
- Van den Broeck, A.; Vansteenkiste, M.; De Witte, H.; Lens, W. Explaining the relationships between job characteristics, burnout, and engagement: The role of basic psychological need satisfaction. Work Stress 2008, 22, 277–294. [Google Scholar] [CrossRef] [Green Version]
- Niemiec, C.P.; Ryan, R.M.; Deci, E.L. The path taken: Consequences of attaining intrinsic and extrinsic aspirations in post-college life. J. Res. Pers. 2009, 43, 291–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabene, S.M.; Orchard, C.; Howard, J.M.; Soriano, M.A.; Leduc, R. The importance of human resources management in health care: A global context. Hum. Resour. Health 2006, 4, 20. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, K.M.; Turban, D.B.; Brown, K.G.; Barrick, M.R.; Judge, T.A. Applying self-determination theory to organizational research. Res. Pers. Hum. Resour. Manag. 2003, 22, 357–393. [Google Scholar]
- Gagné, M. The Oxford Handbook of Work Engagement, Motivation, and Self-Determination Theory; Oxford University Press: New York, NY, USA, 2014; ISBN 9780199794911. [Google Scholar]
- Gagné, M.; Deci, E.L. Self-determination theory and work motivation. J. Organ. Behav. 2005, 26, 331–362. [Google Scholar] [CrossRef] [Green Version]
- Deci, E.L.; Ryan, R.M.; Gagné, M.; Leone, D.R.; Usunov, J.; Kornazheva, B.P. Need satisfaction, motivation, and well-being in the work organizations of a former eastern bloc country: A cross-cultural study of self-determination. Personal. Soc. Psychol. Bull. 2001, 27, 930–942. [Google Scholar] [CrossRef]
- Di Domenico, S.I.; Fournier, M.A. Socioeconomic Status, Income Inequality, and Health Complaints: A Basic Psychological Needs Perspective. Soc. Indic. Res. 2014, 119, 1679–1697. [Google Scholar] [CrossRef]
- Tay, L.; Diener, E. Needs and subjective well-being around the world. J. Pers. Soc. Psychol. 2011, 101, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. On Happiness and Human Potentials: A Review of Research on Hedonic and Eudaimonic Well-Being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. Handbook of Self-Determination Research; University of Rochester Press: New York, NY, USA, 2002; ISBN 1580461565. [Google Scholar]
- Baumeister, R.F.; Leary, M.R. The Need to Belong: Desire for Interpersonal Attachments as a Fundamental Human Motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef] [PubMed]
- Lynch, M.F.; Plant, R.W.; Ryan, R.M. Psychological Needs and Threat to Safety: Implications for Staff and Patients in a Psychiatric Hospital for Youth. Prof. Psychol. Res. Pract. 2005, 36, 415–425. [Google Scholar] [CrossRef]
- Javadi, D.; Vega, J.; Etienne, C.; Wandira, S.; Doyle, Y.; Nishtar, S. Women Who Lead: Successes and Challenges of Five Health Leaders. Heal. Syst. Reform 2016, 2, 229–240. [Google Scholar] [CrossRef]
- Reamy, J.; Pong, R. Physician workforce composition by gender: the implications for managing physician supply. In Proceedings of the 4th FICOSSER General Conference, Cuernavaca, Mexico, 28–30 July 1998; pp. 28–30. [Google Scholar]
- European Foundation for the Improvement of Living and Working Conditions—Eurofound. Sixth European Working Conditions Survey: 2015. Available online: https://www.eurofound.europa.eu/surveys/european-working-conditions-surveys/sixth-european-working-conditions-survey-2015 (accessed on 11 July 2018).
- Gomez-Baya, D.; Lucia-Casademunt, A.M. A self-determination theory approach to health and well-being in the workplace: Results from the sixth European working conditions survey in Spain. J. Appl. Soc. Psychol. 2018, 48, 269–283. [Google Scholar] [CrossRef]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis; Guilford Press: New York, NY, USA, 2017; ISBN 9781609182304. [Google Scholar]
- Preacher, K.J.; Kelley, K. Effect size measures for mediation models: Quantitative strategies for communicating indirect effects. Psychol. Methods 2011, 16, 93–115. [Google Scholar] [CrossRef] [PubMed]
- Eikemo, T.A.; Bambra, C.; Joyce, K.; Dahl, E. Welfare state regimes and income-related health inequalities: A comparison of 23 European countries. Eur. J. Public Health 2008, 18, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Galvez, J. Discovering complex interrelationships between socioeconomic status and health in Europe: A case study applying Bayesian Networks. Soc. Sci. Res. 2016, 56, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, M.S. Using a single-item approach to measure facet job satisfaction. J. Occup. Organ. Psychol. 2002, 75, 77–86. [Google Scholar] [CrossRef]
- Wanous, J.P.; Reichers, A.E.; Hudy, M.J. Overall job satisfaction: How good are single-item measures? J. Appl. Psychol. 1997, 82, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- European Foundation for the Improvement of Living and Working Conditions—Eurofound. Legal and Data Protection Notices. Eurofound. Available online: https://www.eurofound.europa.eu/about-eurofound/who-we-are/legal-and-data-protection-notices (accessed on 11 July 2018).
- Hem, E.; Haldorsen, T.; Aasland, O.G.; Tyssen, R.; Vaglum, P.; Ekeberg, Ø. Suicide rates according to education with a particular focus on physicians in Norway 1960–2000. Psychol. Med. 2005, 35, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.S.; Patten, S. Well-being in residency training: A survey examining resident physician satisfaction both within and outside of residency training and mental health in Alberta. BMC Med. Educ. 2005, 5, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puriene, A.; Aleksejuniene, J.; Petrauskiene, J.; Balciuniene, I.; Janulyte, V. Self-reported occupational health issues among Lithuanian dentists. Ind. Health 2008, 46, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Fritschi, L.; Morrison, D.; Shirangi, A.; Day, L. Psychological well-being of Australian veterinarians. Aust. Vet. J. 2009, 87, 76–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azam, K.; Khan, A.; Alam, M.T. Causes and adverse impact of physician burnout: A systematic review. J. Coll. Physicians Surg. Pak. 2017, 27, 495–501. [Google Scholar] [PubMed]
- Dewa, C.S.; Loong, D.; Bonato, S.; Thanh, N.X.; Jacobs, P. How does burnout affect physician productivity? A systematic literature review. BMC Health Serv. Res. 2014, 14, 325. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Erwin, P.J.; Shanafelt, T.D. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet 2016, 388, 2272–2281. [Google Scholar] [CrossRef]
- Edwards, D.; Burnard, P.; Coyle, D.; Fothergill, A.; Hannigan, B. Stress and burnout in community mental health nursing: A review of the literature. J. Psychiatr. Ment. Health Nurs. 2000, 7, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.; Burnard, P. A systematic review of stress and stress management interventions for mental health nurses. J. Adv. Nurs. 2003, 42, 169–200. [Google Scholar] [CrossRef] [PubMed]
- Fiabane, E.; Giorgi, I.; Sguazzin, C.; Argentero, P. Work engagement and occupational stress in nurses and other healthcare workers: The role of organisational and personal factors. J. Clin. Nurs. 2013, 22, 2614–2624. [Google Scholar] [CrossRef] [PubMed]
- Sveinsdóttir, H.; Biering, P.; Ramel, A. Occupational stress, job satisfaction, and working environment among Icelandic nurses: A cross-sectional questionnaire survey. Int. J. Nurs. Stud. 2006, 43, 875–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, E.; Mageau, G.A. The importance of perceived autonomy support for the psychological health and work satisfaction of health professionals: Not only supervisors count, colleagues too! Motiv. Emot. 2012, 36, 268–286. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Shanafelt, T.D.; Balch, C.M.; Satele, D.; Sloan, J.; Freischlag, J. Relationship between work-home conflicts and burnout among American surgeons: A comparison by sex. Arch. Surg. 2011, 146, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, M.T.; Branscombe, N.R.; Kobrynowicz, D.; Owen, S. Perceiving discrimination against one’s gender group has different implications for well-being in women and men. Personal. Soc. Psychol. Bull. 2002, 28, 197–210. [Google Scholar] [CrossRef]




| Instruments to Assess Variables | Basic Psychological Needs | Outcome Variables | ||||
|---|---|---|---|---|---|---|
| Autonomy | Competence | Relatedness | Job Satisfaction 1 | Health Problems | Psychological Well-Being Well-Being Index (WHO-5) 2 | |
| Items from 6th EWCS | You can influence decisions that are important for your work? | Your job gives you the feeling of work well done? | You are treated fairly at your workplace? | On the whole, are you very satisfied, satisfied, not very satisfied or not at all satisfied with working conditions in your main paid job? | Over the last 12 months, did you suffer from any of health problems? Hearing problems, skin problems, backache, muscular pains in the shoulders, neck and/or upper limbs, muscular pains in lower limbs, headaches or eyestrain, injury/ies, anxiety, overall fatigue, and other. | How you have been feeling over the last two weeks. I have felt cheerful and in good spirits |
| You are involved in improving the work organisation or work processes of your department or organisation? | You have the feeling of doing useful work? | Your colleagues help and support you? | I have felt calm and relaxed | |||
| You are consulted before objectives are set for your work? | You know what is expected of you at work? | Your manager helps and supports you? | I have felt active and vigorous | |||
| You are able to apply your own ideas in your work? | You have enough time to get the job done? | I woke up feeling fresh and rested | ||||
| You have a say in the choice of your work colleagues? | My daily life has been filled with things that interest me | |||||
| Likert-Type | Valued from 1 to 5: never, rarely, sometimes, most of the time, and always. | Valued from 1 to 4: not all satisfied, not very satisfied, satisfied, and very satisfied | Two response options are offered (yes/no) | Valued from 1 to 6: at no time, some of the time, less than a half of the time, more than a half of the time, most of the time, and all of the time. | ||
| Variables | Min–Max | M(SD) | M(SD) Women | M(SD) Men | Gender Differences | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Autonomy | 1–5 | 3.13 (0.94) | 3.06 (0.93) | 3.46 (0.95) | t(1562) = 6.26, p < 0.001, md = 0.40 | (0.78) | ||||||
| 2. Competence | 1.25–5 | 4.36 (0.53) | 4.34 (0.53) | 4.43 (0.53) | t(1753) = 2.67, p = 0.008, md = 0.09 | 0.26 *** | (0.63) | |||||
| 3. Relatedness | 1–5 | 4.08 (0.71) | 4.08 (0.72) | 4.11 (0.69) | t(1530) = 0.59, p = 0.556, md = 0.03 | 0.36 *** | 0.45 *** | (0.66) | ||||
| 4. Basic Need Satisfaction | 1.28–5 | 3.82 (0.54) | 3.80 (0.54) | 3.93 (0.55) | t(1441) = 3.37, p = 0.001, md = 0.13 | 0.79 *** | 0.66 *** | 0.79 *** | (0.78) | |||
| 5. Satisfaction with Work Conditions | 1–4 | 3.12 (0.69) | 3.10 (0.69) | 3.21 (0.68) | χ2(3) = 8.23, p = 0.042, V = 0.07 | 0.29 *** | 0.32 *** | 0.41 *** | 0.43 *** | 1 | ||
| 6. Psychological Well-being | 1–6 | 4.46 (0.98) | 4.42 (0.99) | 4.63 (0.90) | t(1763) = 3.43, p = 0.001, md = 0.21 | 0.23 *** | 0.36 *** | 0.35 *** | 0.40 *** | 0.40 *** | (0.88) | |
| 7. Health Problems | 0–10 | 2.48 (2.09) | 2.60 (2.09) | 1.90 (1.96) | t(1752) = −5.37, p < 0.001, md = −0.70 | −0.14 *** | −0.18 *** | −0.21 *** | −0.23 *** | −0.30 *** | −0.38 *** | (0.70) |
| Country and Welfare State Regime | Code | Direct Effect Model: Wellbeing | Direct Effect Model: Health Problems | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| R2 | F | c’ | b1 | b2 | R2 | F | c’ | b1 | b2 | ||
| Conservative | 0.28 | 55.07 *** | −0.14 | 0.23 *** | 0.39 *** | 0.15 | 31.85 *** | 0.37 *** | −0.05 | −0.33 *** | |
| Austria | AT | 0.32 | 4.51 ** | −0.20 | 0.15 | 0.46 ** | 0.33 | 5.33 ** | 0.21 | −0.24 | −0.42 ** |
| Belgium | BE | 0.39 | 26.12 *** | −0.11 | 0.28 ** | 0.53 *** | 0.18 | 12.93 *** | 0.37 | −0.09 | −0.33 ** |
| France | FR | 0.26 | 6.90 *** | −0.14 | 0.42 ** | 0.18 | 0.14 | 4.44 ** | 0.59 | −0.39 ** | 0.06 |
| Germany | DE | 0.29 | 15.03 *** | −0.19 | 0.37 *** | 0.10 | 0.09 | 6.67 *** | 0.55 ** | 0.05 | −0.22 ** |
| Luxembourg | LU | 0.15 | 3.01 * | −0.18 | 0.03 | 0.42 * | 0.21 | 4.18 * | 0.24 | −0.12 | −0.44 ** |
| Netherlands | NL | 0.41 | 14.56 *** | −0.51 ** | −0.04 | 0.52 *** | 0.13 | 7.20 *** | 0.35 | 0.01 | −0.36 ** |
| Switzerland | CH | 0.19 | 3.96 * | 0.09 | 0.19 | 0.32 ** | 0.20 | 3.43 * | 0.31 | 0.01 | −0.39 * |
| Post-Communist | 0.17 | 31.94 *** | −0.10 | 0.28 *** | 0.20 *** | 0.09 | 20.07 *** | 0.40 *** | −0.05 | −0.25 *** | |
| Bulgaria | BG | 0.09 | 1.49 | −0.03 | 0.05 | 0.28 | 0.46 | 10.14 *** | −0.02 | 0.42 * | −0.47 *** |
| Croatia | HR | 0.31 | 5.05 ** | −0.09 | 0.15 | 0.48 ** | 0.28 | 10.41 *** | 0.38 | 0.01 | −0.57 *** |
| Czech Rep. | CZ | 0.04 | 1.04 | 0.32 | 0.10 | 0.06 | 0.12 | 1.44 | 0.03 | 0.04 | −0.35 * |
| Estonia | EE | 0.17 | 5.39 ** | −0.74 | 0.50 * | −0.07 | 0.03 | 1.25 | 0.02 | −0.15 | 0.20 |
| Hungary | HU | 0.25 | 2.29 | 0.24 | 0.30 * | 0.02 | 0.19 | 4.53 ** | 0.67 *** | −0.05 | −0.17 |
| Latvia | LV | 0.41 | 4.69 * | 0.78 | 0.01 | 0.73 ** | 0.15 | 18.25 *** | 0.05 * | 0.04 | −0.34 |
| Lithuania | LT | 0.31 | 3.86 * | 0.01 | 0.05 | 0.34 * | 0.13 | 1.99 | 0.51 | 0.01 | −0.28 |
| Poland | PL | 0.14 | 2.69 | −0.02 | 0.29 | 0.07 | 0.11 | 2.44 | 0.88 | −0.10 | −0.12 |
| Romania | RO | 0.61 | 13.98 *** | 0.80** | 0.47 *** | 0.41 * | 0.25 | 5.70 ** | 0.17 | −0.33 * | −0.21 |
| Slovakia | SK | 0.35 | 4.81 ** | 0.64 | 0.83 ** | 0.16 | 0.10 | 3.64 * | 0.47 | −0.10 | −0.25 |
| Slovenia | SI | 0.42 | 14.58 *** | −0.02 | 0.70 *** | 0.11 | 0.14 | 6.09 ** | 0.57 * | −0.23 | −0.11 |
| Montenegro | ME | 0.20 | 2.06 | −0.14 | −0.25 | 0.34 * | 0.21 | 7.01 ** | 0.87 ** | 0.04 | −0.27 |
| FYROM | MK | 0.24 | 4.87 ** | −0.19 | 0.56 *** | 0.11 | 0.15 | 2.78 | 0.51 | 0.22 | −0.29 |
| Serbia | RS | 0.08 | 1.57 | −0.62 | 0.11 | 0.19 | 0.18 | 4.17 * | 0.23 | −0.10 | −0.35 * |
| Albania | AL | 0.13 | 3.33 * | −0.35 | 0.17 | 0.15 | 0.02 | 0.19 | 0.01 | 0.01 | −0.10 |
| Mediterranean | 0.25 | 26.71 *** | 0.03 | 0.27 *** | 0.30 *** | 0.15 | 16.87 *** | 0.17 | −0.20 ** | −0.26 *** | |
| Cyprus | CY | 0.13 | 2.37 | −0.06 | 0.02 | 0.39 * | 0.21 | 4.72 ** | −0.04 | 0.12 | −0.48 ** |
| Greece | EL | 0.02 | 0.24 | 0.18 | 0.03 | −0.02 | 0.28 | 1.81 | −0.37 | −0.70 | 0.49 * |
| Italy | IT | 0.26 | 5.72 ** | −0.46 ** | −0.11 | 0.43 ** | 0.21 | 7.52 *** | 0.44 | 0.02 | −0.48 *** |
| Malta | MT | 0.57 | 12.75 *** | 0.22 | 0.60 *** | 0.32 ** | 0.25 | 5.75 ** | 0.64 ** | −0.11 | −0.21 |
| Portugal | PT | 0.58 | 9.41 ** | −0.89 ** | 0.64 ** | 0.07 | 0.10 | 1.06 | 0.11 | −0.34 | −0.02 |
| Spain | ES | 0.28 | 14.53 *** | 0.09 | 0.40 ** | 0.19 | 0.29 | 13.81 *** | 0.14 | −0.50 *** | −0.10 |
| Turkey | TR | 0.42 | 12.05 *** | 0.16 | 0.18 | 0.46 ** | 0.19 | 2.20 | −0.11 | 0.24 | −0.56 * |
| Social-Democratic | 0.22 | 26.46 *** | −0.13 | 0.39 *** | 0.13 | 0.10 | 9.08 *** | 0.09 | −0.24 *** | −0.07 | |
| Denmark | DK | 0.38 | 10.91 *** | −0.16 | 0.32 ** | 0.24 * | 0.20 | 3.56 * | −0.12 | −0.29 * | −0.14 |
| Finland | FI | 0.32 | 9.16 *** | 0.05 | 0.18 | 0.38 ** | 0.25 | 4.53 ** | −0.31 ** | −0.37 | −0.11 |
| Sweden | SE | 0.13 | 3.84 * | −0.06 | 0.35 * | 0.05 | 0.10 | 3.35 * | 0.28 | −0.25 * | 0.03 |
| Norway | N | 0.29 | 15.81 *** | −0.57 | 0.74 *** | −0.10 | −13 | 5.17 ** | 0.58 ** | −0.15 | −0.17 |
| Liberal | 0.17 | 9.36 *** | −0.13 | 0.24 * | 0.25 ** | 0.14 | 6.24 *** | 0.19 | −0.22 * | −0.19 * | |
| Ireland | IE | 0.19 | 4.35 ** | 0.21 | 0.09 | 0.33 * | 0.10 | 2.47 | −0.27 | −0.22 * | −0.07 |
| UK | UK | 0.19 | 6.26 *** | −0.31 | 0.34 * | 0.17 | 0.20 | 6.09 ** | 0.48 * | −0.14 | −0.28 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Baya, D.; Lucia-Casademunt, A.M.; Salinas-Pérez, J.A. Gender Differences in Psychological Well-Being and Health Problems among European Health Professionals: Analysis of Psychological Basic Needs and Job Satisfaction. Int. J. Environ. Res. Public Health 2018, 15, 1474. https://doi.org/10.3390/ijerph15071474
Gómez-Baya D, Lucia-Casademunt AM, Salinas-Pérez JA. Gender Differences in Psychological Well-Being and Health Problems among European Health Professionals: Analysis of Psychological Basic Needs and Job Satisfaction. International Journal of Environmental Research and Public Health. 2018; 15(7):1474. https://doi.org/10.3390/ijerph15071474
Chicago/Turabian StyleGómez-Baya, Diego, Ana M. Lucia-Casademunt, and José A. Salinas-Pérez. 2018. "Gender Differences in Psychological Well-Being and Health Problems among European Health Professionals: Analysis of Psychological Basic Needs and Job Satisfaction" International Journal of Environmental Research and Public Health 15, no. 7: 1474. https://doi.org/10.3390/ijerph15071474